
Abstract
Background
Taste or smell disorders have been reported as strongly associated with COVID-19 diagnosis. We aimed to identify subject characteristics, symptom associations, and antibody response intensity associated with taste or smell disorders.
Methods
We used data from SAPRIS, a study based on a consortium of five prospective cohorts gathering 279,478 participants in the French general population. In the analysis, we selected participants who were presumably infected by SARS-CoV-2 during the first epidemic wave.
Results
The analysis included 3,439 patients with a positive ELISA-Spike. Sex (OR = 1.28 [95% CI 1.05–1.58] for women), smoking (OR = 1.54 [95% CI 1.13–2.07]), consumption of more than 2 drinks of alcohol a day (OR = 1.37 [95% CI 1.06–1.76]) were associated with a higher probability of taste or smell disorders. The relationship between age and taste or smell disorders was non-linear. Serological titers were associated with taste or smell disorders: OR = 1.31 [95% CI 1.26–1.36], OR = 1.37 [95% CI 1.33–1.42] and OR = 1.34 [95% CI 1.29–1.39] for ELISA-Spike, ELISA-Nucleocapsid and seroneutralization, respectively. Among participants with taste or smell disorders, 90% reported a wide variety of other symptoms whereas 10% reported no other symptom or only rhinorrhea.
Conclusions
Among patients with a positive ELISA-Spike test, women, smokers and people drinking more than 2 drinks a day were more likely to develop taste or smell disorders. This symptom was strongly associated with an antibody response. The overwhelming majority of patients with taste or smell disorders experienced a wide variety of symptoms.
Similar content being viewed by others


Background
Symptoms of COVID-19 are commonly cough, fever, dyspnea, myalgia, headache, arthralgia and diarrhea [1, 2]. The spread of the epidemic highlighted a new disease presentation: patients with taste or smell disorders (TSD). This symptom has been reported to be highly predictive of COVID-19 diagnosis [3]. There is no consensus in the literature about patient characteristics associated with this symptom [4, 5]. There remain many unanswered questions about the relationships between antibody response intensity and TSD and their association with other COVID-19 symptoms. Although long-term data in the general population are still scarce, it appears that TSD may be persistent over time in some patients [6].
To provide a better understanding of TSD in COVID-19 patients, we conducted an analysis based on data from the SAPRIS multicohort study. Our main goals were to identify subject characteristics associated with TSD, to investigate the relationship between TSD and antibody response intensity and to characterize symptom associations for subjects with or without TSD.
Methods
Design
We used data from SAPRIS (“Santé, Perception, pratiques Relations et Inégalités Sociales en population générale pendant la crise COVID-19”) based on a consortium of prospective cohort studies involving three general population-based adult cohorts: CONSTANCES, a “general population” cohort including a representative sample of 215,000 adults (including 66,000 followed by internet) aged 18 to 69 years at inclusion and recruited from 2012; E3N / E4N, a multigenerational adult cohort based on a community of families with 113,000 participants (women recruited in 1990 and still actively followed, their offspring and the fathers of this offspring) among whom 90,000 have been invited to an internet follow-up; and NutriNet-Santé a nutritional general population-based internet cohort started in 2009, with 170,000 included participants. Details on the SAPRIS survey are available elsewhere [7].
Participants and dates
All participants were invited to respond to two electronic self-administered questionnaires. Questionnaires were sent as of April 1, 2020 and returned before May 27, 2020, thus they covered the lockdown and post lockdown period (in France, the first lockdown occurred between March 17, 2020 and May 11, 2020). These data were combined with serological results from the SAPRIS-SERO study, in which a random sample of SAPRIS participants were invited to provide self-sampling dried-blood spot (DBS) aimed at serology testing [8].
Overall, 279,478 participants were invited to respond to SAPRIS questionnaires, 102,001 (37%) completed both questionnaires, and among them, 93,610 were invited to perform the serology, 86,913 (93%) returned dried blood spot and a serology could be performed and interpretable in 82,787.
In this analysis, we selected participants who had been presumably infected by SARS-CoV-2 based on serological results, i.e. all participants with a positive ELISA-S result, leading to a set of 3,695 participants.
