
Abstract
Background
Aortic valve area (AVA) estimation in patients with aortic stenosis may be obtained using several methods. This study was undertaken to verify the cardiovascular magnetic resonance (CMR) planimetry of aortic stenosis by comparing the findings with invasive catheterization, transthoracic (TTE) as well as tranesophageal echocardiography (TEE) and anatomic CMR examination of autopsy specimens.
Methods
Our study was performed in eight patients with aortic valve stenosis. Aortic stenosis was determined by TTE and TEE as well as catheterization and CMR. Especially, after aortic valve replacement, the explanted aortic valves were examined again with CMR ex vivo model.
Results
The mean AVA determined in vivo by CMR was 0.75 ± 0.09 cm2 and ex vivo by CMR was 0.65 ± 0.09 cm2 and was closely correlated (r = 0.91, p < 0.001). The mean absolute difference between AVA derived by CMR ex vivo and in vivo was −0.10 ± 0.04 cm2. The mean AVA using TTE was 0.69 ± 0.07 with a significant correlation between CMR ex vivo (r = 0.85, p < 0.007) and CMR in vivo (r = 0.86, p < 0.008). CMR ex vivo and in vivo had no significant correlation with AVA using Gorlin formula by invasive catheterization or using planimetry by TEE.
Conclusion
In this small study using an ex vivo aortic valve stenosis model, the aortic valve area can be reliably planimetered by CMR in vivo and ex vivo with a well correlation between geometric AVA by CMR and the effective AVA calculated by TTE.
Similar content being viewed by others


Background
Aortic valve stenosis is the most common cardiac valve disease resulting in valve therapy [1]. Exact determination of the severity of stenosis is essential to guide therapy [2]. Standard methods, such as cardiac catheterization and transthoracic echocardiography (TTE) have to calculate the effective orifice area by measurement of the transvalvular pressure gradient [3,4], as they do not allow a direct and precise measurement of the geometric orifice area. Therefore it seems desirable to directly determine the geometric orifice area by a flow independent technique such as planimetry. Several cardiologists take the view that TTE using the Doppler-technique is now the best reference (“gold standard”) whereas the Gorlin-formula is the historical reference.
Cardiovascular magnetic resonance (CMR) is a noninvasive method that allows visualization of cardiac function, structure and valves [5,6]. Recently, we and others have reported the success of planimetry by CMR in aortic valve [7–14].
However, to date, no studies have been published describing ex vivo CMR stenotic aortic valves. It therefore seemed useful to compare anatomic data with CMR imaging.
We hypothesized that direct planimetry of the stenotic aortic valve in an autopsy human valve as a standard of reference using CMR corresponds to the planimetry of the stenotic aortic valve in vivo using CMR. To address this hypothesis, we performed a head-to-head comparison between aortic valve area (AVA) planimetry preoperatively by CMR and postoperatively of the explanted aortic valve by CMR in a series of eight patients with aortic valve stenosis. In addition, CMR measurements were compared with TTE and transesophageal echocardiography (TEE) as well as catheterization data
Methods
Patients
Eight patients referred to our institution for evaluation of aortic valve stenosis and were prospectively included in the study undergoing aortic valve replacement. All diagnostic procedures and measurements were performed by experienced observers, who were blinded to the results of the other imaging modalities. Informed consent was obtained in all patients. The study approved by local ethics committee of the Universität Regensburg.
Clinical characteristics of the patients
Clinical data of the eight patients are summarized in Table 1. Mean age was 76 ± 6 (62 to 82) years. The majority of patients presented with clinical symptoms of severe aortic stenosis, such as systolic murmur, dyspnea, chest pain or syncope. Concomitant aortic regurgitation was present in 5 patients and was defined as mild/trivial (n = 4) or moderate (n = 1) by CMR and echocardiography. TEE planimetry of AVA was not possible in one patient because of heavy calcifications. Planimetry of AVA was possible in all patients undergoing CMR. An impaired image quality was observed in one patient due to trigger problems by cardiac arrhythmia.
