
Abstract
Background
To address a current paucity of European data, this study developed equations to predict risks of mortality, major adverse cardiac events (MACE) and renin angiotensin-aldosterone system inhibitor (RAASi) discontinuation using time-varying serum potassium and other covariates, in a UK cohort of chronic kidney disease (CKD) patients.
Methods
This was a retrospective observational study of adult CKD patients listed on the Clinical Practice Research Datalink, with a first record of CKD (stage 3a–5, pre-dialysis) between 2006 and 2015. Patients with heart failure at index were excluded. Risk equations developed using Poisson Generalized Estimating Equations were utilised to estimate adjusted incident rate ratios (IRRs) between serum potassium and adverse outcomes, and identify other predictive clinical factors.
Results
Among 191,964 eligible CKD patients, 86,691 (45.16%), 30,629 (15.96%) and 9440 (4.92%) experienced at least one hyperkalaemia episode, when defined using serum potassium concentrations 5.0–< 5.5 mmol/L, 5.5–< 6.0 mmol/L and ≥ 6.0 mmol/L, respectively. Relative to the reference category (4.5 to < 5.0 mmol/L), adjusted IRRs for mortality and MACE exhibited U-shaped associations with serum potassium, with age being the most important predictor of both outcomes (P < 0.0001). A J-shaped association between serum potassium and RAASi discontinuation was observed; estimated glomerular filtration rate was most predictive of RAASi discontinuation (P < 0.0001).
Conclusions
Hyperkalaemia was associated with increased mortality and RAASi discontinuation risk. These risk equations represent a valuable tool to predict clinical outcomes among CKD patients; and identify those likely to benefit from strategies that treat hyperkalaemia, prevent RAASi discontinuation, and effectively manage serum potassium levels.
Similar content being viewed by others


Background
Hyperkalaemia, typically defined as serum potassium concentration exceeding 5.0 mmol/L, is a potentially life-threatening electrolyte imbalance [1]. Recent epidemiological studies have consistently demonstrated associations between hyperkalaemia and adverse clinical outcomes; notably hospitalisation, cardiovascular morbidity and mortality [2,3,4,5,6].
As a consequence of impaired renal function, patients with chronic kidney disease (CKD) are at increased risk of hyperkalaemia; and renin-angiotensin-aldosterone system inhibitor (RAASi) agents routinely indicated for CKD management [1, 7] are known to exacerbate this risk [8]. Despite this, the current practice of down-titrating or discontinuing guideline-recommended RAASi therapy in response to acute hyperkalaemia [9, 10] has recently been associated with worsening clinical outcomes and greater total costs in patients with CKD or other comorbidities [11,12,13,14].
Real-world studies associating serum potassium and adverse clinical outcomes in CKD patients, including death, major adverse cardiac events (MACE), hospitalisation and RAASi discontinuation, have previously been conducted in the US [2,3,4,5,6]. In contrast to other industrialised countries, healthcare in the US is largely privatised, and the availability of clinical data may be limited by the size, length and claims-based nature of US healthcare records. Thus, it is unclear whether existing data describing the epidemiology and burden of hyperkalaemia may be generalisable to a European CKD population. Using primary care data obtained from the Clinical Practice Research Datalink (CPRD) [15], this study sought to develop risk equations describing the relationship between serum potassium concentration and incidence of death, MACE and RAASi discontinuation, in a contemporary UK cohort of CKD patients.
Methods
Study data and patient population
This retrospective analysis utilised data from the CPRD and linked Hospital Episode Statistics (HES). The CPRD is an observational research database comprised of anonymised, longitudinal primary care records for approximately 7% of the UK population. It is broadly representative of the general population, and is the world’s largest computerised database of medical records suitable for public health research [16]. Linked HES data described admissions, outpatient appointments, and emergency episodes in National Health Service hospitals in England [17]. The study was approved by the Independent Scientific Advisory Committee for Medicines and Healthcare Products Regulatory Agency database research on 15 December 2016 (study protocol 16_223R).
Inclusion criteria for the study were adult CKD patients (aged ≥18 years) in the CPRD between 1 January 2006 and 31 December 2015, who experienced a first record of CKD (stage 3a to 5, pre-dialysis; herein referred to as the index date) after the study start date. Patients were selected on the basis of estimated glomerular filtration rate (eGFR; defined as < 60 mL/min/1.73m2 [7]), Read codes (CPRD), and ICD-10 codes (HES). Exclusion criteria comprised patients on dialysis at index date or with a CKD event prior to 1 January 2006, and patients with a history of heart failure (HF; identified by Read and ICD-10 codes) at index date, due to the increased risk of hyperkalaemia associated with RAASi usage [9]. Read and ICD-10 codes were further used to define clinical outcomes and covariates (Additional file 1: Table S1).