Ethical approval and written or electronic informed consent were obtained from each participant before enrolment in the original cohort. The SAPRIS survey was approved by the Inserm ethics committee (approval #20–672 dated March 30, 2020). The SAPRIS-SERO study was approved by the Sud-Mediterranee III ethics committee (approval #20.04.22.74247) and electronic informed consent was obtained from all participants for DBS testing.
Data sources/measurement
Symptoms were reported if they had been present at least once within 14 days prior to each questionnaire. Smoking status, alcohol consumption and body mass index (BMI) were extracted from the original cohort databases and updated in 2020 with self-reported questionnaires.
The ELISA test (Anti-SARS-CoV-2 ELISA, Euroimmun®, Lübeck, Germany) was used to detect anti-SARS-CoV-2 antibodies (IgG) directed against the S1 domain of the spike protein of the virus (ELISA-S). Following the manufacturer’s instructions, an ELISA-S test was considered to be positive with an optical density ratio ≥ 1.1, indeterminate between 0.8 and 1.1, and negative < 0.8. The sensitivity and specificity of the ELISA-S test at the 1.1 threshold (considering indeterminate results as negative) were reported to be 87% and 97.5%, respectively [9].
All samples with an ELISA-S test ≥ 0.7 were also tested with an ELISA test to detect IgG antibodies against the SARS-CoV-2 nucleocapsid protein (Anti-SARS-CoV-2 NCP ELISA, Euroimmun®, Lübeck, Germany, ELISA-NP) using the same thresholds as above and with an in-house micro-neutralization assay to detect neutralizing anti-SARS-CoV-2 antibodies (SN), as described elsewhere with a positive SN defined as a titer ≥ 40 (SN titer was determined by iterative dilutions, leading to discrete values for titers, equal to 10, 20, 40, 80 or 160) [10].
Variables
The main outcome was the presence of self-reported TSD on either the first or the second questionnaire. Systemic symptoms were defined as presence of fever or muscular aches or headaches; digestive symptoms as presence of diarrhea or nausea; pulmonary symptoms as presence of cough, dyspnea or chest pain. Smoking status was defined as a binary variable “active smoker” versus “non-smoker or former smoker”. Alcohol consumption was defined as a binary variable “ ≤ 2 drinks per day” versus “ > 2 drinks per day”. BMI was defined as a binary variable “overweighted or obese (BMI ≥ 25 kg/m2)” versus “underweighted or normal (BMI < 25 kg/m2)”.
We considered the optical density ratios of ELISA-S and ELISA-NP as well as neutralizing anti-SARS-CoV-2 antibody titers as quantitative variables. To compensate for the non-normality of the distribution, statistical analyses were conducted on log-transformed titers.
Missing data
Participants with missing data on the main outcome or other covariates were excluded from the analyses. A sensitivity analysis with multiple imputation of missing data was conducted to assess robustness of results: 20 imputed datasets were generated with multiple imputation by chained equations (predictive mean matching), among which all estimates were poled using Rubin’s rule.
Statistical method
Logistic regression models were used to identify factors associated with TSD. These models considered sex, age, smoking status, alcohol consumption and BMI. To account for nonlinearity, age was included in the regression models using restricted cubic splines. We also tested interactions between sex and either smoking status or alcohol consumption. Interaction terms and nonlinear terms for age were retained in the final model if they improved the BIC criterion.
Logistic regression models were used to estimate the association between TSD and serological titers according to the three assays, respectively. Analyses were adjusted for age, sex, smoking status, alcohol consumption and BMI, as potential cofounders, in each model. Associations with TSD were reported as odds ratios (OR) with their 95% confidence intervals (CI).
Marginal and joint distributions of symptoms were reported with upset plots. For the group of patients with TSD, the TSD symptom was included in the analysis whereas in the group without TSD, an “asymptomatic” category was created and included in the analysis. Both analyses included digestive, respiratory, systemic, fatigue and rhinorrhoea symptoms. Hierarchical ascending classification was used to identify subsamples of subjects with similar symptoms associations. The optimal number of clusters was determined visually by means of the Elbow method for hierarchical clustering [11].
All analyses were conducted with the R statistical software version 4.0.3. Reporting of this research follows STROBE guidelines [12].