Transthoracic echocardiography
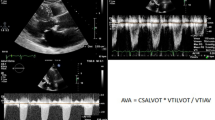
Standardized transthoracic echocardiography was performed with measurements of the left ventricular outflow tract diameter, the velocity of across the aortic valve and flow data of the left ventricular outflow tract to calculate the AVA using the continuity equation [15].
Transesophageal Echocardiography
Multiplane TEE was performed using a 5-Mhz annular phased array probe. For examination of the aortic valve, the imaging plane was rotated from 0° to 180° until the best image of the aortic valve opening in the short axis view was obtained (usually around 60°). Minimal probe manipulation was performed to ensure that the smallest orifice of the aortic valve at the leaflet tips was identified. Planimetry of the smallest orifice at the time of maximum opening in early systole (triggered by the electrocardiogram) was performed. At least three consecutive measurements were averaged.
Catheterization
A standard cardiac catheterization procedure was performed via the percutaneous femoral approach, including right and left heart pressure measurement. Peak to peak and mean pressure gradients were determined between left ventricle and ascending aorta. Cardiac output was measured by thermodilution, averaging at least 3 measurements. AVA was estimated using the Gorlin formula [16].
Surgery and autopsy
The description of the aortic valve was obtained from one surgeon. We obtained human valves from patients with aortic valve stenosis at the time of surgical valve replacement. Despite the heavy calcification, all valves could be explanted totally. Specimens were originally preserved in formaldehyde solution.
Cardiovascular magnetic resonance studies – in vivo
All patient studies were performed on a 1.5 T scanner (Sonata, Siemens Medical Solutions, Erlangen, Germany). CMR studies were performed in supine position with a phased-array receiver coil and breath-hold acquisitions prospectively gated to the ECG. Cine images were acquired in multiple short axis and long axis views with fast imaging with steady state free precession (trueFISP, slice thickness 8 mm, echo time 1.53 ms, readout bandwidth 1.085 Hz/pixel, repetition time 3.14 ms, matrix 256*202).
Image analysis was performed off-line using the semiautomatic ARGUS evaluation program (Siemens Medical Solutions, Erlangen, Germany), which is a part of the commercially available cardiac package of the scanner software.
The imaging plane of the aortic valve was defined by acquiring a systolic 5-chamber view parallel to the long axis of the left ventricular outflow tract and a long axis view of the left ventricular outflow tract and the proximal aorta, perpendicular to the 5-chamber view, as described previously [7]. In brief, the subsequent slices were defined parallel to the valvular plane and, additionally, in cases of orifices with an eccentric outlet, perpendicularly to the direction of the jet. At least 4 slices (range 4–7) at different levels of the aortic valve were acquired and the imaging plane with the smallest orifice was chosen. Planimetry of the smallest orifice at the time of maximum opening in early systole in the acquisitions prospectively triggered to the electrocardiogram was performed by two independent observers, who were unaware of the echocardiographic, catheterization and ex vivo results. We placed our traces at the point of the bright pixels. Three measurements were performed and average for calculating the AVA. Intraobserver and interobserver variabilities regarding AVA were 3 % and 6 % for in vivo CMR, respectively.
Cardiovascular magnetic resonance studies – ex vivo
All specimens were examined on a 1.5 T scanner (Magnetom Sonata, Siemens Medical Solutions, Erlangen, Germany). The CMR imaging protocol included a 3D-CISS protocol (TR/TE/flip angle 17/8.08 ms/70° ms, band width 130 Hz/pixel, effective slice thickness 1 mm pixel size 0.6 × 0.45 mm). The aortic valve was placed on a rack into a water container. Then the container with the aortic valve was placed in the gantry. Slices in the orthogonal planes (transverse, coronal and sagittal) were obtained (Fig. 1). Serial angulated-axis views from the base to tip of the valve were acquired with 3D sequence (Fig. 2). Planimetry of the smallest orifice was performed by two independent observers, who were unaware of the echocardiographic, catheterization and in vivo results. We placed our traces at the edge of the bright pixels. Three measurements were performed and average for calculating the AVA. Intraobserver and interobserver variabilities were 1 % and 4 % for ex vivo CMR, respectively.

