
Abstract
Background
Bacterial resistance to antibiotics is an increasingly threatening consequence of antimicrobial exposure for many decades now. In urinary tract infections (UTIs), antibiotic prophylaxis (AP) increases bacterial resistance. We studied the resistance patterns of positive urinary cultures in spina bifida children on clean intermittent catheterization, both continuing and stopping AP.
Methods
In a cohort of 176 spina bifida patients, 88 continued and 88 stopped using AP. During 18 months, a fortnightly catheterized urine sample for bacterial pathogens was cultured. UTIs and significant bacteriuria (SBU) were defined as a positive culture with a single species of bacteria, respectively with and without clinical symptoms and leukocyturia. We compared the percentage of resistance to commonly used antibiotics in the isolated bacteria in both groups.
Results
In a total of 4917 cultures, 713 (14.5%) had a positive monoculture, 54.3% of which were Escherichia coli. In the group stopping AP, the resistance percentage to antibiotics in UTI / SBU bacteria was lower than in the group remaining on AP, even when excluding the administered prophylaxis.
Conclusion
Stopping antibiotic prophylaxis for urinary tract infections is associated with reduced bacterial resistance to antibiotics in children with spina bifida.
Trial registration
ISRCTN ISRCTN56278131. Registered 20 December 2005.
Similar content being viewed by others


Background
Due to increasing antibiotic use, bacterial resistance has emerged as an significant healthcare problem. The use of broader antibiotics for infections is driven by local antibiotic susceptibility and is influenced by preventive measures, use of antibiotic prophylaxis and previous antibiotic use.
Prior to the recent AAP Guidelines, there has been a trend to prescribe antibiotic prophylaxis (AP) to prevent recurrence of urinary tract infections (UTIs) and possible subsequent renal parenchymal scarring in otherwise healthy children and children with congenital abnormalities of kidney and urological tract [1]. The time-delay in culture results leads to the prescription of broad-spectrum antibiotics in suspicion of a UTI. Bacterial resistance for an increasing number of antibiotics is therefore seen in UTIs [2–5].
In children with spina bifida, renal insufficiency due to urological impairments and recurrent UTIs has been the major cause of morbidity and mortality [6]. The introduction of clean intermittent bladder catheterization (CIC) in 1972 by Lapides et al. enabled more adequate bladder emptying and a significant decline in UTIs, renal insufficiency and the need for kidney transplantation [7]. However, since the introduction of CIC, many clinicians started prescribing AP to prevent CIC-related UTIs [8–10]. Due to the lack of general guidelines on the use of AP for children with spina bifida applying CIC [11], caretakers were guided by the clinical course in the individual patient to either continue or stop AP.
To study the value of AP in children with spina bifida applying CIC, we conducted the SPIN UTI trial in the Netherlands and Belgium [12]. In this trial 176 patients were randomized to continue or to stop AP. Stopping AP resulted in significantly more non-febrile UTIs (relative risk 1.44, 95% confidence interval 1.13 – 1.83, p 0.003). However, the absolute risk of UTI was low: on average, AP has to be administered for more than two years to prevent one non-febrile, and therefore non-renal scarring UTI. The recommendation from this study was to start AP upon diagnosing spina bifida, and to stop AP as soon as vesico-ureteral reflux is excluded, overactive bladder symptoms are treated with anticholinergics and CIC is properly implemented. Only spina bifida patients with persisting high grade vesico-ureteral reflux and severe overactive bladder despite anticholinergic medication, which results in significantly more UTIs, may benefit from continuation of AP [12].
During the SPIN UTI study, catheterized urine samples of the 176 patients were investigated fortnightly for a period of 18 months by dip stick and subsequent culture only if the dip stick was positive. This resulted in almost 5000 cultures. In case of a positive culture with one strain of bacteria (monoculture), antimicrobial susceptibility was determined. The main aim of the present analysis was to study the difference in antimicrobial susceptibility in positive urine cultures between patients continuing and stopping AP. Our hypothesis was that children stopping prophylaxis would have better susceptibility of bacteria to commonly used antibiotics.
