
Abstract
Background
Enterohemorrhagic Escherichia coli (EHEC) is an important cause of gastroenteritis in Japan. Although non-O157 EHEC infections have been increasingly reported worldwide, their impact on children has not been well described.
Methods
We collected national surveillance data of EHEC infections reported between 2010 and 2013 in Japan and characterized outbreaks that occurred in childcare facilities. Per Japanese outbreak investigation protocol, faecal samples from contacts of EHEC cases were collected regardless of symptomatic status. Cases and outbreaks were described by demographics, dates of diagnosis and onset, clinical manifestations, laboratory data, and relation to specific outbreaks in childcare facilities.
Results
During 2010–2013, a total of 68 EHEC outbreaks comprised of 1035 cases were related to childcare facilities. Among the 66 outbreaks caused by a single serogroup, 29 were serogroup O26 and 22 were O157; 35 outbreaks were caused by stx1-producing strains. Since 2010, the number of reported outbreaks steadily increased, with a rise in cases and outbreaks caused by stx1-producing O26. Of 7069 EHEC cases reported nationally in 2010–2011, the majority were caused by O157 (n = 4938), relative to O26 (n = 1353) and O111 (n = 195). However, relative to 69 cases of O157 (2 %) associated with childcare facility EHEC outbreaks, there were 131 (10 %) such cases of O26, and this trend intensified in 2012–2013 (O157, 3 %; O26, 24 %; O111, 48 %). Among family members of childcare facility cases, the proportion of cases that were symptomatic declined with age; 10/16 cases (63 %) aged 6 years or younger, 16/53 cases (30 %) 6–19 years old, 23/120 cases (19 %) 20–49 years old and 2/28 cases (7 %) 50 years or older were symptomatic. Thirty one of the 68 outbreaks (46 %) were classified as foodborne-related.
Conclusions
Childcare facility EHEC outbreaks due to non-O157 serogroups, particularly O26 and O111, increased during 2010–2013. These facilities should pay extra attention to health conditions in children. As older family members of childcare facility cases appear to be less symptomatic, they should be vigilant about hand-washing to prevent further transmission.
Similar content being viewed by others


Background
Enterohemorrhagic Escherichia coli (EHEC) is known to cause diarrhea and hemorrhagic colitis in humans [1]. Vulnerable populations of EHEC infection include small children and the elderly. Severe cases are reported more often in children than in adults (under 65 years of age), and may include life-threatening hemolytic uremic syndrome (HUS) [2]. EHEC cases in outbreaks have predominantly been attributed to EHEC O157:H7; however, recent studies have reported an increased in the number of cases affected by non-O157 serogroups, including O26, O103, O111, and O145 [3]. Non-O157 E. coli strains have been isolated from patients in the USA [4], Europe [5, 6], Australia [7], New Zealand [8], and Japan [9]. Notably, non-O157 E. coli tended to affect younger children more often than O157 in the USA [4].
EHEC outbreaks in childcare facilities have been reported from several countries [10–19]. Higher rates of secondary transmission have been detected in EHEC O157 outbreaks among people with a median age of less than 6 years compared with those with a median age of 6–59 years [12]. Although information regarding non-O157 outbreaks in childcare settings have been limited, non-O157 infections seem to occur more frequently than O157 infections in childcare facilities [13–19]. However, the reasons remain unknown and there is no consensus regarding how these outbreaks should be controlled.
EHEC is a notifiable disease in Japan and approximately 4000 EHEC cases are reported annually in the country, including outbreaks associated with childcare facilities [16–19]. After being notified of a case by a physician, Local Public Health Centers (LPHCs) conduct active case-finding among contacts of case patients as described previously [20]. LPHC staff interview contacts about their health status, collect their faecal specimens (regardless of symptomatic status), and monitor their health status. Such protocol is designed to allow for rapid and timely reporting of outbreaks, including those associated with childcare facilities, through the National Epidemiological Surveillance of Infectious Diseases (NESID) system from each LPHC. In August 2013, an increase in the reported number of EHEC outbreaks in childcare facility settings was noted, especially after 2012. Although more than 2.2 million children attending childcare facilities are at potential risk of EHEC infection [21], the overall picture on outbreaks in these settings has yet to be determined.