Study design and data structuring
The clinical outcomes studied in this analysis included all-cause mortality, incidence of MACE (myocardial infarction, arrhythmia, HF, and stroke), and discontinuation of RAASi medications. Using the medicines possession ratio, RAASi discontinuation was defined as the first 90-day gap after the estimated end-date of a RAASi prescription. Agents comprising RAASi therapy included angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), mineralocorticoid receptor antagonists (MRAs), and renin inhibitors. Hyperkalaemia was defined according to serum potassium intervals of ≥5.0 mmol/L to < 5.5 mmol/L, ≥5.5 mmol/L to < 6.0 mmol/L, and ≥ 6.0 mmol/L. Serum potassium < 3.5 mmol/L was classified as hypokalaemia.
Serum potassium was time-updated during the follow-up period; an illustrative example of this methodology is provided in Additional file 1 and Additional file 2: Figure S1. In brief, each patient’s most recent serum potassium measurement was applied until a new measurement became available, using a last-observation-carried-forward (LOCF) approach [4]. Further, time-updated eGFR readings were the most recently available at the time of each serum potassium measurement. The period between serum potassium measurements defined patient-intervals, and clinical events of interest were assigned to these based on the date on which they occurred.
Time-updated serum potassium was evaluated categorically (< 3.5, 3.5 to < 4.0, 4.0 to < 4.5, 4.5 to < 5.0, 5.0 to < 5.5, 5.5 to < 6.0, and ≥ 6.0 mmol/L). Exposure time in each serum potassium category was quantified in patient-years. Patients were followed up to and including the first occurrence of loss to follow-up, end of study period (31 December 2015), or death.
Statistical analyses
The data were analysed using R version 3.3.2 [18]. Means, medians, counts and/or proportions, and associated measures of variability were used to describe patient demographics. Patient characteristics at index date were used to calculate summary statistics; baseline clinical measurements were defined as the first measurement taken in the 3 months following the index date. Disease history was analysed over the 5 years prior to the index date and was expressed using counts and proportions. Medication usage at baseline was defined as having at least one prescription during a six-month period centred around the index date and expressed as counts and proportions. Missing values were not included in calculations relating to baseline patient characteristics, disease history and medication usage.
Hyperkalaemia episodes of increasing severity were defined as serum potassium measurements within each interval (≥5.0 mmol/L to < 5.5 mmol/L, ≥5.5 mmol/L to < 6.0 mmol/L, and ≥ 6.0 mmol/L), without a hyperkalaemic measurement of at least that severity (serum potassium ≥5.0 mmol/L, ≥5.5 mmol/L, and ≥ 6.0 mmol/L, respectively) in the preceding 7 days. Subsequently, hyperkalaemia episodes were assumed to persist for a maximum duration of 1 week. The median time between successive episodes was calculated among only those patients who experienced the given number of episodes; censoring due to death, loss to follow-up or end of study period was not taken into account.
The incidence of each outcome (death, MACE and RAASi discontinuation) was predicted using a risk equation obtained by fitting a statistical model to the event count in each patient-interval. Risk equations were estimated using Generalized Estimating Equations with an exchangeable working correlation structure to account for intra-patient correlation. Events were assumed to be Poisson distributed. Risk equations included a natural logarithm link function and an offset equal to the natural logarithm of patient-years (defined as the exposure time in each patient-interval). Patients with a serum potassium of 4.5 to < 5.0 mmol/L were used as the reference group for comparison, from which incident rate ratios (IRRs) were estimated.
To address the possibility of long durations between measurements of serum potassium and the incidence of death, MACE and RAASi discontinuation, adjusted IRRs were re-estimated after restricting patient-intervals to a maximum of 30 days post-potassium measurement. Additional sensitivity analysis explored the relationship between CKD stage and observed associations between serum potassium and clinical outcomes, by estimating adjusted IRRs in CKD patients stratified according to time-updated eGFR: 45 to < 60 mL/min/1.73m2 (CKD 3a); 30 to < 45 mL/min/1.73m2 (CKD 3b); 15 to < 30 mL/min/1.73m2 (CKD 4); < 15 mL/min/1.73m2 (CKD 5).
Multiple imputation was used to inform missing baseline measurements when estimating the risk equations, which were carried forward using LOCF. Five multiply imputed datasets were produced; model coefficients and their standard errors were pooled across datasets using Rubin’s Rules [19], in order to capture the variance of the coefficients both within and between the imputed datasets. Using the method of Chained Equations, as implemented in the R package ‘mice’ [18], multiple imputation was performed on all clinical variables with all candidate covariates and outcome variables from the analysis models included in the imputation models.
Model assessment and final selection was informed by the Quasi-Likelihood Information Criterion on a randomly selected training sub-sample, and the prediction mean squared error on a randomly-selected validation sub-sample [20]. Predicted incidence rates and IRRs were adjusted for covariates, included as explanatory variables in the risk equations. Adjusted IRRs relating serum potassium to the incidence of mortality and MACE estimated by the fitted risk equations were validated against those published by Luo et al. [4]: a real-world study of CKD stage 3+ patients of similar design to the present study, but using data collected in the US.
