
Abstract
Background
Private healthcare providers are important to tuberculosis (TB) management globally, although internationally there are reports of suboptimal management and disparities in treatment commencement in the private sector. We compared the management of TB patients receiving private versus public healthcare in Victoria, an industrialised setting with low tuberculosis (TB) incidence.
Methods
Retrospective cohort study: 2002–2015. Private healthcare provision was included as an independent variable in several multivariate logistic and Cox proportional hazard regression models that assessed a range of outcome variables, encompassing treatment commencement delays, management and treatment outcomes.
Results
Of 5106 patients, 275 (5.4%) exclusively saw private providers, and 4714 (92.32%) public. Private care was associated with a shorter delay to presentation (HR 1.36, p = 0.065, 95% CI 1.02–2.00). Private patients were less likely to have genotypic testing (OR 0.66, p = 0.009, 95% CI 0.48–0.90), those with pulmonary involvement were less likely to have a sputum smear (OR 0.52, p = 0.011, 95% CI 0.31–0.86) and provided samples were less likely to be positive (OR 0.54, p = 0.070, 95% CI 0.27–1.05). Private patients with extrapulmonary TB were less likely to have a smear sample (OR 0.7, 95% CI 0.48–0.90, p = 0.009) and radiological abnormalities (OR 0.71, p = 0.070, 95% CI 0.27–1.05). Treatment commencement delays from presentation were comparable for cases with pulmonary involvement and extrapulmonary TB, although public extrapulmonary TB patients received radiological examinations slightly earlier than private patients (HR 0.79, p = 0.043, 95% CI 0.63–0.99) and public patients with pulmonary involvement from high burden settings commenced treatment following an abnormal CXR more promptly than their private counterparts (HR 0.41, p = 0.011, 95% CI 0.21–0.81). Private patients were more likely to receive <4 first-line medications (OR 2.17, p = 0.001, 95% CI 1.36–3.46), but treatment outcomes were comparable between sectors.
Conclusions
The differences we identified are likely to reflect differing case-mix as well as clinician practice. Sputum smear status was an important covariable in our analysis; with its addition we found no significant disparity in the health-system delay to treatment commencement between sectors. Our study highlights the importance of TB programs engaging with private providers, enabling comprehensive data collection that is necessary for thorough and true comparison of TB management and optimisation of care.
Similar content being viewed by others
Background
Private healthcare providers are important to tuberculosis (TB) management globally, contributing an estimated 6–48% of all total case notifications in 2015 [1]. However, reports from a variety of contexts have suggested differences in the timely diagnosis and initiation of therapy between public and private sectors [2]. Longer delays have been identified in the private sector, including treatment delays (variably defined as the time from symptom onset to either smear test result, diagnosis or treatment commencement) [3,4,5,6] and health system delays (time from healthcare presentation to treatment initiation) [7,8,9]. Surveys of private providers have revealed TB patient management practices that fall short of recommended guidelines in various settings [10,11,12,13,14,15,16].
Despite these reports of suboptimal management and disparities in treatment initiation, there are very few studies that compare the care provided and treatment outcomes between private and public settings. A study in Vietnam found poorer management and treatment outcomes of patients treated in one semi-private clinic compared to patients treated by the national TB control program [17], but another in Nigeria reported comparable outcomes [18]. While it is acknowledged that the size, structure and function of private healthcare providers in health systems vary greatly between settings, to our knowledge there have been no studies that have investigated diagnostic delays, TB management and outcomes for patients receiving private versus public healthcare in any setting.
Victoria is Australia’s second most populous state with an estimated resident population of 5.97 million (December quarter 2015) people [19], universal health care and both a low incidence of TB (6.7/100,000 in 2013) [20] and low TB-related mortality [21]. TB patients are predominantly managed in the public sector, although some do attend private healthcare providers. The Victorian TB program (VTP) engages with both public and private providers and collects detailed data on all TB patients diagnosed in Victoria, including consistently recording whether care is provided through private or public services. All microbiological diagnoses of TB, regardless of healthcare sector, are managed centrally, with routine molecular testing conducted at a single statewide reference laboratory [22]. In the interest of ensuring that TB care is optimal in Victoria, we sought to compare the quality of healthcare received between public and private settings. Specifically, we aimed to investigate whether disparities in treatment initiation and TB management reported elsewhere in the world are present in Victoria, and to examine any effect on treatment outcomes.