We describe a recent increase in the number of reported EHEC outbreaks related to childcare facilities in Japan based on analysis of national surveillance data. We discuss the outbreaks in terms of number of outbreaks and cases, proportion of symptomatic cases among cases detected through active investigations, characteristics of isolated serogroups and stx types, and mode of transmission.
Ethics
This study was conducted by the Act on Prevention of Infections and Medical Care for Patients with Infections in Japan. Thus, this study did not require approval from an ethics committee.
Methods
Data collection
EHEC infection is a notifiable disease in Japan, requiring an immediate report after diagnosis per “Act on Prevention of Infections and Medical Care for Patients with Infections”. Local governments collect and submit case-based data via NESID to the Ministry of Health, Labour and Welfare (MHLW). For the present study, the following data were extracted from NESID: dates of notification, age, sex, occupation, clinical manifestations, serogroup and stx type from isolated EHEC strains, suspected route of infection (foodborne, direct contact, both foodborne and direct contact, or unspecified, as indicated by the reporting physicians and LPHC), and relationship to a specific outbreak in a childcare facility.
A symptomatic case was defined as EHEC infection confirmed by culture and serological testing for anti-Shiga toxin (stx) antibody or Polymerase Chain Reaction (PCR), after the development of at least one gastrointestinal illness, such as watery diarrhea, abdominal pain or cramps, bloody diarrhea, or vomiting. The presence of Shiga toxin in stool samples was confirmed by enzyme immunoassay or PCR. Standardized methods for laboratory tests are recommended to LPHCs under the guidance of the National Institute of Infectious Diseases, based on guidelines from World Health Organization for Escherichia coli and Klebsiella [22]. An asymptomatic case was defined as an EHEC infection confirmed by the laboratory tests described above for symptomatic cases, detected by active case finding during outbreak investigation or from routine screenings required in designated occupations (e.g. food handler, nursery school employee).
Childcare facility-related EHEC outbreaks
Per Japanese outbreak investigation protocol, after being notified of a case by a physician, LPHCs conduct active case-finding among contacts of case patients. When symptomatic EHEC cases are detected at a childcare facility, asymptomatic children at the same facility are screened by the laboratory tests described above. For our study, an outbreak at a childcare facility was defined as a cluster of at least two cases aged less than 7 years, attending the same childcare facility, affected by the same EHEC serogroup and stx type, reported from the same LPHC, and occurring within 3 weeks of diagnosis (approximately double the 10 days-incubation period). Outbreak-related cases were defined as cluster cases described above and cases with the same serogroup and stx as the cluster cases, and sharing the same information as cluster cases for any of the following: belonged to the same family, living in the same household, or epidemiologically linked to the same childcare facility or cluster. The suspected route of infection was indicated by the reporting physicians and LPHCs and categorized as either foodborne, direct contact, or unspecified.
All descriptive statistical analyses were based solely on the extracted NESID surveillance data. Based on the extracted data, cases reported during the period when an increase in EHEC outbreaks in childcare facilities was observed (2012–2013) were compared to an immediately prior period of the same length (2010–2011).
Results
Reported number of EHEC cases and childcare facility outbreaks
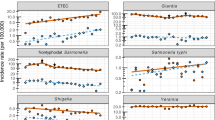
Approximately 4000 EHEC cases were reported annually, peaking consistently at around epidemiological week 30 during 2010–2013 (Fig. 1). We identified 1035 outbreak-related cases among the 68 childcare facility outbreaks that occurred during this period. The number of outbreaks doubled during 2010–2013 and outbreak-related cases increased steadily over this period (Table 1). The increase in number of cases per outbreak in 2011–2013 was largely due to an increase in asymptomatic cases. However, the median number of symptomatic cases per outbreak remained the same (4, range: 1–15 for 2010–2011 and 1–47 for 2012–2013); moreover, in 2012–2013 there were 3 large scale outbreaks with more than 15 symptomatic cases compared to none in 2010–2011. Among the 68 outbreaks, 65 (96 %) outbreaks occurred between epidemiological weeks 22 and 50.