Results
Patient demographics and characteristics at baseline
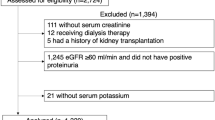
The analysed cohort consisted of 191,964 eligible CKD patients, with a mean follow-up time of 4.96 years (Fig. 1; Table 1). At baseline, the mean age was 72.48 years, the majority of the cohort was female (60.61%), and diabetes was the most prevalent comorbidity (14.63%). Based on the earliest measurement recorded in the first 3 months post-index, mean eGFR was 50.96 mL/min/1.73m2 and mean serum potassium was 4.47 mmol/L. When patients were stratified by serum potassium category at baseline, the proportion of female patients in each subgroup decreased from 68.50% (< 3.5 mmol/L category) to 53.22% (≥6.0 mmol/L category).

Study participation flow diagram. CKD: chronic kidney disease; CPRD: Clinical Practice Research Datalink; eGFR: estimated glomerular filtration rate; HF: heart failure; ICD: International Classification of Diseases
Approximately half of patients (48.06%) received RAASi therapy, with ACE inhibitors being the most commonly used agent (35.36%). When stratified according to baseline serum potassium, patients with increasing potassium levels were typically more likely to receive ACE inhibitors, ARBs and MRAs. Other frequently prescribed medications included statins (43.14%), diuretics (40.19%), β-blockers (25.30%), and dihydropyridine calcium channel blockers (23.78%).
In the absence of CKD-specific dosing guidelines, Table 2 presents the proportion of patients who received RAASi agents at doses recommended in European Society of Cardiology guidelines for heart failure management [9]. Over one-third of patients receiving ACE inhibitors or MRAs (36.11% and 36.02%, respectively) achieved the target maintenance dose for these therapies; in contrast, 3.28% of those receiving ARBs achieved the target dose. The majority of ARB-treated patients (59.48%) achieved less than 50% of the recommended target dose, compared to 37.38% of patients receiving ACE inhibitors. No patients in receipt of MRAs achieved less than 50% of the recommended target dose.
Serum potassium and hyperkalaemia
Using serum potassium intervals of ≥5.0 mmol/L to < 5.5 mmol/L, ≥5.5 mmol/L to < 6.0 mmol/L, and ≥ 6.0 mmol/L to define hyperkalaemia of increasing severity, 86,691 (45.16%), 30,629 (15.96%) and 9440 (4.92%) patients experienced at least one episode over the follow-up period, respectively (Table 3). Based on these serum potassium thresholds, crude incidence rates of hyperkalaemia were 246.02, 62.66 and 15.00 events per 1000 patient-years, respectively. Hyperkalaemia recurrence exhibited a notable pattern; time intervals between successive episodes of serum potassium ≥5.0 mmol/L to < 5.5 mmol/L decreased from 1.80 years (time to first episode), to 0.99 years (first to second episode), to 0.76 years (second to third episode), and to 0.61 years (third to fourth episode). Similar patterns held true when hyperkalaemia was defined according to serum potassium intervals of ≥5.5 mmol/L to < 6.0 mmol/L and ≥ 6.0 mmol/L.
Incidence of death, MACE, and RAASi discontinuation
In total, 44,961 deaths, 80,038 MACE and 75,488 RAASi discontinuation events were observed over the follow-up period, which corresponded to crude event rates of 47, 84 and 79 per 1000 patient-years, respectively (Additional file 1: Table S2).
When considering the full duration of patient-intervals between serum potassium measurements, adjusted IRRs for death exhibited a U-shaped association with categorical serum potassium levels (Fig. 2a). Relative to the reference category of 4.5 to < 5.0 mmol/L, serum potassium < 4.0 mmol/L and ≥ 5.0 mmol/L were each associated with increased mortality risk. Among patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L, the adjusted IRR for mortality was 1.60 (95% CI: 1.52–1.68) compared with the reference category, which increased to 2.88 (2.61–3.18) in patients with serum potassium ≥6.0 mmol/L. In validation, the U-shaped association pattern between potassium and mortality observed in this study was similar to that published by Luo et al. [4] (Additional file 3: Figure S2); in the case of the latter, an adjusted IRR of 1.60 (1.37–1.88) was estimated for patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L (as observed in our study), but a somewhat larger IRR of 3.31 (2.52–4.34) was estimated for patients with serum potassium ≥6.0 mmol/L (compared to 2.88 in our study).

