
Abstract
Background
Falls occurring on stairs or in bathrooms are associated with a high risk of injuries among older adults. Home environmental assessments are frequently used to guide fall-prevention interventions. The aims of this review were to describe how, where, by whom, and for whom environmental hazard checklists are used, and to examine the characteristics of environmental hazard assessment checklists with specific attention to features of bathrooms and stairs/steps assessed in them.
Methods
Studies published before January 5, 2018, were identified using several databases. Publications reporting the use and/or evaluation of environmental hazard checklists were eligible if they assessed bathrooms or stairs/steps in homes of older adults (≥65 years). Content analysis was conducted on publications that provided a complete list of specific environmental hazards assessed. Checklist items related to bathrooms and stairs/steps were extracted and categorized as structural or non-structural and as objective or subjective.
Results
1119 studies were appraised. A pool of 136 published articles and 4 checklists from the grey literature were included in this scoping review. Content analysis was conducted on 42 unique checklists. There was no widely used checklist and no obvious consensus definition of either environmental hazards overall or of single hazards listed in checklists. Checklists varied greatly with respect to what rooms were assessed, whether or not outdoor stair/steps hazards were assessed, and how responses were coded. Few checklists examined person-environment fit. The majority of checklists were not oriented towards structural hazards in bathrooms. Although the majority of checklists assessing stair/steps hazards evaluated structural hazards, most features assessed were not related to the construction geometry of stairs/steps. Objective features of bathrooms and stairs/steps that would deem them safe were rarely specified. Rather, adequacy of their characteristics was mostly subjectively determined by the evaluator with little or no guidance or training.
Conclusion
The lack of standard definitions and objective criteria for assessing environmental hazards for falls is limiting meaningful cross-study comparisons and slowing advances in this field. To inform population health interventions aimed at preventing falls, such as building code regulations or municipal housing by-laws, it is essential to include objectively-assessed structural hazards in environmental checklists.
Similar content being viewed by others

Background
Falls among older adults are considered a major public health concern [1]. Falls can lead to loss of autonomy, greater isolation and depression, reduced mobility, and increased morbidity and mortality [2]. In Canada, the direct and indirect costs of falls among older adults are estimated at over $3 billion annually [3]. Aging-in-place policies highlight the importance of mitigating fall risks in the home [4]; safer homes may enable independent rather than dependent living arrangements for older persons.
Although causes of falls are considered multi-factorial, it is well-established that environmental hazards are implicated in as many as one third of all falls among older adults [5,6,7,8,9]. Research on falls indicates that two areas in the home are particularly hazardous for injurious falls; bathrooms, and indoor or outdoor stairs or steps [10,11,12]. In the most recently available National Electronic Injury Surveillance data for 2017, for example, the product category stairs, ramps, landings and floors is the top-ranked location of injuries in the United States for those 65 years and older, while bathtub and shower structures rank fourth for this age group [13]. Furthermore, when time spent on stairs or in bathrooms (risk exposure time) is taken into account, these locations account for a significantly higher incidence of falls than other room locations (Jake Pauls, personal communications, June 12, 2018). Stairs and bathrooms are problematic because they involve navigating transitions and transfers, and structural features of these locations (such as poor stair geometry or the lack of transfer assists) may challenge an individual’s capacity to respond to the pressure exerted by these environmental features, thereby exceeding optimal person-environment fit parameters [14,15,16,17,18,19,20,21,22,23].
Both primary studies and systematic reviews have documented the effectiveness of efforts to address environmental hazards generally, or more specifically in bathrooms and stairs [4, 6, 24,25,26,27,28,29,30]. Still, studies that assessed the influence of home environmental hazards, or of removing such hazards, on the occurrence of falls have frequently shown no significant associations [5, 31,32,33,34,35,36,37,38,39] or conflicting results [7] even if this relationship makes intuitive sense. It is our contention that these discrepant findings are influenced by how and which hazards are assessed or removed. Indeed, systematic reviews of fall prevention initiatives show that a variety of checklists have been used to assess environmental hazards and that information about their strengths and weaknesses is sparse [4, 6, 40]. Therefore, a review of what environmental hazard checklists have been developed and used is needed to more effectively prevent falls and to assess the potential for data on environmental hazards to inform policies such as building code legislation and regulated universal design.
The purpose of this scoping review was three-fold: a) to summarise how environmental hazards are defined by those developing or using environmental hazard checklists; b) to describe how, where, by whom, and for whom environmental hazard checklists are used; and, c) to examine the characteristics of environmental hazard checklists, with specific attention to features of bathrooms, and stairs/steps assessed in same. This review complements those that have focused on the relationships between falls and environmental hazards [4, 6, 40, 41] and provides a detailed examination of the assessment criteria used for two important locations in homes for injurious falls involving environmental hazards, namely bathrooms and stairs/steps.
Methods
This scoping review was conducted in a systemic manner according to the steps outlined by Arksey and O’Malley [42], and Levac et al. [43]. Reporting follows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement guidelines, as appropriate. Ethics approval was not required.
Identification of relevant articles
Papers were identified using various databases, namely: Medline, Embase, Web of Science, Scopus, CINAHL, AgeLine, HAPI, and PsychTESTS. No restrictions were set regarding the publication year. The search covered articles published up to January 5, 2018. A combination of descriptors (e.g. MESH terms) and key words was used. The authors reviewed the search syntax and strategy and provided additional search terms. The search strategy was finalized after consultation with a professional librarian and tailored for each database (Additional file 1). As an example, the following strategy was used for the search in Medline:
-
(Fall OR accident OR accidental fall)
-
AND (home adj3 hazard* OR environment* adj3 hazard*)
-
AND (housing OR public housing OR Housing for the elderly OR home OR dwelling)
Backward searching from reference lists of reviewed articles was also done.
Inclusion and exclusion criteria
We applied inclusion and exclusion criteria in two stages. The first stage yielded a more complete set of articles, all with at least some information about environmental hazard checklists. For the first stage, the inclusion criteria were:
-
Assess environmental hazards for falls in one or more of the following settings: personal homes or apartments, public housing, and housing for older persons including retirement residences, even if the checklist was not entirely described.
-
Include an assessment of environmental hazards in bathrooms and/or on stairs/steps by lay and/or professional raters (e.g. nurses providing home healthcare services).
-
Involve a population aged 65 years of age or older.
-
Primary research study or research protocols for primary studies.
Exclusion criteria used for this first stage were:
-
Focus exclusively on hospital or long-term care settings.
-
Focus exclusively on a population aged less than 65 years of age (e.g. children).
-
Not written in English or French.
-
Conference and poster abstracts; letters, commentaries, editorials, reviews (e.g. narrative reviews, systematic reviews, meta-analysis studies), and practice guideline papers.
The second stage identified a subset of publications included in stage one that either included the checklists or provided a list of all specific environmental hazards assessed.
Study selection
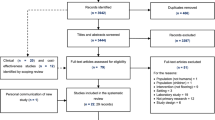
Figure 1 summarizes the two-stage process used to identify and select papers included in this review. The initial database searches yielded a total of 1114 articles. The search in HAPI and PsychTESTS yielded five additional articles, for a total of 1119 articles. All articles were entered in Zotero. Duplicates were removed, leaving 470 articles. First stage inclusion and exclusion criteria were pilot-tested and refined on a subset of 10 random titles and abstracts by the two authors. Titles and abstracts were then reviewed for stage one eligibility by two independent raters (first author and a research associate) and classified as eligible (n = 36), ineligible (n = 284) or unclear (n = 150). Any discrepancies in eligibility were discussed until a consensus was reached. Articles classified as eligible or unclear underwent full-text review by the first author. After full-text review, 105 articles were deemed eligible. An additional 35 eligible articles or checklists were identified through the hand search of reference lists.

