
Abstract
Background
Multimorbidity is a growing concern for healthcare systems, with many countries experiencing demographic transition to older population profiles. Chronic kidney disease (CKD) is common but often considered in isolation. The extent and prognostic significance of its comorbidities is not well understood. This study aimed to assess the extent and prognostic significance of 11 comorbidities in people with CKD stage 3.
Methods
A prospective cohort of 1741 people with CKD stage 3 was recruited from primary care between August 2008 and March 2010. Participants underwent medical history, clinical assessment, blood and urine sampling. Comorbidity was defined by self-reported doctor-diagnosed condition, disease-specific medication or blood results (hemoglobin), and treatment burden as number of ongoing medications. Logistic regression was used to identify associations with greater treatment burden (taking >5 medications) and greater multimorbidity (3 or more comorbidities). Kaplan Meier plots and multivariate Cox proportional hazards models were used to investigate associations between multimorbidity and all-cause mortality.
Results
One thousand seven hundred forty-one people were recruited, mean age 72.9 +/−9 years. Mean baseline eGFR was 52 ml/min/1.73 m2. Only 78/1741 (4 %) had no comorbidities, 453/1741 (26 %) had one, 508/1741 (29 %) had two and 702/1741 (40 %) had >2. Hypertension was common (88 %), 30 % had ‘painful condition’, 24 % anemia, 23 %, ischaemic heart disease, 17 % diabetes and 12 % thyroid disorders. Median medication use was 5 medications (interquartile range 3–8) and increased with degree of comorbidity. Greater treatment burden and multimorbidity were independently associated with age, smoking, increasing body mass index and decreasing eGFR. Treatment burden was also independently associated with lower education status. After median 3.6 years follow-up, 175/1741 (10 %) died. Greater multimorbidity was independently associated with mortality (hazard ratio 2.81 (95 % confidence intervals 1.72–4.58), p < 0.001) for 3 or more comorbidities vs 0 or 1).
Conclusions
Isolated CKD was rare and multimorbidity the norm in this cohort of people with moderate CKD. Increasing multimorbidity was associated with greater medication burden and poorer survival. CKD management should include consideration of comorbidities.
Similar content being viewed by others

Background
Chronic kidney disease (CKD) is often viewed in isolation and clinical guidelines for the condition commonly focus on the consequences of impaired glomerular function and proteinuria [1, 2]. This approach neglects the reality that the prevalence of CKD rises steeply with age and it is therefore likely to occur in the setting of multiple comorbid conditions including hypertension, diabetes and cardiovascular disease [3]. ‘Multimorbidity’ is usually defined as having two or more chronic morbidities, therefore people with CKD who have one or more comorbidity meet this definition [3]. Comorbidities are important because they may impact on treatment burden, medications management, quality of life, and survival [4–6]. In addition multiple comorbidity and associated polypharmacy have major implications for patients’ capacity to cope with treatment as considered in a ‘burden of treatment model’ [7, 8]. This describes the actions that patients are required to undertake to successfully manage their condition as ‘work’ (both self-management and in interaction with health services) and their ability to respond appropriately as ‘capacity’ [7, 8]. As disease burden increases (due to disease complexity, severity or number of conditions) so does the work required of patients, and their capacity to respond may suffer, leading to poor outcomes as shown in other chronic conditions such as stroke [9].
Optimal clinical management of CKD would therefore benefit from better understanding of the nature, extent and prognostic implications of its common comorbidities in combination. This has been studied to some extent in dialysis populations and comorbidities have been included in risk scores to aid clinical decision making in transplant evaluation in the elderly, but less studied in earlier CKD [10, 11]. In many countries, including the UK, early CKD and its common comorbidities are principally managed in primary care [12]. This study therefore aimed to describe the extent, distribution and survival implications of eleven comorbidities, and the associated medication burden, in a cohort of people with CKD stage 3 in a primary care setting.
