
Abstract
Background
Self-reported health is a widely used measure of health status across individuals. As the ageing population increases, the health of the elderly also becomes of growing concern. The elderly go through life facing social, economic and financial hardships. These hardships are known to affect the health status of people as they age. The purpose of this study is to assess social and health related factors of self-reported health among the elderly in Ghana.
Methods
A multivariate regression analysis in form of a binary and ordinal logistic regression were used to determine the association between socioeconomic, demographic and health related factors, on self-reported health. The data used for this study was drawn from the World Health Organization (WHO) Study on Global Ageing and Adult Health (SAGE) Wave 1.
Results
In total, out of 2613 respondent, 579 (20.1%) rated their health status as poor and 2034 (79.9%) as good. The results showed that the odds of reporting poor health was 2.5 times higher among the old-old compared to the young old. The elderly with one or more than one chronic condition had the odds of 1.6 times and 2 times respectively, of reporting poor health. Engaging in mild to moderate exercise increased the chances of reporting poor health by 1.8 times. The elderly who had never worked in a lifetime were 2 times more likely to report poor health. In the same way, residents of Eastern and Western parts of Ghana were 2 times more likely to report poor health compared to those in the Upper West region. Respondents with functional limitations and disabilities were 3.6 times and 2.4 times respectively, more likely to report poor health. On the other hand, the odds of reporting poor health was 29, 36 and 27% less among respondents in the highest income quintiles, former users of tobacco and those satisfied with certain aspects of life respectively. Also, current alcohol users were 41% less likely to report poor health.
Conclusion
The health status of the elderly is to an extent determined by the circumstances in which they are born, grow and live. The findings suggest that addressing social issues faced by individuals in youthful age will go a long way to achieving good health in the future. People with physical limitations and disabilities are most vulnerable to unmet healthcare needs and support system from government, policy makers and family.
Similar content being viewed by others


Background
Self-reported health (SRH) has been used by many researchers as a proxy for measuring individual health state, including that of the elderly [1,2,3]. It not only measures current and long term health status but also predicts mortality [4]. Self-reported health which comprises of all three aspects of health: social, mental and physical wellbeing has been widely studied in the western world using different methods. Most findings show a significant relationship between certain social, economic and demographic factors and SRH. It is important to examine past life experiences of elderly persons together with individual characteristics when exploring differences in reporting health. Some of these experiences include cultural factors, historical (wars), individual and national factors (availability of health services) [5]. In North Korea, for example, among North Korean refuges living in South Korea, Wang et al. found poor SRH to be related to individuals of low socioeconomic statues, elderly females and those with physical and mental disabilities including other chronic conditions [6], owing to past wartime experiences and economic recession. Other studies have found that individual factors like low educational attainment increases the chances of reporting poor health [7, 8]. A possible pathway could be through lack of employment, low economic condition and consequential inability to take care of healthcare needs. In the same way, socio-cultural factors have an impact on SRH across racial-ethnic groups [9] owing to the different perception of health. To be precise, objective health states such as presence of chronic condition is positively associated with poor health among the less racially discriminated blacks, while demographic factors are highly associated with SRH among the most racially discriminated African Americans.
Evidence have also shown that being single or divorced increases the chance of reporting poor health [10]. This is often associated with emotional instability, loneliness as well as economic vulnerability. In the same light, low income, poor lifestyle choices such as smoking, excessive drinking and lack of exercise are other risk factors associated with poor health [11]. Smoking for example increases the chances of dying from medical conditions like ischemic heart disease, lung cancer, stroke and coronary heart disease [12, 13]. Sedentary lifestyle can predispose one to these diseases as well. However, research shows that physical activity in the form of exercise has the potential of reducing the onset of chronic disease and thus improve health outcome [14, 15]. Some of these health consequences are reversible when the individual is no longer exposed to these poor habits. In terms of physical health states, there is a growing body of evidence that relates functional limitation and disabilities to poor health [16,17,18]. Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) are used globally to measure functional health states of adults [19, 20]. These health states, IADL often present in states of mild cognitive impairment or early dementia [21] whereas ADL declines present in the late stages of dementia [22]. Exploring what drives SRH among elderly persons will provide baseline evidence to uphold public health promotive and preventive strategies against disease onset. Some school of thought hold that SRH can be better understood when an attempt is made to explore the rationale behind the responses in order to illustrate the sociocultural context of how individuals assess their health state [23].
The population of the world is ageing. The number of people aged 60 years and older have been projected to increase from its current state of 800 million to two billion by the year 2050 [24]. In Ghana for example, the population of the elderly (ages 60 years and above) is expected to double from its current state of 6.7% of the national population to more than 12% by the year 2050 [25]. Indeed, the age structure of Ghana’s population is gradually changing following the global pattern. This can be attributed to the decline in mortality and fertility rates and an increase in life expectancy, from advancement in medical technology and improved living standards [26]. Concerning elderly health, few studies exist on the elderly with respect to SRH and risk factors in Ghana. One of such health related risk factor among elderly Ghanaians is the presence of chronic diseases. The most common of them include cardiovascular diseases, cancers, respiratory diseases, arthritis and other infectious diseases [27]. Other health challenges include chronic malnutrition, anemia, osteoporosis, hearing and sight problems. In general, causes of chronic conditions are multifaceted ranging from genetic predisposition, poor lifestyle decisions to poor social and economic conditions, all these having as consequence, a negative impact on elderly health status [28, 29]. With the rising prevalence of chronic diseases, the health system in Ghana is less prepared to meet the health care needs of the elderly, with little infrastructure and few specialized personnel for older populations [30]. Further, in terms of health access, Saeed et al. found that most elderly persons in Ghana reporting poor health use health facilities more owing to the National Health Insurance policy which offers free healthcare to elderly persons above 70 years [31]. While this is seen as a positive development at national level, the quality of services rendered are not encouraging and the range of services offered are limited.
Although elderly women in Ghana have longer life expectancy than men, they report worst health outcomes compared to men [32]. This is in line with other studies that have shown gender difference in reporting poor health [33, 34]. Also among elderly Ghanaians, Debpuur et al. [35] found SRH to be associated with education, functional limitation and lifetime employment. However, this single study on SRH in Ghana used primary data from one rural district, which is not representative of the national situation. Given variations in health status across locality, this study aims to assess the factors that influence the health status of the elderly, with self-reported health as a measure of health outcome using a national-level dataset. It is worth noting that most interventions in Ghana focus on children and youthful population, with little emphasis on the elderly. Understanding what explains SRH among elderly persons in Ghana is thus a first step to improving their health state through successful implementation of policies, interventions and programs.