Methods
Patients
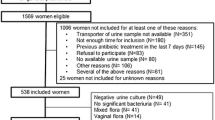
All patients with a meningomyelocele (spina bifida) known at the outpatient clinics of Wilhelmina’s Children’s Hospital in Utrecht, the Netherlands and Gasthuisberg University Hospital in Leuven, Belgium were eligible for inclusion in the study, provided they had been on CIC and AP during the last 6 months. One hundred and seventy-six patients participated in the study. The study period was from February 2005 until March 2009. This study was approved and registered by the ISRCTN, trial number 56278131 (http://bit.ly/2hvP2Uq).
Interventions
Patients were randomly allocated to continue or discontinue AP, using a computer based random concealed allocation scheme. Randomization was stratified for ages under and over 3 years, presence of vesico-ureteral reflux, gender and participating centre. Patients randomized to continuation of AP continued the individually prescribed type and dosage of antibiotics. The dosages and types were allowed to differ between patients according to antimicrobial susceptibility in pre-study cultures. Patients randomized to stopping of AP were instructed to discontinue the prescribed AP upon study start. The first urine sample was taken two weeks after stopping AP.
Follow-up, outcome measurements, primary outcome definition
During an 18 months follow-up period, fortnightly dip sticks and urine cultures were performed after CIC by the patients themselves, their parents or their primary care takers.
The dip stick for both urinary leukocytes and nitrite (Combur2-LN®, Roche Diagnostics) was rated either as negative (no color change) or as positive (any color change) by the primary care takers. If the dipstick was positive for leukocytes and / or nitrite, a urine culture was performed using a Uricult™ test (Orion Diagnostica, Finland) with MacConkey and CLED media.
In Utrecht, the Netherlands, the Uricult™ was sent to the laboratory of clinical microbiology of the University Medical Centre Utrecht for a 24 hour incubation period at 37 °C (98°F). If rated positive, the Uricult was subcultured on a sheep blood agar for 72 hours followed by identification to the species level by automated bacterial identification and automated antimicrobial susceptibility testing providing MICs (Phoenix, Becton & Dickinson, MD). Enterococcus species were identified to the genus level by selective growth on bile esculin agar (BEA) and salt tolerance agar (STA). Enterococcal antimicrobial susceptibility testing was performed with disk diffusion. CLSI breakpoints for MICs and disk diffusion were used for interpretation. When negative, the Uricult™ was not subcultured.
In Leuven, Belgium, the 24 hour incubation period was performed at home by the primary care takers (parents or nurses), using a feeding bottle warmer (Philips®) at 37 °C. If rated positive, the Uricult™ was sent to the laboratory of clinical microbiology for the incubation and identification process. When rated negative at home, the Uricult™ was sent to the trained research nurse for professional review. When she rated the Uricult™ positive, it was yet sent to the laboratory for incubation.
Significant bacteriuria (SBU) was defined as more than 10,000 colony forming units of a single specimen per milliliter in the catheterized urine sample. Urinary tract infection (UTI) was defined as an SBU combined with a positive reading of leukocyturia on the dip stick and clinical symptoms, such as increasing incontinence, foul smell or cloudiness of the catheterized urine. Cultures presenting more than one species of bacteria, regardless of clinical symptoms, were considered as a contamination rather than SBU or UTI.
To avoid repeated calculations for bacterial resistance patterns on one period of persistent SBU, we considered multiple consecutive positive cultures (SBU) without clinical signs of UTI, and therefore no antibiotic treatment, as one ongoing colonization.
Primary outcome
The primary outcome in this analysis was bacterial resistance of uropathogens in children with spina bifida on clean intermittent catheterization to commonly used antibiotics.