Methods
Participants
Participants were recruited from 32 general practitioner surgeries for the Renal Risk in Derby (RRID) study, a prospective cohort study of CKD stage 3 in a primary care setting. Detailed methods for the RRID study have been published elsewhere [13]. Eligible participants were 18 years or over, met the Kidney Disease Outcomes Quality Initiative (KDOQI) criteria for CKD stage 3 (current guidelines at the time of recruitment), able to attend their GP surgery and to give informed consent. People with previous transplant or terminal illness were excluded. Screening and baseline visits were combined due to the large proportion of elderly participants and logistical challenges of conducting study visits in multiple primary care centers. First study visits occurred from August 2008 to March 2010, questionnaire information was checked, anthropomorphic measurements taken, urinalysis performed, and blood specimens taken. All participants provided written informed consent. The study was approved by Nottingham Research Ethics Committee 1 and included on the National Institute for Health Research Clinical Research Portfolio (NIHR Study ID:6632).
Definitions
The eleven comorbidities included in these analyses were hypertension, diabetes, ischaemic heart disease, heart failure, peripheral vascular disease, cerebrovascular disease, chronic respiratory disorder, depression, chronic painful condition, thyroid disorder and anaemia. These comorbidities were chosen for pragmatic reasons including ease of identification from patient report, medication history, and laboratory data, and because they represent a broad spectrum of chronic conditions prevalent among older people.
Participants were asked to list chronic medications on a questionnaire including details of any regular pain medication taken. These were confirmed verbally at study visits and further verified by examination of repeat prescriptions where possible.
Blood pressure was measured after a minimum of five minutes rest in the sitting position, using a validated oscillometric device, recommended by the British Hypertension Society (Digital Blood Pressure Monitor Model UA-767, A & D Instruments Ltd, Abingdon, UK). The same device was used for all readings. BP was calculated as the mean of three readings that differed by <10 %. Hypertension was defined as taking current antihypertensive medication, or systolic BP >140 mmHg or diastolic BP >90 mmHg at baseline. Diabetes was defined by self-report of having a previous clinical diagnosis in line with World Health Organisation criteria or being on medication for diabetes [14]. Ischemic heart disease was defined as participant-reported myocardial infarction or coronary revascularisation procedure. Heart failure was defined as patient reported clinical diagnosis. Peripheral vascular disease was defined as peripheral arterial revascularization or amputation. Cerebrovascular disease was defined as participant-reported stroke or transient ischemic attack. Chronic respiratory disorder was defined by chronic use of inhaled beta-2 adrenergic agonists (either short or long acting) and / or inhaled steroid. The details of all reported comorbidities were checked verbally with participants at study vists. Depression was defined as ongoing use of a selective serotonin reuptake inhibitor or serotonin–norepinephrine reuptake inhibitor. Thyroid disorders were defined by taking thyroxine or carbimazole. Anemia was defined according to Kidney Disease Improving Global Outcomes (KDIGO) guidelines as haemoglobin <13.0 g/dl (<130 g/l) in males and <12.0 g/dl (120 g/l) in females at baseline [1]. Painful condition was defined as ongoing regular analgesia use.
Smoking status was categorized as never smoked, ex-smoker, and current smoker. Socioeconomic status (SES) was defined by two methods. First, using the Indices of Multiple Deprivation score (IMD); a small area social deprivation score comprising a composite measure of seven domains (income, employment, health and disability, education skills and training, barriers to housing and other services, crime and living environment) [15]. Second, using self-reported education status; an important indicator of socioeconomic status in elderly populations [16]. Education status was categorized into three groups (1: no formal qualifications, 2 : school or equivalent qualifications, 3: degree or equivalent). Self-reported ethnicity information was collected and, due to the small number of non-white participants, categorized into ‘White’ and ‘Other’ for analysis. eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKDEPI) equation [17]. Albuminuria was defined as albumin/creatinine ratio (uACR) ≥3 mg/mmol in at least two of the three urine specimens. uACR was fitted as a continuous variable in regression analyses as log of the mean of three uACR values. Body mass index (BMI) was calculated from weight in kilograms divided by height squared in meters [18].
Outcomes
Participants were registered with the Health and Social Care Information Centre to obtain date and cause of death. The observation period was from date of recruitment until 24th February 2013. Cause of death was as recorded on the death certificate. Causes of death were independently reviewed by three investigators and classified as cardiovascular, cancer, infection or other. Classification differences were resolved by discussion.