Results
Out of the 93,610 participants who completed both questionnaires and were invited to perform a DBS, 3,439 (3.7%) with a positive ELISA-S with available information on TSD were included in the analysis. A detailed flow diagram is provided (Fig. 1). Sensitivity analyses relying on multiple imputation provided similar results whenever conducted (Supplementary Tables S1 and S2).

Inclusion of participants in the study. Legend: Flow diagram describing the process of inclusion in our study for participants to SAPRIS cohort
Patients’ characteristics and association with TSD
Table 1 presents the characteristics of participants with positive ELISA-S (PE-S), along with ORs from univariable and multivariable analyses. Out of the 3,439 PE-S participants, 750 (21.8%) reported TSD. Among participants with and without TSD, 534 (71.2%) and 1,848 (68,7%) were women, respectively. Median ages were 51 (Q1-Q3, 42–61) for participants with TSD and 46 (Q1-Q3, 40–60) years for participants without TSD.
Multivariable analyses included 3,439 participants with PE-S. No interaction was found between sex and either smoking status or alcohol consumption. Nonlinear terms for age improved the BIC criterion and were kept in the selected model. Sex (OR = 1.28 [95% CI 1.05–1.58] for women), smoking (OR = 1.54 [95% CI 1.13–2.07]), alcohol consumption of at least 3 drinks per day (OR = 1.37 [95% CI 1.06–1.76]) were associated with a higher probability of TSD. Compared with subjects aged 40 years as a reference, those aged 30 (OR = 1.82 [95% CI 1.27–2.60]), 50 (OR = 1.91 [95% CI 1.63–2.23]), 60 (OR = 4.33 [95% CI 3.54–5.29]) or 70 (OR = 1.67, [95% CI 1.35–2.05]) had a higher probability of reporting TSD. The nonlinear age-dependent estimated OR is reported in Fig. 2.

Age-dependent estimated OR (95% CI) of taste or smell disorder, participants aged 40 as reference. Legend: Graphic representation of age-dependent estimated OR (and 95% CI) of taste and smell disorders in multivariable analyses. People aged 40 are considered as reference
Serology
Distributions of serological titers in PE-S participants are reported in Table 2. Associations between serological titers and TSD were estimated in three independent multivariable models. Related ORs are reported per 0.1 augmentation in the log-transformed titers and can approximately be interpreted as ORs per 10% increase in serological titers. All titers were associated with a higher probability of TSD: OR = 1.31 [95% CI 1.26–1.36], OR = 1.37 [95% CI 1.33–1.42] and OR = 1.34 [95% CI 1.29–1.39] for ELISA-S, ELISA-NP and seroneutralization, respectively.
Symptoms
Analyses regarding the association of TSD with other symptoms included 3,247 participants with PE-S and no missing data for symptoms. Table 3 reports results of the hierarchical clustering analysis, using only reported symptoms in PE-S participants. Four clusters were identified: cluster #1 groups all asymptomatic participants; cluster #2 groups participants with various associations of symptoms; cluster #3 groups participants with TSD, mostly isolated or associated with rhinorrhea; whereas cluster #4 groups patients with digestive symptoms, mostly isolated or associated with fatigue. Table 3 also presents the distribution of age, sex and serological titers in these clusters. These characteristics were not used to identify clusters.
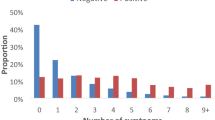
Results are also presented using two upset plots (Supplementary Fig. S1): one for participants with TSD (Fig. S1A; n = 698) and one for participants without TSD (Fig. S1B; n = 2,549). Both plots took into account self-reported symptoms in at least one of the two questionnaires.
Discussion
Taste or smell disorders have been extensively reported as common symptoms in SARS-CoV-2 infections [13]. Direct contact and interaction of the virus with gustatory or olfactory receptor cells may be the main cause for this symptom, though other pathophysiologic pathways are possible [14].