Statistical methods
Main treatment effect analyses were published previously [12]. In brief, differences in rates of UTI between the two treatment groups were analyzed using Poisson regression and pointed at no clinically relevant difference in risk of SBU/UTI after stopping AP.
The present analysis represents a secondary analysis of bacterial resistance patterns observed in incubated cultures of urine samples of children with spina bifida and SBU or UTI and the influence of AP. Bacterial species, type of AP used and antibiotic susceptibility (both AP and non-AP antibiotic) were described according to the randomization group (intention-to-treat) and according to the actual use of antibiotics (per protocol).
Prevalence of AP and non-AP resistance in positive urine cultures was calculated as the number of cultures with resistant pathogens divided by the total number of positive cultures. In this calculation we assumed independence of multiple cultures within patients, which was deemed appropriate given the fact that we only included incident episodes of SBU/UTI. Results were stratified for actual AP use (yes/no) and type of AP used.
Differences in prevalence of pathogenic resistance between cultures with and without AP were statistically tested using the Generalized Linear Mixed Model (GLMM) module of SPSS which takes into account the repeated assessments in patients. We applied the binary logistic link function and a random effect for the individual intercept. As primary predictor of interest we included AP use (yes/no) at the time of SBU/UTI to explore the effect of AP use on the risk of resistance against non-AP antibiotics. In addition we explored the effect of country (the Netherlands vs. Belgium), SBU or UTI and gender as potential confounders by adding these variables to the model with AP. Results from this analysis were expressed as odds ratio (OR) with 95% confidence intervals (95% CI).
All analyses were performed using SPSS, version 19.0 and statistical significance was accepted at a two-sided p-value of 0.05.
Results
Of the 176 participants, 88 were randomized to continue AP and 88 to stop using AP. In the latter group, 38 restarted AP during the 18 month study period, due to recurrent UTIs or specific parental request.
Not all patients complied with the fortnightly cultures in the entire study period of eighteen months. From a possible 6864 cultures if all 176 patients had complied with the protocol during the entire study period, 4917 urine samples were sent to and evaluated by the laboratories. Seven hundred and thirteen (14.5%) of these were positive single-strain cultures, of which 315 (44.2%) were considered a UTI due to clinical symptoms and leukocyturia on the dip stick. The remaining 398 (55.8%) were considered SBU, lacking clinical symptoms or leukocyturia (Table 1). No significant differences were seen between boys and girls.
The most common pathogen seen in about half of both SBU and UTI was Escherichia coli (E.coli) (54.3%). The other 45.7% consisted of other well-known uropathogens, like Klebsiella species (8.8%), Enterococcus species (7.9%), Pseudomonas aeruginosa (6.6%), Proteus mirabilis (4.8%) and 17.6% of less common pathogens (Table 1). Of the 713 single strain cultures only 82 (11.5%) were Gram-positive bacteria, mostly Enterococcus species and Staphylococcus aureus. Again, there were no differences between boys and girls in pathogens in either group.
Almost half of the cultures were performed in patients randomized to continue AP (n = 343, 48.1%), the remaining 370 cultures (51.9%) were from patients randomized to stopping AP. However, 79 (21%) cultures in the stop group were performed after AP was restarted due to recurrent UTIs or specific parental request. Thus, the majority of SBU and UTI occurred while using AP (N = 422, 59.2%), mostly trimethoprim and/or nitrofurantoin (Table 2).
Microbial resistance
Microbial resistance against any antibiotic was present in 65.2% of SBU/UTIs, and significantly more prevalent in urine cultures taken in children with spina bifida on AP (72.2%) than in children without AP (53.3%).