Epidemiological curve of EHEC cases in childcare facility-related outbreaks in Japan, 2010–2013. EHEC cases in childcare facility-related outbreaks are shown by week of diagnosis during 2010–2013 in black (indicated as Outbreak-related cases); total EHEC cases for the same period are shown in grey (indicated as Total cases)
Majority of EHEC cases in 2010–2013 were caused by six serogroups (O26, O157, O111, O103, O121 and O145). While O157 was responsible for the majority of EHEC cases with a single serogroup and stx1 and/or stx2 type identified (4938/7069), O26 was the major serogroup among childcare-facility outbreaks (131/218), with 1 % of O157 cases vs. 10 % of O26 cases being outbreak-related (Table 2). This contrast between O157 and O26 became greater in 2012–2013 (2 % and 24 %, respectively). There were no childcare facility outbreaks associated with O111 in 2010–2011, but 173 O111 outbreak-related cases were reported in 2012–2013. Moreover, the proportion of O111 outbreak-related cases reached 48 % in 2012–2013.
Characteristics of cases related to childcare facility outbreaks
Among a total of 1035 outbreak-related cases, 484 (47 %) were male and the median age was 4 years (range: 0–88 years) (Table 3). A total of 761 (74 %) cases were cluster cases, i.e. pediatric cases who were attending the childcare facilities that had an outbreak. Of 761 cases, 329 (43 %) were symptomatic. The majority of the remaining outbreak-related cases were family members, and the majority of family members were aged 20–49 years (120 cases). In 2010–2011, older age groups were less likely to be symptomatic than other family members. For example, 60 % of siblings of cluster cases less than 7 years old and with no evidence of going to the same childcare facility were symptomatic, while all 16 family members over 50 years old were asymptomatic. This trend continued in 2012–2013, when this youngest age group remained more likely to be symptomatic (64 %) than cases 7–19 and 20–49 years of age (23 % and 10 %, respectively). During both 2010–2011 and 2012–2013, among family member cases, age was inversely associated with being symptomatic, with only 7 % of those 50 years and older being symptomatic during 2010–2013 (Table 3). Four HUS cases were reported during 2010–2013; all four were less than 7 years old and affected by O157 that had both stx1 and stx2 and recorded in three outbreaks in 2013. Based on the available information among symptomatic cases, the longest interval between the onsets of cases in these outbreaks was 18 days.
Serogroups and stx types of the isolated EHEC strains in the childcare facility outbreaks
Among outbreaks caused by a single serogroup (n = 66; excluding two O26/O103 co-infection outbreaks), the stx1-producing strain was the most predominant (35/66, 53 %) (Table 4); 19/66 (29 %) outbreaks were associated with both the stx1- and stx2-producing strains and 12/66 (18 %) outbreaks were associated with the stx2-producing strain. Considering both Serogroups and stx types, O26 stx1 accounted for the largest proportion (26/66, 39 %), followed by O157 stx1 and stx2 (14/66, 21 %) and O157 stx2 (7/66, 11 %). During 2012–2013, there was a greater increase in both the number of cases and outbreaks associated with O26 relative to those associated with O157, particularly for stx1-producing O26 (Table 4).
Mode of transmission
Among the 68 outbreaks, suspected transmission routes were direct contact (24 outbreaks, 35 %), both foodborne and direct contact (24 outbreaks, 35 %), foodborne (7 outbreaks, 10 %), and unspecified (13 outbreaks, 19 %).
Discussion
In this study, we identified 68 EHEC outbreaks associated with childcare facilities in Japan from 2010 to 2013. Notably, the proportion of cases associated with outbreaks varied by serogroup (Table 2). In particular, the number of such outbreaks increased in 2012–2013. O26 stx1 cases comprised the majority of cases related to such outbreaks (39 % of outbreaks) during the period and contributed to much of the increase. O111 cases were also associated with childcare facility outbreaks and nearly half of all reported O111 cases were related to such outbreaks that occurred during 2012–2013 (Table 2). O157, however, appeared to be much less associated with such outbreaks. Fortunately, stx1-producing O26 is known to be less severe than O157 [2]. In fact, all four reported HUS cases during the study period were among O157 infections and much of the increase in outbreak-related cases was associated with an increase in asymptomatic cases. Family members, particularly older persons, of cases that were attending childcare facilities were less likely to be symptomatic. To our knowledge, this is the first study to show profiles of childcare facility-related EHEC outbreaks in Japan.
