
Abstract
Background
Frailty, neurodegeneration and geriatric syndromes cause a significant impact at the clinical, social, and economic level, mainly in the context of the aging world. Recently, Information and Communication Technologies (ICTs), virtual reality tools, and machine learning models have been increasingly applied to the care of older patients to improve diagnosis, prognosis, and interventions. However, so far, the methodological limitations of studies in this field have prevented to generalize data to real-word. This review systematically overviews the research designs used by studies applying technologies for the assessment and treatment of aging-related syndromes in older people.
Methods
Following the PRISMA guidelines, records from PubMed, EMBASE, and Web of Science were systematically screened to select original articles in which interventional or observational designs were used to study technologies’ applications in samples of frail, comorbid, or multimorbid patients.
Results
Thirty-four articles met the inclusion criteria. Most of the studies used diagnostic accuracy designs to test assessment procedures or retrospective cohort designs to build predictive models. A minority were randomized or non-randomized interventional studies. Quality evaluation revealed a high risk of bias for observational studies, while a low risk of bias for interventional studies.
Conclusions
The majority of the reviewed articles use an observational design mainly to study diagnostic procedures and suffer from a high risk of bias. The scarce presence of methodologically robust interventional studies may suggest that the field is in its infancy. Methodological considerations will be presented on how to standardize procedures and research quality in this field.
Similar content being viewed by others


Introduction
Worldwide, life expectancy is rapidly increasing and according to the previsions, the proportion of people older than 60 years will reach 21.1% by 2050 compared to the 9.2% in 1990 and the 11.7% in 2013 (World Health Organization; https://www.who.int/news-room/fact-sheets/detail/ageing-and-health). Despite the improvement of instruments and standards of care, late life is not empty of complex chronic medical conditions that represent major problems in particular for health care systems still focusing on a disease-oriented approach [1].
Accordingly, the transition towards an aging world is boosting a gradual passage to more person-focused care models [2]. Within these models, frailty, comorbidity, and multimorbidity have recently caught the attention of scholars and clinicians, with a significant increase of publications [3], even about the application of technological tools for diagnosis and intervention of these conditions. However, recent literature reviews underlined limitations linked to methodological procedures of research conducted in this field, reducing studies’ validity and results’ generalizability [4, 5]. Indeed, most of the studies testing technology feasibility use observational designs with assessment purposes in limited and heterogeneous samples of frail, comorbid, or multimorbid older patients, while interventional studies involving groups of patients defined by clear inclusion and exclusion criteria are under-represented. These methodological difficulties may be also linked to the interchangeable modality by which frailty, comorbidity, and multimorbidity are often defined, with a lack of consensus regarding their operational translation in practice [6]. Although frequently used as synonyms, these conditions are separate clinical concepts [7] that can independently coexist or mutually interact constituting pre-disability conditions [8].
There is an agreement depicting frailty as a dynamic and multicomponential condition depending on or leading to an extreme vulnerability to stressors and reduced resiliency [9, 10]. Despite this consensus, frailty has been alternatively defined as the result of the accumulation of deficits [11] or as a clinical syndrome (i.e., Frailty Phenotype) [7], with both these definitions failing to include symptoms belonging to psychosocial and cognitive domains, that are instead captured by the more recent concept of intrinsic capacity [12, 13].
The controversy about definitions of multimorbidity and comorbidity depends on the nature, time of onset, and assessment of the diagnosed clinical diseases [14] that co-occur, not interdependently, in the case of multimorbidity or that generate combined effects in reference to an index chronic disease in the case of comorbidity [15].
The prevalence of frailty, comorbidity and multimorbidity increases with aging [16], leading to reduce life expectancy, impairments in daily living activities and postoperative complications, increased risk of mortality, and costs for public health, in terms of frequency and duration of emergency room visits and hospital admissions [17,18,19,20]. Therefore, care pathways aiming at personalizing interventions based on the needs of older patients, namely patient-centered health systems, may be crucial to cover the urgency to manage the impactful long-term consequences of these conditions [17]. Going further, these novel care approaches could benefit from the use of assistive health technology (i.e., technological solutions aiming to maintain or improve functionality, autonomy, and well-being) or medical devices (i.e., technological solutions aiming to support prevention, diagnosis, and treatment) to prioritize integration between different settings of care and care professionals, the inclusion of caregivers in the treatment programs, development of remote self-management solutions and procedures [21,22,23].