Statistical analyses
Descriptive statistics were used to summarise the frequency and distribution of the numbers and types of comorbidities and the numbers of medications at baseline. These were described in terms of having isolated CKD, CKD plus one, two, or more than two comorbidities, and taking less than five, more than five, or more than ten medications. Chi square tests were used to compare categorical variables.
Univariate and multivariable logistic regression models were used to identify associations with greater treatment burden (defined as taking more than five medications) and greater multimorbidity (defined as more than two comorbidities). Specific conditions were not included in the treatment burden analysis as several conditions were defined by medication status. A Kaplan Meier plot for all-cause mortality and Cox proportional hazards models were used to describe survival by degree of comorbidity. Cox regression models were developed with multimorbidity fitted as a categorical variable (comparing people with more than two vs. two comorbidities vs none or one) with subsequent addition of sociodemographic (age, sex, education status, IMD) and then lifestyle and clinical variables (smoking, BMI, eGFR, uACR). The final model included variables with a p value < 0.10 on univariate analysis. Proportional hazards assumptions were checked using Nelson–Aalen plots. Interactions between age and smoking, sex and smoking and comorbidity and smoking were checked because of the potential for these factors to modify the mortality effect of smoking [19].
Results
A total of 1741 people were recruited to the RRID study. The study population was predominantly white (>98 %) and elderly. Mean age was 72.9 +/−9 and 67 % were over 70 years. Mean baseline eGFR was 52 ± 10 ml/min/1.73 m2 (911 participants (52.3 %) were CKD stage 3a, 386 participants (22.2 %) were stage 3b). Isolated CKD was uncommon; only 78/1741 (4 %) had no comorbidities in the list considered, 453/1741 (26 %) had at least one comorbidity, 508/1741 (29 %) had two comorbidities of the list considered and 702/1741 (40 %) had more than two comorbidities. At baseline, having three or more comorbidities was more common in men, older people, people with CKD G3b, ex-smokers, and people with greater socioeconomic deprivation, lower educational attainment, higher BMI, or any albuminuria (Table 1). Hypertension was the commonest comorbidity and painful condition the second (Table 2). The median number of medications at baseline was five (interquartile range 3–8); 1033/1741 (59 %) were taking five or more medications and 198/1741 (11 %) ten or more and only 46 (3 %) were taking no medication. Greater comorbidity burden was associated with taking higher numbers of medications (p < 0.001 for trend, Table 1). On multivariable logistic regression, greater treatment burden (taking more than five medications) and greater multimorbidity (three or more comorbidities) were both independently associated with increasing age, smoking, increasing BMI and decreasing eGFR (Table 3). Greater treatment burden was also independently associated with lower education status (Table 3).
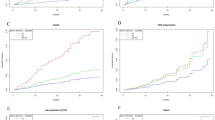
Overall mean follow-up time was 3.6 ± 0.8 years (1317 ± 287 days). 175 participants (10 %) died during follow up and 1537 (90 %) remained alive. Those who died tended to be older, male, have fewer educational qualifications, have a history of smoking, and have CVD and/or diabetes. The commonest cause of death was CVD (41 %) followed by cancer (29 %). People with two or more comorbidities experienced poorer survival (Fig. 1). On univariate Cox regression analyses, male sex, age, history of smoking, lower BMI, lower eGFR, albuminuria, and greater number of comorbidities were associated with increased risk of all-cause mortality (full data not shown). After adjustment for socio-demographic variables, the relationship between number of comorbidities and all-cause mortality was attenuated (from 4.58 (95 % confidence intervals (CI) 2.85–7.38) to 3.15 (95 % I 1.95–5.10, p < 0.001) for three or more compared to one or no comorbidities). Greater number of comorbidities, increasing age, male sex, ex-smoking and lower eGFR remained significantly associated with increased risk of all-cause mortality in the final model (adjusting for age, sex, lifestyle and clinical variables, Table 4). No interactions were identified.

