
Abstract
Background
Trichinosis is a worldwide food-borne zoonotic parasitic disease, which is mainly obtained by ingesting undercooked meat containing infected larvae. The purpose of our article is to introduce and discuss two rare cases of pleural effusion caused by Trichinella spiralis.
Case presentation
Here we described two male patients who presented to the respiratory department of our hospital with a massive unilateral pleural effusion, their serum eosinophils were in the normal range, laboratory serological tests revealed that Trichinella spiralis IgG antibody was positive. After the oral administration of antiparasitic drugs, the pleural effusion of two patients was completely absorbed.
Conclusion
Both patients were diagnosed with Trichinosis complicated with pleural effusion, which is very rare in the clinic and easy to be misdiagnosed because of normal eosinophils.
Similar content being viewed by others


Background
Trichinellosis is a worldwide food-borne zoonotic parasitic disease caused by the infection of all species of Trichinella spp, which is mainly acquired by eating undercooked meat containing infected larvae [1]. From 1964 to 2011, more than 600 outbreaks of human Trichinosis were recorded in China, which were prevalent in southwest, northeast, and central regions. The outbreaks mainly occurred in Yunnan province, the outbreak time was concentrated in winter and spring, and the majority of people were young adults. The World Organization for Animal Health (OIE) defines this disease as a class B zoonotic disease, and China lists this disease as a class II animal disease, which is required to be detected in pig slaughtering and quarantine. Trichinella spiralis infection can cause fever, eyelid edema, muscle pain, eosinophilia, and other symptoms [2]. Severe Trichinosis is characterized by cardiovascular, pulmonary, and central nervous system involvement [3]. Trichinella spiralis infection causes pleural effusion, which is relatively rare clinically. Because clinicians have little understanding of this disease, it is easy to miss and misdiagnose.
Case report
Case 1
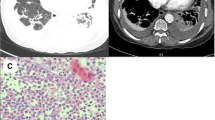
A 75-year-old man was admitted to the hospital on December 20th, 2020, because his left pleural effusion was found by physical examination for half a month. He had no obvious edema around the eyes and face, and no muscle pain. Previous history of hypertension. Admission physical examination: Temperature: 36.8 ℃, Pulse: 78 times/min, Respiratory Rate: 20 times/min, Blood Pressure: 143/67 mmHg, Low breath sounds in the lower left lung, normal auscultation in the right lung. Lung Computed Tomography (CT) in our hospital on December 18th, 2020: Moderate pleural effusion on the left side with partial distension of the left lung; the right lung is scattered in solid nodules (Figs. 1, 2). After the patient was admitted to the hospital, the absolute value of serum eosinophils was 0.30 × 109/L (the normal range is 0.05–0.50 × 109/L), Serum creatine kinase was 48 u/L (the normal range is 38–174 u/L). Other serum laboratory tests were normal. Serum protein was 55.1 g/L (the normal range is 65–85 g/L), and serum lactate dehydrogenase (LDH) was 141 u/L (the normal range is 125–243 u/L). Routine examination of pleural effusion: Color: red; Transparency: turbid; Coagulation: there are clots; Specific gravity: 1.022; Rivalta test: positive; Number of nucleated cells: 3180/ul; Mononuclear cells (included lymphocytes and monocytes): 98.9%; Multiple nuclear cells (included neutrophils and eosinophils): 1.1%. Biochemical examination of pleural effusion: Glucose: 5.52 mmol/L (the normal range is 3.9–6.1 mmol/L); Protein: 36.5 g/L (the normal range is 20–40 g/L); Albumin: 22.2 g/L (the normal range is 20–40 g/L); Chlorine: 111.3 mmol/L (the normal range is 110-130 mmol/L); Pleural LDH: 220 U/L (the normal range is 230–460 u/L); Adenosine deaminase (ADA):9U/L(the normal range is 0–18 u/L). No obvious abnormality was found in urological and cardiac ultrasound. Chest ultrasound suggested massive effusion in the left pleural cavity (the maximum anteroposterior diameter is about 7.6 cm). Positron emission tomography/computed tomography (PET/CT) showed: No signs of muscle involvement; no obvious signs of malignant tumor lesions were found at the detection site.