Key findings
We found that the risk of reporting TSD for participants with a positive SARS-CoV-2 ELISA-S test is higher in women, smokers and participants drinking more than 2 drinks of alcohol a day, after adjustment for age. The association with age was nonlinear, with a lower probability of TSD for participants aged around 40, compared with younger or older ones. In addition, our analyses showed a strong association between developing TSD and an intense antibody response for people with a positive ELISA-S. Regarding symptoms, our study shows two patterns of symptom association in participants with TSD: in 90% of them, TSD are associated with a wide variety of symptoms, while in 10% of them, TSD are isolated or associated with rhinorrhea.
Interpretation
Patient profile
The association between TSD and female gender in SARS-CoV-2 infected subjects is well documented [5, 15, 16] and previous findings support our results. The nonlinear association with age, suggesting that patients around 40 years present a lower probability to report TSD, is not easily interpretable as conflicting results were reported regarding the association of TSD with age: a study showed that age higher than 18 years was associated with TSD, compared to 15–17 years, with results suggesting a higher frequency of TSD in infected subjects aged 18–44 years than adolescents and older subjects [5]. Another study found a lower prevalence of TSD in elderly patients [17]. Regarding the association we found between smoking status and TSD, previous studies also reported conflicting results, some of them finding a similar association [18, 19] while others did not [4, 17, 20]). A possible explanation for this association is that functional interactions between nicotine and the angiotensin-converting enzyme 2 (ACE2) facilitate the infection of cells by the virus [21]. To our knowledge, the association between TSD and alcoholic consumption was reported – and nonsignificant – in only one case–control study with a limited sample size [22]. No obvious biological mechanism is likely to explain this result and a spurious association due to residual confounding cannot be ruled out. The non-association between TSD and overweight is consistent with the literature [17].
Antibody response
We found that the development of TSD was strongly associated with the antibody response. Even though the pathophysiology of TSD in SARS-CoV-2 infection is still poorly understood, these results, combined with the literature, suggest the existence of a biological mechanism between antibody response and TSD. Animal studies suggest that the interaction between ACE2 and the spike protein may yield to massive infection of sustentacular cells in the olfactory epithelium and immune cell infiltration leading to global desquamation of this epithelium [23, 24]. Other studies support that cell infection by the SARS-CoV-2 and infiltration of immune cells in the olfactory epithelium could lead to olfactory sensory neurons infection by horizontal spreading [25] or to loss of odorant receptor [26].
Symptoms
We discerned different patterns of symptoms associations in participants with a positive ELISA-S test. Participants with TSD were more likely to report a wide variety of symptoms, while most participants without TSD reported a complete absence of symptoms or isolated symptoms (systemic or rhinorrhea mainly). In the literature, the majority of patients with TSD experienced at least one other symptom [17, 27, 28], which is consistent with our findings.
Strengths and limitations
The participants in the SAPRIS study are drawn from cohorts whose source population is the general population with a high participation rate and whose participants are well characterised and well followed. The study design allows for results to be obtained from a large sample of individuals from the general population rather than from inpatients or outpatients. In addition, the case definition is based on an objective result and not on self-reported symptoms and is prospective, hence the large number of asymptomatic patients.
Regarding serology, DBS has been performed between May 04, 2020 and September 30, 2020 corresponding to a timeframe of very low level of virus circulation in France; it is therefore very unlikely that a patient would have been infected between the completion of the questionnaires and the DBS. Serological analyses were centralized and performed according to a double-blind design (participants and investigator). Results obtained with different serological assays (ELISA-S, ELISA-NP and seroneutralization) regarding the associations of antibody responses with TSD were consistent, which supports their robustness.