Methods
The aim, design and setting of the study
The aim of the study was to assess factors associated with SRH among the elderly in Ghana. The study used secondary data obtained from a cross national Study of Global Ageing and Adult health (SAGE) Wave 1, a cross sectional study conducted in Ghana from 2007 to 2010 by the World Health Organization (WHO). The data was obtained from the WHO, publicly available online with no identifiable information on participants [36]. Prior to the study, 30 interviewers and supervisors were trained in two phases in Accra, supported by WHO Geneva. There were a total of four interviewers and a supervisor for each primary sampling unit. They interviewed at most two respondents per day and each interview lasted for at most 30 min [37]. For quality control measures, the supervisors checked to ensure that proxy interviews were justifiable and completed. In addition, selected variables in the questionnaires were re-tested a week after initial interview for consistencies.
The study sample was stratified by 10 administrative regions and then by locality into urban and rural areas. A total of 20 strata were identified. In the urban and rural areas, census enumerated areas were used as the sampling frame. A total of 251 census enumerated areas were identified. Enumerated areas were then selected from each stratum based on the size of the population of the elderly in that area. Twenty households were randomly selected from each enumerated area. Adults older than 50 years were selected from each household, and individuals between the ages of 18–24 years were selected as proxies. The analysis in this study defines the elderly as those aged 60 and above resulting in a sample of 2613 individuals. The data was collected by face to face interviewer administered questionnaires to each household and individual respondent. The questionnaires were divided into various sections that assessed the different characteristics of the elderly such as socio-demographic characteristics, work history and benefits, health state descriptions, chronic conditions and health services coverage.
Description of materials
Dependent variable
The dependent variable used for this study was self- reported health. The survey contained the following questions as it relates to SRH: ‘How do you rate your health today?’ Responses were rated on a 5-point scale as ‘very good’ (1), ‘good’ (2), ‘fair’ (3), ‘poor’ (4), and ‘very poor’ (5). Responses were further classified into a dichotomous measure; ‘good health (very good/good/fair) defined as optimal health state and coded as 0, while poor health (/poor/very poor) as less than optimal health, coded as 1. This approach of dichotomizing the health variable was adopted from previous studies on self-reported health [38,39,40]. We used similar approach which include SRH as the dependent variable comprising of good health, 0 and poor health 1. Other approaches have been used by different scholars. For example, Arnadotti and colleagues analyzed all five health states of SRH using ordinal logistic regression [41] whereas Wu et al. used three SRH states good, fair and poor [42]. For the purpose of sensitivity, we used an ordinal logit model, using all five health states to have a broad perspectives of factors associated with SRH among elderly persons in Ghana. That is, SRH was coded as 5 when very poor, and 1–4 otherwise.
Independent variables
The explanatory variables include demographic factors such as age, sex, marital status. Following the classification by the 2010 population census in Ghana, age was classified into three groups - the young old (60–69), the middle old (70–79) and the old-old (above 80) [43, 44]. In respect to marital status, respondents were classified as never married, married/cohabiting, separated/divorced and widowed. Socioeconomic factors included income, education and work status. Income was grouped into five quintiles (highest, high, middle, low and lowest). It was reclassified into three categories; high (high/highest), middle income (middle), low income (low/lowest). The SAGE study relied on income from household assets, dwellings characteristics and reported incomes which were converted into income quintiles, with quintile 1 representing the lowest income and quintile 5 representing the highest income. Education was grouped into (no formal education, primary education, secondary and tertiary education). Lifetime work status was grouped into four categories (never worked, private employer, public employer and informal). Health insurance status categorized into two groups, being insured and uninsured.
The classification of chronic diseases were based on the respondent’s response to the question ‘In the past 12 months, have you been told by a medical professional you had any of the following conditions (diabetes, hypertension, arthritis, angina, stroke, chronic lung disease, depression and asthma?’ Three categories were formed from the responses given, no chronic condition, one chronic condition and more than one chronic condition.
Functioning assessment was evaluated using the questions from SAGE questionnaire found under the section Health State Description. Functional limitation was measured using ADL. Respondents were asked if they had difficulties in carrying out any of the following eight activities (sitting, walking, standing from sitting, long periods of standing, climbing stairs, kneeling, picking up things and taking care of household responsibilities). Each of these 8 items were classified on a four point response scale. A dichotomy measure was constructed grouping no limitations in any of the activities as 0 and mild to severe limitations as 1. Respondents were considered functionally limited if they experienced difficulties in carrying out 4 or more of these activities. Disability was constructed based on the World Health Organization Disability Assessment Schedule (WHODAS 2.0) made up of 15 questions also referred to as IADL [35, 45]. Respondents were considered disabled if they had difficulties in performing 7 or more of these 15 activities [46].
In terms of subjective wellbeing, respondents were asked how satisfied they were with their health state, themselves, personal relationships, living conditions and in general life. Subjective wellbeing was seen to be good if respondents were satisfied with four or five of the domains and poor if satisfied with three or less. A self-reported response of how well respondents rated their quality of life was used to construct the quality of life variable. Responses were rated on a 5 point scale: ‘very good’ ‘good’ ‘fair’ ‘bad’ and ‘very bad.’ Very good and good responses were grouped as good quality of life, fair, bad and very bad as poor quality of life.
Lifestyle factors include use of any of the following tobacco products like cigarettes, cigars, pipe, chewing tobacco or snuff, alcohol use and physical activity. Respondents were grouped into three groups “never used”, “previously used” and “currently use” tobacco. Alcohol was grouped into three groups as well, “non-drinkers” of alcohol, “previous drinkers” and “current drinkers”. Physical activity was assessed on the basis of any form of moderate to intensity sports that increased the heart rate for at least 10 min a day.
Geographical characteristics include urban-rural locality and regions (Upper West, Western, Upper East, Central, Ashanti, Brong Ahafo, Northern, Eastern, Greater Accra and Volta). Upper West is considered the poorest region in the country hence was used as the base case for comparison with other regions.
Statistical analysis
STATA version 13 was used as statistical package for data analysis. First, a descriptive analysis was done to describe the general characteristics of the study population. Second, we explored the difference in reporting SRH against the independent variables, reporting p-values of Pearson’s Chi2. Third, a multivariate analysis in the form of a binary logistic regression and an ordinal regression analysis were used to determine the association between social/health related factors and self-reported health. Odd’s ratio (OR) was used as a measure of effect. The level of significance was set at a 95% confidence interval with a p-value of 0.05.