Screening process. Screening process for the scoping review on the assessment of environmental hazards for falls on stairs and in bathrooms
A pool of 136 published articles [1, 5, 7, 8, 14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39, 44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64, 65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147] and 4 checklists from the grey literature [148,149,150,151] were included in the first stage of this scoping review. The 136 published articles represented 126 unique studies—nine studies had multiple citations.
From these documents, 42 unique checklists were identified and included in the second stage of this review [8, 15,16,17, 20,21,22,23, 34, 44, 49, 51, 53, 58, 66, 69, 72, 79, 82, 86, 87, 98, 102, 108, 110,111,112, 115, 121, 124, 126, 132, 135, 137, 139, 140, 144, 148,149,150,151,152].
Data extraction
Each of the 140 articles or checklists identified during stage one was read thoroughly and all pertinent information extracted in Excel by the first author. Extraction was overseen by the second author. The key data fields extracted are detailed in Table 1. During stage two, the first author extracted details about which and how hazards were assessed in bathrooms or on stairs/steps (indoor and outdoor). Data extracted about studies described in multiple articles were combined. When checklists were described in multiple articles, data for the checklists were combined from all sources.
An asterisk was inserted in database cells when information was not reported or not applicable. Questions that arose during the process about what data to extract were discussed until consensus was reached. The database is available upon request from the corresponding author.
Data coding and analysis
Stage 1
We grouped studies or checklists into four main categories based on their objectives: 1- developed a checklist and/or tested its validity or reliability; 2- used a checklist to assess environmental hazards or the impact of environmental hazards on falls; 3- used a checklist in an intervention study and/or reported home modifications; 4- not applicable, checklist only. We dichotomized checklists according to reports of psychometric testing (those with versus those without reports of validity and/or reliability testing in current or previous studies) and assessor training (authors did or did not report training of assessors). Checklists were categorized according to whether they assessed solely fall-related hazards or whether they included non-fall-related environmental hazards. The former items were defined as “aspects of the physical environment, including objects, space and the elements in and about the house that pose a risk or danger of causing the person to fall” [56] (p. 171). Items considered unrelated to falls included fire hazards, medication misuse, and wandering.
Descriptive analyses were conducted in IBM SPSS Statistics for Windows (version 24.0, Armonk, NY). We examined whether or not reports of training assessors were associated with reports of developing checklist or testing its validity or reliability (yes/no) using a Pearson chi-square test. We tested the association between time (by 1-year and 5-year period) and the proportion of studies using checklists with prior psychometric testing using Spearman correlations. P values < 0.05 were considered significant.
Stage 2
Detailed information was extracted about how hazards were evaluated in bathrooms and on stairs/steps (indoor and/or outdoor), and if and how person-environment fit was assessed. This data was then content analyzed [43, 153] using two sets of categorical descriptors. First, we rated hazards as structural or non-structural. We defined structural hazards as environmental features that were anchored in walls or on floors (e.g., grab bars affixed to wall, handrails on stairs) or were features of building construction (e.g. stair geometry). We defined non-structural hazards as environmental features that were not anchored in walls or on floors (e.g., presence of bathmats, cluttered stairs). Second, we rated assessment criteria as objective or subjective. We defined objective criteria as defined physical properties not involving personal judgment (e.g. presence of handrail, tread length, lumens of light on stairs). We defined subjective criteria as undefined descriptors requiring the individual judgement of the assessor (e.g., steep or narrow stairs/steps, sturdy handrails or grab bars, slippery surface). Using these definitions, all items for the three locations of hazards (bathrooms, indoor stairs/steps and outdoor stairs/steps) were independently rated by the authors using the two sets of categories for increased internal reliability. Any discrepancies in ratings were discussed until a consensus was reached.
Results
Stage 1
Definitions of environmental hazards
Only 22 studies (17%) provided a definition for the term environmental hazards, and there was considerable variation in these definitions across studies. Most authors who defined hazards, described them by giving examples such as, “features of the home environment such as loose rugs, floor clutter, and poor lighting” [19] (p. 2) or “environmental features such as poor lighting, lack of handrails on staircases, objects in pathways, and slippery rugs” [25] (p. 16). The most comprehensive definition provided was “home fall hazards are aspects of the physical environment, including objects, space and the elements in and about the house that pose a risk or danger of causing the person to fall and, therefore, risk injury” [56] (p. 171).
Geographic location and objectives of studies
The 126 eligible studies and 4 checklists assessed hazards in 25 countries (Additional file 2: Table S1), with the leading sites being USA (n = 43, 33%), Australia (n = 17, 13%) and Canada (n = 13, 10%). Most studies had been undertaken in higher-income countries (n = 112, 86%).
Forty-one per cent (n = 52, 41%) of publications described used a checklist to assess environmental hazards and/or their impact on falls. Another 36% (n = 45, 36%) of publications presented intervention studies that aimed to prevent falls by reducing home environmental hazards. One quarter of studies (n = 32, 25%) reported the development of a checklist or tested its validity or reliability. Six studies were classified simultaneously in two of the above categories (n = 6, 5%), and six additional entries were categorized as solely the environmental hazard checklist (n = 6, 5%).
Checklist used
Seventy-seven different checklists were reported, with just one fourth (n = 19, 25%) used in two or more studies (see Table 2). Five checklists (6%) were used in at least five studies (Additional file 3: Table S2), the Westmead Home Safety Assessment (WeHSA, n = 10) [24, 48, 55,56,57,58, 61, 68, 136, 145], Minimum Data Set–Home Care instrument (MDS-HC; n = 7) [52, 54, 74, 99, 106, 112, 147], Tideiksaar et al. checklist (n = 7) [5, 14, 70, 94, 100, 129, 140], Home Falls and Accidents Screening Tool (HOME FAST; n = 6) [27, 101,102,103, 110, 122], and Housing Enabler Instrument (n = 5) [80, 83, 84, 118, 154]. A majority of studies (n = 57, 74%) used “in house” questionnaires. Only three checklists, the MDS-HC, Housing Enabler and Housing Enabler-screening tool had been used in cross-country studies [49, 80, 83, 84, 112].
Psychometric properties of checklists
Most studies summed up hazardous items into an overall safety score. There was little discussion of the clinical appropriateness of this approach. Studies varied markedly in terms of the psychometric data presented. Some authors reported criterion validity [49, 62, 110, 112, 120, 124], others reported content validity [56, 81, 82, 91, 97, 103] or predictive validity [27]. Only two authors reported sensitivity and specificity of checklists items [62, 103]. Thirty studies reported inter-rater reliability [8, 14, 15, 19, 23, 51, 54, 57,58,59, 72, 77, 80, 81, 84, 85, 98, 103, 106, 110,111,112, 115, 120,121,122,123, 133, 135, 152]; fewer reported test-retest reliability [36, 81, 98, 122] or internal consistency [53, 81, 86, 97]. The inter-rater reliability of checklists, when used by professional and lay older adult pairs, was reported in four studies; three showed that professionals identified more hazards than lay older adults [23, 111, 133] and one showed that lay older adults reported more of some hazards, while professionals reported more of other hazards [110]. Further, the reliability of items on a checklist was often reported as excellent for some but poor for others [8, 19, 58, 80, 103, 110, 111, 115, 121]. Two authors noted that objective items had a higher reliability coefficient than subjective items [19, 80]. Interestingly, no time trend was observed in the proportion of studies using checklists with prior psychometric testing versus checklists without this prior testing (see Fig. 2).

Number of articles published according to whether the checklist used had prior psychometric testing (n = 96)
Study populations
About half of the studies (n = 73, 57%) drew their sample from the general population. The remainder targeted populations at a higher risk of falls such as individuals who had fallen in the previous year; frail individuals; or individuals with mental or visual impairments.