CT of the lung: obvious effusion signs were seen in the left thoracic cavity, patchy consolidation shadows were seen in the left lower lobe with incomplete swelling

CT of the lung: the right lung is scattered in solid nodules
The patient received an anti-infective treatment (cefotaxime sodium and sulbactam) for 1 week and then the pleural effusion had no significant decrease. Cytological report of pleural effusion showed that there were a few lymphocytes and mesothelial cells, and no obvious atypical epithelial cells. On the 11th day of admission, he was given diagnostic anti-Tuberculosis treatment for 25 days (rifampicin 450 mg quaque die (QD) + isoniazid 0.3gQD + moxifloxacin 0.4gQD). Pleural ultrasonography showed no obvious pleural fluid absorption, so he stopped using anti-Tuberculosis drugs. We questioned closely the patient's past history, He complained that he ate undercooked pork sausages sold in a small shop a month and a half ago, and after that, symptoms of diarrhea occurred (about 4 days). At this time, we considered whether there was parasitic infection. Therefore, the patient's serum was sent to Wuhan Tongji hospital, and the detection of parasite antibody IgG indicated Trichinella spiralis (+) by enzyme-linked immunosorbent assay (ELISA), and the diagnosis was Trichinosis. Albendazole tablets were given 800 mg/d for 1 week. Two weeks later, a chest ultrasound showed that the pleural effusion disappeared.
Case 2
A 59-year-old male was admitted to the hospital on November 24th, 2021 because of a cough for 1 week. The patient's cough was a mainly dry cough, accompanied by chest wall pain and wheezing at night. The symptoms worsened two days ago, accompanied by white phlegm and hoarseness, but no fever, so he came to our hospital for further treatment. Past physical fitness. Physical examination on admission: Temperature: 36.5 ℃, Pulse: 113 times/min, Respiratory Rate: 19 times/min, Blood Pressure: 119/79 mmHg, SpO2: 98%. A little moist rale can be heard in the upper right lung, and the left lung was normal, without wheezing or bronchospasm on lung auscultation. After the patient was admitted to the hospital, the absolute value of serum eosinophils was 0.2 × 109/L (the normal range is 0.05–0.5 × 109/L), other serum laboratory tests were normal. Electrocardiogram and purified Tuberculin pure protein derivative (PPD) tests were normal. Serum protein was 61.3 g/L. Routine examination of pleural effusion: color: light yellow; Transparency: slightly turbid; Coagulation: there are clots; Specific gravity: small quantity; Rivalta test: positive; Number of nucleated cells: 2488/ul; Mononuclear cells (included lymphocytes and monocytes): 86.7%; Multiple nuclear cells (included neutrophils and eosinophils): 13.3%. Biochemical examination of pleural effusion: Glucose: 7.38 mmol/L; Protein: 43.4 g/L; Albumin: 28.0 g/L; Chlorine: 108.9 mmol/L; Pleural LDH: 636 U/L; ADA:2U/L. Cytological examination of pleural effusion showed that a large number of inflammatory cells (mainly lymphocytes and neutrophils) and a few tissue cells were observed under a microscope. CT of the lung: Inflammation of the right lower lobe of the lung; Right pleural effusion with right lower lobe atelectasis (Fig. 3). Chest ultrasound suggested a massive pleural effusion on the right side (maximum anteroposterior diameter is about 10.7 cm). On the 8th day after admission, the patient's serum was sent to Wuhan Tongji hospital, and the detection of parasite antibody IgG indicated Trichinella spiralis (+) by ELISA, and the diagnosis was Trichinosis. After oral treatment with mebendazole tablets 300 mg/d for 1 week, his cough symptoms were completely relieved, one month later, the reexamination of lung CT showed that the right pleural effusion was absorbed (Fig. 4).