Background characteristics of respondents
Out of 2613 respondents, 20% reported poor health and 80% reported good health (Table 1). The young old (60–69 years) represented 45% of the sample, middle old (70–79 years) 38% and the old-old (80 and above), 17% of the entire population. Equal number of males (50%) and females (50%) were represented in the sample. In terms of marital status, most respondents were married (49%), followed by 37% of elderly persons who had lost a spouse. More than half (66%) elderly persons had never been to school and just a small proportion (3%) had completed tertiary education.
Table 1 further shows that the highest proportion of respondents (87%) were employed in the informal sector, and just a few employees (8 and 3%) in the public and private sectors respectively. Fifty seven percent of elderly Ghanaians lack health insurance coverage while 43% had some form of insurance coverage. With respect to comorbidities, 24% elderly men and women had one of the eight chronic conditions explored in this study and 12% had more than one of these conditions. Forty two percent were considered poor and most (61%) lived in the rural areas. In terms of subjective well-being, 66% elderly persons were unsatisfied with life and their surroundings, 60% rated poor quality of life, 49% were functionally limited and 38% were classified as disabled.
Lifestyle factors assessed showed that the same proportion of elderly Ghanaians (78%) do not exercise or take any form of tobacco. In terms of drinking habits, 47% elderly men and women do not drink, 24% were previous drinkers and 27% current drinkers. Based on regions, the table shows that most (15%) elderly persons were from the Ashanti region, followed by the Eastern (14%) and Western (11.3%) regions respectively. Just a few proportions were from the Upper West (3%).
Summary statistic of the population by self-reported health
In comparing the differences in SRH across the various socioeconomic demographic and health related factors, the proportion of respondents reporting good health in all categories were more than those reporting poor health. This is represented in Table 2. Age was statistically related to SRH and the highest proportion (83%) of respondents reporting good health were the young old while the oldest old reported poor health more (36%). In other words, reporting good health declined from 83 to 64% as age increased while poor health increased with age, from 17 to 36%. Most males (84%) were seen to report good health compared to 71% of females. On the other hand, 26% of females reported poor health while only 18% of males reported poor health.
A high proportion of elderly persons (82%) who were married reported good health while poor health was reported most (26%) by the widowed. Most elderly Ghanaians with tertiary education (86%) reported good health and just a few proportion (11%) reported poor health. Respondents in the private sector reported good health the most (84%) while those who had never worked reported the highest proportion of poor health (34%). Eighty one percent of respondents with none of the listed chronic conditions reported good health and as few as 19% reported poor health. In respect to income, the highest proportion of respondents (81%) reporting good health was from the high income category and the highest reporting poor health (24%) was from the low income category. Elderly persons who performed no physical activity reported poor health more (79.2%) compared to reporting good health (22.8%). A great number of non-users of tobacco (77%) reported good health while the highest proportion of poor health (26%) was reported by current users of tobacco.
As for regions, the highest proportion of respondents (91%) reporting good health was from the Upper East region and the highest proportion (30%) reporting poor health was from the Western region. All these variables showed a statistically significant difference in SRH except the variables health insurance, locality, alcohol, subjective well-being, quality of life and functioning assessments.
Socio-demographic/health related factors and self-reported health
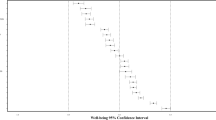
Table 3 shows results of a multivariate logit model explaining the relationship between SRH and the independent variables. From model 1, a statistically significant association can be seen between age and SRH after controlling for all life-course exposures used in this analysis. As age increases by one unit, the odds of reporting poor health against good health is 2.5 times more among the oldest old [OR = 2.5 at 95% CI (1.94–3.35)] compared to the young old. In other word, the odds of reporting poor health increases with age. At 5% level of significance, there was no statistical difference in SRH among the middle old. Respondents who had never worked in a lifetime were two times more likely to report poor health compared to those working in the informal sector [OR = 2.3 at 95% CI (1.60–2.06)]. Similarly, respondents with chronic conditions were 1.6 times [OR = 1.63 at 95% CI (1.33–2.10)] and 2 times [OR = 1.9 at 95% CI (1.41–2.52)] more likely to report poor health if they had one or more than one chronic conditions respectively. The more medical conditions an individual has, the more likely he/she is to report poor health.
Those in the highest income quintiles were 29% [OR = 0.71 at 95% CI (0.59–0.91)] less likely to report poor health compared to those in the lower income quintiles. As income increases, the chance of reporting poor health reduces. Satisfaction with life and surroundings among elderly persons reduces the chances of reporting poor health by about 26% [OR = 0.74 at 95% CI (0.59–0.93)]. Respondents who engaged in mild to moderate exercise were 1.5 times more likely to report poor health compared to their sedentary counterparts. Additionally, previous users of tobacco were 36% less likely to report poor health in contrast to reporting good health [OR = 0.64 (0.45–0.92)].
In comparing the nine regions of Ghana to the Upper West region which is one of the poorest and least developed regions in the country, the odds of reporting poor health was 2 times more among residents in the Western [OR = 2.34 at 95% CI (1.14–4.8)] and Eastern [OR = 2.21 at 95% CI (1.08–4.51)] regions. There was no statistical difference in SRH within other regions. In the same way, there was no significant association between SRH and the following categories; marital status, sex, education, health insurance, quality of life and locality.
In Model 2, elderly persons with functional limitations and disabilities had the odds of 3.6 [OR = 3.57 at 95% CI (2.88–4.41)] and 2.6 [OR = 2.61 at 95% CI (2.13–3.27)] respectively, of reporting very poor health compared to reporting good health. Similarly, current alcohol drinkers were 41% less likely to report very poor health [OR = 0.59 at 95% CI (0.49–0.72)].
Discussion
The study has analysed factors that influence the elderly self-reporting poor health compared to reporting good health. Age, prior employment, existing chronic conditions, income status, subjective well-being, physical activity, former use of tobacco, functional limitation and disability, current alcohol use and regional residence in Eastern and Western regions of Ghana have been shown to be significantly associated with SRH.