These results suggest that certain non-O157 strains, such as O111 and O26, may be more likely to occur in childcare facility settings and could indicate transmission concerns in these settings, particularly given the presence of asymptomatic cases. In fact, direct contact was the suspected route of transmission of EHEC infections in 48 of the 68 outbreaks (direct contact in 24 outbreaks and both foodborne and direct contact in 24 outbreaks), relative to foodborne transmission suspected in 31 outbreaks (foodborne in 7 outbreaks and both foodborne and direct contact in 24 outbreaks). Majority of adult family member cases were asymptomatic, particularly those over 50 years of age. Taken together, we speculate that a sizable proportion of adolescent and adults were unaware of their EHEC infection, and could transmit the infection to other family members, including their children, before control measures could be undertaken. Thus, adolescents and adults in close contact with young children should be vigilant about hand-washing even if they do not notice any signs or symptoms of gastroenteritis themselves. In particular, as O26, the most frequent serogroup detected among childcare facilities, tends to be more asymptomatic than O157, asymptomatic cases may contribute to further spread, resulting in larger outbreaks.
As EHEC shedding is known to be relatively long lasting, earlier detection of events and rapid outbreak investigations are important in minimizing the number of infected cases and reducing potential further spread. While only few studies have assessed such information, long duration of shedding has been documented for several EHEC serotypes. The duration of shedding ranged from 15 to 46 days in an EHEC O26 outbreak in the USA [15]. Shedding periods of up to 71 days were found in an EHEC O145 outbreak in a Norwegian childcare center [23]. Furthermore, a sensitive detection method used in a German outbreak showed that shedding lasted up to 62 days in those with diarrhea or hemorrhagic colitis [24]. Moreover, some outbreaks in Japan were difficult to control quickly, taking a mean of 46.5 days (range: 32–63) after the onset of index cases, partly due to secondary infections [25], emphasizing the need for early detection to prevent transmission. Family members are also affected by childcare facility-related cases, and while the direction of transmission between family members and cases in childcare facilities is unknown, proper hand washing and hygiene practice are important in households.
While the O157 serogroup is known for its severity, the United States Department of Agriculture pointed out that awareness of non-O157 serogroups as a food safety concern has increased in the USA and added six non-O157 serogroups (O26, O45, O103, O111, O121, and O145) to the list of pathogens that should be considered to be of public health importance [26]. Indeed, while O26 serogroup is known to be relatively less severe, concerns regarding O26 are starting to emerge. For example, a novel type of O26 clone harboring the stx2 gene was found in Germany, and has been spreading across Europe, the USA, and South America [5, 27–30]. These studies suggested that stx2-producing O26 might be a more virulent type, and could pose a threat to children in childcare facilities in Japan and in other countries. The stx2-producing strain of O157 can also result in severe outcomes, including HUS [2]. The second major serogroup in our study was stx2-producing EHEC O157, and indeed, all four HUS cases detected in our study were affected by stx1 and stx2-producing O157.
A key limitation in our study is understanding the reason why childcare facility-related non-O157 outbreaks have increased, which remains unclear from national surveillance-based analysis. As the increase was associated with increase in asymptomatic cases, possibility of enhanced outbreak investigations at child care facilities exist. However, there was no change in policy for diagnostic practices or surveillance criteria. Moreover, while the median number of symptomatic cases per outbreak remained the same, there was an increase in large scale outbreaks in 2012–2013. In addition, while specific alerts regarding childcare facility-related EHEC outbreaks were distributed from MHLW to LPHCs in late August 2013, this notification was based on increased EHEC cases from NESID data; thus, it cannot explain the increase in the number of outbreaks in 2012 or the increase during the period up to August in 2013, when the number of outbreaks had already reached almost twice as many as that in 2012.
Conclusions
In Japan, the reported frequency of EHEC outbreaks and cases related to childcare facilities, especially those with non-O157 strains, have been increasing. Once infections with non-O157 serogroups in childcare facilities are recognized, family members should be vigilant about hand washing to prevent further transmission. Early detection and response is required to minimize the extent of outbreaks, and further investigation into the potential reasons of the increase in such outbreaks is warranted.
Abbreviations
- EHEC:
-
Enterohemorrhagic Escherichia coli
- HUS:
-
Hemolytic uremic syndrome
- stx :
-
Shiga toxin
- NESID:
-
National Epidemiological Surveillance of Infectious Diseases
- MHLW:
-
Ministry of Health Labour and Welfare
References
Gerald L, Mandell JE, Bennett RD. Principles and practice of infectious diseases. London: Churchill Livingstone; 2009.
Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet. 2005;365:1073–86.
Johnson KE, Thorpe CM, Sears CL. The emerging clinical importance of non-O157 Shiga toxin-producing Escherichia coli. Clin Infect Dis. 2006;43:1587–95.
Centers for Disease Control and Prevention. National Enteric Disease Surveillance: Shiga toxin-producing Escherichia coli (STEC) Annual Report, 2011. Available at http://www.cdc.gov/ncezid/dfwed/PDFs/national-stec-surv-summ-2011-508c.pdf.
Käppeli U, Hächler H, Giezendanner N, Beutin L, Stephan R. Human infections with non-O157 Shiga toxin-producing Escherichia coli, Switzerland, 2000–2009. Emerg Infect Dis. 2011;17:180–5.
Friesema I, van der Zwaluw K, Schuurman T, Kooistra-Smid M, Franz E, van Duynhoven Y, et al. Emergence of Escherichia coli encoding Shiga toxin 2f in human Shiga toxin-producing E. coli (STEC) infections in the Netherlands, January 2008 to December 2011. Eurosurveillance. 2014;19:26–32.
Vally H, Hall G, Dyda A, Raupach J, Knope K, Combs B, et al. Epidemiology of Shiga toxin producing Escherichia coli in Australia, 2000–2010. BMC Public Health. 2012;12:63.
Jaros P, Cookson AL, Campbell DM, Besser TE, Shringi S, Mackereth GF, et al. A prospective case–control and molecular epidemiological study of human cases of Shiga toxin-producing Escherichia coli in New Zealand. BMC Infect Dis. 2013;13:450.
Hiroi M, Takahashi N, Harada T, Kawamori F, Iida N, Kanda T, et al. Serotype, Shiga toxin (Stx) type, and antimicrobial resistance of Stx-producing Escherichia coli isolated from humans in Shizuoka Prefecture, Japan (2003–2007). Jpn J Infect Dis. 2012;65:198–202.
Bielaszewska M, Mellmann A, Bletz S, Zhang W, Köck R, Kossow A, et al. Enterohemorrhagic Escherichia coli O26:H11/H-: A new virulent clone emerges in Europe. Clin Infect Dis. 2013;56:1373–81.
Gallagher L, Soyemi K, Conover C, Austin C, Saathoff-Huber L, Nelson S, et al. Outbreak of Escherichia coli O157:H7 in a child care center in Cook County, Illinois, with prolonged shedding and household transmission. Am J Infect Control. 2013;41:936–8.
Snedeker KG, Shaw DJ, Locking ME, Prescott RJ. Primary and secondary cases in Escherichia coli O157 outbreaks: a statistical analysis. BMC Infect Dis. 2009;9:144.
Brown J, Hite D, Gillim-Ross L, Maguire H, Bennett J, Patterson J, et al. Outbreak of shiga toxin-producing Escherichia coli serotype O26: H11 infection at a child care center in Colorado. Pediatr Infect Dis J. 2012;31:379–83.
Møller-Stray J, Eriksen HM, Bruheim T, Kapperud G, Lindstedt BA, Skeie Å, et al. Two outbreaks of diarrhoea in nurseries in Norway after farm visits, April to. Eurosurveillance. 2009;2012:1–7.
Tourdjman M, Hostetler T, Reuer J, Ciaffoni C, Cieslak P, Lewis P, Leman R: Duration of Shedding and Secondary Household Transmission of Shiga Toxin – Producing Escherichia coli O26 During an Outbreak in a Childcare Center, Oregon, October – December 2010. J Pediatric Infect Dis Soc 2012;1:329–332.
Iizuka S, Tsunomori Y, Tabara K, Tsuda K, Fukuma T. An outbreak of mixed infection of enterohemorrhagic Escherichia coli O26:H11 and norovirus genogroup II at a kindergarten in Shimane, Japan. Jpn J Infect Dis. 2005;58:329–30.
Kanazawa Y, Ishikawa T, Shimizu K, Inaba S. Enterohemorrhagic Escherichia coli outbreaks in nursery and primary schools. Jpn J Infect Dis. 2007;60:326–7.