Almost no studies adapted the type of specific home hazards assessed to the specific needs of participants. There were two exceptions. The HEAVI was developed for visually impaired individuals and focusses on related environmental features such as lighting and visual cues [19]. The HEAP was developed for individuals with dementia and includes an assessment of pressure gates at the top and bottom of stairways [15, 78].
Who completed the assessment
Among the studies that assessed environmental hazards (n = 122), evaluations were conducted by occupational therapists (n = 45, 37%), nurses (n = 28, 23%), researchers or research assistants (n = 20, 16%), the participant or a family member (n = 18, 15%), other professionals (n = 16, 13%; e.g.; physicians, home inspectors, house retailers), or physiotherapists (n = 7, 6%). In 17 studies (14%), two or more types of assessors conducted assessments. Assessors were not described in 7 studies (6%). Forty-nine (40%) studies specified that assessors had been trained or had experience in home assessment, and two studies (2%) mentioned that the checklist used does not require prior training in home evaluation or modification [18, 21]. The rest of the studies (n = 69, 57%) provided no details about training. The assessments in 22 (32%) of these latter studies were conducted by occupational therapists. When described, training approaches varied in duration (one-hour to one-week workshop) and format (theoretical lectures, video of home assessment or practical sessions using the checklist in real/mock homes). Studies that described training assessors were more likely to report developing a checklist or testing its validity or reliability (X2 = 15.840, df = 1, p < 0.0001, Table 3).
Stage 2
Most checklists assessed solely fall-related environmental hazards; a quarter of them (n = 10) were imbedded in a checklist designed to also capture non-fall related hazards. As shown in Tables 2 and 4, checklists varied greatly in their length and in the number of bathroom and stair items assessed. Checklists differed with respect to what rooms were assessed (e.g. all bathrooms or bathroom most often used), whether or not outdoor hazards were assessed, and how responses were coded. Some hazards were assessed using dichotomous response categories (e.g.; present/absent); others were coded as continuous variables (e.g.; number of stairs/steps).
Person-environment fit
Most checklists did not assess person-environment fit. There were a few exceptions [15, 34, 53, 58, 69, 83, 87, 98, 102, 110, 140]. Examples of items that assessed person-environment fit included either participants’ self-reports or assessors’ observations of difficulties (or lack or thereof) walking from room to room, over different floor surfaces; climbing and descending stairs/steps; transferring from beds, chairs, and toilets; and getting in and out of bathtubs or showers. Notably, the Housing Enabler Instrument [83] assesses the environment and older adults’ functional limitations separately. Uniquely, these authors provide an analytic matrix and a software program to examine the gap between the environment and the person’s limitations.
Summary of key findings related to bathrooms
Thirty-nine checklists assessed bathrooms. Few checklists indicated which bathroom to assess when there were more than one in the home. As shown in Table 5, a majority of checklists (n = 25, 63%) used mostly subjective items to assess hazards in bathrooms. For instance, they assessed an “awkward toilet seat”, or “slippery floor”. Similarly, over three quarters of checklists (n = 30, 77%) assessed primarily non-structural hazards such as non-skid mats, abrasive strips in the bath or shower, or objects on the bathroom floor. The most frequently assessed structural hazard was the absence of grab bars.
Grab bars
Although most checklists assessed grab bars in bathrooms, there was a lot of variation as to where (in the bathtub, shower and/or next to the toilet) and how they were assessed. For instance, in some checklists, grab bars were assessed with a single item and a bathroom would need to have grab bars in three locations (toilet, bath, shower) not to be hazardous, while in others, grab bars were also assessed with a single item but the presence of only one grab bar was enough to code the item as having the grab bar present. In other studies, each location was assessed separately and one, two or three items were listed in the checklist accordingly. Two checklists coded the lack of grab bars as a hazard only if the person needed them [23, 115], one coded using a grab bar as a hazard [20], and another described grab bars as assistive devices and did not consider their absence to be an environmental hazard [108].
None of the checklists distinguished between diagonal, horizontal or vertical grab bars in the tub/shower; or documented where they were situated (e.g. side wall and/or back wall). Four checklists assessed grab bar placement; one had objective height measures [149], whereas others relied on subjective criteria such as “properly installed” [71], “properly placed” [151], or “can be reached without leaning enough to lose balance” [102]. Four checklists assessed if grab bars were sturdy or well anchored to walls [16, 139, 140, 151]. Illustrations of grab bars in another checklist included two types that were not fixed to a wall [111]. Only three checklists provided a definition of grab bars or specified that towel racks are not grab bars [102, 111, 121].
Summary of key findings related to stairs/steps
Thirty-nine checklists included items on stairs and/or steps. Most (n = 22, 63%) assessed both indoor and outdoor stairs/steps, while eleven (31%) assessed only indoor stairs/steps and two assessed only outdoor stairs/steps. The location of stairs/steps (whether indoors or outdoors) was not differentiated in four of the checklists (10%). Very few checklists assessed the number of stairs/steps or staircases in the home.
Indoor stairs/steps
Among the 33 checklists that assessed indoor stairs/steps, twenty-six (79%) assessed features of stairs/steps not related to handrails (see Table 6). Most checklists (n = 23, 70%) used a majority of subjective items (e.g. stairs/steps in need of repair, sloping or broken steps, stairs too steep) and most (n = 30, 91%) included a majority of structural items. Yet, most structural features assessed were not related to the construction geometry of stairs/steps (e.g., height of riser, tread width).
Indoor handrails
Handrails were the most commonly assessed structural features of stairs/steps (n = 30, 91%). Eight checklists (27%) solely assessed if handrails were present; the others assessed specific features of handrails: sturdiness (n = 18, 60%); height, length and/or if they were continuous (n = 13, 43%); and diameter or ease of grip (n = 7, 23%). There was also variability in the number of handrails that needed to be present to code stairs/steps as not hazardous. For the majority (n = 24, 80%) the presence of only one handrail resulted in this categorization, while for six checklists (n = 6, 20%), two handrails had to be present for this categorization.
Outdoor stairs/steps
There were fewer items and fewer features assessed for outdoor than indoor stairs/steps. Of the 23 checklists that assessed outdoor stairs/steps, eight (35%) assessed some features of stairs/steps other than handrails. Assessment criteria were predominantly subjective in most of these checklists (n = 13, 57%). Most checklists assessed structural hazards (n = 20, 87%). Yet, similarly to indoor stairs/steps, the features assessed were not related to their construction geometry.
Outdoor handrails
Handrails were assessed in 15 (65%) checklists. Almost all of these checklists assessed at least one specific feature of handrails (n = 13, 87%): sturdiness (n = 7, 50%); height, length and/or if they were continuous (n = 5, 31%); and diameter or ease of grip (n = 2, 13%). Similarly to the assessment of indoor handrails, 87% (n = 13) of checklists required the presence of only one handrail to code outdoor stairs/steps as not hazardous.
Discussion
This is the first scoping review to examine the characteristics of environmental hazards checklists. Given the pervasive presence of environmental hazards in homes and their causal relationship with falls and independent functional mobility among the older adults, examining the status and quality of such checklists is imperative.
Despite over three decades of research in this field, there are still no widely used environmental assessment checklists. There is a lot of variability among checklists in terms of the number of items, which parts of the home were assessed, and among those assessing bathrooms and stairs/steps whether checklists emphasized structural or non-structural features or used primarily objective or subjective criteria for assessments. The lack of standardized assessment items in checklists severely limits cross-study comparisons [58]. In 2003, Gitlin concluded that there was a “lack of psychometrically sound measures” to assess home environments and that most assessment methods used were study-specific with unknown reliability and validity [155]. Our review indicates that this conclusion still largely holds. Developing “gold standard” environmental hazards checklists with known psychometric properties is critical to advance the field and inform fall-related prevention practices. This requires the development of a consensus definition of environmental hazards [58], and the identification of priority structural and non-structural attributes of safe bathrooms and safe stairs/steps. There is substantial data available from ergonomic studies to support this prioritization. Furthermore, statistical modeling of the relationship between checklist items and falls would help establish the predictive validity of checklist items, determine if it is clinically appropriate to sum all items into an overall hazard score, and identify priority objective measures for inclusion in abbreviated checklists.
