
Abstract
Background
Multidrug-resistant organisms (MDRO) are a worldwide problem. International migration and travel facilitate the spread of MDRO. Therefore the goal of our study was to assess the risk of influx of MDRO from patients transferred to one of Central Europe’s largest hospitals from abroad.
Methods
A mono-centre study was conducted. All patients transferred from other countries were screened; additional data was collected on comorbidities, etc. Presence of carbapenemases of multidrug-resistant Gram-negatives was confirmed by PCR. The association between length of stay, being colonized and/or infected by a MDRO, country of origin, diagnosis and other factors was assessed by binomial regression analyses.
Results
From 2012 to 2013, one fifth of all patients were colonized with MDRO (Methicillin-resistant Staphylococcus aureus [4.1 %], Vancomycin-resistant Enterococci [2.9 %], multidrug-resistant Gram-negatives [12.8 %] and extensively drug-resistant Gram-negatives [3.4 %]). The Gram-negatives carried a variety of carbapenemases including OXA, VIM, KPC and NDM. The length of stay was significantly prolonged by 77.2 % in patients colonized with a MDRO, compared to those not colonized (p<0.0001).
Conclusions
Country-to-Country transfer of patients to European hospitals represents a high risk of introduction of MDRO and infection control specialists should endorse containment and screening measures.
Similar content being viewed by others

Background
Multidrug-resistant organisms (MDRO) are a worldwide problem and the speed at which resistance rates are increasing is worrying. Antibiotic resistance crosses international boundaries and spreads easily between continents [1]. Surveillance systems such as the European Antimicrobial Resistance Surveillance System network report a continuing increase in antimicrobial resistance. International travel and patient transfers from hospitals located in high-prevalence regions to hospitals in low-prevalence regions facilitate the spread of MDRO. This condition triggers the introduction and establishment of MDRO into previously unaffected or less affected regions [2]. Methicillin-resistant Staphylococcus aureus (MRSA), for example, is a major cause of healthcare- and community associated infections worldwide [3]. It appears, however, to be regionally very differently distributed. While prevalence rates in some countries such as the Netherlands or Scandinavian countries are very low, MRSA are highly prevalent in the USA, Japan and Greece [4–6]. In addition, the epidemiology of vancomycin-resistant Enterococci (VRE) exhibits a remarkable geographic diversity and variable temporary trends [6–9]. Though the situation in Gram-positives appears to be rather stable, the situation in multidrug-resistant Gram-negatives (MDR-GN) is disquieting. The extensive use of broad-spectrum antibiotics has triggered the proliferation of highly resistant Gram-negative organisms [10]. In the last decade these organisms have spread over the whole world and can be found (sporadically or endemic) almost everywhere now [11–13].
The identification of patients carrying these MDRO is of utmost importance for infection control. Screening and pre-emptive contact isolation in single rooms, however, is also very costly. In addition, being colonized might also increase the risk of infection and, hence, has an influence on morbidity and mortality as well. This could result in an increased length of stay (LOS) and higher in-hospital costs. We therefore conducted a study to estimate the risk of influx of MDRO from country-to-country transfer of patients.
Methods
Study population
Only patients transferred from abroad to Heidelberg University Hospital (HUH) were included. HUH is a one of Germany’s largest hospitals with 2,000 beds and 90,000 in-patients per year. HUH provides a full range of medical and surgical services, including transplantation programmes, and is one of the leading medical centres in Europe. Approximately 500 patients per year are transferred from other countries to HUH, mainly from the Middle East.
Start of the study was the 15th of July 2012; endpoint was the 15th of September 2013. Patients were included and screened if they spent 48 h or longer in a hospital abroad (i.e. outside of Germany) within 14 days prior to admission to HUH and if they had an expected stay of 24 h or longer at HUH. All patients were pre-emptively isolated in single rooms until negative screening results were obtained. The screening regimen included nasal, rectal and if applicable wound or stoma swabs (eSwab, Copan). In addition, clinical specimens were also checked for MDRO. Infection with an MDRO was defined as patients with clinical MDRO infection. Criteria were based on CDC/NHSN definitions for healthcare-assocoiated infections (http://www.cdc.gov/HAI/infectionTypes.html). We retrospectively collected additional data including: Patients’ age and gender, country of origin and/or residency, diagnosis related groups (DRG), type of hospital ward, LOS, type of specimen sent for microbiological testing, and type of pathogen isolated.