Methods
Study population
The study population comprised patients diagnosed with active TB in Victoria and notified to the Department of Health & Human Services between 1/1/2002 and 31/12/2015. In Victoria, all medical practitioners and diagnostic laboratories are required to report patients with TB to health authorities under public health legislation [20]. All patients, regardless of their choice of health provider, are followed up by the VTP. Confirmation of TB diagnosis by culture and drug susceptibility testing is routinely performed where possible [23].
Australia has a publicly funded universal health insurance scheme (Medicare). TB management within public hospitals and clinics are provided free of charge to all TB patients in Victoria [24]. Patients that choose to attend private hospitals or physicians are frequently charged additional fees over and above the cost that is covered by Medicare or their private health insurers. Medications for the treatment of TB are provided free of charge for all patients by the VTP.
Patient records were extracted from an existing programmatic database (Public Health Event Surveillance System, PHESS), which contains detailed demographic information, laboratory results and patient notes including notifying medical practitioners and hospital identification numbers.
Definitions
Sites of disease were categorised as cases with pulmonary involvement (excluding disseminated cases), disseminated and extrapulmonary manifestations (including lymph node TB). Any disease with two non-pulmonary, non-contiguous sites of disease was categorised as disseminated.
Figure 1 illustrates definitions of the various possible delays during TB management. Symptom onset, healthcare presentation dates, treatment commencement dates and dates of chest x-ray/CT-scan (CXR) were as specified on notification forms, or obtained by VTP nurses from clinicians, patients or medical records. Specimen collection dates and dates that test results were received were as recorded by laboratories.

Conceptual illustration of definitions of delays (adapted from Van Wyk et al. 2011)
Statistical analyses
Wilcoxon-Mann-Whitney tests and Chi squared tests were used to compare demographic and clinical differences between public and private cohorts.
Private healthcare provision was included as an independent variable in univariate and multivariate logistic regression to analyse the investigations, symptoms, laboratory tests, treatment regimens and treatment outcomes. All independent variables with P < 0.25 in univariate analysis were considered in multivariate analysis [25].
Kaplan-Meier curves were used to illustrate various delays in diagnosis and treatment between public and private cohorts, and private healthcare provision was included as an independent variable in Cox proportional hazard analyses to assess these delays (Table 3). All independent variables with P < 0.25 in univariate (log-rank) analysis were considered in multivariate analysis [25]. Proportionality assumptions were assessed using Kaplan-Meier survival curves; by including time-dependent covariates in the model; and with Schoenfeld and scaled Schoenfeld residuals. Interactions were explored and likelihood-ratio tests, Akaike information criterions (AIC) and multiway cross tabulations were performed to guide which to include. No interactions causing variable combination frequencies of less than ten were included, except where noted.
In multivariate analyses, p-values below 0.05 were considered significant, although findings with p-values less than 0.10 are also discussed.
Analyses involving symptom onset data were only possible from 2012 onwards for pulmonary cases, due to limited prior data.
All data preparation and analysis was conducted using Microsoft Excel 2010 and Stata version 13.1 (Stata Corp., College Station, TX, USA).
Results
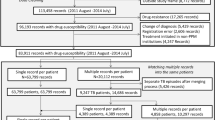
Of 5106 TB patients, 275 (5.4%) were seen exclusively by private healthcare providers, and 4714 (92.3%) by public. Excluded from analysis were patients who moved from private to public healthcare during their care (n = 18, 0.4%), those who moved from public to private care (n = 2, 0.04%), those for whom the healthcare service provider was unable to be classified due to missing data, patient transfer overseas or death before healthcare presentation (n = 97, 1.9%). The characteristics of TB patients attending private and public healthcare providers, and their treatment outcomes, are listed in Table 1.
There were several significant demographic and clinical differences between private and public patients. Those attending private health care were significantly older (p < 0.001), less likely to be born overseas (p = 0.001), less likely to have pulmonary involvement (p < 0.001) and more likely to have extrapulmonary TB (p < 0.001) (Table 1).
Multivariate logistic regression
Table 2 presents results of private healthcare provision as an independent variable in univariate and multivariate logistic regression analyses of laboratory tests, results, treatment and outcomes. Full tables of results are provided in the Additional file 1: Tables S1–S21.