Kaplan Meier plot showing cumulative survival (all-cause mortality) by comorbidity status. Footnote to Fig. 1: Please note that the x axis does not cross the y axis at 0 %
Discussion
In this cohort study of predominantly older people with mild to moderate CKD we found high levels of comorbidity and polypharmacy and demonstrated that increased comorbidity was associated with reduced survival. While our list of included comorbidities was not exhaustive, our findings demonstrate that, even in a cohort recruited in primary care, CKD rarely occurs in isolation. Virtually all patients were ‘multimorbid’ according to the usual definition of having two or more chronic morbidities [3]. Our finding that only 4 % of people with CKD stage 3 had no comorbidity is striking and clinically important.
Strengths and limitations
This study had several strengths, including large numbers of people with CKD, being conducted in a primary care setting, ascertainment of a broad range of comorbidities by interview rather than routine data, and prospective follow-up. However, we recognise important limitations. We did not have an age-matched control group without CKD with whom to compare multimorbidity burden. It is also likely that we under-identified some comorbidities by use of patient self-report (such as heart failure) and medication-definition; depression and respiratory disorders, for example, were defined by medication only, thus reducing their prevalence in our study. We were unable to include certain important CKD comorbidities such as cancer and liver disease because people with terminal illness were excluded and, although participants were asked about co-exisiting conditions, specific questions about all forms of cancer were not included in the baseline questionnaire. In addition, the prevalence of patient-reported liver disease was considered too low to meaningfully include in analyses and thought likely to be under-ascertained by patient self-report as largely asymptomatic (data not shown). The use of a medication-driven definition will, to some extent, be a reflection of the ‘work’ patients are required to do in managing a condition, but defining conditions by medication meant that we were unable to include them as variables in our logistic regression models. This reduced our ability to examine whether medication burden had greatest association with specific conditions. There is also no agreed method of defining morbidities. We considered causative factors and potential CKD complications if they affected quality life per se or treatment burden through their management, and or prognosis. Anaemia and hypertension were included for these reasons. We did not include obesity as this is largely asymptomatic, though we recognise that following lifestyle advice maybe burdensome and symptoms may develop as obesity increases. Including obesity as an additional comorbidity would have increased overall burden. These uncertainties would benefit from further discussion and consensus in people with CKD [20].
We were unable to consider frailty (which has been shown to be associated with CKD) or cognitive impairment both of which may influence patient capacity and outcome, or other outcomes such as quality of life (which might be more sensitive to some of our morbidities than mortality), this will be assessed in later follow up stages of this cohort [21–23]. Similarly, our assessment of comorbidities does not account for disease severity. Conditions causing pain, such as osteoarthritis, were not identified individually. Participants volunteered for this study, so we may have selected a population with less comorbidity and lower frailty. We also had no data on the burden of health care (such as clinic visits) or medication adherence. The combined effects of these limitations is that even the high prevalence of comorbidities that we have reported is likely to be an underestimate.
Comparison with existing literature
The debate regarding the relevance of early or mild CKD has often focussed on the hypothetical person with reduced GFR and no other medical problems but our data show that this combination is only present in a very small minority [24]. In the majority, CKD was associated with other medical problems and 40 % had more than two comorbidities. Multiple studies have shown that the presence of CKD increases the risk of adverse outcomes associated with a wide range of other diseases and, as we have shown, greater comorbidity is associated with increased all-cause mortality even in mild to moderate CKD [25–28]. In a historical prospective cohort study of people with CKD identified from electronic patient records, Gullion et al. identified that, compared to age and sex matched controls without CKD, people with CKD had higher levels of comorbidity and higher risk of mortality for the same degree of comorbidity [29]. Thus there is mutual amplification of risks associated with CKD and comorbid conditions. Taken together these observations imply that it is important to consider the implications of CKD for the integrated care of patients with multimorbidity. The presence of multiple comorbid conditions has important implications for medicines management [30]. We identified very high prevalence of polypharmacy with 59 % of people taking five or more medications and 11 % taking ten or more. Furthermore, perhaps unsurprisingly, a greater number of comorbidities was associated with a greater number of medications. We showed that taking more than five medications was independently associated with older age and lower education status. Many commonly used medications require dose adjustments for reduced GFR and polypharmacy is associated with increased risk of adverse drug interactions and risk of acute kidney injury [31]. As the majority of patients with CKD are elderly and more susceptible to adverse drug effects, our data suggest that careful medicines management (including coordination between pharmacists and community and hospital physicians) should form an important part of the care of people with CKD.