CT of the lung: patchy shadow can be seen in the lower lobe of the right lung, and effusion signs can be seen in the right chest cavity with hypodynamia of the lower lobe of the right lung

CT of the lung: after treatment, the right pleural effusion was significantly absorbed and the lung tissue was restretched
Discussion
Trichinella spiralis belongs to nematodes. Trichinella spiralis can infect pigs, dogs, cattle, cats, wolves, weasels, minks, foxes, whales, and others. Human infection with Trichinella is mainly due to eating raw or semi-raw animal meat (pork, wild boar, dog meat, etc.). Trichinosis patients themselves are not contagious, and their typical clinical manifestations after infection are high fever, periorbital and facial edema, muscle pain, subconjunctival hemorrhage, an allergic rash, and crescent or linear hemorrhage under fingers or toenails. Severe patients may have complications such as myocarditis, encephalitis, or pneumonia [4]. According to statistics from the zoonotic disease surveillance conducted by the European Union (MS) in 2017, half of the member states reported zero cases, and these countries have never reported any cases of Trichinosis [5]. In China, trichinellosis is mainly prevalent in the southwest, northeast, and central regions, and the outbreak mainly occurred in Yunnan Province.
The diagnosis of human Trichinellosis is mainly based on clinical symptoms and serological tests, such as ELISA, indirect immunofluorescence assay (IFA), enzyme immunohistochemistry technique (EIH), and Western-Blotting (WB), The International Commission on Trichinosis recommends ELISA, which detects anti-trichinella IgG in patients' serum by excretory secretion (E/S) antigen of Trichinella spiralis larvae. The sensitivity and specificity of total IgG were 93.6% and 94.3%, respectively [6]. The limitations of this method are that it has a high false-negative rate in the early stage of infection (1–3 months) and cannot distinguish between acute and previous infection [7]. Detection of circulating antigens (CAg), such as anti-immunoelectrophoresis, immunoradiometric assay, direct ELISA, and sandwich ELISA, is an effective method to distinguish between acute and previous infections. CAg is an excretory or secretory antigen produced by live insects, which can directly enter the peripheral blood circulation and can be used for early diagnosis and curative effect evaluation of Trichinosis. However, the detection rate of circulating antigens in serum is usually only 30–50% [8]. Therefore, it is not recommended for the diagnosis of Trichinosis. The discovery of Trichinella larvae cysts from muscle biopsy is the gold standard for the diagnosis of Trichinosis, but due to its invasiveness, the positive rate is only about 50%, and early infection cannot be detected, so it is not recommended [9]. The European Center for Disease Control has classified human Trichinosis into the clinical, laboratory, and epidemiological cases, of which laboratory cases refer to Trichinosis larvae found by muscle biopsy or seropositive. In this paper, the patient had a history of eating pork sausage, and the serological test was positive. After being treated with insect repellent (albendazole or mebendazole), pleural effusion was absorbed, so it was diagnosed as Trichinosis. The treatment plan for Trichinosis includes antiparasitic drugs (mebendazole or albendazole) and glucocorticoids [10]. Our patients were not given glucocorticoids during treatment. Albendazole is currently the preferred drug for the treatment of Trichinosis in China, the dosage is 20–30 mg/(kg·d), divided into two oral courses for 5–7 days [10]. Most patients have a good prognosis and recover within 1–2 months.