In multivariate analysis, when compared to TB patients that attended public providers, patients who attended private providers were significantly less likely to have a genotypic investigation and were significantly less likely to have a sputum smear sample taken (for those with pulmonary involvement) and smear samples were less likely to be a positive. Private patients with extrapulmonary TB were significantly less likely to have a smear sample. Those with pulmonary involvement were significantly less likely to begin on treatment following an abnormal CXR and prior to other test results.
Patients who attended private healthcare providers were significantly more likely to receive fewer than four first-line medications, but there were no observed differences in treatment outcomes between public and privately treated patients.
Delays and survival analysis
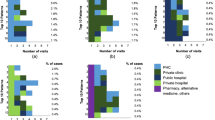
Considering the median delays (Table 3), log-rank and Kaplan-Meier survival curves (Figs. 2, 3 and 4), private patients did not commence treatment as promptly as patients that attended public healthcare providers. The only disparities that remained in Cox proportional hazard analysis were that private patients attended healthcare sooner after symptom onset than public patients, private extrapulmonary TB patients received radiological examinations less promptly than public patients and a significant interaction in the model of treatment initiation delay 1 indicated that private patients born in a high burden country with pulmonary involvement (n = 20) were not initiated on treatment as quickly as their public counterparts following an abnormal CXR (Table 3). Full tables of results are provided in the Additional file 1: Tables S22–S29.

Kaplan-Meier curves for TB patients with pulmonary involvement in Victoria from 2002 to 2015. a Health system delay. b Diagnostic delay to first CXR. c Treatment initiation delay 1

Kaplan-Meier curves for extrapulmonary TB patients in Victoria from 2002 to 2015. a Health system delay. b Diagnostic delay to first CXR

Kaplan-Meier curves for TB patients in Victoria. a Patient delay 2012–2015. b Laboratory delay 2011–2015. c Treatment initiation delay 2 2002-2015
Discussion
In our setting, there were differences in the care received by TB patients in private compared to public healthcare settings that are likely to reflect both differences in clinician practice and the case-mix managed. Private physicians were less likely to perform genotypic testing, take a sputum sample, and less likely to prescribe all four first-line medications. Patients attending private healthcare did so sooner after symptom onset, were less likely to have positive sputum specimens and certain groups did not receive assessments or commence treatment as promptly as public patients. Despite these disparities, treatment outcomes were comparable and no significant differences in health system delays to treatment commencement were found in Cox proportional hazard analyses.
The ability to distinguish patient delay from health system delays allowed us to demonstrate that in our setting public and private patients exhibited different health-seeking behaviour, with private patients attending sooner after symptom onset. Although it has been proposed that seeking medical care more promptly may indicate more severe disease and symptoms [26], our results were consistent with studies showing a negative association between symptom duration and smear-positivity [27, 28]. In our cohort, private patients with pulmonary involvement were less likely to have a smear-positive sputum sample than public patients, and extrapulmonary private patients were less likely to have an abnormal CXR, suggesting that private patients may present to healthcare with less severe disease. The degree to which the disparity in health-seeking behaviour reflects barriers that public patients experienced in accessing their care is unknown, and collection of more detailed qualitative information on health-seeking behaviour would be valuable.
Following healthcare attendance, several of our findings suggested that certain groups of private patients do not receive assessments or commence treatment as promptly as public patients. While it is possible these findings are due to differences in clinician practice, it may also reflect differing disease severity of the cohorts presenting to each provider type. For example, the lower likelihood of sputum examination in private patients may reflect a decreased ability to expectorate rather than clinician practice. Similarly, the fact that private extrapulmonary patients didn’t receive radiological examinations as promptly and certain groups took longer to commence treatment following an abnormal radiological result may be consistent with either 1) avoidable diagnostic delays, 2) logistical issues related to access to radiological and/or treatment, or 3) generally less severe presentations posing little risk of significant morbidity and disease transmission or greater diagnostic difficulty. While contributions from the first two possibilities cannot be discounted, the latter explanation is supported by investigation results among private patients indicating less severe disease and the fact that no significant health system delay was present overall, and treatment outcomes were comparable. From a public health perspective, the patterns of earlier presentation, less frequent smear-positivity and less severe disease also suggest a lower risk of transmission of infection.
Despite this, two of our findings, necessitate action due to the increasing incidence of multi-drug resistant TB (MDR-TB) in our setting, namely the less frequent use of genomic diagnostics and of a full complement of first-line drugs in private settings [20]. The VTP engages closely with both public and private physicians, so educational engagement will be possible across the sector to ensure improved uptake of genotypic testing and appropriate treatment regimens.