In Table 3, determination of resistance patterns to commonly used antibiotics performed on positive urinary cultures with Gram negative bacterial species, tested more than ten times in our patient group, is shown. There were too few Gram positive urinary cultures results to significantly differentiate resistance percentages between the groups on and off AP. The main result shown in this table is that use of AP increases the risk of resistance compared to stopping AP: the percentages of resistance to a specific antibiotic in any bacteria found in the urine cultures were higher when using AP. GLMM analysis estimated the risk of resistance against one or more antibiotics (including the AP) to be 2.3 (95% CI 1.6-3.1) fold higher while using AP relative to not using AP. Adding country, gender or type of culture (SBU or UTI) in the GLMM analysis did not change this estimate. Excluding resistance to the administered AP changed the estimate slightly to OR 1.7 (95% CI 1.2-2.3) for AP use relative to no AP use.
Table 2 depicts the association between type of AP on resistance patterns in 624 Gram negative cultures. Due to statistical insignificance, we left out the few Gram-negative cultures on other AP than trimethoprim, nitrofurantoin, ciprofloxacin or a combination of trimethoprim and nitrofurantoin.
Antibiogram of uropathogens and the influence of antibiotic prophylaxis on resistance
Penicillins
In our study cohort, resistance against amoxicillin and piperacillin was common with a overall prevalence of 66.7% and 68.2% in E.coli UTIs (Table 3). Stopping AP decreased the percentage of resistance in E.coli UTIs against amoxicillin and piperacillin from respectively 73.8 and 73.5% to 56.3% and 59.5%. Resistance against amoxicillin/clavulanic acid (29.7%) and piperacillin/tazobactam (7.8%) was less common in E. coli UTIs, as well as in other Gram negative UTIs. When discontinuing AP, the prevalence of resistance against amoxicillin/clavulanic acid and piperacillin / tazobactam decreased to respectively 22.7 and 5.5% (Table 2).
Cephalosporins
Gram negative bacteria such as E.coli showed moderate resistance for first and second generation cephalosporins (17.9% and 11.4% respectively) in our cohort of spina bifida patients, whereas for third generation cephalosporins E.coli had significantly lower resistance of 1.7-1.9% (Table 3). In UTIs with the uropathogen Klebsiella pneumoniae however, one in five is resistant to a third generation cephalosporin. Compared to not using AP, trimethoprim (0% and 5%) and nitrofurantoin alternating with trimethoprim (3% and 15%) as AP did not significantly influence resistance to second and third generation cephalosporins. However, the resistance for second generation cephalosporins increased significantly when using nitrofurantoin (21%) or ciprofloxacin (70%) as AP (Table 2).
Fluoroquinolones
In our cohort there was an overall low resistance of around 5% for fluoroquinolones in Gram negative bacteria while not using AP (Table 2). This was negatively influenced by prophylaxis: nitrofurantoin and trimethoprim prophylaxis doubled the resistance percentage (7.1 and 13.0% for ciprofloxacin respectively) (Table 2). When trimethoprim and nitrofurantoin were taken alternately, the resistance rate remained as low as without AP. The use of ciprofloxacin as AP was associated with a sharp increase in fluoroquinolones resistance (58.3-63.6%) (Table 2).
Trimethoprim/sulfamethoxazole
Even without AP, in our cohort E.coli bacteria had high resistance for both trimethoprim (42.9%) and trimethoprim/sulfamethoxazole (35.4%) (Table 3). Resistance obviously increased when using AP involved trimethoprim (90.1% and 77.7% respectively) (Table 2). Nitrofurantoin as AP however was not associated with increased resistance for trimethoprim (38.1%) or trimethoprim/sulfamethoxazole (30.7%) in Gram negative bacteria, whereas ciprofloxacin as AP only mildly increased resistance to trimethoprim (45.5%) and trimethoprim/sulfamethoxazole (33.3%) (Table 2).
Aminoglycosides
There was a low resistance rate for intravenous aminoglycosides in our cohort (3%), not influenced by AP nitrofurantoin (4%) or trimethoprim (3%). When using ciprofloxacin as AP, the Gram negative bacteria also remained sensitive to gentamicin, amikacin or tobramycin (Table 3).