Age is seen here as a significant positive predictor of SRH. Respondents in the old-old category (80 and above) were more likely to report poor health compared to reporting good health. This result is consistent with other studies that have found age to be associated with poor health [47, 48]. The biological process of ageing could possibly explain this correlation; though old people tend to experience decline in mobility and other physical and health conditions, requiring support to undertake usual activities, the situation tends to be worse for older people within the elderly category. Besides, the social (including health) infrastructure in Ghana tends not to be supportive of everyday life and care for older persons – for instance, there are few or no specialist gerontologists in most African countries including the Ghanaian health systems [49]. Thus, this study’s result is expected. A similar study in Thailand found old age to be positively associated with poor health [50] due to decline in mobility and activities. In Japan, Liang et al. found poor health to be highest among those aged 60–85 [51]. According to some authors, increasing stressors and poor conditions increase the chances of disability, frailty and death, thereby outlining the importance of good wellbeing earlier on in life [52]. The cultural setting in Ghana (i.e. the extended family system) provides some form of guaranteed support by their children and grandchildren [53]. However, the current day modernisation and urbanisation of the Ghanaian society has led to economic hardship with more focus on the nuclear family and a collapse of the traditional family support system to elderly persons [54]. This means that reporting poor health could be due to lack of emotional and financial support from loved ones, often feeling that they have become a burden to society.
Previous studies have shown that elderly persons with chronic conditions report poor health compared to those without these conditions [29, 55]. This study showed similar findings. One possible explanation for this is that over 89% of Ghanaians including elderly persons lack in-depth knowledge of diseases and disease preventive practices [56]. Even the National Health Insurance Scheme (NHIS) instituted in 2004 to increase access to healthcare service failed to cover a significant proportion of elderly persons. This invariable implies less access to healthcare services for the elderly, late detection of diseases, rising incidence of chronic diseases and consequent poor health outcome. Equally, the rising incidence of non-communicable diseases (NCDs) can be partly attributed to the increasing ageing population and poor lifestyle [57,58,59]. High incidence of NCDs indicates increase healthcare needs for the elderly with associated cost implications in the future [60]. Society’s inability to meet these needs likely impacts the quality of life of older populations.
Income was shown to have a negative effect on SRH; Respondents of the highest income quintiles were less likely to report poor health compared to those in the middle and low income quintiles. In other words, low income earners were more likely to report poor health. With higher demand for health care, a population’s affordability of health care services remains crucial in lessening the burden of diseases. This finding is consistent with Tajvar et al. who found that most elderly Iranians who were poor and lived under poor conditions with little or no earnings, perceived their health to be poor [61]. It is known from literature that people in the high income groups can easily afford healthcare and as such, take care of their healthcare needs better and live longer [62]. By implication, high income increase the ability to purchase healthcare services. Also, some scholars found that high income exposes individuals to a good living environment which positively impacts on health [63]. Others hold that low income leads to a feeling of incompleteness, inferiority complex and psychosocial stress [64, 65], which in themselves influence self-reported health status. Some authors carried out a similar study in Ghana with related findings [35]. In the contrary, some authors found no association between income and individual health status, most likely due to the use of an objective measurement of health state [66].
In line with previous studies [67, 68] we found prior unemployment to be related to low health perception. In this analysis, the absence of work invariably increases the chances of reporting poor health in comparison to working in the informal sector were over 70% of Ghanaians obtain their livelihood from. The resultant effect of lifetime joblessness is financial insecurity, otherwise seen as potential risk to poor health. It is important to note here that according to the 2010 population and housing census report, most elderly Ghanaians who were self-employed engaged essentially in agricultural activities (63%), service or sales workers (13.1%) and just a few proportion were professionals (2.7%). Though informal sector workers in Ghana seemed better off when compared to those who have never worked in a life time, low income earnings and lack of social security remains a problem at old age.
In relation to subjective well-being, satisfaction with certain aspects of life was used to assess individual health state. The results showed that persons with high feeling of satisfaction were less likely to report poor health. Supportive findings in Brazil revealed similar association [69, 70]. Elderly people’s satisfaction in Ghana often relates to having children, living with family members and involvement with community affairs [71].
Exercise improves individual fitness, health and general wellbeing. Most studies have found a significant relationship between physical inactivity and poor health [28, 72]. Our study showed the contrary. Respondents who were engage in mild to moderate exercise for 10 min a day were more likely to report poor health. This is rather surprising. Some researchers however argue that few people may actually meet the minimum levels of physical activities which can lead to any health benefit [73, 74]. Others hold that increase stress levels may render physical activities less beneficial [75, 76]. For example, individuals may feel bad being criticized for weight gain or one’s inability to keep up with exercise pace may stir up a feeling of embarrassment and subsequent less pleasure for such activity. These unpleasant life events may alter an individual’s pace of physical activity, cause program attrition and subsequent poor health.
Respondents who previously used tobacco were less likely to report poor health. A plausible explanation could be that early cessation of tobacco reverses harmful effects in the body, improves individual health state and thus lead to a better health outcome [77, 78]. This is contrary to Nakamura et al. [79] who carried out a study on SRH among former smokers in Japan and found poor SRH to be associated with former smokers. According to the authors, bad health may be one of the reasons for quitting smoking in the first place. Such individuals in that case are more likely to report poor health. Contrastingly, in Ghana, the prevalence of tobacco use is low compared to other African countries [80]. The low prevalence could be attributed to the advertising ban on tobacco use in 1982 by the government of Ghana. This ban was later reinforced through the public health act 851 in 2012 were public smoking was completely prohibited [81]. Ever since, it has become increasingly difficult for Ghanaians to smoke in the open consequently increasing the tendency to quit smoking early, thereby reducing the danger of falling into poor health later on in life. In respect to alcohol consumption, the results reveal further that current alcohol consumers are less likely to report poor health contrary to other studies [82, 83]. A major limitation of this finding could be the inability to classify alcohol consumption in terms of content and quantity consumed by respondents. Related studies however, find moderate alcohol beverages to be associated with certain health benefits such as reduction in heart disease [84] and stroke [85].
Regional variations in reporting poor health have been shown to exist from previous studies [86, 87]. Mediating factors may include environments with poor access to health care, low political engagements, lack of transport services and low income generating activities [88]. It is therefore necessary to assess regions with poor health status and determine which areas are a country’s priority to government interventions and better policies. Contrary to the notion of poor health being less in the more affluent cities and regions, we found that elderly persons living in the Western (one of the richest region in the country) and Eastern regions of Ghana, were more likely to report poor health compared to the poorest Upper West region. The Western and Eastern regions second to the Ashanti region contain the highest proportion of elderly persons. These two regions are most suitable for agricultural activities and attract migrants particularly elderly persons engaged in agricultural activities [53]. Internal migrations in Ghana may resort to the elderly living in slums, under poor social and economic conditions and consequent poor health.