Several limitations must be noted. First, we considered participants with a positive ELISA-S as having been infected by the SARS-CoV-2. This assumption may lead to an underestimation of the number of subject (participants who have been infected with the SARS CoV-2) as (i) participants with an intermediate level of serological response (ELISA-S between 0.8 and 1.1) are considered as negative, (ii) it has been shown that the initial serological response decreases over time following the infection, which may yield a loss of sensitivity due to seroreversion at the time of DBS collection, this latter issue was partially addressed as DBS were mostly collected shortly after the first epidemic wave, before seroreversion was likely to occur [29], and (iii) 10% to 20% of infected individuals will not mount a detectable humoral response [30, 31]. Thus, though this case definition favoured specificity over sensitivity and limits the occurrence of false positive cases, we may have selected infected participants whose initial antibody response was intense while infected participants with a milder antibody response may have not been detected. As only one sample was analysed per participant, within-participant dynamics of the serological response could not be studied. Second, TSD, as well as all other symptoms, were self-reported. It has been shown that self-reporting of TSD may lead to under-reporting of this symptom, compared with objective assessment by a professional [27]. We may also assume that participants who reported a TSD are those who are the most likely to report other types of symptoms, which may partly explain the frequent associations of TSD with several other symptoms. Additionally, self-reporting of symptoms may also be subject to recall bias, for instance if the likelihood of recalling symptoms is higher in patients who have been previously positively tested for SARS-CoV-2. This may concern only 295 (8.6%) out of the 3,439 participants with positive ELISA-S, as others completed questionnaires blinded to their serological status. Though the expected effect of a hypothetical recall bias therefore seems very limited, we cannot rule out a loss of statistical power in our analyses due to non-differential misclassification in self-reported symptoms.
Conclusions
In conclusion, our study shows that among patients with a positive serology ELISA-S test, women, smokers and people drinking more than 2 drinks a day were more likely to develop TSD. We also found a strong association between antibody response and TSD. Regarding symptoms associations, the overwhelming majority of participants with TSD experienced a wide variety of acute symptoms, while a few of them only developed TSD either isolated or associated with only rhinorrhea.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Change history
26 July 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12879-023-08450-2
References
Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, Escalera-Antezana JP, et al. Clinical, laboratory and imaging features of COVID-19: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;34:101623. https://doi.org/10.1016/j.tmaid.2020.101623.
Wan S, Xiang Y, Fang W, Zheng Y, Li B, Hu Y, et al. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J Med Virol. 2020;92:797–806. https://doi.org/10.1002/jmv.25783.
Bénézit F, Le Turnier P, Declerck C, Paillé C, Revest M, Dubée V, et al. Utility of hyposmia and hypogeusia for the diagnosis of COVID-19. Lancet Infect Dis. 2020;20:1014–5. https://doi.org/10.1016/S1473-3099(20)30297-8.
Chary E, Carsuzaa F, Trijolet J-P, Capitaine A-L, Roncato-Saberan M, Fouet K, et al. Prevalence and recovery from olfactory and gustatory dysfunctions in Covid-19 infection: a prospective multicenter study. Am J Rhinol&Allergy. 2020;34:686–93. https://doi.org/10.1177/1945892420930954.
Carrat F, Touvier M, Severi G, Meyer L, Jusot F, Lapidus N, et al. Incidence and risk factors of COVID-19-like symptoms in the French general population during the lockdown period: a multi-cohort study. BMC Infect Dis. 2021;21:169. https://doi.org/10.1186/s12879-021-05864-8.
Carrat F, de Lamballerie X, Rahib D, Blanché H, Lapidus N, Artaud F, et al. Antibody status and cumulative incidence of SARS-CoV-2 infection among adults in three regions of France following the first lockdown and associated risk factors: a multicohort study. Int J Epidemiol. 2021:dyab110. https://doi.org/10.1093/ije/dyab110.
Patel EU, Bloch EM, Clarke W, Hsieh Y-H, Boon D, Eby Y, et al. Comparative performance of five commercially available serologic assays to detect antibodies to SARS-CoV-2 and identify individuals with high neutralizing titers. Infect Dis (except HIV/AIDS); 2020. https://doi.org/10.1101/2020.08.31.20184788.
Gallian P, Pastorino B, Morel P, Chiaroni J, Ninove L, de Lamballerie X. Lower prevalence of antibodies neutralizing SARS-CoV-2 in group O French blood donors. Antivir Res. 2020;181:104880. https://doi.org/10.1016/j.antiviral.2020.104880.
Shi C, Wei B, Wei S, Wang W, Liu H, Liu J. A quantitative discriminant method of elbow point for the optimal number of clusters in clustering algorithm. J Wireless Com Network. 2021;2021:31. https://doi.org/10.1186/s13638-021-01910-w.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–9. https://doi.org/10.1016/j.jclinepi.2007.11.008.