Burden of treatment is a relatively under-studied consideration in CKD, the more common focus being burden of illness [32–34]. The cumulative complexity of developing new comorbidities and the balance of work and capacity have implications for the success of self- and shared-management efforts, increasingly recognised in other chronic conditions such as stroke and heart failure [9, 35, 36]. The burden of comorbidities is usually higher in groups with lower socioeconomic status and/or lower educational attainment as we have shown in this cohort [3]. Lower socioeconomic status is also linked to lower health literacy - a key component of patients’ capacity [37]. An unexpected but important finding of our study was the high prevalence of certain conditions in this population, for example ‘painful condition’ and depression, though both were probably underestimated in our study due to reliance on medication for their definition. Both may also adversely influence capacity and are common in older people in general population studies in the UK [38, 39]. Thus our data confirm that mild CKD is associated with high disease burden, high treatment burden and reduced capacity to cope with the demands of treatment. These factors should be considered when developing and agreeing care plans for people with CKD.
Implications for research and practice
A patient-centred approach to managing patients with multimorbidity (such as that recommended by the American Geriatrics Society) is in line with evidence that risks of fragmentation of care and medical error related to multimorbidity can be ameliorated by a dedicated clinician acting in an overseeing role [40–42]. Generalists in integrated primary care teams are usually best placed to offer this continuity of care and clinical oversight in mild to moderate CKD though, as CKD advances, nephrologists commonly adopt this role. Improving care coordination has the potential to improve outcomes and reduce health care costs for people with multimorbidity. This includes improving medicines management as discussed above. Informed decision-making is challenging in multimorbidity and there is need to be judicious in adding to patients’ treatment burden, particularly for treatments that do not relieve symptoms but reduce future risk. This may be particularly important in older patients with CKD, whom we have shown have a high prevalence of comorbidities and reduced capacity.
We were unable to describe severity of the comorbid conditions or quality of life in this study, which represent important considerations for future research. There are also implications of the high prevalence of comorbidities to clinical trial design in people with CKD (where people with comorbidities may be excluded from trials). Further research should also investigate to what extent comorbidities may be caused or exacerbated by CKD (e.g. anaemia).
Conclusions
In this cohort of people with moderate CKD, we identified that isolated CKD was rare and multimorbidity the norm. Polypharmacy as a measure of treatment burden was common, linked to degree of comorbidity and associated with older age and lower education status. Survival was independently associated with greater number of comorbidities. Integrated care for people with CKD should go beyond a focus on reduced GFR or albuminuria and include consideration of the burden of comorbidities (and their treatments) balanced against patient capacity to cope with further investigation and treatment.
Meetings
This (or similar data from this study) was presented as a poster at the American Society of Nephrology Kidney Week Conference, Philadelphia, November 2014.
It was also presented at the British Society of Nephrology conference, Leeds, UK July 2015 and as a poster at the European Renal Association congress, London, UK, May 2015.
Change history
21 December 2020
An amendment to this paper has been published and can be accessed via the original article.
Abbreviations
- CKD:
-
Chronic kidney disease
- RRID:
-
Renal Risk in Derby (study)
- NHS:
-
National Health Service
- uACR:
-
Urinary albumin to creatinine ratio
- eGFR:
-
Estimated glomerular filtration rate
- AKI:
-
Acute kidney injury
- RAASi:
-
Renin-angiotensin aldosterone system inhibitors
- CVD:
-
Cardiovascular disease
- NICE:
-
National Institute for Health and Care Excellence
- IMD:
-
Index of Multiple Deprivation
- GP:
-
General practitioner
- BP:
-
Blood pressure
- SES:
-
Socioeconomic status
- KDOQI:
-
Kidney Disease Outcomes Quality Initiative
- KDIGO:
-
Kidney Disease Improving Global Outcomes
References
KDIGO. 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):150.
