
Abstract
Introduction
Chronic inflammation and malnutrition play important roles in muscle loss. Although albumin, globulin and albumin to globulin ratio (AGR) are considered to be useful inflammatory-nutritional biomarkers, their relationship with muscle mass remain unclear. This study aimed to investigate the relationship between them in adults.
Methods
We utilized data from the National Health and Nutrition Examination Survey (NHANES) 2011–2014 for analysis. Data on albumin, globulin, appendicular skeletal muscle mass, body mass index (BMI) and potential confounders (sociodemographic characteristics, medical conditions, laboratory parameters) were extracted and analyzed. We conducted multivariate linear regression models and smooth curve fittings to investigate the association between albumin, globulin, AGR and muscle mass. Subgroup analysis based on gender and muscle mass were performed.
Results
A total of 4110 participants were included, there were 294 participants with low muscle mass (LMM) and 3816 participants with normal muscle mass (NMM). LMM individuals were older, had greater prevalence of diabetes, higher BMI, globulin and triglycerides, lower albumin and AGR. Albumin was positively correlated to muscle mass in men, but negatively correlated with muscle mass in women. There were negative association between globulin and muscle mass, and positive association between AGR and muscle mass among men, but no significant associations were detected among women. Moreover, a linear relationship between albumin, globulin and muscle mass, as well as a non-linear relationship between AGR and muscle mass in men were identified.
Conclusions
The relationships between albumin, globulin, AGR and muscle mass were sex-specific. We speculate these indicators may be useful in assessing muscle mass in men.
Similar content being viewed by others


Introduction
With the global population aging, the incidence of sarcopenia continues to rise, literatures reported the prevalence varied from 11 to 50% in people aged over 80 years old [1, 2]. A progressive decrease of skeletal muscle mass is the main feature of sarcopenia, which leads to poor metal health, increased morbidity rate, decreased physical ability, and declined quality of life [3,4,5]. Acknowledging the high prevalence and harmful impacts of muscle loss, more and more researches have been conducted to explore its pathogenesis, but the results remain incomplete and controversial [6].
The decrease of muscle mass was once considered to be the result of physical inactivity, malnutrition, neurodegeneration, and impaired hormone secretion [7]. Only recently have scholars started to investigate the links between age-related chronic low-grade inflammation and muscle loss [8]. A growing number of studies have demonstrated that individuals with low muscle mass have an elevated inflammatory marker profile [6, 9], which was believed to play an important role in the process of muscle decline [10]. Albumin can reflect not only the nutritional but also the inflammatory status [11]. Globulin consists of many proteins associated with inflammation, increases during the inflammatory process. The AGR takes into account both albumin and globulin to give a more accurate indication of the body’s nutritional and inflammatory status [12]. To date, whether there are any associations between these indicators and muscle mass remain largely unknow. Therefore, we conducted this study to investigate the relationships between albumin, globulin, AGR and muscle mass.
Methods
Research design and study population
The National Health and Nutrition Examination Survey is a cross-sectional survey, which provides a wealth of information on the nutrition and health of the general population in United States using a multistage, complex clustered, probability sampling design [13]. The NHANES protocols were approved by the National Center for Health Statistics ethics review board, and informed consent forms were obtained from all participants [14]. The survey data are free available for researchers worldwide, and operational instructions are available on the CDC website.
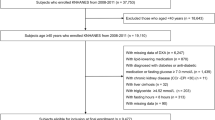
We utilized data from 2 two-year cycles (2011–2012 and 2013–2014) of NHANES for analysis. Participants aged 20 years or older, with complete data of serum albumin, serum globulin, appendicular skeletal muscle mass (ASM) and BMI were included in this study. (The flowchart of selection processes is shown in Fig. 1.) Then data on serum albumin, serum globulin, ASM, BMI and potential confounders (sociodemographic characteristics, medical conditions, laboratory parameters) were extracted and aggregated.

The flowchart of selection processes
Study variables
Muscle mass
The body composition measurements were performed using whole-body dual-energy x-ray absorptiometry (DXA) exams (Hologic, Inc., Bedford, Massachusetts), which provided values for total and regional bone mineral content, fat mass and lean soft tissue mass. ASM was defined as the sum of the lean soft tissue mass of both arms and legs [15]. BMI was obtained from body measures. We further quantified muscle mass using appendicular skeletal muscle index (ASMI), calculated as the ratio of ASM and BMI [16]. Based on the Foundation for the National Institutes of Health recommendation, LMM was defined as ASMI < 0.789 for men and ASMI < 0.512 for women [16].