Boscutti A, Delvecchio G, Pigoni A, Cereda G, Ciappolino V, Bellani M, et al. Olfactory and gustatory dysfunctions in SARS-CoV-2 infection: a systematic review. Brain Behav Immun Health. 2021;15:100268. https://doi.org/10.1016/j.bbih.2021.100268.
Finsterer J, Stollberger C. Causes of hypogeusia/hyposmia in SARS-CoV2 infected patients. J Med Virol. 2020;92:1793–4. https://doi.org/10.1002/jmv.25903.
Galmiche S, Bruel T, Madec Y, Tondeur L, Grzelak L, Staropoli I, et al. Characteristics associated with olfactory and taste disorders in COVID-19. Neuroepidemiology. 2021;55:381–6. https://doi.org/10.1159/000517066.
Kusnik A, Weiss C, Neubauer M, Huber B, Gerigk M, Miethke T, et al. Presence of gustatory and olfactory dysfunction in the time of the COVID-19 pandemic. BMC Infect Dis. 2021;21:612. https://doi.org/10.1186/s12879-021-06294-2.
Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol. 2020;277:2251–61. https://doi.org/10.1007/s00405-020-05965-1.
Izquierdo-Domínguez A, Rojas-Lechuga M, Chiesa-Estomba C, Calvo-Henríquez C, Ninchritz-Becerra E, Soriano-Reixach M, et al. Smell and taste dysfunction in COVID-19 is associated with younger age in ambulatory settings: a multicenter cross-sectional study. J Investig Allergol Clin Immunol. 2020;30:346–57. https://doi.org/10.18176/jiaci.0595.
Talavera B, García-Azorín D, Martínez-Pías E, Trigo J, Hernández-Pérez I, Valle-Peñacoba G, et al. Anosmia is associated with lower in-hospital mortality in COVID-19. J Neurol Sci. 2020;419:117163. https://doi.org/10.1016/j.jns.2020.117163.
Galluzzi F, Rossi V, Bosetti C, Garavello W. Risk factors for olfactory and gustatory dysfunctions in patients with SARS-CoV-2 infection. Neuroepidemiology. 2021;55:154–61. https://doi.org/10.1159/000514888.
Husain Q, Kokinakos K, Kuo Y-H, Zaidi F, Houston S, Shargorodsky J. Characteristics of COVID-19 smell and taste dysfunction in hospitalized patients. Am J Otolaryngol. 2021;42:103068. https://doi.org/10.1016/j.amjoto.2021.103068.
Mercante G, Ferreli F, De Virgilio A, Gaino F, Di Bari M, Colombo G, et al. Prevalence of taste and smell dysfunction in coronavirus disease 2019. JAMA Otolaryngol Head Neck Surg. 2020;146:723. https://doi.org/10.1001/jamaoto.2020.1155.
Kabbani N, Olds JL. Does COVID19 infect the brain? If so, smokers might be at a higher risk. Mol Pharmacol. 2020;97:351–3. https://doi.org/10.1124/molpharm.120.000014.
Dev N, Sankar J, Gupta N, Meena RC, Singh C, Gupta DK, et al. COVID-19 with and without anosmia or dysgeusia: a case-control study. J Med Virol. 2021;93:2499–504. https://doi.org/10.1002/jmv.26784.
Meunier N, Briand L, Jacquin-Piques A, Brondel L, Pénicaud L. COVID 19-induced smell and taste impairments: putative impact on physiology. Front Physiol. 2021;11:625110. https://doi.org/10.3389/fphys.2020.625110.
Letko M, Marzi A, Munster V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat Microbiol. 2020;5:562–9. https://doi.org/10.1038/s41564-020-0688-y.
de Melo GD, Lazarini F, Levallois S, Hautefort C, Michel V, Larrous F, et al. COVID-19–related anosmia is associated with viral persistence and inflammation in human olfactory epithelium and brain infection in hamsters. Sci Transl Med. 2021;13:eabf8396. https://doi.org/10.1126/scitranslmed.abf8396.
Rodriguez S, Cao L, Rickenbacher GT, Benz EG, Magdamo C, Gomez LR, et al. Innate immune signaling in the olfactory epithelium reduces odorant receptor levels: modeling transient smell loss in COVID-19 patients. Neurology. 2020. https://doi.org/10.1101/2020.06.14.20131128.