Position of the ex vivo aortic valve fixed in a water container and planning the slices. a, overview; b, coronar view; c, angulation for planning the orthograd view; d, the resulting orthograd view

To avoid assessing the aortic valve area beyond or above the leaflet tips, the imaging plane was moved shift wise in one mm steps in an orthograd direction. Planimetry was chosen on the slice where the smallest orifice was surrounded totally by the edge of the valve

Images derived from the in vivo CMR (a), from the aortic valve specimen (b) and from the ex vivo CMR (c) in a bicuspid stenotic valve (top) and in a tricuspid stenotic valve (bottom)
Statistical analysis
Data expressed as mean ± standard deviation. Linear regression analysis was performed to describe correlations between the different techniques. The mean AVA of the different techniques was compared by student's t-Test for paired samples. Intra- and interobserver variability (n = 8) were expressed as the percentage of variability (absolute value of the difference between 2 measurements divided by the mean of 2 measurements). Agreement between the different techniques was assessed as described by Bland and Altman. A level of significance of below 0.05 was defined as statistically significant. SPSS version 21 (SPSS Institute, Chicago) was used for statistical analysis.
Results
CMR planimetry of AVA in vivo and ex vivo
The measurements of all patients by the various modalities are depicted in Table 2. Six valves were tricuspid and two valves were bicuspid. Images of aortic valve specimen, in vivo and ex vivo CMR are depicted in Fig 3.
The mean AVA determined ex vivo by CMR was 0.65 ± 0.09 cm2. Mean AVA determined in vivo by CMR was 0.75 ± 0.09 cm2. The mean absolute difference between AVA derived by CMR ex vivo and in vivo was 0.10 ± 0.04 cm2 (p < 0.001, Fig. 4 and Table 3 ). The AVA in vivo and ex vivo by CMR was closely correlated (r = 0.91, p < 0.001).

Agreement between aortic valve area assessed by CMR in vivo and by CMR ex vivo (a). According to Bland-Altman (b), the difference between the two comparative measurements is plotted against their mean. The continuous line represents the mean difference and dashed lines represent the limits of agreement (mean difference ± 2SD)
The mean absolute difference between AVA derived by CMR ex vivo and calculated using the continuity equation by TTE was −0.04 ± 0.05 cm2 (p = 0.066). The mean absolute difference between AVA derived by CMR in vivo and calculated using the continuity equation by TTE was +0.07 ± 0.04 cm2. In linear regression analysis the correlation between CMR ex vivo and TTE (r = 0.85, p < 0.007) was similar to that between CMR in vivo and TTE (r = 0.86, p < 0.008).
The mean absolute difference between aortic valve area derived by CMR ex vivo and TEE was +0.12 ± 0.09 cm2 (p = 0.012). The mean absolute difference between aortic valve area derived by CMR in vivo and TEE was −0.02 ± 0.10 cm2 (p = 0.75). In linear regression analysis the correlation between CMR ex vivo and TEE was r = 0.44, p = 0.323) and between CMR in vivo and TEE r = 0.28, p = 0.551.
The mean absolute difference between AVA derived by CMR ex vivo and calculated using the Gorlin formula by catheterization was +0.07 ± 0.26 cm2 (p = 0.498). The mean absolute difference between AVA derived by CMR in vivo and calculated using the Gorlin formula by catheterization was +0.17 ± 0.27 cm2 (p = 0.117). In linear regression analysis the correlation between CMR ex vivo and Gorlin formula by catheterization was r = 0.09, p = 0.835 and between CMR in vivo and Gorlin formula by catheterization was r = −0.03, p = 0.952.
AVA with other methods
The mean of the aortic valve area calculated using the Gorlin formula by catheterization was 0.60 ± 0.27 cm2. The mean aortic valve area determined by TEE was 0.79 ± 0.15 cm2. The mean of the aortic valve area calculated by TTE was 0.69 ± 0.07 (Table 3).