Adjusted incident rate ratios for death (a), MACE (b) and RAASi discontinuation (c) as a function of serum potassium in CKD patients. Black: full patient-intervals; grey: patient-intervals restricted to 30 days. Incident rate ratios were adjusted to account for confounding patient demographics, clinical histories and comorbidities, clinical measurements, and medication usage, as reported in Table 4 and Additional file 1 : Table S3. CKD: chronic kidney disease; MACE: major adverse cardiac event; RAASi: renin-angiotensin-aldosterone system inhibitor. Error bars represent 95% confidence intervals
Similar to mortality, serum potassium levels < 4.0 mmol/L were associated with increased risks of MACE when the full duration of patient-intervals were utilised (Fig. 2b). However, confidence intervals relating to serum potassium ≥5.0 mmol/L contained an IRR of unity, reflecting increased uncertainty of the association between hyperkalaemia and MACE. Relative to the reference category, adjusted IRRs for MACE were 1.07 (1.00–1.15) and 1.15 (0.98–1.36) for patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L and ≥ 6.0 mmol/L, respectively. In validation, the association between serum potassium and MACE estimated by Luo et al. [4] exhibited a more pronounced U-shaped pattern than that observed in our study (Additional file 3: Figure S2), with larger and statistically significant adjusted IRRs of 1.12 (1.05–1.20) and 1.88 (1.66–2.12) for patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L and ≥ 6.0 mmol/L, respectively.
Associations between adverse event risk and serum potassium concentration were more pronounced after restricting patient-intervals to a maximum of 30 days from each serum potassium measurement. Relative to the reference category, adjusted IRRs for patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L were estimated as 2.03 (1.84–2.23) and 0.97 (0.89–1.06) for mortality and MACE, respectively; these increased to 4.39 (3.88–4.97) and 1.29 (1.08–1.55), respectively, among patients with serum potassium ≥6.0 mmol/L.
The association between categorical serum potassium and the incidence of RAASi discontinuation was observed to be J-shaped (Fig. 2c). Based on the full duration of patient-intervals between serum potassium measurements, adjusted IRRs for RAASi discontinuation were estimated as 1.47 (1.42–1.53) for patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L, and increased to 2.79 (2.61–2.99) among those with serum potassium ≥6.0 mmol/L, when compared to the reference category. Following restriction of patient-intervals to a maximum of 30 days from each serum potassium measurement, adjusted IRRs for RAASi discontinuation increased to 1.90 (1.79–2.03) and 4.37 (3.99–4.79) among patients with serum potassium ≥5.5 mmol/L to < 6.0 mmol/L and ≥ 6.0 mmol/L, respectively.
Observed associations between serum potassium and clinical outcomes were preserved when patients were stratified by CKD stage in sensitivity analyses (Additional file 4: Figure S3). Adjusted IRRs for mortality, MACE and RAASi discontinuation in patients with CKD 3a, CKD 3b, CKD 4 and CKD 5 demonstrated similar trends to one another and to the overall cohort; however, smaller sample sizes gave rise to wider confidence intervals and greater uncertainty, particularly for patients with eGFR < 15 mL/min/1.73m2.
Table 4 summarises coefficient estimates and statistical inferences relating to the final fitted risk equations. In addition to serum potassium concentration, age and sex were significant risk factors for both death and MACE (P < 0.0001). Death was also significantly associated with RAASi usage, time with CKD and eGFR, while history of MACE of baseline was a significant risk factor for MACE during follow-up (all P < 0.0001). For RAASi discontinuation, the most important risk factors were eGFR, diuretics usage, diabetes status and sex (all P < 0.0001). Coefficient estimates and statistical inferences obtained after re-estimating the equations on patient-intervals restricted to a maximum of 30 days are provided in Additional file 1 (Table S3).
To illustrate the predictive outputs of the risk equations, Fig. 3 presents the expected rates of death (per 1000 patient-years) as a function of serum potassium level. Predicted mortality rates were further disaggregated by the four most important predictive factors: age, RAASi usage, time with CKD and eGFR (Fig. 3a, b, c and d, respectively). Similarly, association patterns between serum potassium and MACE incidence, disaggregated by age, history of MACE, time from index and sex, are illustrated in Fig. 4a, b, c and d, respectively. Expected rates of RAASi discontinuation according to serum potassium level are presented in Fig. 5, disaggregated by eGFR, diuretics usage, diabetes status and sex (Fig. 5a, b, c and d, respectively).