Hornuss D, Lange B, Schröter N, Rieg S, Kern WV, Wagner D. Anosmia in COVID-19 patients. Clin Microbiol Infect. 2020;26:1426–7. https://doi.org/10.1016/j.cmi.2020.05.017.
Speth MM, Singer-Cornelius T, Oberle M, Gengler I, Brockmeier SJ, Sedaghat AR. Olfactory dysfunction and sinonasal symptomatology in COVID-19: prevalence, severity, timing, and associated characteristics. Otolaryngol Head Neck Surg. 2020;163:114–20. https://doi.org/10.1177/0194599820929185.
Marot S, Malet I, Leducq V, Zafilaza K, Sterlin D, Planas D, et al. Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers. Nat Commun. 2021;12:844. https://doi.org/10.1038/s41467-021-21111-9.
Wei J, Matthews PC, Stoesser N, Maddox T, Lorenzi L, Studley R, et al. Anti-spike antibody response to natural SARS-CoV-2 infection in the general population. Nat Commun. 2021;12:6250. https://doi.org/10.1038/s41467-021-26479-2.
Oved K, Olmer L, Shemer-Avni Y, Wolf T, Supino-Rosin L, Prajgrod G, et al. Multi-center nationwide comparison of seven serology assays reveals a SARS-CoV-2 non-responding seronegative subpopulation. EClinicalMedicine. 2020;29:100651. https://doi.org/10.1016/j.eclinm.2020.100651.
Acknowledgements
The authors warmly thank all the volunteers of the Constances, E3N-E4N, and NutriNet-Sante cohorts.
We thank the staff of the Constances, E3N-E4N and NutriNet-Sante cohorts that have worked with dedication and engagement to collect and manage the data used for this study and to ensure continuing communication with the cohort participants. We thank the CEPH-Biobank staff for their adaptability and the quality of their work. In the virology department, Dr Nadege Brisbarre and the technical staff for impeccable management of samples and serological assays.
The SAPRIS study group
Nathalie Bajos (co-Principal investigator), Fabrice Carrat (co-Principal investigator), Pierre-Yves Ancel, Marie-Aline Charles, Florence Jusot, Claude Martin, Laurence Meyer, Ariane Pailhe, Alexandra Rouquette, Gianluca Severi, Alexis Spire, Mathilde Touvier, Marie Zins
The SAPRIS-SERO study group
- Fabrice Carrat (Principal investigator), Pierre-Yves Ancel, Marie-Aline Charles, Gianluca Severi, Mathilde Touvier, and Marie Zins, for the SAPRIS-SERO coordination
- Sofiane Kab, Adeline Renuy, Stéphane Le Got, Céline Ribet, Mireille Pellicer, Emmanuel Wiernik, Marcel Goldberg, and Marie Zins, for the Constances cohort
- Fanny Artaud, Pascale Gerbouin-Rérolle, Mélody Enguix, Camille Laplanche, Roselyn Gomes-Rima, Lyan Hoang, Emmanuelle Correia, Alpha Amadou Barry, Nadège Senina, and Gianluca Severi, for the E3N-E4N cohort
- Julien Allegre, Fabien Szabo de Edelenyi, Nathalie Druesne-Pecollo, Younes Esseddik, Serge Hercberg, Mélanie Deschasaux and Mathilde Touvier, for the NutriNet-Santé cohort
- Marie-Aline Charles, Pierre-Yves Ancel, Valérie Benhammou, Anass Ritmi, Laetitia Marchand, Cécile Zaros, Elodie Lordmi, Adriana Candea, Sophie de Visme, Thierry Simeon, Xavier Thierry, Bertrand Geay, Marie-Noelle Dufourg, and Karen Milcent, for the Epipage2 and Elfe child cohorts
- Delphine Rahib, Nathalie Lydie (Santé Publique France)
- Clovis Lusivika-Nzinga, Gregory Pannetier, Nathanael Lapidus, Isabelle Goderel, Céline Dorival, Jérôme Nicol, Olivier Robineau and Fabrice Carrat, for the IPLESP – methodology and coordinating data center
- Cindy Lai, Liza Belhadji, Hélène Esperou, and Sandrine Couffin-Cadiergues, for the Inserm
- Jean-Marie Gagliolo, for the Institut de Santé Publique
- Hélène Blanché, Jean-Marc Sébaoun, Jean-Christophe Beaudoin, Laetitia Gressin, Valérie Morel, Ouissam Ouili, and Jean-François Deleuze, for the CEPH-Biobank
- Laetitia Ninove, Stéphane Priet, Paola Mariela Saba Villarroel, Toscane Fourié, Souand Mohamed Ali, Abdenour Amroun, Morgan Seston, Nazli Ayhan, Boris Pastorino, and Xavier de Lamballerie, for the Unité des Virus Emergents
Funding
This study
ANR (Agence Nationale de la Recherche, #ANR-20-COVI-000, #ANR-10-COHO-06), Fondation pour la Recherche Medicale (#20RR052-00), Inserm (Institut National de la Sante et de la Recherche Medicale, #C20-26).