The mean absolute difference between AVA derived calculated using the Gorlin formula by catheterization and calculated using the continuity equation by TTE was −0.11 ± 0.25 cm2 (p = 0.278). The mean absolute difference between AVA using the Gorlin formula by catheterization and TEE was −0.13 ± 0.19 cm2 (p = 0.122). The mean absolute difference between AVA calculated using the continuity equation by TTE and TEE was −0.08 ± 0.10 cm2 (p = 0.97). In linear regression analysis the correlation between Gorlin formula by catheterization and TEE was r = 0.71, p = 0.073 and between Gorlin formula by catheterization and the continuity equation by TTE was r = 0.17, p = 0.639 and between TEE and catheterization and the continuity equation by TTE was r = 0.15, p = 0.748.
Discussion
The results of this study demonstrate that aortic valve stenosis can be accurately planimetered by using CMR in vivo compared with ex vivo model. Precise assessment of aortic valve area in aortic stenosis is crucial for optimal patient treatment [17]. However, no comparison of planimetry of the aortic valve area has made with in vivo and ex vivo aortic valves by CMR or other modality. The present study is the first to validate the ability of CMR to accurately and precisely planimetry aortic valve stenosis in vivo comparing by ex vivo CMR.
Characterization of the severity of aortic stenosis is among the most difficult problems in valvular heart disease. Exact determination of the severity of stenosis is essential to guide therapy [18]. In evaluating the severity of the aortic valve stenosis, it is ideally desirable to determine geometric orifice area On the other hand, the opening of the aortic valve is though highly dependent of the flow and gradient. Because planimetry only provides geometric orifice area and does not characterize the flow property, this could be a challenge in low-flow/low-gradient aortic stenosis [19–21]. The guidelines allow various methods to determine the AVA. However, the different available techniques often might lead to discrepancy results. This could demonstrate in the current study and previous studies which show that the planimtery of the AVA was systematically higher than the calculated AVA by Gorlin in catheterization or continuity equation in TTE. This is due to the fact that direct planimetry reflects the anatomical orifice while the calculated valve area reflects the effective orifice area. Despite the different available techniques for the assessment of the AVA all available techniques have their limitations and this should be keep in mind. In TTE, the inexact measurement of the diameter of the left ventricular outflow tract or missed peak transvalvular velocity might lead to a false AVA. In TEE, heavily calcification of the aortic valve could lead to impaired image quality e.g. by the acoustic shadowing, thus exact delineation of the cusps and planimetry of the AVA are impossible or the potential inability to identify the accurate imaging plane for planimetry. Hemodynamic assessment of the aortic valve area by invasive cardiac catheterization has often been challenged because of potential imprecision introduced by the hemodynamic parameters. Finally, CMR has its limitation in valve motion and exact slice orientation or in contraindication for CMR (e.g. claustrophia or metallic implants).
Prior to our study, several other investigators have determined the accuracy of several methods for CMR and cardiac computed tomography planimetry of the aortic valve using an angiographic reference standard or Doppler derived data [7–9,22,23]. However, the ultimate test of the value of the method seems to be comparison with anatomy. The current study extends these findings as it demonstrates that CMR allows to accurately visualizing the anatomic valve area in vivo compared to ex vivo.
To date, most CMR studies for the quantification of stenotic aortic valves have focused on direct planimetry [24], although the dimensions of CMR voxels relative to the size and shape of stenotic orifices sometimes influence this approach. Therefore, an ex vivostudy was deemed as an essential intermediate study for assessing sources of errors in CMR aortic valve estimation prior to in vivo experiments. Ex vivo estimates eliminate errors due to motion blurring, which includes errors resulting from irregular heart rates and images acquired during motion. Furthermore, ex vivo determinations also minimize uncertainties due to edge definition and produced high-contrast edges in which the aortic valve boundary is defined to be pixel values above background. The results of this study should, therefore, be interpreted as the minimum errors which can be achieved using CMR.