Serum albumin, globulin and AGR
The serum albumin (g/dL) and serum globulin (g/dL) were measured using a Beckman UniCel® DxC800 Synchron instrument [17]. The AGR was calculated as the albumin divided by the globulin.
Other covariates
The selection of confounding factors was based on literatures, and the following variables were considered as covariates. Demographic variables, including age (years), gender (man or woman), race (Hispanic, Non-Hispanic White, Non-Hispanic Black, others) were obtained from demographic data. The presence or absence of hypertension and diabetes were defined by participants’ self-report of the diagnosis by a doctor. The serum total calcium (mg/dL), phosphorus (mg/dL), triglycerides (mg/dL) and uric acid (mg/dL) were measured using a Beckman UniCel® DxC800 Synchron instrument. White blood cell counts (1000 cells/uL) and Hemoglobin (g/dL) were measured using the Beckman Coulter MAXM instrument [17]. The serum 25(OH)D (nmol/L) was quantified using ultra-high performance liquid chromatography-tandem mass spectrometry (UHPLC-MS/MS) [18]. The total cholesterol (mg/dL) in serum was determined using Roche/Hitachi Modular P Chemistry Analyzer [19]. (A summary of the reference range of laboratory parameters is demonstrated in Supplemental Table 1). A detailed description of the laboratory methodology, quality-control and quality-assurance protocols can be found on the NHANES website.
Statistical analysis
All statistical analyses were conducted by R 3.4.3 (https://www.r-project.org/) and EmpowerStats software (http://www.empowerstats. com), and P < 0.05 was considered statistically significant. NHANES sample weights was taken into account when calculated all estimates. Weighted linear regression model (for continuous variables) and weighted Chi-square test (for categorical variables) were performed to compare the baseline characteristics of the included participants. Weighted multiple linear regression analysis and smooth curve fittings were used to evaluate the relationship between albumin, globulin, AGR and ASMI. If there was a non-linear relationship, threshold effect analysis was performed using two-piecewise linear regression model.
Results
There were 19,931 participants in the NHANES 2011–2014, 15,821 participants were excluded due to lack of sufficient data or younger than 20 years old, leaving 4110 participants for final analysis. As demonstrated in Table 1, the included participants were subclassified based on the presence or absence of LMM. There were 294 participants (man: 139, woman: 155) with LMM and 3816 participants (man: 1941, woman: 1875) with NMM. Compared to those with NMM, men and women with LMM were older, and had significantly greater prevalence of diabetes, higher BMI, serum globulin and triglycerides, lower serum albumin and AGR.
Association between serum albumin and muscle mass
Table 2 demonstrates the association between serum albumin and muscle mass in three multivariate linear regression models. The serum albumin was positively correlated to muscle mass in all three models (model 1: β = 0.238, 95%CI:0.213–0.262; model 2: β = 0.070, 95%CI:0.051–0.090; model 3: β = 0.023, 95%CI:0.004–0.042). In subgroup analyses stratified by gender, there were a positive association in men, but a negative association in women. When stratified by muscle mass, a significantly positive association was observed only in NMM individuals.
Association between serum globulin and muscle mass
The effect sizes for the association between serum globulin and muscle mass are presented in Table 3. There were significantly negative associations between serum globulin and muscle mass in model 1 (β = -0.091, 95%CI: -0.110-(-0.073)) and model 2 (β = -0.038, 95%CI: -0.049-(-0.028)), but no significant association between them in model 3 (β = -0.010, 95%CI: -0.021–0.001). Stratified by gender and muscle mass, the significant association was observed only in men.
Association between AGR and muscle mass
As show in Table 4, AGR was positively correlated to muscle mass in model 1 (β = 0.186, 95%CI:0.145–0.227) and model 2 (β = 0.064, 95%CI:0.042–0.087), but not in model 3 (β = 0.017, 95%CI: -0.001–0.034). Stratified by gender and muscle mass, the significant correlations retained only in men.