After adjustment for covariables (listed in the comments section of Table 3), we found no significant difference in health system or laboratory delays between public and private patients using Cox proportional hazard analysis. Similar analyses in other settings have revealed treatment delays by private providers and have proposed that these may be due to “deficiencies” [3], poorer knowledge regarding TB management [7, 8] or a lack of “effective diagnostic tools and follow-up routines” [2]. Although these factors may well be contributing, most previous studies did not consider important covariables, such as sputum smear status, which have previously been associated with health system delays [28] and that we found to be an important confounder in analyses of treatment commencement. A physician’s index of suspicion and their decision to commence treatment is inevitably influenced by their own knowledge, experience and biases, but also by factors beyond their control, including patient characteristics, manifestation, severity of disease and investigation results. These factors differed between public and private patients in our setting, and had an important influence on our results. Understanding the effect of such covariables is therefore important in any analysis of TB management.
The majority of studies comparing public and private settings have been performed in middle to high incidence settings that differ from ours. Factors associated with diagnostic and treatment delays may differ due to differing health systems, types of practitioners and health-seeking behaviour [4], so results are likely to be context-specific. In our setting, all TB patients, both public and private, are supervised and monitored by the VTP and TB medication is free– factors that have long been identified as leading to successful implementation of TB management [29]. The VTP has improved engagement with both public and private sectors over time, which allows comprehensive data collection, detailed analysis of care and effective feedback of results to practitioners. Our analyses showed that programmatic indicators such as treatment completion improved in our setting over the period of observation. In other settings, including many that have high TB burdens and growing private health sectors [30], we recognise that such engagement may be absent, data may be unavailable, and comprehensive and meaningful assessment of healthcare may be impossible. Fostering engagement between public and private healthcare sectors should therefore be the first priority in such settings. As has been noted, “private sector involvement might not be a bad thing in itself, but… public resources must be more effectively deployed for capturing and curating data of public interest from the private sector” [30].
As a well-resourced setting, we are privileged to have a large, well-curated dataset, and can provide a comprehensive analysis of TB management in both sectors, including treatment outcomes. However, we acknowledge the uncertainty inherent in any statistical analyses and the limitations of making multiple statistical comparisons, and urge caution in the interpretation of presented differences. Our study is also limited by the use of retrospective surveillance data and therefore subject to the influence of factors such as changes in data collection practices over time. Furthermore, analyses of some aspects of care were impossible due to small samples of private patients. We were also unable to include several covariables in analyses that have been shown to affect health system delays in some settings, including comorbidities [31] and education level [32]. However, the addition of comorbidities may further moderate disparities in diagnostic delay in our study, given the older age of private patients [33]. Further exploration regarding health-seeking behaviour and access to care, and the inclusion of outcomes such as relapse and the extent of onward transmission are planned.
Conclusions
We found small differences between public and private sectors in approach to care that are likely to reflect a differing case-mix as well as differing clinician practice. With the addition of covariables such as sputum smear status in Cox regression no significant differences in health system delays to treatment commencement were found, and treatment outcomes were comparable between public and private patients. The private sector is a significant provider of TB care globally [1]. In many countries, significant progress has been made in capturing notifications from the private sector, although considerable work is still required to foster communication and cooperation between sectors. Our study highlights the importance of having a TB program that engages well with both public and private providers, enabling comprehensive data collection that is necessary for thorough and true comparison of TB management and optimisation of care.
Abbreviations
- aOR:
-
Adjusted odds ratio
- CXR:
-
Chest x-ray/CT-scan
- HR:
-
Hazard ratio
- IQR:
-
Interquartile range
- lab:
-
Laboratory
- MDR-TB:
-
Multi-drug resistant TB
- NA:
-
Not applicable, not included in multivariate analysis, private p > 0.25 in univariate analysis
- obs:
-
Observations
- OR:
-
Odds ratio
- PHESS:
-
Public Health Event Surveillance System
- TB:
-
Tuberculosis
- VTP:
-
The Victorian TB program
References
World Health Organization. Global tuberculosis report, vol. 2016. Geneva: WHO Press, World Health Organization; 2016.