Predicted incidence rates of death, disaggregated by age (a), RAASi usage (b), time from index (c) and eGFR (d). a light grey line: 60 years, dark grey line: 70 years, black line: 80 years. b grey line: not prescribed, black line: prescribed. c light grey line: 1 year, dark grey line: 5 years, black line: 10 years. d light grey line: 15 mL/min/1.73m2, dark grey line: 30 mL/min/1.73m2, black line: 60 mL/min/1.73m2. The four most important variables for each event (according to the absolute value of the t statistic) were varied, with all other baseline covariates reflective of the cohort average: female; aged 72 years; non-smoker; no history of comorbidities; no medications prescribed; 1066 days elapsed since initial CKD event; no history of heart failure during follow-up period; eGFR 51 mL/min/1.73m2; BMI 29 kg/m2; haemoglobin 13.6 g/dL; total cholesterol 4.98 mmol/L. BMI: body mass index; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; RAASi: renin-angiotensin-aldosterone system inhibitor

Predicted incidence rates of MACE, disaggregated by age (a), history of MACE (b), time from index (c) and sex (d). a light grey line: 60 years, dark grey line: 70 years, black line: 80 years. b grey line: yes, black line: no. c light grey line: 1 year, dark grey line: 5 years, black line: 10 years. d grey line: male, black line: female. The four most important variables for each event (according to the absolute value of the t statistic) were varied, with all other baseline covariates reflective of the cohort average: female; aged 72 years; non-smoker; no history of comorbidities; no medications prescribed; 1066 days elapsed since initial CKD event; no history of heart failure during follow-up period; eGFR 51 mL/min/1.73m2; BMI 29 kg/m2; haemoglobin 13.6 g/dL; total cholesterol 4.98 mmol/L. BMI: body mass index; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; MACE: major adverse cardiac event

Predicted incidence rates of RAASi discontinuation, disaggregated by eGFR (a), diuretics usage (b), presence of diabetes (c), and sex (d). a light grey line: 15 mL/min/1.73m2, dark grey line: 30 mL/min/1.73m2, black line: 60 mL/min/1.73m2. b grey line: yes, black line: no. c grey line: yes, black line: no. d grey line: male, black line: female. The four most important variables for each event (according to the absolute value of the t statistic) were varied, with all other baseline covariates reflective of the cohort average: female; aged 72 years; non-smoker; no history of comorbidities; no medications prescribed; 1066 days elapsed since initial CKD event; no history of heart failure during follow-up period; eGFR 51 mL/min/1.73m2; BMI 29 kg/m2; haemoglobin 13.6 g/dL; total cholesterol 4.98 mmol/L. BMI: body mass index; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; RAASi: renin-angiotensin-aldosterone system inhibitor
Discussion
Using real-world data from 191,964 CKD patients in the UK, we derived risk equations that may be used in clinical practice to relate serum potassium and other predictive factors to the incidence of mortality, MACE and RAASi discontinuation. Adjusted IRRs derived in this analysis demonstrated U-shaped associations between serum potassium and the risks of mortality and MACE (though not as strongly in the case of the latter); and a J-shaped association between serum potassium and the incidence of RAASi discontinuation. Other statistically important predictors of adverse clinical outcomes included age and sex, time with CKD, RAASi usage, eGFR, and history of MACE. The risk equations presented here represent a valuable tool to identify CKD patients at increased risk of adverse clinical outcomes; and those most likely to benefit from strategies that avoid hyperkalaemia, prevent RAASi discontinuation, and effectively maintain serum potassium homeostasis.
Our findings are broadly consistent with literature reporting relationships between hypo- and hyperkalaemia and worsening clinical outcomes in CKD patients [2,3,4,5]. In particular, mortality risk was lowest among patients with serum potassium between 4.0–5.0 mmol/L; an optimal range similarly identified in recent US studies associating serum potassium with all-cause mortality in patients with and without CKD, HF and/or diabetes [6], and those examining in-hospital mortality risk among hospitalised patients with CKD and/or cardiovascular disease [21]. Other US studies have also demonstrated significant relationships between all-cause mortality and both hypo- (< 3.5 mmol/L) and hyperkalaemia (> 5.0 mmol/L) in patients with CKD stages 3–4 [22]; and between both all-cause mortality and hospital admissions and hyperkalaemia (> 5.0 mmol/L) in cardiovascular disease patients treated with antihypertensive medications that impair potassium homeostasis [23]. Although cause of death was not explored in our analysis due to a paucity of relevant CPRD data, a previous study of CKD patients with coronary artery disease found that the risk of sudden cardiac arrest and death doubled when serum potassium measurements taken before the event exceeded 5.0 mmol/L [24].
Additional sensitivity analyses found that observed relationships between serum potassium and mortality, MACE and RAASi discontinuation were preserved when patients were stratified by CKD stage, with little variation in the association patterns between stages. This finding is consistent with a similar study by Luo et al., who found no significant interaction between eGFR and serum potassium when predicting mortality in a US CKD 3+ population [4]. However, it is noteworthy that observed relationships between serum potassium and risks of mortality and MACE in the overall CKD cohort were comparatively weaker than those estimated by Luo et al. [4]. While our study examined an incident CKD cohort, associations reportered herein may have been strengthened by the inclusion of a prevalent CKD population. Death within 30 days of MACE occurred for approximately 2% of MACE events recorded in this study; therefore, relationships between serum potassium and MACE may be underestimated, due to potential under-reporting of fatal MACE in primary care and a lack of cause of death data. Moreover, although previous studies have generally found that deaths recorded on the CPRD are in concordance with Office for National Statistics national mortality registrations [25], less is known about the reverse. However, an important consideration is the difference in contextual settings and populations captured by each database, particularly regarding patient demographics, clinical characteristics, treatment paradigms and healthcare systems. One notable strength of our study is the use of the CPRD, which contains primary care data for a large, diverse population with access to publicly-funded healthcare. Compared to existing US data, it could therefore be suggested that our results are more generalisable to other countries and healthcare systems, particularly those across Europe.