Functional limitations and disabilities are risk factors to poor quality of life. Some authors suggest that this relationship is worst in persons with moderate to severe cognitive impairment or with dementia [89,90,91]. In addition to the wealth of evidence that exists [92,93,94], our study found a significant relationship between reporting poor health and functional limitation and disability irrespective of cognitive ability. This is in concordance with Depuur et al. who found functional limitation to be associated with poor health among elderly Ghanaians [35]. Most elderly persons in Ghana live in rural areas, in the context of inadequate access to health and other social services, all factors that enhance individuals reporting poor health. Nevertheless, some authors have found this relationship between functional limitation and poor health to be insignificant among blacks though not among whites [95]. The insignificant findings could be related to information bias in which case elderly persons under report their limitations given the sensitivity of the question. We also did not find any significant association between SRH and marital status, health insurance, education, locality and quality of life owing to the confounding effects of other variables.
Study limitations
A causal relationship cannot be ascertained between the social factors and self-reported health because the study was cross-sectional. However, it is recommended that future research be carried out in form of a cohort study to establish a cause and effect relationship. Further, although previous studies have often used SRH to compare major differences across males and females, rich and poor, or demographic and socioeconomic variables, it has its own drawbacks. Heterogeneity is one of the challenges often faced as individuals may have differences in understanding the question often asked. This commonly causes under reporting or over reporting of health states [96]. Again, SRH may limit people’s experiences and thinking, with women often seen as being sentimental in reporting their health state. However, studies on SRH have been carried out in 70 different countries with good results [97]. Lastly, the use of income as a measure of socioeconomic status was a drawback in the sense that in developing countries, income is often self-reported, and as such respondents may be biased in reporting monthly income in hope of receiving financial aid [98].
Policy implications
The health status of the elderly is of growing public health concern owing to the social and economic implication of their increasing demographic profile. This study shows that the wealthier enjoy better health compared to the poor. It is therefore important that the health and income security of elderly persons should be of priority to Ghanaian authorities. Government is encouraged to improve economic and social integration through its policies and decisions. For example, employing more youths into the public sector will improve living standards and chances of social security in old age.
The Ghanaian government and its development partners should continue to reinforce policies that will encourage citizens to quit smoking and avoid other risky behaviours. Cessation of smoking can reverse harmful effects in the body and improve health benefits. Measures should be appropriated to reduce the onset of non-communicable diseases through health promotion activities and disease prevention program. Particular interest should be given to the Eastern and Western regions that have one of the highest proportion of elderly persons engaging in agricultural activities. Their welfare and health needs should be prioritized in these industrialised cities to avoid health inequity. Generally speaking, improving elderly health will reduce government expenditure on elderly health needs in future.
Age is already a risk factor for poor health as well as poor performance in basic physical activities. Bearing in mind these risk factors, government is recommended to reinforce its effort to provide a sustainable long term care plan for the elderly and ensure that the existing policies on ageing in Ghana, adopted from the Madrid International Plan of Action on Ageing (MIPAA) be revised and implemented to suit the country’s context. Existing social protection programs such as Livelihood Empowerment against Poverty (LEAP) and National Health Insurance Scheme have helped reduced economic burden and improved health and other aspects, improving living standards. What is needed is sustainability and expansion of such programs to improve the overall well-being of the elderly.
Conclusion
This study used secondary data from WHO SAGE study in Ghana and used a binary and ordinal logit model to analyse the correlation between SRH and socioeconomic and demographic factors. Self-reported health was found to be significantly related to increasing age, presence of one or more than one chronic condition, physical limitations and disabilities, being a resident of the Eastern and Western regions of Ghana. Also, the results revealed that elderly persons who belonged to the high income quintile, current alcohol drinkers, formerly used tobacco and satisfied with life, were less likely to report poor health. Contrary to other studies, we found mild to moderate physical activity to be positively associated to SRH.
Self-reported health has proven to be a valid indicator in assessing factors that affect elderly health. These factors will increasingly be an issue of concern in Ghana and most developing countries. Managing an aging society in this setting will prove challenging particularly where few health interventions on the elderly exist and geriatric medicine is still an untapped area. It is hoped that this study will pave the way for future studies to explore further, the inexhaustible factors that impede elderly health in Ghana using different research methods. Findings will be used to enlighten policy makers, governing bodies, health professionals and justify the compulsion to implement policies that will help plan for an ageing society. Societal growth is realized when social, economic and health conditions of individuals are improved.
Abbreviations
- ADL:
-
Activities of Daily Living
- IADL:
-
Instrumental Activities of Daily Living
- MIPAA:
-
Madrid International Plan of Action on Ageing
- NCDs:
-
Non-Communicable Diseases
- SAGE:
-
Study of Ageing and Adult Health
- SRH:
-
Self-Reported Health
References
Mora PA, DiBonaventura MD, Idler E, Leventhal EA, Leventhal H. Psychological factors influencing self-assessments of health: toward an understanding of the mechanisms underlying how people rate their own health. Ann Behav Med. 2008;36(3):292–303. doi:10.1007/s12160-008-9065-4.
Ichoku HE, Fonta W, Thiede M. Socioeconomic gradients in self-rated health: a developing country case study of Enugu state, Nigeria. Econ Change Restructuring. 2011;44(3):179–202. doi:10.1007/s10644-010-9098-0.
Onadja Y, Bignami S, Rossier C, Zunzunegui MV. The components of self-rated health among adults in Ouagadougou, Burkina Faso. Popul Health Metr. 2013;11(1):1. doi:10.1186/1478-7954-11-15.
Guimarães JM, Chor D, Werneck GL, Carvalho MS, Coeli CM, Lopes CS, et al. Association between self-rated health and mortality: 10 years follow-up to the Pró-Saúde cohort study. BMC Public Health. 2012;12(1):676.
French DJ, Browning C, Kendig H, Luszcz MA, Saito Y, Sargent-Cox K, et al. A simple measure with complex determinants: investigation of the correlates of self-rated health in older men and women from three continents. BMC Public Health. 2012;12:649.
Wang BR, Yu S, Noh JW, Kwon YD. Factors associated with self-rated health among north Korean defectors residing in South Korea. BMC Public Health. 2014;14:999. doi:10.1186/1471-2458-14-999.
Krokstad S, Kunst AE, Westin S. Trends in health inequalities by educational level in a Norwegian total population study. J Epidemiol Community Health. 2002;56(5):375–80.