Microbiological methods
Swabs were inoculated on Columbia 5 % sheep blood agar plate (BD) and chromogenic plates for MRSA detection (ChromAgar MRSA II, BD), for ESBL/MDR-GN detection (chromID ESBL, bioMerieux), and for VRE detection (Chromagar VRE, Mast Diagnostica); incubated aerobically for 48 h at 36 °C. Columbia-sheep blood agar was used as growth control. If growth on chromogenic plates was detected, identification by matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (Bruker, Germany), as described elsewhere, was performed [14]. Susceptibility-testing was performed by VITEK2 (bioMerieux) according to EUCAST criteria. Presence of resistence genes was confirmed by multiplex RT-PCR; mecA, femB for MRSA, vanA, vanB for VRE, and various carbapenemase resistance genes for MDR-GN as described elsewhere [15].
Classification
MDR-GN were classified as multidrug-resistant (MDR) and extensively drug-resistant (XDR) as described elsewhere [16].
Spa-typing
Spa typing was performed on each of the MRSA isolates as described elsewhere [17].
Statistics
For descriptive purposes, arithmetic mean value, standard deviation, median, interquartile range, and cumulative frequencies were calculated as appropriate. The LOS follows a zero inflated distribution. Therefore we performed negative binomial regression to assess the influence of colonization with MDRO and other factors on LOS. Two different models were fitted to patients with information on diagnosis (n = 343). The first model contained being colonized, age and main diagnosis of the patient. The diagnoses were included due to the obvious influence of severity of underlying disease on the LOS. The second model contained being colonized or infected with VRE, MRSA, MDR-GN or XDR-GN, age, and main diagnosis. To evaluate possible risk factors of being colonized logistic regression analysis was performed, including the country areas of Africa, Asia, the Middle East, Non-EU Europe and EU-Europe. The model included age, grouped DRG diagnoses, and the aforementioned country areas. P values of ≤0.05 were regarded as statistically significant. Statistical analysis was performed using SAS Software (Version 9.2, SAS, Inc., Cary, NC, USA).
Ethical considerations
At HUH, all MDRO strains are routinely collected for disease surveillance and outbreak detection. The current study thus is descriptive of a bacterial collection and microbiological characteristics could only be combined with the sex, age, clinical outcome, hospitalization, and travel history for the patients from which the strains were isolated. Additionally, data collected from patients with negative screening results was anonymised and restricted to sex, age, clinical outcome, hospitalization, and travel history. Ethical approval was therefore not required. Also, the German Act relating to the control of communicable diseases obliges HUH to monitor the MDRO on a regular basis (Infektionsschutzgesetz; http://www.gesetze-im-internet.de/ifsg/). For these reasons, consent to analyze the bacterial samples for this research project was not obtained from the patients.
Results
Demographic data
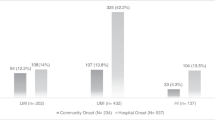
The mean age of all screened patients was 42.0 years (±23.1 SD); 59.9 % were males. The majority came from the Middle East (57.5 %), followed by Non-EU-Europe (17.9 %), EU-Europe (13.0 %), and Africa (8.5 %) (Table 1). Of all countries, patients most frequently came from Saudi Arabia (15.9 %), Russia (13.5 %), and Kuwait (10.1 %). Most common diagnoses at admission were solid organ malignancies (43.4 %), hereditary genetic disorders (9.9 %), acute (9.0 %) and chronic (8.5 %) internal medical diseases, and infections (7.6 %).
Microbiological results
Eighty-seven of 414 patients were colonized with MDRO (MRSA [4.1 %], VRE [2.9 %] or MDR-GN [12.8 %] and XDR-GN [3.4 %]. The majority (83.9 %, n = 73/87) was colonized with only one bacterial species, while 16.1 % (n = 14/87) were colonized with either two or more different MDRO. Of all isolated Gram-negatives, 81.1 % (n = 60/74) were MDR-GN, and 18.9 % XDR-GN, respectively. The XDR-GN carried various carbapenemases from different classes. Detailed information on the pathogens is listed in table 2. One third (26/87; 29.9 %) of the patients was diagnosed with an infection caused by a MDRO upon admission. The most frequent infections were wound infections and urinary tract infections, accounting for 38.5 % (n = 10/26) and 38.5 % (n = 10/26), respectively; followed by intra-abdominal infections 19.2 % (5/26) and catheter related infections 3.8 % (1/26). The most frequent MDRO causing infections were 53.8 % MDR-GN (n = 14/26), 19.2 % XDR-GN (n = 5/26), 19.2 % MRSA (n = 5/26), and 7.7 % VRE (n = 2/26). The type of swabs obtained for specimen screening were 48.0 % nasal, 45.8 % rectal, 5.0 % wound and 1.2 % stoma.