Nitrofurantoin
Without AP, 13.2% of UTIs were resistant for nitrofurantoin treatment (Table 2). This resistance for nitrofurantoin treatment remained stable when using trimethoprim as AP (11.6%), while resistance significantly increased when using ciprofloxacin (77.8%) or nitrofurantoin itself (56.1%) as AP (Table 2).
The presence of resistance was not associated with age or gender. Microbial resistance against the prophylactic AP was not 100%: bacterial pathogens were still sensitive for treatment with the used AP in 43.9% of nitrofurantoin, 41.7% of ciprofloxacin and 9.5% of trimethoprim prescribed patients (Table 2).
Discussion
Bacterial resistance is an emerging and hazardous phenomenon occurring with ever-increasing use of antibiotics. Antibiotic prophylaxis (AP) administered to prevent recurrent urinary tract infections (UTIs) contributes to this resistance [13], although it has been proven that AP does not decrease the risk of renal scarring [1].
We compared bacterial susceptibility patterns in positive urine cultures in children with spina bifida and CIC continuing or stopping AP. Overall, our study showed a decrease in resistance to commonly used antibiotics when AP is stopped, confirming our hypothesis. Even when the administered AP is excluded from these calculations, the number of antibiotics to which the cultured pathogen is resistant remains higher in the continuing group. These findings in spina bifida patients on CIC is in accordance with previous studies for resistance patterns comparing AP to no AP in patients with community-acquired UTIs [14–18]. The fact that a particular class of antibiotics is associated with resistance towards other classes of antibiotics might be explained by the observation that bacterial resistance traits can be linked [19, 20].
E.coli accounts for 75-90% of community-acquired UTIs [21, 22], whereas E.coli is responsible for only 54.3% of the SBUs and UTIs in our specific population of children with spina bifida, with higher percentages of other uropathogens causing SBU/UTI. This difference is a common feature in non community-acquired UTIs, as described in previous studies in non-spina bifida patients, from Landhani et al (40% E.coli in children with underlying pathology), Lutter et al (58% E.coli in non-spina bifida children on AP) and Wagenlehner et al (35-60% E.coli in adult hospital-acquired UTIs due to catheterization with introduction of alternative pathogens) [15, 16, 23].
Choice of antibiotic prophylaxis in children with spina bifida
Our SPIN UTI study has shown that, whenever safe according to urological care, AP to prevent UTIs should be stopped in children with spina bifida. In a previous article we have shown that every child has to take two years of daily AP to prevent one extra non-febrile, non-scarring UTI [12], and this current study reveals a significant improvement in susceptibility to any necessary antibiotic treatment for a UTI when stopping AP. This article therefore emphasizes the necessity to stop the use of AP in children whenever possible to prevent bacterial resistance, especially since AP has proven not to prevent renal scarring [1].
When however, for reasons of recurrent UTIs, a persistent overactive bladder or high grade vesico-ureteral reflux, AP is a necessity, the choice of prophylaxis has impact on the bacterial resistance to commonly used therapeutic antibiotics. Trimethoprim as AP has the least negative influence on bacterial resistance: in our study cohort, the susceptibility of most therapeutic antibiotics remains relatively stable, except for fluoroquinolones, trimethoprim itself and trimethoprim/sulfamethoxazole. In our study, the use of nitrofurantoin as AP is associated with an increased resistance to cephalosporines, aminoglycosides and fluoroquinolones, with an increased risk of treatment failure, compared to non-AP patients. Particularly AP with fluoroquinolones is associated with a high percentage of resistance, especially to therapeutic oral antibiotic possibilities when necessary, and should therefore be discouraged.