National Institute for Health and Clinical Excellence guideline 182; Chronic kidney disease: early identification and management of chronic kidney disease in adults in primary and secondary care. London, National Institute of Health and Care Excellence, 2014.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43.
Mahmoodi BK, Matsushita K, Woodward M, Blankestijn PJ, Cirillo M, Ohkubo T, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: a meta-analysis. Lancet. 2012;380:1649–61.
Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJ, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet. 2012;380:1662–73.
Jesky M, Lambert A, Burden AC, Cockwell P. The impact of chronic kidney disease and cardiovascular comorbidity on mortality in a multiethnic population: a retrospective cohort study. BMJ Open. 2013;3:e003458.
May CR, Eton DT, Boehmer K, Gallacher K, Hunt K, MacDonald S, et al. Rethinking the patient: using burden of treatment theory to understand the changing dynamics of illness. BMC Health Serv Res. 2014;14:281.
Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. 2012;65:1041–51.
Gallacher KI, Batty GD, McLean G, Mercer SW, Guthrie B, May CR, et al. Stroke, multimorbidity and polypharmacy in a nationally representative sample of 1,424,378 patients in Scotland: implications for treatment burden. BMC Med. 2014;12:151.
Dusseux E, Albano L, Fafin C, Hourmant M, Guérin O, Couchoud C, et al. A simple clinical tool to inform the decision-making process to refer elderly incident dialysis patients for kidney transplant evaluation. Kidney Int. 2015;88(1):121–9.
Miskulin D, Bragg-Gresham J, Gillespie BW, Tentori F, Pisoni RL, Tighiouart H, et al. Key comorbid conditions that are predictive of survival among hemodialysis patients. Clin J Am Soc Nephrol. 2009;4(11):1818–26.
Stevens PE, de Lusignan S, Farmer CK, Tomson CR. Engaging primary care in CKD initiatives: the UK experience. Nephrol Dial Transplant. 2012;27 Suppl 3:S5–11.
McIntyre NJ, Fluck RJ, McIntyre CW, Taal MW. Skin autofluorescence and the association with renal and cardiovascular risk factors in chronic kidney disease stage 3. Clin J Am Soc Nephrol. 2011;6:2356–63.
The World Health Organization and International Diabetes Federation. The Definition and Diagnosis of Diabetes Mellitus and Intermediate Glycaemia. WHO Press. World Health Organisation, Geneva, Switzerland 2006.
Jordan H, Roderick P, Martin D. The index of multiple deprivation 2000 and accessibility effects on health. J Epidemiol Community Health. 2004;58:250–7.
Grundy E, Holt G. The socioeconomic status of older adults: how should we measure it in studies of health inequalities? J Epidemiol Community Health. 2001;55:895–904.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro 3rd AF, Feldman HI, et al. A new equation to estimate Glomerular Filtration Rate. Ann Intern Med. 2009;150:604–12.
Pinto-Sietsma SJ, Navis G, Janssen WMT, de Zeeuw D, Gans RO, de Jong PE, et al. A central body fat distribution is related to renal function impairment, even in lean subjects. Am J Kidney Dis. 2003;41:733–41.
Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1519.
van Nooten FE, Green J, Brown R, Finkelstein FO, Wish J. Burden of illness for patients with non-dialysis chronic kidney disease and anemia in the United States: review of the literature. J Med Econ. 2010;13:241–56.
Khan IH. Comorbidity: the major challenge for survival and quality of life in end-stage renal disease. Nephrol Dial Transplant. 1998;13 suppl 1:76–9.
Hailpern SM, Melamed ML, Cohen HW, Hostetter TH. Moderate chronic kidney disease and cognitive function in adults 20 to 59 years of age: Third National Health and Nutrition Examination Survey (NHANES III). J Am Soc Nephrol. 2007;18:2205–13.
Walker SR, Gill K, Macdonald K, Komenda P, Rigatto C, Sood MM, et al. Association of frailty and physical function in patients with non-dialysis CKD: a systematic review. BMC Nephrol. 2013;14:228.