We found limited descriptions of training approaches used and a lack of information on whether or not assessors were trained to use checklists. We recognize that training is costly, but agree with authors who have suggested that training is essential to achieve consistent assessments among raters [57]. For instance, interviewers have been shown to incorrectly identify towel racks as grab bars [8], highlighting the need to train them and to provide definitions of hazards. We also think that scaling-up the use of robust environmental hazard assessment checklists is important; their reach could be extended by training lay people to conduct assessments, and reducing the number of items on hazard checklists.
Given the disproportionately high rate of injurious falls that occur on stairs/steps and in bathrooms [10,11,12], it was surprising to us that checklists did not always include an assessment of these locations and that outdoor stairs/steps were so infrequently included. Outdoor stairs/steps often comprise part of older adults’ walking paths (Edwards & Dulai, under review); affect the visitability of a home; and may be more prone to hazardous characteristics since they may not be covered by building code legislation. In our view, comprehensive environmental hazard checklists need to assess both indoor and outdoor home environments.
Most of the authors describing environmental hazard checklists seemed to conceptualize the environment as an independent static entity, ignoring how older adults interact with their environment or the degree of their exposure [155, 156]. Ideally, checklists that assess person-environment fit and/or dynamic variability of the environment would be used alongside standard checklists, providing more insights on how older adults navigate their home environment in ways that either reduce or increase their risk of falls [157]. For example, checklists should assess whether older adults use stair handrails to compensate for poor balance or use a toilet or bathtub grab bar to aid transfers. Checklists should also contain items and directions pertaining to assessing the dynamic and variable nature of some environmental hazards (e.g. outdoor stairs/steps that were dry versus covered in ice or snow, friction coefficient of wet versus dry bathroom floor, combinations of natural and artificial lighting on stairs/steps that changed at different times of the day) [56].
There has been a tendency to define the problem of environmental risk modification as an individual behaviour change problem rather than as an environmental issue that requires a multi-level and inter-sectoral approach such as building code legislation and regulated universal design [158]. This behavioural emphasis may in part, explain the emphasis on subjective and non-structural items that was evident in checklists that assessed bathrooms and stairs/steps. In the longer-term, policy interventions, are likely to be more effective than behavioural interventions in facilitating some environmental modifications, such as safer stair geometry and universal access to grab bars for toilets, showers and bathtubs [159, 160]. It is imperative that we identify those constellations of hazards that are priorities and best tackled through policy change. This requires cumulative knowledge about the prevalence of structural environmental hazards and their relationship to falls. The inclusion of consistent, objectively-assessed, structural items in environmental hazard checklists could help address this knowledge gap.
Limitations
This review has several limitations. First, we focussed on hazards related to bathrooms and stairs/steps. This may have resulted in the exclusion of a few checklists assessing solely other parts of homes. Second, we did not attempt to access unpublished training manuals for checklists, which may include descriptions of items that would have led us to categorize them as objective rather than subjective. However, most studies did not mention training their assessors or having a training manual, so it seems unlikely that this would have substantially shifted our results. Third, it was sometimes hard to categorize items as structural or non-structural, or as objective or subjective due to the limited descriptors of hazards contained in many checklists. For instance, “dim lightning” could be caused by a lack of proper ceiling light fixtures (structural) or by a burned-out light bulb (non-structural). To improve reliability, both authors independently rated the environmental hazard items on checklists and discussed discrepant results until a consensus emerged. However, it might have been more rigorous to involve an independent rater in this process. Lastly, we did not judge the appropriateness of objective criteria used to evaluate hazards. We did observe that objective criteria were inconsistent across checklists. In the future, an assessment of objective criteria should include a quality assessment against standards such as those suggested in ergonomic studies or those used in existing building code legislation.
Conclusion
The lack of standard definitions and consistent objective criteria for assessing environmental hazards for falls is limiting meaningful cross-study comparisons and slowing advances in this field. This gap may partly explain conflicting results regarding the effectiveness of interventions targeting home environmental hazards (in particular those involving bathrooms and stairs/steps) to prevent falls among older adults. This field of research would be improved with standardized environmental hazard checklists containing objective criteria to assess structural hazards. To inform population health interventions aimed at preventing falls, such as building code regulations or municipal housing by-laws, it is essential to include objectively-assessed, structural hazards in environmental checklists.
Abbreviations
- CDC:
-
Center for Disease Control
- CINAHL:
-
Cumulative Index to Nursing and Allied Health Literature
- HAPI:
-
Health and Psychosocial Instruments
- HEAP:
-
Home Environmental Assessment Protocol
- HEAVI:
-
Home Environment Assessment for the Visually Impaired
- HOME FAST:
-
Home Falls and Accidents Screening Tool
- MAHC-10:
-
Missouri Alliance for Home Care-10
- MDS-HC:
-
Minimum Data Set-Home Care
- MeSH:
-
Medical Subject Headings
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- WeHSA:
-
Westmead Home Safety Assessment
References
Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319:1701–7.
Public Health Agency of Canada. Seniors’ falls in Canada: Second report. 2014. https://www.canada.ca/en/public-health/services/health-promotion/aging-seniors/publications/publications-general-public/seniors-falls-canada-second-report.html. Accessed 29 Sep 2017.
Parachute. The cost of injury in Canada. Toronto: Parachute; 2015.
Clemson L, Mackenzie L, Ballinger C, Close JCT, Cumming RG. Environmental interventions to prevent falls in community-dwelling older people: a meta-analysis of randomized trials. J Aging Health. 2008;20:954–71.
Gill TM, Williams CS, Tinetti ME. Environmental hazards and the risk of nonsyncopal falls in the homes of community-living older persons. Med Care. 2000;38:1174–83.
Gillespie L, Robertson M, Gillespie W, Sherrington C, Gates S, Clemson L, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;9:CD007146. https://doi.org/10.1002/14651858.CD007146.pub3.
Nevitt MC, Cummings SR, Kidd S, Black D. Risk factors for recurrent nonsyncopal falls. A prospective study. JAMA. 1989;261:2663–8.
Sattin RW, Rodriguez JG, DeVito CA, Wingo PA. Home environmental hazards and the risk of fall injury events among community-dwelling older persons. Study to assess falls among the elderly (SAFE) group. J Am Geriatr Soc. 1998;46:669–76.
Speechley M, Tinetti M. Falls and injuries in frail and vigorous community elderly persons. J Am Geriatr Soc. 1991;39:46–52.
Blazewick DH, Chounthirath T, Hodges NL, Collins CL, Smith GA. Stair-related injuries treated in United States emergency departments. Am J Emerg Med. 2017. https://doi.org/10.1016/j.ajem.2017.09.034.
Stevens JA, Haas EN, Haileyesus T. Nonfatal bathroom injuries among persons aged ≥15 years--United States, 2008. J Saf Res. 2011;42:311–5.
Hanba C, Gupta A, Svider PF, Folbe AJ, Eloy JA, Zuliani GF, et al. Forgetful but not forgotten: bathroom-related craniofacial trauma among the elderly. Laryngoscope. 2017;127:820–7.
Consumer Product Safety Commission. 2017 NEISS data highlights: top 20 injury estimates by age. Maryland: Consumer Product Safety Commission; 2018. https://www.cpsc.gov/s3fs-public/2017-NEISS-data-highlights-age.pdf?pKuMH.4NqENxSLIyA9fVd1U0g0F5MGV
Gill TM, Williams CS, Robison JT, Tinetti ME. A population-based study of environmental hazards in the homes of older persons. Am J Public Health. 1999;89:553–6.