Threshold effect analysis
Generalized additive models and smooth curve fittings were performed to find the non-linear relationship between serum albumin, serum globulin, AGR and muscle mass (Figs. 2, 3 and 4). The results demonstrated linear relationships between globulin and muscle mass (Fig. 2b), albumin and muscle mass (Fig. 3b) in men, and non-linear relationships between albumin and muscle mass in women (Fig. 3b), AGR and muscle mass in men (Fig. 4b). Then threshold effect values of serum albumin in women and AGR in men were identified by using two-piecewise linear regression models (Table 5).

a The relationship between serum globulin and ASMI. The area between two blue dotted is expressed as 95% CI. Each point shows the magnitude of the globulin and is connected to form a continuous line. b The relationship between serum globulin and ASMI, stratified by sex

a The relationship between serum albumin and ASMI. The area between two blue dotted is expressed as 95% CI. Each point shows the magnitude of the albumin and is connected to form a continuous line. b The relationship between serum albumin and ASMI, stratified by sex

a The relationship between AGR and ASMI. The area between two blue dotted is expressed as 95% CI. Each point shows the magnitude of the AGR and is connected to form a continuous line. b The relationship between AGR and ASMI, stratified by sex
Discussion
Various factors have been suggested to involve in the occurrence and development of muscle loss, chronic low-grade inflammation and malnutrition were considered to be important causative factors [8, 20]. Although several elevated inflammatory factors have been identified in LMM individuals, a biomarker with a clear link to muscle mass measurement is still lacking. The results of our study demonstrated a significantly higher serum globulin, and lower serum albumin and AGR in LMM individuals. Furthermore, albumin and AGR were positively correlated with muscle mass, globulin was negatively correlated with muscle mass in men.
There is a growing awareness that even health ageing cannot avoid an elevated inflammatory status, which is considered to be related with muscle loss and function impairment [21]. Several elevated inflammatory markers, including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α), have been identified in patients with poor muscle strength and muscle mass [21, 22]. Serum globulin contains various proteins involving in inflammatory responses, such as complements, immunoglobulins, and acute phase response proteins, which has been recognized as a reliable indicator for inflammatory state [23]. However, the relationship between globulin and muscle mass has long been disregarded. Our study not only found a higher globulin level in individuals with LMM, but also identified a negative association between globulin and muscle mass in men. This finding further corroborated the role of inflammation in muscle loss.
Albumin, which has been commonly used for evaluating nutritional status, is currently regarded as an inflammatory marker. Previous studies demonstrated that it was a negative phase reactant that decreased with inflammation, irrespective of patients’ nutritional state [24, 25]. Some scholars hold the view that hypoalbuminemia might be related with inflammation rather than malnutrition [25]. Recently, several studies have been conducted to investigate the relationship between albumin and muscle function. Based on the results of a longitudinal study including 1320 older men and women, Schalk et al. suggested that low albumin levels, even within the normal limits, were independently associated with weaker muscle strength [26]. In another cross-sectional study, the authors reported that serum albumin levels were positively correlated with gait speed and handgrip strength [11]. The finding of our study further suggested a close relationship between albumin and muscle mass, which demonstrated a positive association between albumin and muscle mass in men. Two possible explanations were that, first, albumin reflected nutritional status, which was positively associated with muscle mass. Second, inflammatory mediators could not only promote albumin escape from blood capillaries, but also decrease the synthesis of albumin [24]. As both albumin and muscle mass were negatively associated with inflammation, there was no doubt that albumin would show a positive association with muscle mass.
The AGR, which takes both albumin and globulin into account, is a convenient serological indicator to identify serum protein abnormalities [27]. Several studies indicated that it could reflect not only a change in nutritional condition, but also a medium to long-term inflammatory status [27, 28]. Literatures reported AGR could serve as a diagnostic biomarker for infection diseases, or a prognostic marker for various types of cancer [29, 30]. However, few studies have investigated the relationship between AGR and muscle mass. Our study showed a positive association between AGR and muscle mass in men, which suggested it might also be a useful biomarker for assessing muscle mass.
Although evidences for sex difference in hemoglobulin, serum creatinine, serum immunoglobulin, serum albumin levels have been reported by several previous studies [31, 32]. There is a lack of knowledge about the effect of sex on the relationship between serum albumin, globulin and muscle mass. The present study demonstrated albumin, globulin, AGR were differentially associated with muscle mass between men and women. The inherent differences in hormone and inflammatory levels may partially explain the sex-specific outcomes [33], but further studies are still required to elucidate the underlying mechanisms.