Storla DG, Yimer S, Bjune GA. A systematic review of delay in the diagnosis and treatment of tuberculosis. BMC Public Health. 2008;8:15.
Salinas J, Calvillo S, Cayla J, Nedel FB, Martin M, Navarro A. Delays in the diagnosis of pulmonary tuberculosis in Coahuila, Mexico. Int J Tuberc Lung Dis. 2012;16(9):1193–8.
Van Wyk SS, Enarson DA, Beyers N, Lombard C, Hesseling AC. Consulting private health care providers aggravates treatment delay in urban South African tuberculosis patients. Int J Tuberc Lung Dis. 2011;15(8):1069–76.
Lambert ML, Delgado R, Michaux G, Volz A, Speybroeck N, Van Der Stuyft P. Delays to treatment and out-of-pocket medical expenditure for tuberculosis patients, in an urban area of South America. Ann Trop Med Parasitol. 2005;99(8):781–7.
Sreeramareddy CT, Qin ZZ, Satyanarayana S, Subbaraman R, Pai M. Delays in diagnosis and treatment of pulmonary tuberculosis in India: a systematic review. Int J Tuberc Lung Dis. 2014;18(3):255–66.
Rifat M, Hall J, Oldmeadow C, Husain A, Milton AH. Health system delay in treatment of multidrug resistant tuberculosis patients in Bangladesh. BMC Infect Dis. 2015;15:526.
Belay M, Bjune G, Ameni G, Abebe F. Diagnostic and treatment delay among tuberculosis patients in afar region, Ethiopia: a cross-sectional study. BMC Public Health. 2012;12:369.
Belkina TV, Khojiev DS, Tillyashaykhov MN, Tigay ZN, Kudenov MU, Tebbens JD, Vlcek J. Delay in the diagnosis and treatment of pulmonary tuberculosis in Uzbekistan: a cross-sectional study. BMC Infect Dis. 2014;14:624.
Mahendradhata Y, Lestari T, Probandari A, Indriarini LE, Burhan E, Mustikawati D, Utarini A. How do private general practitioners manage tuberculosis cases? A survey in eight cities in Indonesia. BMC Res Notes. 2015;8:564.
Yimer SA, Holm-Hansen C, Bjune G. Assessment of knowledge and practice of private practitioners regarding tuberculosis control in Ethiopia. J Infect Dev Ctries. 2012;6(1):13–9.
Satyanarayana S, Subbaraman R, Shete P, Gore G, Das J, Cattamanchi A, Mayer K, Menzies D, Harries AD, Hopewell P, et al. Quality of tuberculosis care in India: a systematic review. Int J Tuberc Lung Dis. 2015;19(7):751–63.
Bell CA, Duncan G, Saini B. Knowledge, attitudes and practices of private sector providers of tuberculosis care: a scoping review. Int J Tuberc Lung Dis. 2011;15(8):1005–17.
Bronner Murrison L, Ananthakrishnan R, Sukumar S, Augustine S, Krishnan N, Pai M, Dowdy DW. How do urban Indian private practitioners diagnose and treat tuberculosis? A cross-sectional study in Chennai. PLoS One. 2016;11(2):e0149862.
Naseer M, Khawaja A, Pethani AS, Aleem S. How well can physicians manage tuberculosis? A public-private sector comparison from Karachi, Pakistan. BMC Health Serv Res. 2013;13:439.
Dato MI, Imaz MS. Tuberculosis control and the private sector in a low incidence setting in Argentina. Rev Salud Publica (Bogota). 2009;11(3):370–82.
Lonnroth K, Thuong LM, Lambregts K, Quy HT, Diwan VK. Private tuberculosis care provision associated with poor treatment outcome: comparative study of a semi-private lung clinic and the NTP in two urban districts in ho chi Minh City, Vietnam. National Tuberculosis Programme. Int J Tuberc Lung Dis. 2003;7(2):165–71.
Adejumo OA, Daniel OJ, Adejumo EN, Oluwole EO, Olumuyiwa OO. Treatment outcomes of tuberculosis patients managed at the public and private DOTS facilities in Lagos, Nigeria. Int J Trop Dis. 2015;10(2):1–9.
Australian Bureau of Statistics (ABS). 3101.0 - Australian demographic statistics, 2015 [http://www.abs.gov.au/ausstats/abs@.nsf/mf/3101.0]. Accessed 27 Feb 2017.