Sonoda C, Tagami A, Nagatomo D, Yamada S, Fuchiwaki R, Haruyama M, et al. An Enterohemorrhagic Escherichia coli O26 Outbreak at a Nursery School in Miyazaki, Japan. Jpn J Infect Dis. 2008;61:92–3.
Hiruta N, Murase T, Okamura N. An outbreak of diarrhoea due to multiple antimicrobial-resistant Shiga toxin-producing Escherichia coli O26:H11 in a nursery. Epidemiol Infect. 2000;127:221–7.
Yahata Y, Misaki T, Ishida Y, Nagira M, Watahiki M, Isobe J, et al. Epidemiological analysis of a large enterohaemorrhagic Escherichia coli O111 outbreak in Japan associated with haemolytic uraemic syndrome and acute encephalopathy. Epidemiol Infect. 2015;20:1–12.
Ministry of Health, Labour and Walfare: Data on chid-care facilities in Japan as of 1 April, 2013 [http://www.mhlw.go.jp/file/04-Houdouhappyou-11907000-Koyoukintoujidoukateikyoku-Hoikuka/0000022681.pdf]. (in Japanese)
WHO Collaborating Centre for Reference and Research on Escherichia and Klebsiella: Identification of three vtx1 and seven vtx2 subtypes of Verocytotoxin encoding genes of Escherichia coli by conventional PCR amplification. Copenhagen, Denmark: Statens Serum Institut. http://www.ssi.dk/~/media/Indhold/EN%20-%20engelsk/Public%20Health/National%20Reference%20Laboratories/vtx%20detection%20%20subtyping%20protocolrev6final.ashx.
Wahl E, Vold L, Lindstedt BA, Bruheim T, Afset JE. Investigation of an Escherichia coli O145 outbreak in a child day-care centre--extensive sampling and characterization of eae- and stx1-positive E. coli yields epidemiological and socioeconomic insight. BMC Infect Dis. 2011;11:238.
Karch H, Rüssmann H, Schmidt H, Schwarzkopf A, Heesemann J. Long-term shedding and clonal turnover of enterohemorrhagic Escherichia coli O157 in diarrheal diseases. J Clin Microbiol. 1995;33:1602–5.
National Institute of Infectious Diseases. EHEC update as of April 2014. Infect Agents Surveill Rep. 2014;35:117–8.
Zhang WL, Bielaszewska M, Liesegang A, Tschäpe H, Schmidt H, Bitzan M, et al. Molecular characteristics and epidemiological significance of Shiga toxin-producing Escherichia coli O26 strains. J Clin Microbiol. 2000;38:2134–40.
Office of Public Health Science, Office of Policy and Program Development, Food Safety and Inspection Service, United States Department of Agriculture: Risk Profile for Pathogenic Non-O157 Shiga Toxin-Producing Escherichia coli. [http://www.fsis.usda.gov/shared/PDF/Non_O157_STEC_Risk_Profile_May2012.pdf].
Brooks JT, Sowers EG, Wells JG, Greene KD, Griffin PM, Hoekstra RM, et al. Non-O157 Shiga Toxin – Producing Escherichia coli Infections in the United States, 1983–2002. J Infect Dis. 2005;192:1422–9.
Rivas M, Miliwebsky E, Chinen I, Roldán CD, Balbi L, García B, et al. Characterization and epidemiologic subtyping of Shiga toxin-producing Escherichia coli strains isolated from hemolytic uremic syndrome and diarrhea cases in Argentina. Foodborne Pathog Dis. 2006;3:88–96.
Pollock KG, Bhojani S, Beattie TJ, Allison L, Hanson M, Locking ME, et al. Highly virulent escherichia coli O26, Scotland. Emerg Infect Dis. 2011;17:1777–9.
Acknowledgements
We are grateful for the cooperation and support of the local governmental public health centers and health-care providers. We appreciate the helpful input from Dr. John M. Kobayashi (University of Washington).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AK designed the study and conducted all descriptive and statistical analyses of the data and drafted the manuscript. YY and YA helped with the design, analyses, and interpretation and revised the manuscript. TT, TS, KK, KK, TS, TM and KO contributed to the revision. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kanayama, A., Yahata, Y., Arima, Y. et al. Enterohemorrhagic Escherichia coli outbreaks related to childcare facilities in Japan, 2010–2013. BMC Infect Dis 15, 539 (2015). https://doi.org/10.1186/s12879-015-1259-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-015-1259-3