We demonstrated a J-shaped association pattern between serum potassium and RAASi discontinuation risk. Adjusted IRRs reported here relate to RAASi discontinuation rates estimated among all patients and intervals observed during the study period. However, when alternative definitions of RAASi exposure were investigated (such as only including patients in receipt of RAASi over the duration of the follow-up period, or intervals where a RAASi therapy had been prescribed), the association pattern between serum potassium levels and the likelihood of RAASi discontinuation was preserved. This J-shaped association is consistent with prescribing guidelines, where hyperkalaemia risk among patients treated with RAASi is commonly managed through the down-titration or discontinuation of such potassium-retaining agents [9, 10]. When delivered at guideline-recommended doses, RAASi have been evidenced to control blood pressure, delay disease progression and improve long-term outcomes in CKD patients [7, 9, 26,27,28]; however, suboptimal dosing has conversely been associated with increased adverse event risks and healthcare costs [11,12,13,14]. Consequently, strategies to control serum potassium and avoid RAASi discontinuation represent an important advance in CKD management, and have significant potential to improve health economic outcomes. The risk equations generated in this study are intended to inform the potential value of maintaining normal serum potassium levels in CKD patients, and identify clinical factors that place patients at greater risk of RAASi discontinuation, MACE and death.
There is no single definition of hyperkalaemia; therefore, comparisons of incidence and outcomes across epidemiological studies are often obscured by inconsistent serum potassium thresholds. As shown in this study, the incidence of hyperkalaemia was highly sensitive to the serum potassium threshold used to define it; and estimated IRRs of death, MACE and RAASi discontinuation were higher with increasing serum potassium levels. Had the sample size allowed for such analysis, we believe that further stratification of patients with serum potassium ≥6.0 mmol/L would have strengthened the association pattern between serum potassium and adverse event risk. Nevertheless, our results highlight the importance of a standardised definition of hyperkalaemia, to facilitate valid comparisons between observational studies and across different populations.
To our knowledge, few studies have examined the time between successive hyperkalaemia episodes in patients with recurrent hyperkalaemia. A noteworthy pattern observed in our analyses was the shortening of intervals between successive hyperkalaemia episodes, irrespective of the serum potassium intervals used to define events of increasing severity (≥5.0 mmol/L to < 5.5 mmol/L, ≥5.5 mmol/L to < 6.0 mmol/L, and ≥ 6.0 mmol/L). Given the impact of hyperkalaemia on patient morbidity, mortality and associated resource utilisation, our findings highlight the importance of sustained potassium management following discharge from immediate medical care, in order to avoid the burden of recurrent hyperkalaemia on patients and healthcare systems.
A number of limitations of this study are worth noting, and predominantly relate to the constraints of the data used to inform our analyses. The CPRD dataset may overestimate the incidence of hyperkalaemia due to pseudo-hyperkalaemia, a consequence of haemolysis following traumatic venepuncture, fist clenching during phlebotomy, blood sample contamination, inadequate blood sample storage, and delays between venepuncture and sample analysis [29]. Although causality cannot be inferred from this retrospective, observational database study, estimated IRRs for death, MACE and RAASi discontinuation were adjusted to account for confounding patient demographics, clinical histories and comorbidities, clinical measurements, and selected medication usage. Declining renal function was controlled for in our risk equations by including eGFR as a time-varying covariate; however, we acknowledge that related indices of kidney function (such as proteinuria) were not included in our analyses. Other candidate covariates were limited to those variables available within the CPRD; consequently, a number of unobserved or poorly-recorded potential confounders were not considered, such as socio-demographics, diet, lifestyle, ethnicity, smoking status, and the use of potassium-binding agents. Despite these limitations, the size of the CPRD dataset allowed this study to produce statistically-robust estimates of adverse event risk that verified the association curves observed across different geographical locations and comorbid populations.
Conclusions
In conclusion, this retrospective, observational cohort study sought to describe relationships between serum potassium levels and adverse clinical outcomes among CKD patients in UK clinical practice. Data arising from our analyses emphasise the importance of maintaining serum potassium levels within a narrow physiological range, in order to lower the risks of mortality, MACE and RAASi discontinuation. The risk equations derived represent a valuable tool to predict the incidence of adverse outcomes based on clinical characteristics; and identify CKD patients most likely to benefit from strategies that avoid hypo- and hyperkalaemia, enable optimal RAASi therapy, prevent RAASi discontinuation, and improve long-term outcomes.
Abbreviations
- ACE:
-
Angiotensin-converting enzyme
- ARB:
-
Angiotensin II receptor blocker
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- CPRD:
-
Clinical Practice Research Datalink
- eGFR:
-
Estimated glomerular filtration rate
- HES:
-
Hospital Episode Statistics
- HF:
-
Heart failure
- IRR:
-
Incident rate ratio
- LOCF:
-
Last-observation-carried-forward
- MACE:
-
Major adverse cardiac event
- MRA:
-
Mineralocorticoid receptor antagonist
- RAASi:
-
Renin-angiotensin-aldosterone system inhibitor
References
Hollander-Rodriguez JC, Calvert JF. Hyperkalemia. Am Fam Physician. 2006;73(2):283–90.