Choice of therapeutic antibiotics in children with spina bifida
First consideration in choosing an appropriate antibiotic when a UTI is suspected or confirmed is the manner of administration: when clinically not ill, oral antibiotic treatment is adequate, whilst in sick children with spina bifida due to a UTI intravenous administration of antibiotics is often necessary. This determines the choice of antibiotic treatment, along with previous culture results and resistance patterns, presence or absence of fever and recently prescribed AP. In our study cohort, nitrofurantoin is first choice medication for a UTI without fever or recent AP. Without fever but with prophylaxis, in children with trimethoprim as AP nitrofurantoin is still first choice. In other AP and in children with fever on or off AP, oral treatment for UTI depends on local susceptibility, with ciprofloxacin and cefuroxim as antibiotics with high a priori chance of treatment success in our study cohort. When intravenous treatment is warranted, a third generation cephalosporin, fluoroquinolon or carbapenem is possible. However, we emphasize that the choice of therapeutic antibiotics depends on local susceptibility and individual resistance patterns in previous urinary cultures.
The strength of this study is the large number of adequate catheterized urinary cultures in a cohort of susceptible children with spina bifida. Remarkable is the relatively high percentage of susceptibility of bacteria for the already administered AP.
Conclusion
Discontinuation of antibiotic prophylaxis decreases bacterial resistance for commonly used antibiotics in children with spina bifida on clean intermittent catheterization should be pursued to prevent bacterial resistance, long term side effects of prophylactic antibiotics and the need for hospital admissions for broad spectrum intravenous antibiotics.
Abbreviations
- AP:
-
Antibiotic prophylaxis
- CI:
-
Confidence interval
- CIC:
-
Clean intermittent catheterization
- GLMM:
-
Generalized Linear Mixed Model
- OR:
-
Odds ratio
- SBU:
-
Significant bacteriuria
- UTI:
-
Urinary tract infection
References
RIVUR Trial Investigators, Hoberman A, Greenfield SP, Mattoo TK, Keren R, Mathews R, Pohl HG, Kropp BP, Skoog SJ, Nelson CP, Moxey-Mims M, Chesney RW, Carpenter MA. Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med. 2014;370(25):2367–76.
Dayan N, Dabbah H, Weissman I, Aga I, Even L, Glikman D. Urinary tract infections caused by community-acquired extended-spectrum beta-lactamase-producing and nonproducing bacteria: a comparative study. J Pediatr. 2013;163(5):1417–21.
Ilic K, Jakovljevic E, Skodric-Trifunovic V. Social-economic factors and irrational antibiotic use as reasons for antibiotic resistance of bacteria causing common childhood infections in primary healthcare. Eur J Pediatr. 2012;171(5):767–77.
Shepherd AK, Pottinger PS. Management of urinary tract infections in the era of increasing antimicrobial resistance. Med Clin North Am. 2013;97(4):737–57. xii.
Beetz R, Westenfelder M. Antimicrobial therapy of urinary tract infections in children. Int J Antimicrob Agents. 2011;38(Suppl):42–50.
Pruitt LJ. Living with spina bifida: a historical perspective. Pediatrics. 2012;130(2):181–3.
Lapides J. Urinary diversion. Surgery. 1971;69(0039-6060; 0039-6060; 1):142–54.
Schlager TA, Dilks S, Trudell J, Whittam TS, Hendley JO. Bacteriuria in children with neurogenic bladder treated with intermittent catheterization: natural history. J Pediatr. 1995;126(0022-3476; 3):490–6.
Schlager TA, Anderson S, Trudell J, Hendley JO. Nitrofurantoin prophylaxis for bacteriuria and urinary tract infection in children with neurogenic bladder on intermittent catheterization. J Pediatr. 1998;132(0022-3476; 4):704–8.
Dik P, Klijn AJ, van Gool JD, de Jong-de Vos van Steenwijk CC, De Jong TP. Early start to therapy preserves kidney function in spina bifida patients. Eur Urol. 2006;49(0302-2838; 5):908–13.
Zegers BS, Winkler-Seinstra PL, Uiterwaal CS, de Jong TV, Kimpen JL, van de Jong-de Vos van Steenwijk CC. Urinary tract infections in children with spina bifida: an inventory of 41 European centers. Pediatr Nephrol. 2009;24(0931-041; 4):783–8.