Mackenbach JP, Stirbu I, Roskam AJ, Schaap MM, Menvielle G, Leinsalu M, et al. Socioeconomic inequalities in health in 22 European countries. N Engl J Med. 2008;358(23):2468–81.
Landrine H, Corral I, Hall MB, Bess JJ, Efird J. Self-rated health, objective health, and racial discrimination among African-Americans: explaining inconsistent findings and testing health pessimism. J Health Psychol. 2016;21(11):2514–24.
Lindstrom M. Marital status, social capital, material conditions and self-rated health: a population-based study. Health Policy. 2009;93(2–3):172–9.
Theme Filha MM, Souza Junior PR, Damacena GN, Szwarcwald CL. Prevalence of chronic non-communicable diseases and association with self-rated health: National Health Survey, 2013. Rev Bras J Epidemiol. 2015;18(2):83–96. doi:10.1590/1980-5497201500060008.
Centers for Disease Control and Prevention. Smoking-Attributable Mortality, Morbidity, and economic Costs (SAMMEC): Adult SAMMEC and Maternal and Child Health (MCH) SAMMEC software, 2004. Available from: https://apps.nccd.cdc.gov/sammec/login.asp. Accessed 22 Jan 2017.
U.S. Department of Health and Human Services. A report of the Surgeon General. The health consequences of smoking: What It Means to You. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2004. Accessed 12 Jan 2017.
Rosenkranz RR, Duncan MJ, Kolt GS, Rosenkranz SK. Active lifestyles related to excellent self-rated health and quality of life: cross sectional findings from 194,545 participants in the 45 and up study. BMC Public Health. 2013;13(1):1–24.
Tsai J, Ford ES, Li C, Zhao G, Balluz LS. Physical activity and optimal self-rated health of adults with and without diabetes. BMC Public Health. 2010;10(1):365.
Cesari M, Onder G, Zamboni V, Cesari M, Onder G, Zamboni V, et al. Physical function and self-rated health status as predictors of mortality: results from longitudinal analysis in the ilSIRENTE study. BMC Geriatr. 2008;8:34.
Feng Q, Zhu H, Zhen Z, Gu D. Self-rated health, interviewer-rated health, and their predictive powers on mortality in old age. J Gerontol B Psychol Sci Soc Sci. 2016;71(3):538–50. doi:10.1093/geronb/gbu186.
Haseen F, Adhikari R, Soonthorndhada K. Self-assessed health among Thai elderly. BMC Geriatr. 2010;10(1):30.
Herman DR, Solomons NW, Mendoza I, Qureshi AK. Self-rated health and its relationship to functional status and well-being in a group of elderly Guatemalan subjects. Asia Pac J Clin Nutri. 2001;10(3):176–82.
Tomioka K, Kurumatani N, Hosoi H. Self-rated health predicts decline in instrumental activities of daily living among high-functioning community-dwelling older people. Age Ageing. 2016:1–6. doi:10.1093/ageing/afw164.
Perneczky R, Pohl C, Sorg C, Hartmann J, Tosic N, Grimmer T, et al. Impairment of activities of daily living requiring memory or complex reasoning as part of the MCI syndrome. Int J Geriatr Psychiatry. 2006;21:158–62.
Cahn-Weiner DA, Farias ST, Julian L, Harvey DJ, Kramer JH, Reed BR, et al. Cognitive and neuroimaging predictors of instrumental activities of daily living. J Int Neuropsychol Soc. 2007;13(05):747–57.
McMullen CK, Luborsky MR. Self-rated health appraisal as cultural and identity process: African American elders’ health and evaluative rationales. The Gerontologist. 2006;46(4):431–8.
Yasamy MT, Dua T, Harper M, Saxena S. Mental health of older adults, addressing a growing concern. World Health Organization, Department of Mental Health and Substance Abuse 2013; 10:4-9.
Population & Housing Census Report. The elderly in Ghana. Accra, Ghana: Ghana Statistical Service. 2010;1–100.
United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing. 2013. ST/ESA/SER.A/348.
Minicuci N, Biritwum RB, Mensah G, Yawson AE, Naidoo N, Chatterji S, et al. Sociodemographic and socioeconomic patterns of chronic non-communicable disease among the older adult population in Ghana. Glob Health Action. 2014;7 doi:10.3402/gha.v7.21292.
Chan YY, Teh CH, Lim KK, Lim KH, Yeo PS, Kee CC, et al. Lifestyle, chronic diseases and self-rated health among Malaysian adults: results from the 2011 National Health and morbidity survey (NHMS). BMC Public Health. 2015;15(1):754.
Mavaddat N, Valderas J, van der Linde R, Kay Tee K, Kinmonth A. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: a cross-sectional study. BMC Fam Pract. 2014;15(1):185–95.
Kwankye SO. Growing old in Ghana: health and economic implications. Postgraduate Med J Ghana. 2013;2(2):88–97.
Saeed BI, Xicang Z, Yawson AE, Nguah SB, Nsowah-Nuamah NN. Impact of socioeconomic status and medical conditions on health and healthcare utilization among aging Ghanaians. BMC Public Health. 2015;15(1):276.
Wrigley-Asante C. Men are poor but women are poorer: gendered poverty and survival strategies in the Dangme West District of Ghana. Norsk Geografisk Tidsskrift-Norwegian J Geography. 2008;62(3):161–70.
Bora JK, Saikia N. Gender differentials in self-rated health and self-reported disability among adults in India. PLoS One. 2015;10(11):e0141953.
Josefsson K, Andersson M, Erikstedt A. Older adults’ self-rated health and differences by age and gender: a quantitative study. Healthy Aging Res 2016;5(1):1-0.
Debpuur C, Welaga P, Wak G, Hodgson A. Self-reported health and functional limitations among older people in the Kassena-Nankana District, Ghana. Glob Health Action. 2010;3(Suppl 2):54Á63.
Kowal P, Chatterji S, Naidoo N, Biritwum R, Fan W, Ridaura RL, et al. Data resource profile: the World Health Organization study on global ageing and adult health (SAGE). Int J Epidemiol. 2012;41(6):1639–49.
Nirmala Naidoo. Ghana duration of interview. SAGE 2007–2010. Available from http://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/6/download/1881. Accessed 24 Nov 2016.
Bourne PA. Dichotomising poor self-reported health status: using secondary cross-sectional survey data for Jamaica. N Am J Med Sci. 2008;1(6):295–302. doi:10.4297/najms.2009.6295.