Toms C, Stapledon R, Waring J, Douglas P. Tuberculosis notifications in Australia, 2012 and 2013. Commun Dis Intell. 2015;38:4.
Dale K, Tay E, Trevan P, Denholm JT. Mortality among tuberculosis cases in Victoria, 2002-2013: case fatality and factors associated with death. Int J Tuberc Lung Dis. 2016;20(4):515–23.
Globan M, Lavender C, Leslie D, Brown L, Denholm J, Raios K, Sievers A, Kelly H, Fyfe J. Molecular epidemiology of tuberculosis in Victoria, Australia, reveals low level of transmission. Int J Tuberc Lung Dis. 2016;20(5):652–8.
Communicable Diseases Network Australia (CDNA). Tuberculosis case definition. [http://www.health.gov.au/internet/main/publishing.nsf/Content/cda-surveilnndss-casedefs-cd_tb.htm]. Accessed 27 Feb 2017.
Department of Health & Human Services: Management, control and prevention of tuberculosis guidelines for health care providers. 2015.
Hosmer DW, Lemeshow S, Sturdivant RX. Applied logistic regression. Chicester: Wiley; 2013.
El-Sony A, Enarson D, Khamis A, Baraka O, Bjune G. Relation of grading of sputum smears with clinical features of tuberculosis patients in routine practice in Sudan. Int J Tuberc Lung Dis. 2002;6(2):91–7.
Madebo T, Lindtjorn B. Delay in treatment of pulmonary tuberculosis: an analysis of symptom duration among Ethiopian patients. MedGenMed. 1999;1(1):E6.
Xu X, Liu JH, Cao SY, Zhao Y, Dong XX, Liang Y, Lu ZX. Delays in care seeking, diagnosis and treatment among pulmonary tuberculosis patients in Shenzhen, China. Int J Tuberc Lung Dis. 2013;17(5):615–20.
Lonnroth K, Uplekar M, Arora VK, Juvekar S, Lan NT, Mwaniki D, Pathania V. Public-private mix for DOTS implementation: what makes it work? Bull World Health Organ. 2004;82(8):580–6.
Byass P. Tuberculosis: a private and public health and data mix. Lancet Infect Dis. 2016;16(11):1206–1207.
Mor Z, Kolb H, Lidji M, Migliori G, Leventhal A. Tuberculosis diagnostic delay and therapy outcomes of non-national migrants in Tel Aviv, 1998-2008. Euro Surveill. 2013;18:12.
Mesfin MM, Newell JN, Walley JD, Gessessew A, Madeley RJ. Delayed consultation among pulmonary tuberculosis patients: a cross sectional study of 10 DOTS districts of Ethiopia. BMC Public Health. 2009;9:53.
Wu YC, Lo HY, Yang SL, Chou P. Factors correlated with tuberculosis reported after death. Int J Tuberc Lung Dis. 2014;18(12):1485–90.
Acknowledgements
The authors would like to acknowledge the support of the Department of Health and Human Services, the clinical nurse consultants of the Victorian Tuberculosis Program and the notifying clinicians and laboratories, including the Victorian Infectious Diseases Reference Laboratory. We also thank the Miller Foundation for funding.
Funding
This work was supported by the Miller Foundation Scholarship for Infection and Immunity, granted to Katie Dale towards her doctoral studies. The sponsors had no involvement in any aspect of the study or manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
JTD conceived the study and supervised KDD in conducting the study and drafting and revising the article. KDD performed data cleaning, analysis and wrote the article. ELT provided the raw data and assisted in data cleaning, analysis and in revising the article. JMT assisted in data analysis and revising the article, and PGT assisted in data interpretation and revising the article. All authors certify that they have participated sufficiently in the work; believe in its overall validity; are willing to take public responsibility for appropriate portions of its content; have seen and agreed to the submitted version of the paper; have agreed to their inclusion as an author; and acknowledge that the material is original and the article has not been published elsewhere, nor is it currently submitted elsewhere. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
As data in this study were collected and used under the legislative authority of the Public Health and Wellbeing Act 2008, approval from a Human Research Ethics Committee was not required under the rules of our institutions.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Dale, K.D., Tay, E.L., Trauer, J.M. et al. Comparing tuberculosis management under public and private healthcare providers: Victoria, Australia, 2002–2015. BMC Infect Dis 17, 324 (2017). https://doi.org/10.1186/s12879-017-2421-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-017-2421-x