Spa typing
In total, spa typing resolved 12 distinct spa types for the collected MRSA strains (t002, t003, t024, t030, t037, t044, t127, t304, t502, t688, t3343, t3379). One patient was colonized with MRSA strains of three different spa types (t127, t304, t3343). Two of the MRSA isolates belonged to the clonal complex (CC) 5, which includes the Rhine-Hesse MRSA prototype and is prevalent in the area where HUH is located. Additionally, two MRSA strains belonged to the spa type t044, representing the major European cMRSA clone ST80. The majority of the collected MRSA-isolates (83 %) belonged to low prevalence spa types with local prevalence rates below 1.5 %.
Regression analysis
Influence of colonization status on length of stay
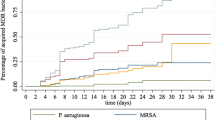
The median LOS for all patients was 10 days (inter quartile range (IQR) = 3–20), and 14 days (IQR: 6–23) when including patients with underlying diseases as classified in DRG registry. LOS was prolonged by 77.2 % in colonized patients (Incidence rate ratio (IRR) = 1.78, p < 0.001) compared to uncolonized patients adjusting for diagnose groups and age. Colonized trauma patients had the longest prolongation of LOS compared to all other colonized patients (125.0 %, IRR = 2.25, p = 0.033). VRE or MDR-GN positive patients were associated with statistically significantly longer LOS (VRE: IRR = 2.9, p<0.001; MDR-GN: IRR = 1.7, p<0.001) (Table 3). The models were run including patients that had more than one isolate, since excluding them did not change the parameter estimates, nor improve the model fit.
Influence of region of origin on colonization status
Of all 414 patients included in the study, 3 were excluded from the logistic regression analysis since patients from the Americas and Australia were all uncolonized and their numbers were too low to be included. The model was adjusted for diagnose groups and age. Patients being transferred from Africa (odds ratio [OR]: 2.5, 95 % confidence interval [CI]: 0.8-7.9, p < 0.12) and the Middle East (OR: 2.4, 95 % CI: 1.0-5.7, p<0.06) had the highest risk of being colonized with a MDRO, followed by patients from Non-EU countries (OR: 1.4, 95 % CI: 0.5-4.1, p < 0.52). Patients transferred from Asia (OR: 0.8, 95 % CI: 0.1-7.9, p<0.9) on the other hand, had a lower risk of being colonized with an MDRO compared to patients from the EU. However, the results did not reach statistical significance (Table 4).
Discussion
We screened all patients transferred from abroad for the presence of MDRO and collected additional clinical and demographic data to assess the impact of MDRO colonization and infection on the individual and the risk of influx of MDRO into large university hospitals. The profile of HUH is representative of other large university hospitals. The analyzed data show that a considerable proportion of patients transferred from abroad are colonized with MDRO, mainly with MDR- and XDR-GN. The proportion of colonization, compared to patients from other hospitals in Germany, was equal with regards to VRE (2.9 % vs. 2.9 %), while it was superior with regards to all other MDROs [MRSA (4.1 % vs. 2.4 %), MDR-GN (12.8 % vs. 2.2 %), XDR-GN (3.4 % vs. 0.3 %)].
Of all Gram-negatives 18.9 % were XDR-GN (n = 14/74) carrying various carbapenemases of different classes including OXA-48, VIM-1, KPC and NDM-1 (Table 2). The carbapenemases carrying strains were mainly Enterobacteriaceae, such as E. coli and K. pneumoniae, which are the main reservoir species for NDM, KPC, and OXA-48 carbapenemases worldwide [13]. Patients carrying XDR-GNs repeatedly act as index patients, leading to outbreaks when transferred from high prevalence areas [18, 19]. In addition, infections with MDR-GN or XDR-GN are associated with worse clinical outcome and prolonged LOS [20–22]. Not only infections, but also colonizations with MDRO can have an impact on clinical outcome and can result in prolonged LOS [20, 23]. In some patients, being colonized also increases the risk of developing an infection with the same MDRO [24, 25]. Our results are concordant with these findings. Being infected or colonized with a MDRO increased the LOS significantly and considerably prolonged the duration of the hospital stay. The most substantial and statistically significant increase in LOS was due to MDR-GN and VRE. The prevalence of VRE in our study, however, was lowest among all MDRO and the overall impact of MDR-GN was therefore much higher. Especially E. coli, with an incidence more than twice as high as any other isolated microorganism in this study, had a major impact. The advantage of our study compared to others investigating the impact of colonization of MDRO on LOS [26], is our adjustment for the severity of underlying illnesses.