Lim WY, Ma S, Heng D, Bhalla V, Chew SK. Gender, ethnicity, health behavior & self-rated health in Singapore. BMC Public Health. 2007;7(1):1–7. doi:10.1186/1471-2458-7-184.
Subramanian SV, Huijts T, Avendano M. Self-reported health assessments in the 2002 world health survey: how do they correlate with education? Bull World Health Organ. 2010;88(2):131–8.
Arnadottir SA, Gunnarsdottir ED, Stenlund H, Lundin-Olsson L. Determinants of self-rated health in old age: a population-based, cross-sectional study using the international classification of functioning. BMC Public Health. 2011;11(1):670.
Wu S, Wang R, Zhao Y, Ma X, Wu M, Yan X, et al. The relationship between self-rated health and objective health status: a population-based study. BMC Public Health. 2013;13(1):320.
Dhamo E, Koҫollari N. Older people quality of life evaluation. Mediterranean J Soc Sci. 2014;5(13):385.
Rockwood K, Mitnitski A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin Geriatr Med. 2011;27(1):17–26. doi:10.1016/j.cger.2010.08.008.
World Health Organization. Measuring health and disability: a manual for the World Health Organization disability assessment schedule (WHODAS 2.0). Geneva: World Health Organization; 2009.
Blay SL, Ramos LR, Mari JJ. Validity of a Brazilian version of the olders Americans resources and services (OARS) mental health Screenig questionnaire. J Am Geriatr Soc. 1988;36(8):687–92.
Kumar P, Kumar A. Socio-economic status and self-rated health status of the elderly in rural Uttar Pradesh. Indian J Prev Soc Med. 2012;43(3):256.
Movahed M, Jahanbazian S, Abbasi Shavazi MT. The study of self-assessed health among elderly women in shiraz and Yasuj cities. Elderly Health Journal. 2016;2(1):27–32.
Gachuhi JM, Kiemo K. Research capacity on ageing in Africa: limitations and ways forward. Generations Review. 2005;15(2):36–8.
Haseen F, Adhikari R, Soonthorndhada K. Self-assessed health among Thai elderly. BMC Geriatr. 2010;10(1):30. doi:10.1186/1471-2318-10-30.
Liang J, Shaw BA, Krause N, et al. How does self-assessed health change with age? A study of older adults in Japan. J Gerontol B: Psychol Sci Soc Sci. 2005;60(4):S224–32.
Mitnitski A, Rockwood K. The rate of aging: the rate of deficit accumulation does not change over the adult life span. Biogerontology. 2016;17(1):199–204.
Aboderin I. Decline in material family support for older people in urban Ghana, Africa: understanding processes and causes of change. J Gerontol Ser B Psychol Sci Soc Sci. 2004;59(3):128–S37.
Mba CJ. Population ageing in Ghana: research gaps and the way forward. J Aging Res. 2010:67–2157. doi:10.4061/2010/672157.
Alves LC, Rodrigues RN. Determinants of self-rated health among elderly persons in Sao Paulo, Brazil. Rev Panam Salud Publica. 2005;17(5–6):333–41.
Yiranbon É, Lulin Z, Antwi AH, Marfo EO, Amoako KO, Offin DK. Exploring the expectation and perception of healthcare needs of the elderly in Ghana: an empirical analysis. Int J Acad Res Econ Manag Sci. 2014;1(3):165.
Ward BW, Schiller JS. Prevalence of multiple chronic conditions among US adults: estimates from the National Health Interview Survey, 2010. Prev Chronic Dis. 2013;10:E65.
St Sauver JL, Boyd CM, Grossardt BR, Bobo WV, Rutten LJ, Roger VL, et al. Risk of developing multi-morbidity across all ages in an historical cohort study: differences by sex and ethnicity. BMJ Open. 2015;5(2):e006413.
Thorpe KE, Allen L, Joski P. The role of chronic disease, obesity, and improved treatment and detection in accounting for the rise in healthcare spending between 1987 and 2011. Appl Health Econ Health Policy. 2015;13(4):381–7.
Vogeli C, Shields AE, Lee TA, Gibson TB, Marder WD, Weiss KB, et al. Multiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costs. J Gen Intern Med. 2007;22(3):391–5. doi:10.1007/s11606-007-0322-1.
Tajvar M, Arab M, Montazeri A. Determinants of health-related quality of life in elderly in Tehran, Iran. BMC Public Health. 2008;8:323. doi:10.1186/1471-2458-8-323.
Demakakos P, Nazroo J, Breeze E, Marmot M. Socioeconomic status and health: the role of subjective social status. Soc Sci Med. 2008;67(2):330–40. http://dx.doi.org/10.1016/j.socscimed.2008.03.038
Wen M, Hawkley LC, Cacioppo JT. Objective and perceived neighborhood environment, individual SES and psychosocial factors, and self-rated health: an analysis of older adults in Cook County, Illinois. Soc Sci Med. 2006;63(10):2575–90.
Wagstaff A, Van Doorslaer E. Income inequality and health: what does the literature tell us? Annu Rev Public Health. 2000;21(1):543–67.
Miething A. A matter of perception: exploring the role of income satisfaction in the income–mortality relationship in German survey data 1995–2010. Soc Sci Med. 2013;99:72–9.
Fink G, Weeks JR, Hill AG. Income and health in Accra, Ghana: results from a time use and health study. Am J Trop Med Hyg. 2012;87(4):608–15. doi:10.4269/ajtmh.2012.12-0062.
Kwon K, Park JB, Lee K-J, Cho Y-S. Association between employment status and self-rated health: Korean working conditions survey. Ann Occup Environ Med. 2016;28(1):43.
Kaleta D, Makowiec-Dabrowska T, Jegier A. Employment status and self rated health. Int J Occup Med Environ Health. 2008;21(3):227–36.
Borim FS, Neri AL, Francisco PM, Barros MB. Dimensions of self-rated health in older adults. Revista de Saude Publica. 2014;48(5):714–22.
Sposito G, Diogo MJ, Cintra FA, Neri AL, Guariento ME, De Sousa ML. Relationship between subjective well-being and the functionality of elderly outpatients. Braz J Physical Ther. 2010;14(1):81–9.
Apt NA. Care of the elderly in Ghana: an emerging issue. J Cross-Cultural Gerontol. 1993;8(4):301–12. doi:10.1007/BF00972559.
Molarius A, Berglund K, Eriksson C. Socioeconomic conditions, lifestyle factors, and self-rated health among men and women in Sweden. Eur J Pub Health. 2007;17(2):125–33. doi:10.1093/eurpub/ckl070.