We summarized some cases of pleural effusion caused by a parasitic infection in Table 1 [11,12,13,14,15,16,17,18,19,20], the eosinophils of patients with parasitic pleurisy can be in the normal range, and the diagnosis of parasitic pleurisy mainly relies on ELISA of antibodies directed, such as Paragonimiasis, Toxocariasis, and Hydatidosis [21, 22]. The pleural effusion in the two patients in this paper was unilateral, and the pleural effusion was a lymphocyte-dominant exudate. The level of ADA was low, and it was difficult to diagnose Tuberculous pleuritis [23]. The tumor, rheumatism immunity, and other related tests were negative, and there was no significant increase in eosinophils in blood and pleural effusion, so we didn't consider parasitic infection when two patients were admitted to the hospital. The patient of case 1, after further questioning the medical history, he complained that he had recently eaten undercooked pork sausages sold in small shops. Considering that Paragonimiasis pleural effusion caused by eating crayfish was found in the Wuhan area. The clinical manifestations and pleural effusion properties of the two patients in this article are very similar. Therefore, we added serum parasite antibody tests. For case 1, it was speculated that the onset stage of the disease was Trichinosis when the patient ate undercooked pork sausage before 1.5 months, and the acute attack showed gastrointestinal symptoms (diarrhea). Then, pleural effusion was found in the physical examination before a month, which was considered as the late stage of Trichinosis and complications of pleural effusion. Studies have proved that respiratory complications are mostly in the late stage of the disease, that is, between the 3rd and 7th week of infection, bacterial pneumonia, pleurisy, and lung infarction may occur [24]. Therefore, the final diagnosis was Trichinosis complicated with pleural effusion in the late stage.
Conclusion
Trichinosis causes unilateral pleural effusion, which is extremely rare in clinical practice and has not been reported yet. The purpose of this paper is to remind clinicians that parasitic diseases should be included in the differential diagnosis of patients with unexplained pleural effusion, even if their serum eosinophils are within the normal range.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- CT:
-
Computed Tomography
- G test:
-
1,3-Beta-D glucan test
- GM test:
-
Galactomannan test
- LDH:
-
Lactate dehydrogenase
- ADA:
-
Adenosine deaminase
- PET/CT:
-
Positron emission tomography/computed tomography
- QD:
-
Quaque die
- PPD:
-
Tuberculin pure protein derivative
- ELISA:
-
Enzyme-linked immunosorbent assay
- CAg:
-
Circulating antigens
References
Capo V, Despommier DD. Clinical aspects of infection with Trichinella spp. Clin Microbiol Rev. 1996;9(1):47–54.
Wilson NO, Hall RL, Montgomery SP, Jones JL. Trichinellosis surveillance–United States, 2008–2012. Morb Mortal Wkly Rep Surveill Summ. 2015;64(1):1–8.
Taratuto AL, Venturiello SM. Trichinosis. Brain Pathol. 1997;7(1):663–72.
Diaz JH, Warren RJ, Oster MJ. The disease ecology, epidemiology, clinical manifestations, and management of trichinellosis linked to consumption of wild animal meat. Wilderness Environ Med. 2020;31(2):235–44.
European Food Safety Authority and European Centre for Disease Prevention and Control (EFSA and ECDC. The European Union summary report on trends and sources of zoonoses, zoonotic agents and food-borne outbreaks in 2017. EFSA J Eur Food Saf Auth. 2018;16(12): e05500.
Kahsay R, Gómez-Morales MA, Rivera HN, McAuliffe I, Pozio E, Handali S. A Bead-based assay for the detection of antibodies against Trichinella spp. infection in humans. Am J Trop Med Hyg. 2021;104(5):1858–62.
Wang ZQ, Fu GY, Jing FJ, Jin J, Ren HJ, Jiang P, Cui J. Detection of Trichinella spiralis circulating antigens in serum of experimentally infected mice by an IgY-mAb sandwich ELISA. Foodborne Pathog Dis. 2012;9(8):727–33.
Nishiyama T, Araki T, Mizuno N, Wada T, Ide T, Yamaguchi T. Detection of circulating antigens in human trichinellosis. Trans R Soc Trop Med Hyg. 1992;86(3):292–3.
Thawornkuno C, Nogrado K, Adisakwattana P, Thiangtrongjit T, Reamtong O. Identification and profiling of Trichinella spiralis circulating antigens and proteins in sera of mice with trichinellosis. PLoS ONE. 2022;17(3): e0265013.
Dupouy-Camet J, Kociecka W, Bruschi F, Bolas-Fernandez F, Pozio E. Opinion on the diagnosis and treatment of human trichinellosis. Expert Opin Pharmacother. 2002;3(8):1117–30.