Einhorn LM, Zhan M, Hsu VD, Walker LD, Moen MF, Seliger SL, et al. The frequency of hyperkalemia and its significance in chronic kidney disease. Arch Intern Med. 2009;169(12):1156–62.
Hayes J, Kalantar-Zadeh K, Lu JL, Turban S, Anderson JE, Kovesdy CP. Association of hypo-and hyperkalemia with disease progression and mortality in males with chronic kidney disease: the role of race. Nephron Clin Pract. 2012;120(1):c8–16.
Luo J, Brunelli SM, Jensen DE, Yang A. Association between serum potassium and outcomes in patients with reduced kidney function. Clin J Am Soc Nephrol. 2016;11(1):90–100.
Korgaonkar S, Tilea A, Gillespie BW, Kiser M, Eisele G, Finkelstein F, et al. Serum potassium and outcomes in CKD: insights from the RRI-CKD cohort study. Clin J Am Soc Nephrol. 2010;5(5):762–9.
Collins AJ, Pitt B, Reaven N, Funk S, McGaughey K, Wilson D, et al. Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes. Am J Nephrol. 2017;46(3):213–21.
Kidney Disease Improving Global Outcomes. KDIGO 2012 clinical practice guideline for the evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3(1):1–150.
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N Engl J Med. 1999;341(10):709–17.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(27):2129–200.
Queen Mary University of London Clinical Effectiveness Group. Summary guidelines: Heart Failure update. 2015. https://www.qmul.ac.uk/blizard/ceg/media/blizard/documents/ceg-documents/Heart-Failure-Update,-Nov-2015.pdf. Accessed 25 Oct 2017.
Epstein M, Reaven NL, Funk SE, McGaughey KJ, Oestreicher N, Knispel J. Evaluation of the treatment gap between clinical guidelines and the utilization of renin-angiotensin-aldosterone system inhibitors. Am J Manag Care. 2015;21(Suppl 11):s212–20.
Epstein M. Hyperkalemia constitutes a constraint for implementing renin-angiotensin-aldosterone inhibition: the widening gap between mandated treatment guidelines and the real-world clinical arena. Kidney Int Suppl. 2016;6(1):20–8.
Ouwerkerk W, Voors A, Anker S, Cleland JG, Dickstein K, Filippatos G, et al. Determinants and clinical outcome of uptitration of ACE-inhibitors and beta-blockers in patients with heart failure: a prospective European study. Eur Heart J. 2017;38:1883–90.
Komajda M, Cowie MR, Tavazzi L, Ponikowski P, Anker SD, Filippatos GS. Physicians' guideline adherence is associated with better prognosis in outpatients with heart failure with reduced ejection fraction: the QUALIFY international registry. Eur J Heart Fail. 2017;19(11):1414–23.
Medicines and Healthcare Products Regulatory Agency. Clinical Practice Research Datalink. 2017. https://www.cprd.com/home/. Accessed 19 Sept 2017.
Herrett E, Gallagher AM, Bhaskaran K, Forbes H, Mathur R, van Staa T, et al. Data resource profile: clinical practice research datalink (CPRD). Int J Epidemiol. 2015;44(3):827–36.
NHS Digital. Hospital episode statistics. 2017. http://content.digital.nhs.uk/hes. Accessed 20 Sept 2017.
The R Foundation. The R Project for Statistical Computing, Vienna, Austria. 2017. https://www.R-project.org/. Accessed 27 July 2017.
Rubin DB. Multiple imputation for nonresponse in surveys. New Jersey: Wiley; 2004.
Pan W. Akaike's information criterion in generalized estimating equations. Biometrics. 2001;57(1):120–5.
Cheungpasitporn W, Thongprayoon C, Kittanamongkolchai W, Sakhuja A, Mao MA, Erickson SB. Impact of admission serum potassium on mortality in patients with chronic kidney disease and cardiovascular disease. QJM. 2017;110(11):713–9.
Nakhoul GN, Huang H, Arrigain S, Jolly SE, Schold JD, Nally JV Jr, et al. Serum potassium, end-stage renal disease and mortality in chronic kidney disease. Am J Nephrol. 2015;41(6):456–63.
Jain N, Kotla S, Little BB, Weideman RA, Brilakis ES, Reilly RF, et al. Predictors of hyperkalemia and death in patients with cardiac and renal disease. Am J Cardiol. 2012;109(10):1510–3.
Pun PH, Goldstein BA, Gallis JA, Middleton JP, Svetkey LP. Serum potassium levels and risk of sudden cardiac death among patients with chronic kidney disease and significant coronary artery disease. Kidney Int Rep. 2017;2(6):1122–31.
Harshfield A, Rhodes K, Barclay S, Payne R. The accuracy of death dates recorded in the clinical practice research datalink (CPRD). Society for Academic Primary Care ASM; 2017.