The present study also has some minor limitations. Our results might overestimate the prevalence rates of MDRO in the different regions, since patients transferred to a university hospital are usually sicker than those treated in smaller regional hospitals. In addition, our study population consisted of patients who previously had contact with hospitals in their home country, thus having an intrinsic increased risk of being colonized with a MDRO. As we only included patients transferred from abroad, we cannot entirely exclude the, however unlikely, possibility that those patients had been to German hospitals in earlier years. Nevertheless, these are exactly the kind of patients that are transferred to large University Hospitals from abroad and probably reflect the prevalence rates that infection control specialists in Western countries have to expect. The external validity of our results might only be hampered by the fact that 57.5 % of all patients came from the Middle East. Thus, results might differ in hospitals where the majority of foreign patients come from other areas.
The low MRSA rates in our study, however, might be influenced by the fact that most of the included patients came from the Middle East and Non-EU Europe and only few came from Asia or the Americas. In fact, the highest MRSA rates worldwide are found in North America and Japan [6]. Spa typing resolved that our collected MRSA strains consisted of highly diverse spa types and only four of all MRSA positive patients had spa types (CC5 and ST-80) also present in the local endemic lineages. Thus, the majority of MRSA strains from international patients are highly diverse and not usually found in the local European environment.
Conclusions
Our data show that a considerable proportion of transferred patients are colonized with MDRO, mainly with MDR- and XDR-GN, which carry a variety of different carbapenemases. Infections with MDRO occurred in approximately one-third of all colonized patients. LOS was significantly prolonged in all colonized patients. In summary, country-to-country transfer of patients to large university hospitals represents a risk of introduction of MDRO. We would like to emphasize that infection control specialists should maintain vigilance, endorse containment and screening measures, and receive transferred patients in an area of the hospital equipped to manage isolation for MDRO [2].
Abbreviations
- MDRO:
-
Multidrug-resistant organisms
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- VRE:
-
Vancomycin-resistant Enterococci
- MDR-GN:
-
Multidrug-resistant Gram-negatives
- XDR-GN:
-
Extensively drug-resistant Gram-negatives
- LOS:
-
Length of stay
- HUH:
-
Heidelberg University Hospital
- DRG:
-
Diagnosis related groups
- IQR:
-
Inter quartile range
- IRR:
-
Incidence rate ratio
- CI:
-
Confidence interval
- OR:
-
Odds ratio
References
Centers-for-Disease-Control-and-Prevention: Antibiotic Resistance Threats in the United States. Edited by CDC: CDC; 2013: 1–114.
Rogers BA, Aminzadeh Z, Hayashi Y, Paterson DL. Country-to-country transfer of patients and the risk of multi-resistant bacterial infection. Clin Infect Dis. 2011;53(1):49–56.
Kock R, Becker K, Cookson B, van Gemert-Pijnen JE, Harbarth S, Kluytmans J, et al. Methicillin-resistant Staphylococcus aureus (MRSA): burden of disease and control challenges in Europe. Euro Surveill. 2010;15(41):19688.
Johnson AP. Methicillin-resistant Staphylococcus aureus: the European landscape. J Antimicrob Chemother. 2011;66 Suppl 4:iv43–8.
Diekema DJ, Pfaller MA, Schmitz FJ, Smayevsky J, Bell J, Jones RN, et al. Survey of infections due to Staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific region for the SENTRY Antimicrobial Surveillance Program, 1997–1999. Clin Infect Dis. 2001;32 Suppl 2:S114–132.
Molton JS, Tambyah PA, Ang BS, Ling ML, Fisher DA. The global spread of healthcare-associated multidrug-resistant bacteria: a perspective from Asia. Clin Infect Dis. 2013;56(9):1310–8.
Mutters NT, Brooke RJ, Frank U, Heeg K. Low risk of apparent transmission of vancomycin-resistant Enterococci from bacteraemic patients to hospitalized contacts. Am J Infect Control. 2013;41(9):778–81.
Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, Pollock DA, et al. NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect Control Hosp Epidemiol. 2008;29(11):996–1011.
Werner G, Coque TM, Hammerum AM, Hope R, Hryniewicz W, Johnson A, et al. Emergence and spread of vancomycin resistance among enterococci in Europe. Euro Surveill. 2008;13(47):1–11.
Nordmann P, Dortet L, Poirel L. Carbapenem resistance in Enterobacteriaceae: here is the storm! Trends in molecular medicine. 2012;18(5):263–72.