Zegers B, Uiterwaal C, Kimpen J, van Gool J, de Jong T, Winkler-Seinstra P, Houterman S, Verpoorten C, de Jong-de Vos van Steenwijk C. Antibiotic prophylaxis for urinary tract infections in children with spina bifida on intermittent catheterization. J Urol. 2011;186(6):2365–70.
Bitsori M, Maraki S, Galanakis E. Long-term resistance trends of uropathogens and association with antimicrobial prophylaxis. Pediatr Nephrol. 2014;29(6):1053–8.
Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. JAMA. 2007;298(1538-3598; 2):179–86.
Lutter SA, Currie ML, Mitz LB, Greenbaum LA. Antibiotic resistance patterns in children hospitalized for urinary tract infections. Arch Pediatr Adolesc Med. 2005;159(10):924–8.
Ladhani S, Gransden W. Increasing antibiotic resistance among urinary tract isolates. Arch Dis Child. 2003;88(1468-2044; 5):444–5.
Narchi H, Al-Hamdani M. Uropathogen resistance to antibiotic prophylaxis in urinary tract infections. Microb Drug Resist. 2010;16(1931-8448; 1076-6294; 2):151–4.
Nelson CP, Hoberman A, Shaikh N, Keren R, Mathews R, Greenfield SP, Mattoo TK, Gotman N, Ivanova A, Moxey-Mims M, Carpenter MA, Chesney RW: Antimicrobial Resistance and Urinary Tract Infection Recurrence. Pediatrics 2016, 137(4):10.1542/peds.2015-2490. Epub 2016 Mar 11.
Stokes HW, Gillings MR. Gene flow, mobile genetic elements and the recruitment of antibiotic resistance genes into Gram-negative pathogens. FEMS Microbiol Rev. 2011;35(5):790–819.
Alekshun MN, Levy SB. Molecular mechanisms of antibacterial multidrug resistance. Cell. 2007;128(6):1037–50.
Friedman S, Reif S, Assia A, Mishaal R, Levy I. Clinical and laboratory characteristics of non-E. coli urinary tract infections. Arch Dis Child. 2006;91(10):845–6.
Edlin RS, Shapiro DJ, Hersh AL, Copp HL. Antibiotic resistance patterns of outpatient pediatric urinary tract infections. J Urol. 2013;190(1):222–7.
Wagenlehner FM, Cek M, Naber KG, Kiyota H, Bjerklund-Johansen TE. Epidemiology, treatment and prevention of healthcare-associated urinary tract infections. World J Urol. 2012;30(1):59–67.
Funding
Full funding was provided by the Wilhelmina Children’s Hospital’s Scientific Foundation at the University Medical Center Utrecht, the Netherlands.
Availability of data and materials
All SPSS-data from this study are available on request for interested and registered colleagues through the corresponding author.
Authors’ contribution
SZ, JK and CJ had a substantial contribution to conception, design, acquisition of data, analysis and interpretation of data. SZ, JD and TB were involved in drafting and revising the manuscript. JK and CJ provided the final approval of the manuscript. All authors read and approved the final manuscript.
Competing interests
All authors state no conflict of interest due to financial, consultant, institutional or other relationships.
Ethics approval and consent to participate
Ethical approval has been granted by the Medical Ethical Committee of the University Medical Center in Utrecht, the Netherlands and the University Hospital Gasthuisberg in Leuven, Belgium. We have gathered informed consent to participate in this study and to publish the date from all participating patients’ parents.
Author information
Authors and Affiliations
Corresponding author
Additional information
The original version of this article was revised: To delete a duplicated author name from the author list.
An erratum to this article is available at http://dx.doi.org/10.1186/s12879-017-2268-1.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zegers, S.H.J., Dieleman, J., van der Bruggen, T. et al. The influence of antibiotic prophylaxis on bacterial resistance in urinary tract infections in children with spina bifida. BMC Infect Dis 17, 63 (2017). https://doi.org/10.1186/s12879-016-2166-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-016-2166-y