Evans M, Bain SC, Hogan S, Bilous RW. Irbesartan delays progression of nephropathy as measured by estimated glomerular filtration rate: post hoc analysis of the Irbesartan diabetic nephropathy trial. Nephrol Dial Transplant. 2012;27(6):2255–63.
Xie X, Liu Y, Perkovic V, Li X, Ninomiya T, Hou W, et al. Renin-angiotensin system inhibitors and kidney and cardiovascular outcomes in patients with CKD: a Bayesian network meta-analysis of randomized clinical trials. Am J Kidney Dis. 2016;67(5):728–41.
Currie G, Taylor AH, Fujita T, Ohtsu H, Lindhardt M, Rossing P, et al. Effect of mineralocorticoid receptor antagonists on proteinuria and progression of chronic kidney disease: a systematic review and meta-analysis. BMC Nephrol. 2016;17(1):127.
Asirvatham JR, Moses V, Bjornson L. Errors in potassium measurement: a laboratory perspective for the clinician. N Am J Med Sci. 2013;5(4):255–9.
Acknowledgements
Editorial assistance in the preparation of this manuscript was provided by Dr. Karina Hamilton and Dr. Daniel Sugrue of Health Economics and Outcomes Research Ltd. The authors also thank Dr. Susan Grandy and Dr. Klas Bergenheim of AstraZeneca, for their support and contribution to this work.
Funding
This study was supported by a grant from AstraZeneca. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, and preparing the manuscript for publication. EP and LQ are full-time employees of AstraZeneca, and were involved in the study conceptualisation and design, interpretation of results, and writing of the manuscript.
Availability of data and materials
The datasets analysed in this study are available in the Clinical Practice Research Datalink (CPRD), https://www.cprd.com/home/.
Author information
Authors and Affiliations
Contributions
HF, ME, CL, AB, EP and LQ were involved in the study conceptualisation and design, interpretation of results, and writing of the manuscript. PM, DA and HB were involved in the study conceptualisation and design, data analysis, interpretation of results, and writing of the manuscript. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Routinely collected, anonymised electronic health records from the Clinical Practice Research Datalink (CPRD) used as part of this study were provided by the Medicines and Healthcare Products Regulatory Agency (MHRA), an executive agency of the Department of Health & Social Care. This study was approved by the Independent Scientific Advisory Committee for MHRA database research on 15 December 2016 (study protocol 16_223R). Patient consent is covered by the CPRD privacy policy, available at https://www.cprd.com/home/. No other patient-level data were collected as part of this study.
Consent for publication
Not applicable.
Competing interests
HF has received modest research grant funding from AstraZeneca (as principal investigator), and modest expert witness funding from Amgen (as consultant). PM, DA and HB have received significant research grant funding from AstraZeneca in relation to this study. ME declares no conflict of interest. CL has received significant research grant funding from AstraZeneca (awarded to institution), and modest speaker honoraria from Biotronik, Medtronic, Abbot, Novartis and Vifor. AB has received modest advisory honoraria from AstraZeneca in relation to this study. EP and LQ are full-time employees of AstraZeneca.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Table S1. Read and International Classification of Diseases (ICD-10) codes used to define heart failure and chronic kidney disease. Example of the time-updating methodology used during data structuring. Table S2. Incidence of death, major adverse cardiac event and renin-angiotensin-aldosterone system inhibitor discontinuation observed in chronic kidney disease patients, stratified by serum potassium category. Table S3. Model output for final risk equations, re-estimated using patient-intervals restricted to a maximum duration of 30 days. (DOCX 58 kb)
Additional file 2:
Figure S1. Illustrative example of time-updated patient-intervals based on timing of serum potassium measurements. eGFR: estimated glomerular filtration rate; K+: serum potassium; MACE: major adverse cardiac event. (TIF 260 kb)
Additional file 3:
Figure S2. Validation of adjusted incident rate ratios for death (A) and MACE (B) as a function of serum potassium against those published by Luo et al. Black: estimated in the present study (UK CKD stage 3+ patients); grey: estimated by Luo et al. (US CKD stage 3+ patients). Error bars represent 95% confidence intervals. (TIFF 41 kb)
Additional file 4:
Figure S3. Adjusted incident rate ratios for death (A), MACE (B) and RAASi discontinuation (C) as a function of serum potassium in patients stratified by CKD stage. Black: CKD 3a patients; dark grey: CKD 3b patients; mid-grey: CKD 4 patients; light grey: CKD 5 patients. Incident rate ratios were adjusted to account for confounding patient demographics, clinical histories and comorbidities, clinical measurements, and medication usage, as reported in Table 4. CKD: chronic kidney disease; MACE: major adverse cardiac event; RAASi: renin-angiotensin-aldosterone system inhibitor. Error bars represent 95% confidence intervals. (TIFF 63 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Furuland, H., McEwan, P., Evans, M. et al. Serum potassium as a predictor of adverse clinical outcomes in patients with chronic kidney disease: new risk equations using the UK clinical practice research datalink. BMC Nephrol 19, 211 (2018). https://doi.org/10.1186/s12882-018-1007-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-018-1007-1