Limitation
There were some limitations in this study. Firstly, this was a cross-sectional study, so we could not establish a causal relationship between albumin, globulin, AGR and muscle mass. Secondly, some potential confounding factors, such as IL-6, TNF-α, CRP and ESR, were not available in this study. Finally, there were different adjustment methods for quantifying muscle mass, such as ASM/height2, ASM/weight, and ASM/BMI. It has been suggested that different adjustment methods may lead to different results in the relationship between muscle mass and clinical outcomes [34]. Therefore, consensus is urgently needed to standardize the adjustment method.
Conclusion
The present study demonstrated a significantly higher serum globulin, and lower serum albumin and AGR in LMM individuals. The relationships between albumin, globulin, AGR and muscle mass were sex-specific, positive associations between albumin, AGR and muscle mass, and negative association between globulin and muscle mass were observed only in men. We speculate these indicators may be useful in assessing muscle mass in men.
Availability of data and materials
The data are available from the corresponding author on reasonable request.
Abbreviations
- NHANES:
-
National Health and Nutrition Examination Survey
- AGR:
-
Albumin to globulin ratio, BMI: body mass index
- DXA:
-
Dual-energy x-ray absorptiometry
- ASM:
-
Appendicular skeletal muscle mass
- ASMI:
-
Appendicular skeletal muscle index
- LMM:
-
Low muscle mass
- NMM:
-
Normal muscle mass
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- IL-6:
-
Interleukin-6
- TNF-α:
-
Tumor necrosis factor-α
References
Morley JE. Sarcopenia in the elderly. Fam Pract. 2012;29(Suppl 1):i44–8. https://doi.org/10.1093/fampra/cmr063.
Cruz-Jentoft AJ, Landi F, Schneider SM, Zúñiga C, Arai H, Boirie Y, Chen LK, Fielding RA, Martin FC, Michel JP, Sieber C, Stout JR, Studenski SA, Vellas B, Woo J, Zamboni M, Cederholm T. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing. 2014;43:748–59. https://doi.org/10.1093/ageing/afu115.
Chhetri JK, de Souto BP, Fougère B, Rolland Y, Vellas B, Cesari M. Chronic inflammation and sarcopenia: a regenerative cell therapy perspective. Exp Gerontol. 2018;103:115–23. https://doi.org/10.1016/j.exger.2017.12.023.
Cao C, Liu Q, Yang L, Zheng X, Lan P, Koyanagi A, Vancampfort D, Soysal P, Veronese N, Stubbs B, Firth J, Smith L. Handgrip strength is associated with suicidal thoughts in men: cross-sectional analyses from NHANES. Scand J Med Sci Sports. 2020;30:92–9. https://doi.org/10.1111/sms.13559.
Henwood T, Hassan B, Swinton P, Senior H, Keogh J. Consequences of sarcopenia among nursing home residents at long-term follow-up. Geriatric nursing (New York, NY). 2017;38:406–11. https://doi.org/10.1016/j.gerinurse.2017.02.003.
Bian AL, Hu HY, Rong YD, Wang J, Wang JX, Zhou XZ. A study on relationship between elderly sarcopenia and inflammatory factors IL-6 and TNF-α. Eur J Med Res. 2017;22:25. https://doi.org/10.1186/s40001-017-0266-9.
Thomas DR. Loss of skeletal muscle mass in aging: examining the relationship of starvation, sarcopenia and cachexia. Clin Nutr (Edinburgh, Scotland). 2007;26:389–99. https://doi.org/10.1016/j.clnu.2007.03.008.
Beyer I, Mets T, Bautmans I. Chronic low-grade inflammation and age-related sarcopenia. Curr Opin Clin Nutr Metab Care. 2012;15:12–22. https://doi.org/10.1097/MCO.0b013e32834dd297.
Bano G, Trevisan C, Carraro S, Solmi M, Luchini C, Stubbs B, Manzato E, Sergi G, Veronese N. Inflammation and sarcopenia: a systematic review and meta-analysis. Maturitas. 2017;96:10–5. https://doi.org/10.1016/j.maturitas.2016.11.006.