Soukup J, Cerny J, Cegan M, Kelbich P, Novotny T. Toxocariasis as a rare parasitic complication of a transthoracic spine surgery procedure. Medicina. 2021;57(12):1328.
Fan T, Zhang Y, Lv Y, Chang J, Bauer BA, Yang J, Wang CW. Cutaneous myiasis with eosinophilic pleural effusion: a case report. World J Clin Cases. 2021;9(18):4803–9.
Park SJ, Jang CW, Kim YK, Seo YH, Kim KH, Kwon TG, Bae JH. Toxocariasis-associated acute perimyocarditis with cardiogenic shock: a case report. Am J Case Rep. 2021;22: e930573.
Savu C, Melinte A, Grigorie V, Iliescu L, Diaconu C, Dimitriu M, Socea B, Stiru O, Varlas V, Savu C, et al. Primary pleural hydatidosis-a rare occurrence: a case report and literature review. Medicina. 2020;56(11):567.
Aggarwal P, Subramanian S, Saini V, Aggarwal D. Filariasis presenting as isolated pleural effusion: a case report and mini review. Trop Doct. 2021;51(1):111–4.
Tourne M, Dupin C, Mordant P, Neuville M, Taillé C, Danel C. Autochthonous hydatid cyst of the lung. Ann Pathol. 2019;39(1):47–53.
Hämäläinen S, Kantele A, Arvonen M, Hakala T, Karhukorpi J, Heikkinen J, Berg E, Vanamo K, Tyrväinen E, Heiskanen-Kosma T, et al. An autochthonous case of cystic echinococcosis in Finland, 2015. Eur Commun Dis Bull. 2015;20(42):30043.
Vallentin B, Carsin A, Dubus JC. Toxocariasis: an unusual cause of pleural effusion. Pediatr Pulmonol. 2015;50(10):E35-36.
Oh Y, Kim JT, Kim MK, Chang YJ, Eom K, Park JG, Lee KM, Choe KH, An JY. Eosinophilic pleuritis due to sparganum: a case report. Korean J Parasitol. 2014;52(5):541–3.
Hernandez C, Cucunuba Z, Parra E, Toro G, Zambrano P, Ramírez JD. Chagas disease (Trypanosoma cruzi) and HIV co-infection in Colombia. Int J Infect Dis. 2014;26:146–8.
Wang J, Luo W, Shen P, He J, Zeng Y. Retrospective study of pleural parasitic infestations: a practical diagnostic approach. BMC Infect Dis. 2019;19(1):576.
Al-Tawfiq JA, Kim H, Memish ZA. Parasitic lung diseases. Eur Respir Rev. 2022;31(166):220093.
Ferreiro L, San José E, Valdés L. Tuberculous pleural effusion. Arch Bronconeumol. 2014;50(10):435–43.
Kociecka W. Trichinellosis: human disease, diagnosis and treatment. Vet Parasitol. 2000;93(3–4):365–83.
Acknowledgements
We thank AJE (www.AJE.com) for its linguistic assistance during the preparation of this manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors had full access to the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. PZZ was the manuscript designer, completing data analysis and writing the first draft of the paper. ZMJ participated in manuscript design and analysis of manuscript results. RYQ participated in manuscript design and analysis of manuscript results. YJ was the conceptionist and head of the manuscript, guiding manuscript design, data analysis, paper writing and revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The manuscript has been approved by Ethics Committee of the institution (Ethical number: 2022257K) and conform to the provisions of the Declaration of Helsinki.
Consent for publication
The manuscript had obtained "written informed consent to publish" from study participants.
Competing interests
There are no any competing commercial interests in relation to the submitted work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pan, Zz., Zhu, Mj., Rong, Yq. et al. Pleural effusion caused by Trichinella spiralis infection: two case reports. BMC Infect Dis 23, 77 (2023). https://doi.org/10.1186/s12879-023-08047-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08047-9