Despite the close correlation between ex vivo and in vivo planimetry by CMR, we observed an underestimation of the aortic valve area by CMR ex vivo. The underlying reason for underestimation of the aortic valve area by CMR may be related to valve motion and slice orientation. Specifically, transplanar valve motion during systole might lead to overestimation of valve area when the imaging plane misses the smallest orifice area. Taking measurement from CMR, one has to make sure that the plane is orthogonal and on the edge of the leaflets. Ex vivo imaging, however, eliminates potential errors caused by cardiac and respiratory motion.
Limitations
Several limitations of our study should be noted. The sample size of the current study was small. Most of the patients had been diagnosed with high-grade aortic valve stenosis, resulting in a selection bias. However, because we decided to use combined left and right heart catheterization and study the explanted aortic valve, we were unable to include patients with mild aortic stenosis, because, in these patients these would not be justified. Furthermore, only the static area of the aortic valve was measured and do not reflect the hemodynamic conditions in vivo. However, it is difficult to assess the dynamic change of stenotic aortic valve area in ex vivo specimens. In this study only due to the heavy calcification of the aortic valve, it was possible to explant the valve as a unit and we presume that the shape of the valve represent the maximum opening of the valve in systole. Consequently, the aortic valve area of the explanted aortic valve corresponds by the calcification the smallest maximal orifice may merely influenced by ejection and diastolic valve closing.
Conclusion
In conclusion, this is the first study to validate planimetry in aortic valve stenosis using CMR in an ex vivo model. CMR in vivo slightly overestimates the valve area in aortic stenosis compared to CMR ex vivo. Furthermore, planimetry of AVA using CMR in vivo and ex vivo model correlated well with calculated AVA by TTE, in contrast to TEE and invasive measurements of AVA. These certain methodical discrepancies between these methods must be taken into account when grading the severity of aortic stenosis by AVA.
Abbreviations
- AVA:
-
Aortic valve area
- CMR:
-
Cardiac magnetic resonance
- TEE:
-
Transoseophageal echocardiography
References
Selzer A. Changing aspects of the natural history of valvular aortic stenosis. N Engl J Med. 1987;317:91–8.
Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, et al. Guidelines on the management of valvular heart disease (version 2012): The joint task force on the management of valvular heart disease of the european society of cardiology (esc) and the european association for cardio-thoracic surgery (eacts). Eur J Cardiothorac Surg. 2012;42:S1–44.
Leborgne L, Tribouilloy C, Otmani A, Peltier M, Rey JL, Lesbre JP. Comparative value of doppler echocardiography and cardiac catheterization in the decision to operate on patients with aortic stenosis. Int J Cardiol. 1998;65:163–8.
Garcia D, Dumesnil JG, Durand LG, Kadem L, Pibarot P. Discrepancies between catheter and doppler estimates of valve effective orifice area can be predicted from the pressure recovery phenomenon: Practical implications with regard to quantification of aortic stenosis severity. J Am Coll Cardiol. 2003;41:435–42.
Schmidt M, Crnac J, Dederichs B, Theissen P, Schicha H, Sechtem U. Magnetic resonance imaging in valvular heart disease. Int J Card Imaging. 1997;13:219–31.
Lee SC, Ko SM, Song MG, Shin JK, Chee HK, Hwang HK. Morphological assessment of the aortic valve using coronary computed tomography angiography, cardiovascular magnetic resonance, and transthoracic echocardiography: Comparison with intraoperative findings. Int J Cardiovasc Imaging. 2012;28 Suppl 1:33–44.
Debl K, Djavidani B, Seitz J, Nitz W, Schmid FX, Muders F, et al. Planimetry of aortic valve area in aortic stenosis by magnetic resonance imaging. Invest Radiol. 2005;40:631–6.
John AS, Dill T, Brandt RR, Rau M, Ricken W, Bachmann G, et al. Magnetic resonance to assess the aortic valve area in aortic stenosis: How does it compare to current diagnostic standards? J Am Coll Cardiol. 2003;42:519–26.