Cohorts funding
The CONSTANCES Cohort Study is supported by the Caisse Nationale d’Assurance Maladie (CNAM), the French Ministry of Health, the Ministry of Research, the Institut national de la sante et de la recherche medicale. CONSTANCES benefits from a grant from the French National Research Agency [grant number ANR-11-INBS-0002] and is also partly funded by MSD, AstraZeneca, Lundbeck and L’Oreal. The E3N-E4N cohort is supported by the following institutions: Ministere de l’Enseignement Superieur, de la Recherche et de l’Innovation, INSERM, University Paris-Saclay, Gustave Roussy, the MGEN, and the French League Against Cancer. The NutriNet-Sante study is supported by the following public institutions: Ministere de la Sante, Sante Publique France, Institut National de la Sante et de la Recherche Medicale (INSERM), Institut National de la Recherche Agronomique (INRAE), Conservatoire National des Arts et Metiers (CNAM) and Sorbonne Paris Nord University. The CEPH-Biobank is supported by the ≪ Ministere de l’Enseignement Superieur, de la Recherche et de l’Innovation ≫.
Author information
Authors and Affiliations
Consortia
Contributions
JR: Design, methodology, writing-all stage. XL: Conceptualisation, design, data gathering, writing-reviewing and editing. OR, HB, GS, MT, MZ: Data gathering, writing-reviewing and editing. NL, FC: Conceptualisation, design, methodology, data gathering, writing-reviewing and editing. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments. The SAPRIS survey was approved by the Inserm ethics committee (approval #20–672 dated March 30, 2020). The SAPRIS-SERO study was approved by the Sud-Mediterranee III ethics committee (approval #20.04.22.74247).
Ethical approval and written or electronic informed consent were obtained from each participant before enrolment in the original cohort. Electronic informed consent was obtained from all participants for DBS testing.
Consent for publication
Not applicable.
Competing interests
Prof Fabrice Carrat reports personal fees from Sanofi, unrelated to the submitted work. Dr Olivier Robineau reports personal fees from MSD, Gilead, ViiV, unrelated to the submitted work.
All other authors declare no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article has been updated to correct the missing collaborators.
Supplementary Information
Additional file 1: Supplementary Figure S1A.
Symptoms associations in participants with positive ELISA-S and taste or smell disorders. Supplementary Figure S1B. Symptoms associations in participants with positive ELISA-S and no taste or smell disorders. Table S1. Characteristics of participants with and without taste or smell disorders (TSD) in the sensitivity analysis conducted with multiple imputation to handle missing values. Categorial variables are reported as average counts (percentages of non-missing values) and quantitative variables as median [Q1–Q3]. Table S2. Distribution of serological titers and associations with taste or smell disorders (TSD) adjusted for sex, age, smoking status, alcohol consumption and BMI in the sensitivity analysis conducted with multiple imputation to handle missing values.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ramillon, J., de Lamballerie, X., Robineau, O. et al. Antibody response, associated symptoms and profile of patients presumably infected by SARS-CoV-2 with taste or smell disorders in the SAPRIS multicohort study. BMC Infect Dis 23, 228 (2023). https://doi.org/10.1186/s12879-023-08162-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08162-7