Rolain JM, Parola P, Cornaglia G. New Delhi metallo-beta-lactamase (NDM-1): towards a new pandemia? Clin Microbiol Infect. 2010;16(12):1699–701.
Drew RJ, Turton JF, Hill RL, Livermore DM, Woodford N, Paulus S, et al. Emergence of carbapenem-resistant Enterobacteriaceae in a UK paediatric hospital. J Hosp Infect. 2013;84(4):300–4.
Nordmann P, Poirel L. The difficult-to-control spread of carbapenemase producers among Enterobacteriaceae worldwide. Clin Microbiol Infect. 2014;20(9):821–30.
Eigner U, Holfelder M, Oberdorfer K, Betz-Wild U, Bertsch D, Fahr AM. Performance of a matrix-assisted laser desorption ionization-time-of-flight mass spectrometry system for the identification of bacterial isolates in the clinical routine laboratory. Clin Lab. 2009;55(7–8):289–96.
Hofko M, Mischnik A, Kaase M, Zimmermann S, Dalpke AH. Detection of carbapenemases by real-time PCR and melt curve analysis on the BD Max system. J Clin Microbiol. 2014;52(5):1701–4.
Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2011;18(3):268–81.
Harmsen D, Claus H, Witte W, Rothganger J, Claus H, Turnwald D, et al. Typing of methicillin-resistant Staphylococcus aureus in a university hospital setting by using novel software for spa repeat determination and database management. J Clin Microbiol. 2003;41(12):5442–8.
Wendt C, Schutt S, Dalpke AH, Konrad M, Mieth M, Trierweiler-Hauke B, et al. First outbreak of Klebsiella pneumoniae carbapenemase (KPC)-producing K. pneumoniae in Germany. Eur J Clin Microbiol Infect Dis. 2010;29(5):563–70.
Moro M, Nizzero P, Biancardi A, Baldan R, Scarpellini P, Curti C, et al. An outbreak caused by multidrug-resistant OXA-58-positive Acinetobacter baumannii in an intensive care unit in Italy. J Hosp Infect. 2008;68(1):97–9.
Ben-David D, Kordevani R, Keller N, Tal I, Marzel A, Gal-Mor O, et al. Outcome of carbapenem resistant Klebsiella pneumoniae bloodstream infections. Clin Microbiol Infect. 2012;18(1):54–60.
Gudiol C, Tubau F, Calatayud L, Garcia-Vidal C, Cisnal M, Sanchez-Ortega I, et al. Bacteraemia due to multidrug-resistant Gram-negative bacilli in cancer patients: risk factors, antibiotic therapy and outcomes. J Antimicrob Chemother. 2011;66(3):657–63.
Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol. 2008;29(12):1099–106.
Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, Schwartz D, Leavitt A, Carmeli Y. Predictors of carbapenem-resistant Klebsiella pneumoniae acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother. 2008;52(3):1028–33.
Russell DL, Flood A, Zaroda TE, Acosta C, Riley MM, Busuttil RW, et al. Outcomes of colonization with MRSA and VRE among liver transplant candidates and recipients. Am J Transplant. 2008;8(8):1737–43.
Niven DJ, Laupland KB, Gregson DB, Church DL, Group SaSI. Epidemiology of Staphylococcus aureus nasal colonization and influence on outcome in the critically ill. J Crit Care. 2009;24(4):583–9.
Nemeth J, Ledergerber B, Preiswerk B, Nobile A, Karrer S, Ruef C, et al. Multidrug-resistant bacteria in travellers hospitalized abroad: prevalence, characteristics, and influence on clinical outcome. J Hosp Infect. 2012;82(4):254–9.
Language editing
We thank Veronika Malek for her detailed proofreading and thorough revisions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
We acknowledge financial support by Deutsche Forschungsgemeinschaft and Ruprecht-Karls-Universität Heidelberg within the funding programme Open Access Publishing for covering the article-processing charge. The authors declare that they have no further competing interests.
Authors’ contributions
N.T.M. performed the literature review, data collection, molecular analysis, statistical analysis and the writing of the manuscript. A.S. performed the statistical analysis and the drafting of the manuscript. F.G. performed the molecular analysis and drafting of the manuscript. A.M. performed data collection and drafting of the manuscript, U.F. is the guarantor of the paper and performed the drafting of the manuscript. All authors read and approved the final manuscript. All authors report no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mutters, N.T., Günther, F., Sander, A. et al. Influx of multidrug-resistant organisms by country-to-country transfer of patients. BMC Infect Dis 15, 466 (2015). https://doi.org/10.1186/s12879-015-1173-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-015-1173-8