Gitlin LN, Schinfeld S, Winter L, Corcoran M, Boyce AA, Hauck W. Evaluating home environments of persons with dementia: interrater reliability and validity of the home environmental assessment protocol (HEAP). Disabil Rehabil. 2002;24:59–71.
Huang TT. Home environmental hazards among community-dwelling elderly persons in Taiwan. J Nurs Res JNR. 2005;13:49–57.
Lan TY, Wu SC, Chang WC, Chen CY. Home environmental problems and physical function in Taiwanese older adults. Arch Gerontol Geriatr. 2009;49:335–8.
Leclerc BS, Bégin C, Cadieux E, Goulet L, Allaire J-F, Meloche J, et al. Relationship between home hazards and falling among community-dwelling seniors using home-care services. Rev Epidemiol Sante Publique. 2010;58:3–11.
Swenor BK, Yonge AV, Goldhammer V, Miller R, Gitlin LN, Ramulu P. Evaluation of the home environment assessment for the visually impaired (HEAVI): an instrument designed to quantify fall-related hazards in the visually impaired. BMC Geriatr. 2016;16:214. https://doi.org/10.1186/s12877-016-0391-2.
Tanner EK. Assessing home safety in homebound older adults. Geriatr Nurs N Y N. 2003;24:250–4 256.
Wyman JF, Croghan CF, Nachreiner NM, Gross CR, Stock HH, Talley K, et al. Effectiveness of education and individualized counseling in reducing environmental hazards in the homes of community-dwelling older women: education and individualized counseling to reduce environmental hazards. J Am Geriatr Soc. 2007;55:1548–56.
Yonge AV, Swenor BK, Miller R, Goldhammer V, West SK, Friedman DS, et al. Quantifying fall-related hazards in the homes of persons with glaucoma. Ophthalmology. 2017;124:562–71.
You L, Deans C, Liu K, Zhang MF, Zhang J. Raising awareness of fall risk among Chinese older adults. Use of the home fall hazards assessment tool. J Gerontol Nurs. 2004;30:35–42.
Cumming RG, Thomas M, Szonyi G, Salkeld G, O’Neill E, Westbury C, et al. Home visits by an occupational therapist for assessment and modification of environmental hazards: a randomized trial of falls prevention. J Am Geriatr Soc. 1999;47:1397–402.
Hornbrook MC, Stevens VJ, Wingfield DJ, Hollis JF, Greenlick MR. Preventing falls among community-dwelling older persons: results from a randomized trial. Gerontologist. 1994;34:16–23.
La Grow SJ, Robertson MC, Campbell AJ, Clarke GA, Kerse NM. Reducing hazard related falls in people 75 years and older with significant visual impairment: how did a successful program work? Inj Prev J Int Soc Child Adolesc Inj Prev. 2006;12:296–301.
Mackenzie L, Byles J, D’Este C. Longitudinal study of the home falls and accidents screening tool in identifying older people at increased risk of falls. Australas J Ageing. 2009;28:64–9.
Palvanen M, Kannus P, Piirtola M, Niemi S, Parkkari J, Jarvinen M. Effectiveness of the Chaos falls clinic in preventing falls and injuries of home-dwelling older adults: a randomised controlled trial. Injury. 2014;45:265–71.
Steinberg M, Cartwright C, Peel N, Williams G. A sustainable programme to prevent falls and near falls in community dwelling older people: results of a randomised trial. J Epidemiol Community Health. 2000;54:227–32.
Sze P-C, Cheung WH, Lam PS, Lo HS, Leung KS, Chan T. The efficacy of a multidisciplinary falls prevention clinic with an extended step-down community program. Arch Phys Med Rehabil. 2008;89:1329–34.
Elley CR, Robertson MC, Garrett S, Kerse NM, McKinlay E, Lawton B, et al. Effectiveness of a falls-and-fracture nurse coordinator to reduce falls: a randomized, controlled trial of at-risk older adults. J Am Geriatr Soc. 2008;56:1383–9.
Hendriks MR, Bleijlevens MH, van Haastregt JC, Crebolder HF, Diederiks JP, Evers SM, et al. Lack of effectiveness of a multidisciplinary fall-prevention program in elderly people at risk: a randomized, controlled trial. J Am Geriatr Soc. 2008;56:1390–7.
Keskinoglu P, Picakciefe M, Bilgic N, Giray H, Karakus N, Ucku R. Home accidents in the community-dwelling elderly in Izmir, Turkey: how do prevalence and risk factors differ between high and low socioeconomic districts? J Aging Health. 2008;20:824–36.
McLean D, Lord S. Falling in older people at home: transfer limitations and environmental risk factors. Aust Occup Ther J. 2010;43:13–8.
Pardessus V, Puisieux F, Di Pompeo C, Gaudefroy C, Thevenon A, Dewailly P. Benefits of home visits for falls and autonomy in the elderly: a randomized trial study. Am J Phys Med Rehabil. 2002;81:247–52.
Pattaramongkolrit S, Sindhu S, Thosigha O, Somboontanot W. Fall-related factors among older, visually-impaired Thais. Pac Rim Int J Nurs Res. 2013;17:181–96.
Peel N, Steinberg M, Williams G. Home safety assessment in the prevention of falls among older people. Aust N Z J Public Health. 2000;24:536–9.
Salminen MJ, Vahlberg TJ, Salonoja MT, Aarnio PTT, Kivelä SL. Effect of a risk-based multifactorial fall prevention program on the incidence of falls: fall prevention and incidence of falls. J Am Geriatr Soc. 2009;57:612–9.
van Bemmel T, Vandenbroucke JP, Westendorp RG, Gussekloo J. In an observational study elderly patients had an increased risk of falling due to home hazards. J Clin Epidemiol. 2005;58:63–7.
Karlsson MK, Vonschewelov T, Karlsson C, CÃster M, Rosengen BE. Prevention of falls in the elderly: a review. Scand J Public Health. 2013;41:442–54.
Chase CA, Mann K, Wasek S, Arbesman M. Systematic review of the effect of home modification and fall prevention programs on falls and the performance of community-dwelling older adults. Am J Occup Ther. 2012;66:284–91.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. https://doi.org/10.1186/1748-5908-5-69.
Bamgbade S, Dearmon V. Fall prevention for older adults receiving home healthcare. Home Healthc Now. 2016;34:68–75.
Bleijlevens MH, Hendriks MR, Van Haastregt JC, Crebolder HF, Van Eijk JT. Lessons learned from a multidisciplinary fall-prevention programme: the occupational-therapy element. Scand J Occup Ther. 2010;17:319–25.
Brotherton SS, Krause JS, Nietert PJ. Falls in individuals with incomplete spinal cord injury. Spinal Cord. 2007;45:37–40.
Camilloni L, Farchi S, Rossi PG, Chini F, Di Giorgio M, Molino N, et al. A case-control study on risk factors of domestic accidents in an elderly population. Int J Inj Control Saf Promot. 2011;18:269–76.
Campbell AJ. Randomised controlled trial of prevention of falls in people aged >=75 with severe visual impairment: the VIP trial. BMJ. 2005;331:817 https://doi.org/10.1136/bmj.38601.447731.55.
Carlsson G, Schilling O, Slaug B, Fänge A, Ståhl A, Nygren C, et al. Toward a screening tool for housing accessibility problems: a reduced version of the housing enabler. J Appl Gerontol. 2009;28:59–80.
Carter SE, Campbell EM, Sanson-Fisher RW, Gillespie WJ. Accidents in older people living at home: a community-based study assessing prevalence, type, location and injuries. Aust N Z J Public Health. 2000;24:633–6.