Winearls CG, Glassock RJ. Dissecting and refining the staging of chronic kidney disease. Kidney Int. 2009;75:1009–14.
Gansevoort RT, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80(1):93–104.
Go AS, Chertow GM, Fan DJ, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305.
Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF, Hoogwerf B, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA. 2001;286:421–6.
Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–81.
Gullion CM, Keith DS, Nichols GA, Smith DH. Impact of comorbidities on mortality in managed care patients with CKD. Am J Kidney Dis. 2006;48:212–20.
St Peter WL, Wazny LD, Patel UD. New models of chronic kidney disease care including pharmacists: improving medication reconciliation and medication management. Curr Opin Nephrol Hypertens. 2013;22(6):656–62.
Chang YP, Huang SK, Tao P, Chien CW. A population-based study on the association between acute renal failure (ARF) and the duration of polypharmacy. BMC Nephrol. 2012;13:96.
de Lissovoy G. Measuring the burden of illness for end-stage renal disease: some heavy lifting required. Kidney Int. 2007;72:1045–7.
Jassal SV, Watson D. Dialysis in late life: benefit or burden. Clin J Am Soc Nephrol. 2009;4:2008–12.
Mansilla Francisco JJ, Díez De los Ríos Cuenca F, Cabrera Azaña S, Cortés Torres J, Macías López MJ, González Castillo JA, et al. Impact of incident comorbidity on functional loss in elderly chronic kidney disease patients undergoing hemodialysis. CANNT J. 2012;22:25–9.
Gallacher K, Morrison D, Jani B, Macdonald S, May CR, Montori VM, et al. Uncovering treatment burden as a key concept for stroke care: a systematic review of qualitative research. PLoS Med. 2013;10:e1001473.
Mair FS, May CR. Thinking about the burden of treatment. BMJ. 2014;349:g6680.
Fraser SD, Roderick PJ, Casey M, Taal MW, Yuen HM, Nutbeam D. Prevalence and associations of limited health literacy in chronic kidney disease: a systematic review. Nephrol Dial Transplant. 2013;28:129–37.
Singleton N, Bumpstead R, O’Brien M, Lee A, Meltzer H. Psychiatric morbidity among adults living in private households. Int Rev Psychiatry. 2003;15:65–73.
Health Survey for England - 2011. Health, social care and lifestyles. London: Health and Social Care Information Centre; 2012.
Hughes LD, McMurdo ME, Guthrie B. Guidelines for people not for diseases: the challenges of applying UK clinical guidelines to people with multimorbidity. Age Ageing. 2013;42(1):62–9.
Boyd CM, McNabney MK, Brandt N, Correa-de-Araujuo R, Daniel KM, Epplin J, et al. Guiding principles for the care of older adults with multimorbidity: an approach for clinicians: American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. J Am Geriatr Soc. 2008;60:E1–E25.
Guthrie B, Saultz JW, Freeman GK, Haggerty JL. Continuity of care matters. BMJ. 2008;337:a867.
Acknowledgements
The authors would like to thank the collaborating GP practices and their staff.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no financial or non-financial competing interests. The results presented in this paper have not been published previously in whole or part, except in abstract format. The Renal Risk in Derby Study was supported by a fellowship grant from Kidney Research UK and the British Renal Society, as well as an unrestricted educational grant from Roche Products plc and a Project Grant from The Dunhill Medical Trust (R302/0713). The study sponsors did not have any role in study design or collection, analysis and interpretation of data, writing the report, or the decision to submit for publication.
Authors’ contributions
SF: design of these analyses, statistical analyses, paper drafting and review. PR: design of these analyses, critical manuscript review. CM: critical manuscript review, expertise on multimorbidity, treatment burden and capacity. NM: data collection and initial analysis. CM, RF, MT: RRID study research development and implementation, critical manuscript review, expert CKD knowledge. AS: data collection (comorbidities). Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Fraser, S.D.S., Roderick, P.J., May, C.R. et al. The burden of comorbidity in people with chronic kidney disease stage 3: a cohort study. BMC Nephrol 16, 193 (2015). https://doi.org/10.1186/s12882-015-0189-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-015-0189-z