Wilson D, Jackson T, Sapey E, Lord JM. Frailty and sarcopenia: the potential role of an aged immune system. Ageing Res Rev. 2017;36:1–10. https://doi.org/10.1016/j.arr.2017.01.006.
van Atteveld VA, Van Ancum JM, Reijnierse EM, Trappenburg MC, Meskers CGM, Maier AB. Erythrocyte sedimentation rate and albumin as markers of inflammation are associated with measures of sarcopenia: a cross-sectional study. BMC Geriatr. 2019;19:233. https://doi.org/10.1186/s12877-019-1253-5.
Wu PP, Hsieh YP, Kor CT, Chiu PF. Association between Albumin-Globulin Ratio and Mortality in Patients with Chronic Kidney Disease. J Clin Med. 2019:8. https://doi.org/10.3390/jcm8111991.
Johnson CL, Dohrmann SM, Burt VL, Mohadjer LK. National health and nutrition examination survey: sample design, 2011–2014. Vital Health Stat. 2014:1–33
Yang L, Cao C, Kantor ED, Nguyen LH, Zheng X, Park Y, Giovannucci EL, Matthews CE, Colditz GA, Cao Y. Trends in sedentary behavior among the US population, 2001–2016. JAMA. 2019;321:1587–97. https://doi.org/10.1001/jama.2019.3636.
Chen L, Shivappa N, Dong X, Ming J, Zhao Q, Xu H, Liang P, Cheng M, Liu J, Sun P, Ban B. Association between appendicular skeletal muscle index and leukocyte telomere length in adults: a study from National Health and Nutrition Examination Survey (NHANES) 1999–2002. Clin Nutr (Edinburgh, Scotland). 2021;40:3470–8. https://doi.org/10.1016/j.clnu.2020.11.031.
Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, Ferrucci L, Guralnik JM, Fragala MS, Kenny AM, Kiel DP, Kritchevsky SB, Shardell MD, Dam TT, Vassileva MT. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci. 2014;69:547–58. https://doi.org/10.1093/gerona/glu010.
Fan Y, Li X, Xu Q, Zhang Y, Yang X, Han X, Du G, Xia Y, Wang X, Lu C (2020) Serum albumin mediates the effect of multiple per- and polyfluoroalkyl substances on serum lipid levels. Environmental pollution (Barking, Essex : 1987) 266:115138. https://doi.org/10.1016/j.envpol.2020.115138
Liu M, Yao X, Zhu Z. Associations between serum calcium, 25(OH)D level and bone mineral density in older adults. J Orthop Surg Res. 2019;14:458. https://doi.org/10.1186/s13018-019-1517-y.
Batsis JA, Mackenzie TA, Jones JD, Lopez-Jimenez F, Bartels SJ. Sarcopenia, sarcopenic obesity and inflammation: results from the 1999–2004 national health and nutrition examination survey. Clinical nutrition (Edinburgh, Scotland). 2016;35:1472–83. https://doi.org/10.1016/j.clnu.2016.03.028.
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48:601. https://doi.org/10.1093/ageing/afz046.
Dalle S, Rossmeislova L, Koppo K. The Role of Inflammation in Age-Related Sarcopenia. Front Physiol. 2017;8:1045. https://doi.org/10.3389/fphys.2017.01045.
Schaap LA, Pluijm SM, Deeg DJ, Harris TB, Kritchevsky SB, Newman AB, Colbert LH, Pahor M, Rubin SM, Tylavsky FA, Visser M. Higher inflammatory marker levels in older persons: associations with 5-year change in muscle mass and muscle strength. J Gerontol A Biol Sci Med Sci. 2009;64:1183–9. https://doi.org/10.1093/gerona/glp097.
Zhou T, Yu ST, Chen WZ, Xie R, Yu JC. Pretreatment albumin globulin ratio has a superior prognostic value in laryngeal squamous cell carcinoma patients: a comparison study. J Cancer. 2019;10:594–601. https://doi.org/10.7150/jca.28817.
Niedziela JT, Hudzik B, Szygula-Jurkiewicz B, Nowak JU, Polonski L, Gasior M, Rozentryt P. Albumin-to-globulin ratio as an independent predictor of mortality in chronic heart failure. Biomark Med. 2018;12:749–57. https://doi.org/10.2217/bmm-2017-0378.