Carter SE, Campbell EM, Sanson-Fisher RW, Redman S, Gillespie WJ. Environmental hazards in the homes of older people. Age Ageing. 1997;26:195–202.
Cesari M, Landi F, Torre S, Onder G, Lattanzio F, Bernabei R. Prevalence and risk factors for falls in an older community-dwelling population. J Gerontol A Biol Sci Med Sci. 2002;57:M722–6.
Chiu T, Oliver R. Factor analysis and construct validity of the SAFER-HOME. OTJR Occup Particip Health. 2006;26:132–42.
Chou KL, Chi I. The temporal relationship between falls and fear-of-falling among Chinese older primary-care patients in Hong Kong. Ageing Soc. 2007;27:181–93.
Clemson L, Cumming RG, Roland M. Case-control study of hazards in the home and risk of falls and hip fractures. Age Ageing. 1996;25:97–101.
Clemson L, Fitzgerald MH, Heard R. Content validity of an assessment tool to identify home fall hazards: the Westmead home safety assessment. Br J Occup Ther. 1999;62:171–9.
Clemson L, Fitzgerald MH, Heard R, Cumming RG. Inter-rater reliability of a home fall hazards assessment tool. Occup Ther J Res. 1999;19:83–100.
Clemson L, Roland M, Cumming R. Occupational therapy assessment of potential hazards in the homes of elderly people: an inter-rater reliability study. Aust Occup Ther J. 1992;39:23–6.
Clemson L, Roland M, Cumming RG. Types of hazards in the homes of elderly people. Occup Ther J Res. 1997;17:200–13.
Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C. Prevention of falls in the elderly trial (PROFET): a randomised controlled trial. Lancet Lond Engl. 1999;353:93–7.
Close JC, Wesson J, Sherrington C, Hill KD, Kurrle S, Lord SR, et al. Can a tailored exercise and home hazard reduction program reduce the rate of falls in community dwelling older people with cognitive impairment: protocol paper for the i-FOCIS randomised controlled trial. BMC Geriatr. 2014;14:89. https://doi.org/10.1186/1471-2318-14-89.
Daniel H, Oesch P, Stuck A, Born S, Bachmann S, Schoenenberger A. Evaluation of a novel photography-based home assessment protocol for identification of environmental risk factors for falls in elderly persons. Swiss Med Wkly. 2013. https://doi.org/10.4414/smw.2013.13884.
Edwards N, Birkett N, Nair R, Murphy M, Roberge G, Lockett D. Access to bathtub grab bars: evidence of a policy gap. Can J Aging/Rev Can Vieil. 2006;25:295–304.
Diener DD, Mitchell JM. Impact of a multifactorial fall prevention program upon falls of older frail adults attending an adult health day care center. Top Geriatr Rehabil. 2005;21:247–57.
Edwards N, Lockett D, Aminzadeh F, Nair RC. Predictors of bath grab-bar use among community-living older adults. Can J Aging/Rev Can Vieil. 2003;22:217–27.
Edwards NI, Jones DA. Ownership and use of assistive devices amongst older people in the community. Age Ageing. 1998;27:463–8.
El-Faizy M, Reinsch S. Home safety intervention for the prevention of falls. Phys Occup Ther Geriatr. 1994;12:33–49.
Elley CR, Robertson MC, Kerse NM, Garrett S, McKinlay E, Lawton B, et al. Falls assessment clinical trial (FACT): design, interventions, recruitment strategies and participant characteristics. BMC Public Health. 2007;7. https://doi.org/10.1186/1471-2458-7-185.
Evci ED, Ergin F, Beser E. Home accidents in the elderly in Turkey. Tohoku J Exp Med. 2006;209:291–301.
Faul AC, Yankeelov PA, Rowan NL, Gillette P, Nicholas LD, Borders KW, et al. Impact of geriatric assessment and self-management support on community-dwelling older adults with chronic illnesses. J Gerontol Soc Work. 2009;52:230–49.
Fisher GS, Baker A, Koval D, Lishok C, Maisto E. A field test of the cougar home safety assessment (version 2.0) in the homes of older persons living alone. Aust Occup Ther J. 2007;54:124–30.
Fisher GS, Coolbaugh K, Rhodes C. A field-test of the cougar home safety assessment for older persons: version 1.0. Californian J Health Promot. 2006;4:181–96.
Fitzharris MP, Day L, Lord SR, Gordon I, Fildes B. The Whitehorse NoFalls trial: effects on fall rates and injurious fall rates. Age Ageing. 2010;39:728–33.
Fletcher PC, Hirdes JP. Risk factors for falling among community-based seniors using home care services. J Gerontol A Biol Sci Med Sci. 2002;57:M504–10.
Gershon RR, Dailey M, Magda LA, Riley HE, Conolly J, Silver A. Safety in the home healthcare sector: development of a new household safety checklist. J Patient Saf. 2012;8:51–9.
Gill TM, Robison JT, Williams CS, Tinetti ME. Mismatches between the home environment and physical capabilities among community-living older persons. J Am Geriatr Soc. 1999;47:88–92.
Gitlin LN, Winter L, Dennis MP, Corcoran M, Schinfeld S, Hauck WW. A randomized trial of a multicomponent home intervention to reduce functional difficulties in older adults. J Am Geriatr Soc. 2006;54:809–16.
Gitlin LN, Hodgson N, Piersol CV, Hess E, Hauck WW. Correlates of quality of life for individuals with dementia living at home: the role of home environment, caregiver, and patient-related characteristics. Am J Geriatr Psychiatry. 2014;22:587–97.
Greene D, Sample P, Fruhauf C. Fall-prevention pilot: Hazard survey and responses to recommendations. Occup Ther Health Care. 2009;23:24–39.
Helle T, Nygren C, Slaug B, Brandt A, Pikkarainen A, Hansen A-G, et al. The Nordic housing enabler: inter-rater reliability in cross-Nordic occupational therapy practice. Scand J Occup Ther. 2010;17:258–66.
Huang TT, Acton GJ. Effectiveness of home visit falls prevention strategy for Taiwanese community-dwelling elders: randomized trial. Public Health Nurs Boston Mass. 2004;21:247–56.
Isberner F, Ritzel D, Sarvela P, Brown K, Hu P, Newbolds D. Falls of elderly rural home health clients. Home Health Care Serv Q. 1998;17:41–51.
Iwarsson S, Horstmann V, Carlsson G, Oswald F, Wahl H-W. Person—environment fit predicts falls in older adults better than the consideration of environmental hazards only. Clin Rehabil. 2009;23:558–67.
Iwarsson S, Nygren C, Slaug B. Cross-national and multi-professional inter-rater reliability of the housing enabler. Scand J Occup Ther. 2005;12:29–39.
Iwarsson S, Slaug B, Fänge AM. The housing enabler screening tool: feasibility and interrater agreement in a real estate company practice context. J Appl Gerontol. 2012;31:641–60.
Johnson M, Cusick A, Chang S. Home-screen: a short scale to measure fall risk in the home. Public Health Nurs Boston Mass. 2001;18:169–77.
Kamei T, Kajii F, Yamamoto Y, Irie Y, Kozakai R, Sugimoto T, et al. Effectiveness of a home hazard modification program for reducing falls in urban community-dwelling older adults: a randomized controlled trial. Jpn J Nurs Sci. 2015;12:184–97.
Kampe K, Kohler M, Albrecht D, Becker C, Hautzinger M, Lindemann U, et al. Hip and pelvic fracture patients with fear of falling: development and description of the “step by step” treatment protocol. Clin Rehabil. 2017;31:571–81.
Keall MD, Howden-Chapman P, Baker MG, Kamalesh V, Cunningham M, Cunningham C, et al. Formulating a programme of repairs to structural home injury hazards in New Zealand. Accid Anal Prev. 2013 Aug;57:124–30.