Friedrich MG, Schulz-Menger J, Poetsch T, Pilz B, Uhlich F, Dietz R. Quantification of valvular aortic stenosis by magnetic resonance imaging. Am Heart J. 2002;144:329–34.
Kupfahl C, Honold M, Meinhardt G, Vogelsberg H, Wagner A, Mahrholdt H, et al. Evaluation of aortic stenosis by cardiovascular magnetic resonance imaging: Comparison with established routine clinical techniques. Heart. 2004;90:893–901.
Garcia J, Pibarot P, Capoulade R, Le Ven F, Kadem L, Larose E. Usefulness of cardiovascular magnetic resonance imaging for the evaluation of valve opening and closing kinetics in aortic stenosis. Eur Heart J Cardiovasc Imaging. 2013;14:819–26.
von Knobelsdorff-Brenkenhoff F, Rudolph A, Wassmuth R, Bohl S, Buschmann EE, Abdel-Aty H, et al. Feasibility of cardiovascular magnetic resonance to assess the orifice area of aortic bioprostheses. Circ Cardiovasc Imaging. 2009;2:397–404. 392 p following 404.
Buchner S, Hulsmann M, Poschenrieder F, Hamer OW, Fellner C, Kobuch R, et al. Variable phenotypes of bicuspid aortic valve disease: Classification by cardiovascular magnetic resonance. Heart. 2010;96:1233–40.
Buchner S, Debl K, Haimerl J, Djavidani B, Poschenrieder F, Feuerbach S, et al. Electrocardiographic diagnosis of left ventricular hypertrophy in aortic valve disease: Evaluation of ecg criteria by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2009;11:18.
Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: Eae/ase recommendations for clinical practice. Eur J Echocardiogr. 2009;10:1–25.
Gorlin R, Gorlin SG. Hydraulic formula for calculation of the area of the stenotic mitral valve, other cardiac valves, and central circulatory shunts. I Am Heart J. 1951;41:1–29.
Baumgartner H. Aortic stenosis: medical and surgical management. Heart. 2005; 91(11):1483–1488.
Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33:2451–96.
Minners J, Allgeier M, Gohlke-Baerwolf C, Kienzle RP, Neumann FJ, Jander N. Inconsistencies of echocardiographic criteria for the grading of aortic valve stenosis. European Heart Journal. 2008;29:1043–8.
Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation. 2007;115:2856–64.
Jander N, Minners J, Holme I, Gerdts E, Boman K, Brudi P, et al. Outcome of patients with low-gradient "severe" aortic stenosis and preserved ejection fraction. Circulation. 2011;123:887–95.
Feuchtner GM, Muller S, Bonatti J, Schachner T, Velik-Salchner C, Pachinger O, et al. Sixty-four slice ct evaluation of aortic stenosis using planimetry of the aortic valve area. AJR. AJR Am J Roentgenol. 2007;189:197–203.
Ropers D, Ropers U, Marwan M, Schepis T, Pflederer T, Wechsel M, et al. Comparison of dual-source computed tomography for the quantification of the aortic valve area in patients with aortic stenosis versus transthoracic echocardiography and invasive hemodynamic assessment. Am J Cardiol. 2009;104:1561–7.
Ko SM, Song MG, Hwang HK. Evaluation of the aortic and mitral valves with cardiac computed tomography and cardiac magnetic resonance imaging. Int J Cardiovasc Imaging. 2012;28 Suppl 2:109–27.
Acknowledgment
The authors thank Marion Merdian and Heike Koitsch for excellent technical assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SB: study design, acquisition of the data, image analysis, statistical analysis, manuscript drafting. KD, AL: study design, image analysis, manuscript revising. FS: acquisition of the data, manuscript revising. BD: study design, acquisition of the data, image analysis, manuscript drafting.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Buchner, S., Debl, K., Schmid, FX. et al. Cardiovascular magnetic resonance assessment of the aortic valve stenosis: an in vivo and ex vivo study. BMC Med Imaging 15, 34 (2015). https://doi.org/10.1186/s12880-015-0076-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-015-0076-x