Oman RF, King AC. The effect of life events and exercise program format on the adoption and maintenance of exercise behavior. Health Psychol. 2000;19(6):605.
Stults-Kolehmainen MA, Sinha R. The effects of stress on physical activity and exercise. Sports Med. 2014;44(1):81–121.
Lutz RS, Stults-Kolehmainen MA, Bartholomew JB. Exercise caution when stressed: stages of change and the stress–exercise participation relationship. Psychol Sport Exerc. 2010;11(6):560–7.
American Psychological Association. Stress in America: our health at risk. Washington DC: American Psychological Association; 2012.
Shin HR, Lee DH, Herrero R, Smith JS, Vaccarella S, Hong SH, et al. Attributable fraction of tobacco smoking on cancer using population-based nationwide cancer incidence and mortality data in Korea. BMC Cancer. 2014;14:406.
McClave AK, Dube SR, Strine TW, Mokdad AH. Associations between health-related quality of life and smoking status among a large sample of U.S. adults. Prev Med. 2009;48(2):173–9. doi:10.1016/j.ypmed.2008.11.012.
Nakamura K, Sakurai M, Nishijo M, Morikawa Y, Nakagawa H. Characteristics of smoking cessation in former smokers in a rural area in Japan. Int J Prev Med. 2012;3:459–65.
Owusu-Dabo E, Lewis S, McNeill A, Anderson S, Gilmore A, Britton J. Smoking in Ghana: a review of tobacco industry activity. BMJ. 2009;18(3):206–11.
Yawson AE, Baddoo A, Hagan-Seneadza NA. Tobacco use in older adults in Ghana: sociodemographic characteristics, health risks and subjective wellbeing. BMC Public Health. 2013;13:979. doi:10.1186/1471-2458-13-979.
Doll R, Peto R, Hall E, Wheatley K, Gray R. Mortality in relation to consumption of alcohol: 13 years’ observations on male British doctors. BMJ. 1994;309:911–8.
Tsai J, Ford ES, Li C, Pearson WS, Zhao G. Binge drinking and suboptimal self-rated health among adult drinkers. Alcohol Clin Exp Res. 2010;34(8):1465–71.
Hines LM, Rimm EB. Moderate alcohol consumption and coronary heart disease: a review. Postgrad Health J. 2001;77:747–52. doi:10.1136/pmj.77.914.747.
Sacco RL, Elkind M, Boden-Albala B, Lin IF, Kargman DE, Hauser WA, et al. The protective effect of moderate alcohol consumption on ischemic stroke. J Am Med Assoc. 1999;281:53–60. doi:10.1001/jama.281.1.53.
Sözmen K, Baydur H, Simsek H, Ünal B. Decomposing socioeconomic inequalities in self assessed health in Turkey. Int J Equity Health. 2012;11(1):1.
Ergin I, Kunst AE. Regional inequalities in self-rated health and disability in younger and older generations in Turkey: the contribution of wealth and education. BMC Public Health. 2015;15(1):1. doi:10.1186/s12889-015-2273-5.
Cummins S, Stafford M, Macintyre S, Marmot M, Ellaway A. Neighborhood environment and its association with self-rated health: evidence from Scotland and England. J Epidemiol Community Health. 2005;59(3):207–13.
Jefferson AL, Byerly LK, Vanderhill S, Lambe S, Wong S, Ozonoff A, et al. Characterization of activities of daily living in individuals with mild cognitive impairment. Am J Geriatr Psychiatry. 2008;16(5):375–83.
Helvik AS, Engedal K, Benth JŠ, Selbæk G. A 52 month follow-up of functional decline in nursing home residents-degree of dementia contributes. BMC Geriatr. 2014;14:45. doi:10.1186/1471-2318-14-45.
Mathiowetz NA, Lair TJ. Getting better? Change or error in the measurement of functional limitations. J Econ Soc Meas. 1994;20(3):237–62.
Arokiasamy P, Uttamacharya, Jain K. Multi-morbidity, functional limitations, and self-rated health among older adults in India. SAGE Open. 2015;5(1): 2158244015571640.
Zunzunegui MV, Nunez O, Durban M, de Yébenes M-JG, Otero Á. Decreasing prevalence of disability in activities of daily living, functional limitations and poor self-rated health: a 6-year follow-up study in Spain. Aging Clin Exp Res. 2006;18(5):352–8.
Mullen SP, McAuley E, Satariano WA, Kealey M, Prohaska TR. Physical activity and functional limitations in older adults: the influence of self-efficacy and functional performance. J Gerontol Ser B Psychol Sci Soc Sci. 2012;67B(3):354–61.
Boyington JE, Howard DL, Holmes DN. Self-rated health, activities of daily living, and mobility limitations among black and white stroke survivors. J Aging Health. 2008;20(8):920–39.
Pfarr C, Schmid A, Schneider U. Reporting heterogeneity in self-assessed health among elderly Europeans. Heal Econ Rev. 2012;2(1):21.
Chuc NT, Debpuur C, Egondi T, Gomez-Olive FX, Hakimi M, Hirve S, et al. Health inequalities among older men and women in Africa and Asia: evidence from eight health and demographic surveillance system sites in the INDEPTH WHO-SAGE study. Glob Health Action. 2010;96 doi:10.3402/gha.v3i0.5420.
Doocy S. BurnhamG. Assessment of socio-economic status in the context of food insecurity: implications for field research. World Health Popul. 2006;8(3):32–42.
Acknowledgements
The authors would like to acknowledge the World Health Organization for making the data openly available online. The authors would like to thank the editor in chief and the two reviewers for very helpful comments, suggestions and technical inputs that helped greatly to improve the quality of our paper.
Funding
No source of funding was used in the study.
Availability of data and materials
Data used for this study is available through WHO’s SAGE website.
(www.who.int/healthinfo/systems/sage) and WHO’s archive using the National Data Archive application (http://apps.who.int/healthinfo/systems/surveydata).
Author information
Authors and Affiliations
Contributions
CLF contributed in planning the study, carried out the statistical analysis and drafted the manuscript. GCA and JN conceived, planned and reviewed the study. AM planned, reviewed and made inputs. EN reviewed the manuscript and made inputs. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This is a secondary analysis of openly available data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Fonta, C.L., Nonvignon, J., Aikins, M. et al. Predictors of self-reported health among the elderly in Ghana: a cross sectional study. BMC Geriatr 17, 171 (2017). https://doi.org/10.1186/s12877-017-0560-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-017-0560-y