Keall MD, Baker M, Howden-Chapman P, Cunningham M. Association between the number of home injury hazards and home injury. Accid Anal Prev. 2008;40:887–93.
Kittipimpanon K, Amnatsatsue K, Kerdmongkol P, Maruo SJ, Nityasuddhi D. Development and evaluation of a community-based fall prevention program for elderly Thais. Pac Rim Int J Nurs Res. 2012;16:222–35.
Lamontagne I, Lévesque B, Gingras S, Maurice P, Verreault R. Dangers environnementaux de chute dans des habitations à loyer modique pour personnes âgées [Environmental hazards for falls in elders in low income housing]. Rev Epidemiol Sante Publique. 2004;52:19–27.
Larsen ER, Mosekilde L, Foldspang A. Correlates of falling during 24 h among elderly Danish community residents. Prev Med. 2004;39:389–98.
Leclerc BS, Begin C, Cadieux E, Goulet L, Leduc N, Kergoat MJ, et al. Risk factors for falling among community-dwelling seniors using home-care services: an extended hazards model with time-dependent covariates and multiple events. Chronic Dis Can. 2008;28:111–20.
Leclerc BS, Bégin C, Cadieux E, Goulet L, Allaire J-F, Meloche J, et al. A classification and regression tree for predicting recurrent falling among community-dwelling seniors using home-care services. Can J Public Health Rev Can Sante Publique. 2009;100:263–7.
Lee HC, Chang KC, Tsauo JY, Hung JW, Huang YC, Lin SI, et al. Effects of a multifactorial fall prevention program on fall incidence and physical function in community-dwelling older adults with risk of falls. Arch Phys Med Rehabil. 2013;94:606–15.
Letts L, Marshall L. Evaluating the validity and consistency of the SAFER tool. Phys Occup Ther Geriatr. 1996;13:49–66.
Letts L, Scott S, Burtney J, Marshall L, McKean M. The reliability and validity of the safety assessment of function and the environment for rehabilitation (SAFER tool). Br J Occup Ther. 1998;61:127–32.
Leung A, Chi I, Lou VWQ, Chan KS. Psychosocial risk factors associated with falls among Chinese community-dwelling older adults in Hong Kong. Health Soc Care Community. 2010;18:272–81.
Lowery K, Buri H, Ballard C. What is the prevalence of environmental hazards in the homes of dementia sufferers and are they associated with falls. Int J Geriatr Psychiatry. 2000;15:883–6.
Lowton K, Laybourne AH, Whiting DG, Martin FC. Can fire and rescue services and the National Health Service work together to improve the safety and wellbeing of vulnerable older people? Design of a proof of concept study BMC Health Serv Res. 2010;10:327. https://doi.org/10.1186/1472-6963-10-327.
Mackenzie L, Byles J, Higginbotham N. Designing the home falls and accidents screening tool (HOME FAST): selecting the items. Br J Occup Ther. 2000;63:260–9.
Mackenzie L, Byles J, Higginbotham N. Reliability of the home falls and accidents screening tool (HOME FAST) for identifying older people at increased risk of falls. Disabil Rehabil. 2002;24:266–74.
Mahoney JE, Shea TA, Przybelski R, Jaros L, Gangnon R, Cech S, et al. Kenosha county falls prevention study: a randomized, controlled trial of an intermediate-intensity, community-based multifactorial falls intervention: multifactorial falls intervention. J Am Geriatr Soc. 2007;55:489–98.
Mann WC, Hurren D, Tomita M, Bengali M, Steinfeld E. Environmental problems in homes of elders with disabilities. Occup Ther J Res. 1994;14:191–211.
Markle-Reid M, Browne G, Gafni A, Roberts J, Weir R, Thabane L, et al. A cross-sectional study of the prevalence, correlates, and costs of falls in older home care clients “at risk” for falling. Can J Aging Rev Can Vieil. 2010;29:119–37.
Marquardt G, Johnston D, Black BS, Morrison A, Rosenblatt A, Lyketsos CG, et al. A descriptive study of home modifications for people with dementia and barriers to implementation. J Hous Elder. 2011;25:258–73.
Marshall SW, Runyan CW, Yang J, Coyne-Beasley T, Waller AE, Johnson RM, et al. Prevalence of selected risk and protective factors for falls in the home. Am J Prev Med. 2005;28:95–101.
Matchar DB, Duncan PW, Lien CT, Ong MEH, Lee M, Gao F, et al. Randomized controlled trial of screening, risk modification, and physical therapy to prevent falls among the elderly recently discharged from the emergency department to the community: the steps to avoid falls in the elderly study. Arch Phys Med Rehabil. 2017;98:1086–96.
Mehraban AH, Mackenzie LA, Byles JE. A self-report home environment screening tool identified older women at risk of falls. J Clin Epidemiol. 2011;64:191–9.
Morgan R, Devito C, Stevens J, Branche C, Virnig B, Wingo P, et al. A self-assessment tool was reliable in identifying hazards in the homes of elders. J Clin Epidemiol. 2005;58(12):1252–9.
Morris JN, Fries BE, Steel K, Ikegami N, Bernabei R, Carpenter GI, et al. Comprehensive clinical assessment in community setting: applicability of the MDS-HC. J Am Geriatr Soc. 1997;45:1017–24.
Nikolaus T, Bach M. Preventing falls in community-dwelling frail older people using a home intervention team (HIT): results from the randomized falls-HIT trial. J Am Geriatr Soc. 2003;51:300–5. https://doi.org/10.1046/j.1532-5415.2003.51102.x.
Northridge ME, Nevitt MC, Kelsey JL. Non-syncopal falls in the elderly in relation to home environments. Osteoporos Int. 1996;6:249–55.
Northridge ME, Nevitt MC, Kelsey JL, Link B. Home hazards and falls in the elderly: the role of health and functional status. Am J Public Health. 1995;85:509–15.
Oliver R, Blathwayt J, Brackley C, Tamaki T. Development of the safety assessment of function and the environment for rehabilitation (SAFER) tool. Can J Occup Ther Rev Can Ergother. 1993;60:78–82.
Pereira CL, Baptista F, Infante P. Role of physical activity in the occurrence of falls and fall-related injuries in community-dwelling adults over 50 years old. Disabil Rehabil. 2014;36:117–24.
Rantakokko M, Törmäkangas T, Rantanen T, Haak M, Iwarsson S. Environmental barriers, person-environment fit and mortality among community-dwelling very old people. BMC Public Health. 2013;13. https://doi.org/10.1186/1471-2458-13-783.
Renfro MO, Fehrer S. Multifactorial screening for fall risk in community-dwelling older adults in the primary care office: development of the fall risk assessment & screening tool. J Geriatr Phys Ther. 2011;34:174–83.
Ritchey KC, Meyer D, Ice GH. Non-therapist identification of falling hazards in older adult homes using digital photography. Prev Med Rep. 2015;2:794–7.
Rodriguez JG, Baughman AL, Sattin RW, de Vito CA, Ragland DL, Bacchelli S, et al. A standardized instrument to assess hazards for falls in the home of older persons. Accid Anal Prev. 1995;27:625–31.
Romli MH, Mackenzie L, Lovarini M, Tan MP, Clemson L. The interrater and test-retest reliability of the home falls and accidents screening tool (HOME FAST) in Malaysia: using raters with a range of professional backgrounds. J Eval Clin Pract. 2017;23:662–9.
Russell MA, Hill KD, Blackberry I, Day LL, Dharmage SC. Falls risk and functional decline in older fallers discharged directly from emergency departments. J Gerontol A Biol Sci Med Sci. 2006;61:1090–5.
Sadasivam RS, Luger TM, Coley HL, Taylor BB, Padir T, Ritchie CS, et al. Robot-assisted home hazard assessment for fall prevention: a feasibility study. J Telemed Telecare. 2014;20:3–10.