Mirsaeidi M, Omar HR, Sweiss N. Hypoalbuminemia is related to inflammation rather than malnutrition in sarcoidosis. Eur J Intern Med. 2018;53:e14–6. https://doi.org/10.1016/j.ejim.2018.04.016.
Schalk BW, Deeg DJ, Penninx BW, Bouter LM, Visser M. Serum albumin and muscle strength: a longitudinal study in older men and women. J Am Geriatr Soc. 2005;53:1331–8. https://doi.org/10.1111/j.1532-5415.2005.53417.x.
Maeda S, Takeya Y, Oguro R, Akasaka H, Ryuno H, Kabayama M, Yokoyama S, Nagasawa M, Fujimoto T, Takeda M, Onishi-Takeya M, Itoh N, Takami Y, Yamamoto K, Sugimoto K, Inagaki H, Ogawa M, Nakagawa T, Yasumoto S, Masui Y, Arai Y, Ishizaki T, Ikebe K, Gondo Y, Kamide K, Rakugi H. Serum albumin/globulin ratio is associated with cognitive function in community-dwelling older people: the septuagenarians, octogenarians, nonagenarians investigation with centenarians study. Geriatr Gerontol Int. 2019;19:967–71. https://doi.org/10.1111/ggi.13751.
Xie HL, Zhang Q, Ruan GT, Ge YZ, Hu CL, Song MM, Song CH, Zhang X, Zhang XW, Li XR, Zhang KP, Liu T, Yang M, Tang M, Xu HX, Shi HP. Evaluation and validation of the prognostic value of serum albumin to globulin ratio in patients with cancer cachexia: results from a large multicenter collaboration. Front Oncol. 2021;11:707705. https://doi.org/10.3389/fonc.2021.707705.
Ye Y, Chen W, Gu M, Xian G, Pan B, Zheng L, Zhang Z, Sheng P. Serum globulin and albumin to globulin ratio as potential diagnostic biomarkers for periprosthetic joint infection: a retrospective review. J Orthop Surg Res. 2020;15:459. https://doi.org/10.1186/s13018-020-01959-1.
Atsumi Y, Kawahara S, Kakuta S, Onodera A, Hara K, Kazama K, Numata M, Aoyama T, Tamagawa A, Tamagawa H, Oshima T, Yukawa N, Rino Y. Low preoperative albumin-to-globulin ratio is a marker of poor prognosis in patients with esophageal cancer. In vivo (Athens, Greece). 2021;35:3555–61. https://doi.org/10.21873/invivo.12658.
Weaving G, Batstone GF, Jones RG. Age and sex variation in serum albumin concentration: an observational study. Ann Clin Biochem. 2016;53:106–11. https://doi.org/10.1177/0004563215593561.
Beregi E, Regius O, Németh J, Rajczy K, Gergely I, Lengyel E. Gender differences in age-related physiological changes and some diseases. Z Gerontol Geriatr. 1995;28:62–6.
Mikó A, Pótó L, Mátrai P, Hegyi P, Füredi N, Garami A, Illés A, Solymár M, Vincze Á, Balaskó M, Pár G, Sarlós P, Bajor J, Tenk J, Rostás I, Pétervári E. Gender difference in the effects of interleukin-6 on grip strength - a systematic review and meta-analysis. BMC Geriatr. 2018;18:107. https://doi.org/10.1186/s12877-018-0798-z.
Kim KM, Jang HC, Lim S. Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in assessing sarcopenia. Korean J Intern Med. 2016;31:643–50. https://doi.org/10.3904/kjim.2016.015.
Acknowledgements
Not applicable.
Funding
There was no funding information to declare.
Author information
Authors and Affiliations
Contributions
Zhi Chen wrote the manuscript, Chenyang Song, Zhipeng Yao, Jun Sun collected and analyzed the data, Wenge Liu designed this study and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The NHANES protocols were approved by the National Center for Health Statistics ethics review board, and informed consent forms were obtained from all participants. We confirmed all methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental table 1.
The summary of laboratory parameters
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, Z., Song, C., Yao, Z. et al. Associations between albumin, globulin, albumin to globulin ratio and muscle mass in adults: results from the national health and nutrition examination survey 2011–2014. BMC Geriatr 22, 383 (2022). https://doi.org/10.1186/s12877-022-03094-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03094-4