Salkeld G, Cumming RG, O’Neill E, Thomas M, Szonyi G, Westbury C. Cost effectiveness of a home hazard reduction program to reduce falls among older persons. Aust N Z J Public Health. 2000;24:265–71.
Lim YM, Sung MH. Home environmental and health-related factors among home fallers and recurrent fallers in community dwelling older Korean women: falls in Korean older women. Int J Nurs Pract. 2012;18:481–8.
Scharlach AE, Graham CL, Berridge C. An integrated model of co-ordinated community-based care. Gerontologist. 2015;55:677–87.
Schwarz DF, Grisso JA, Miles C, Holmes JH, Sutton RL. An injury prevention program in an urban African-American community. Am J Public Health. 1993;83:675–80.
Shaw FE, Bond J, Richardson DA, Dawson P, Steen IN, McKeith IG, et al. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: randomised controlled trial. BMJ. 2003;326:73 https://doi.org/10.1136/bmj.326.7380.73.
Sheffield C, Smith CA, Becker M. Evaluation of an agency-based occupational therapy intervention to facilitate aging in place. Gerontologist Gerontologist. 2013;53:907–18.
Sjosten NM, Salonoja M, Piirtola M, Vahlberg T, Isoaho R, Hyttinen H, et al. A multifactorial fall prevention programme in home-dwelling elderly people: a randomized-controlled trial. Public Health. 2007;121:308–18.
Sophonratanapokin B, Sawangdee Y, Soonthorndhada K. Effect of the living environment on falls among the elderly in Thailand. Southeast Asian J Trop Med Public Health. 2012;43:1537–47.
Sorcinelli A, Shaw L, Freeman A, Cooper K. Evaluating the safe living guide: a home hazard checklist for seniors. Can J Aging/Rev Can Vieil. 2007;26:127–37.
Staeger P, Burnand B, Santos-Eggimann B, Klay M, Siffert C, Livio JJ, et al. Prevention of recurrent hip fracture. Aging Clin Exp Res. 2000;12:13–21.
Stalenhoef P, Diederiks J, Knottnerus A, Witte LD, Crebolder H. How predictive is a home-safety checklist of indoor fall risk for the elderly living in the community? Eur J Gen Pract. 1998;4:114–20.
Stark S, Somerville E, Keglovits M, Conte J, Li M, Hu YL, et al. Protocol for the home hazards removal program (HARP) study: a pragmatic, randomized clinical trial and implementation study. BMC Geriatr. 2017;17:90. https://doi.org/10.1186/s12877-017-0478-4.
Stevens M, Holman CD, Bennett N. Preventing falls in older people: impact of an intervention to reduce environmental hazards in the home. J Am Geriatr Soc. 2001;49:1442–7.
Stevens M, Holman CD, Bennett N, de Klerk N. Preventing falls in older people: outcome evaluation of a randomized controlled trial. J Am Geriatr Soc. 2001;49:1448–55.
The prevention of falls in later life. A report of the Kellogg International Work Group on the Prevention of Falls by the Elderly. Dan Med Bull. 1987;34(Suppl 4):1–24.
Tideiksaar R. Fall prevention in the home. Top Geriatr Rehabil. 1987;3:57–64.
Trader SE, Newton RA, Cromwell RL. Balance abilities of homebound older adults classified as fallers and nonfallers. J Geriatr Phys Ther. 2003;26:3–8.
Tynan C, Cardea JM. Home health hazard assessment. J Gerontol Nurs. 1987;13:25–8.
van Haastregt JCM, van Rossum E, Diederiks JPM, Voorhoeve PM, de Witte LP, Crebolder HFJM. Preventing falls and mobility problems in community-dwelling elders: the process of creating a new intervention. Geriatr Nur. 2000;21:309–14.
Vladutiu CJ, Casteel C, Marshall SW, McGee KS, Runyan CW, Coyne-Beasley T. Disability and home hazards and safety practices in US households. Disabil Health J. 2012;5:49–54.
Wesson J, Clemson L, Brodaty H, Lord S, Taylor M, Gitlin L, et al. A feasibility study and pilot randomised trial of a tailored prevention program to reduce falls in older people with mild dementia. BMC Geriatr. 2013;13:89.
Yates SM, Dunnagan TA. Evaluating the effectiveness of a home-based fall risk reduction program for rural community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2001;56:M226–30.
Yoo IY. Recurrent falls among community-dwelling older Koreans: prevalence and multivariate risk factors. J Gerontol Nurs. 2011;37:28–40.
Centers for Disease Control and Prevention. Check for safety: A home fall prevention checklist for older adults. 2005 https://www.cdc.gov/steadi/pdf/check_for_safety_brochure-a.pdf .
Iwarsson S, Björn S. Environmental component, the complete housing enabler instrument. 2010. http://www.enabler.nu/Environmental_component.pdf. Accessed 14 Nov 2017.
Keall M, Baker M, Howden-Chapman P, Cunningham M, Cunningham C. Healthy housing index pilot study. Final report.2007. Wellington, New Zeland: He Kainga Oranga / Housing and Health Research Programme, Department of Public Health, University of Otago; 2006.
Public Health Agency of Canada. The Safe Living Guide—A guide to home safety for seniors. Ottawa: Public Health Agency of Canada; 2015.
Zhang L, Yan T, You L, Li K, Gao Y. Social isolation and physical barriers in the houses of stroke survivors in rural China. Arch Phys Med Rehabil. 2016;97:2054–60.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–88.
Iwarsson S. The housing enabler: an objective tool for assessing accessibility. Br J Occup Ther. 1999;62:491–7.
Gitlin LN. Conducting research on home environments: lessons learned and new directions. Gerontologist. 2003;43:628–37.
Wahl HW, Fange A, Oswald F, Gitlin LN, Iwarsson S. The home environment and disability-related outcomes in aging individuals: what is the empirical evidence? Gerontologist. 2009;49:355–67.
Nygren C, Oswald F, Iwarsson S, Fänge A, Sixsmith J, Schilling O, et al. Relationships between objective and perceived housing in very old age. Gerontologist. 2007;47:85–95.
Edwards NC. Preventing falls among seniors: the way forward. J Saf Res. 2011;42:537–41.
Edwards N. Chapter 15: knowledge translation for intersectoral action: the case of Canada’s building codes. In: Bourgeault IL, Labonte R, Packer C, Runnels V, editors. Population health in Canada: issues, research, and action. Toronto: Canada Scholars Press; 2017. p. 156–60.
Monson AZ, Pauls J, Leverett M. Applying the regulatory powers of public health. J Law Med Ethics. 2003;31(4 Suppl):68–9.
Acknowledgements
The authors would like to thank Yeonjung Yoo for her help screening potential articles.
Availability of data and material
The datasets used during the current study are available from the corresponding author on reasonable request.
Funding
This research was carried out with funding support from the Canadian Institutes of Health Research, grant number #122510.
Author information
Authors and Affiliations
Contributions
RB: Contributed to the study design, acquired and extracted data for analysis, performed statistical analyses, interpreted the data and drafted the manuscript. NE: Designed the study, oversaw data extraction, interpreted the data, drafted some sections of the manuscript and edited the overall manuscript for critical content. Both authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Since this scoping review did not involve primary research or human subjects, no ethics approval or participant consent was required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Detailed search strategy (DOCX 19 kb)
Additional file 2:
Table S1. Environmental hazard checklists used by country (XLSX 15 kb)
Additional file 3:
Table S2. Characteristics of assessment tools used in five studies or more (XLSX 17 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Blanchet, R., Edwards, N. A need to improve the assessment of environmental hazards for falls on stairs and in bathrooms: results of a scoping review. BMC Geriatr 18, 272 (2018). https://doi.org/10.1186/s12877-018-0958-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-018-0958-1