Accordingly, in the last years, research showed that Information and Communication Technologies (ICTs), machine learning algorithms/models [24], and virtual reality tools [25, 26] may be beneficial for older people [27, 28]. In particular, technologies demonstrated to ameliorate diagnosis, prognosis, and prevention strategies [29] as well as facilitate remote monitoring [30], continuity of care [31], access to healthcare services [32] and even patients’ independence and quality of life [33].
However, studies pointed out also barriers to the use of technology in samples of frail, comorbid, and multimorbid older people, preventing cost-effectiveness analysis and solid integration of technologies within complex assistive models. Beyond technical and economic aspects [33, 34], as already mentioned, research seems to lack rigorous methodological approaches, with a clear displacement towards assessment of frailty, comorbidity, and multimorbidity compared to clinical trials testing technologies as intervention tools in samples suffering from complex geriatric syndromes. Indeed, technologies have been mostly tested in reference to their technical aspects, whereas applications in clinical settings frequently are pilot experiences on small and mixed groups of patients, not providing analysis of patients’ needs, considerations about usability and acceptability of tested devices, exploration of characteristics of the real-world application scenarios [4, 5].
Despite these limitations, to the best of our knowledge, literature still lacks a comprehensive review of research designs, in terms of observational or interventional designs, that studies using technologies for the assessment and treatment of aging-related syndromes in older people have applied so far.
This review aims to fill this gap by systematically describing research designs and procedures currently applied to transfer laboratory results to real-world practices in order to critically appraise studies’ methodological quality based on structured criteria and present considerations on how to standardize studies’ methods and research quality in this field.
Methods
Literature search
Our systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [35]. PROSPERO registration number: CRD42020218053.
The selected keywords were: “frailty”, “multimorbidity”, “comorbidity”, “aging”/“elderly” that were combined, into three arms, with ICT, machine learning, and virtual reality [33, 36,37,38,39]. See Appendix A in the Supplementary material for the details of the search strategies and combinations.
The arms were searched as major topics in Pubmed, Web of Science, and Embase (Ovid), restricting the literature search to title, abstract, and keywords.
Using a web and mobile systematic review manager [40], after duplicates removal, four blinded researchers (A.G., P.D.T., C.T., S.C.) in pairs categorized the records as “included”, “excluded”, or “unsure” based on title/abstract. Then, during the full-text screening, records included or categorized as “unsure” in the first stage were reviewed. In both screening stages conflicts were resolved by consensus of the researchers of each pair and a third author was consulted if discrepancies remained. The authors of papers whose full-text was not available were contacted.
Selection criteria
Eligible for inclusion were peer-reviewed studies published to the end of September 2020. The following hierarchy of eligibility criteria was adopted: (a) English written articles; (b) articles involving human samples; (c) peer-reviewed articles; (d) articles including frail or multimorbid or comorbid participants older than 65 years. In particular, we considered records in which frailty or multimorbidity or comorbidity were the main outcomes of the technology-based assessment or intervention, while we excluded studies where these conditions were simply assessed to describe participants but were not part of the studies’ aims; (e) articles applying technologies with clear diagnostic or intervention purposes. Therefore, we excluded records including technologies only to assess their usability or acceptability. Moreover, we included papers on telerobotics devices, while robotics used in surgical settings were excluded; (f) original peer-reviewed articles with interventional or observational study designs according to types proposed in [41], while narrative or systematic reviews, meta-analyses, case-reports, abstracts, conference proceedings and study protocols were excluded.
Data extraction and synthesis
Data from each of the included studies were collected by one of the authors in each pair by using a specific form. Data were checked for accuracy and completeness by the other pair’s member and discrepancies were solved by consensus and/or by a third author if needed (see Table 1).
Quality assessment
We chose the most appropriate quality assessment tool based on the records’ study design defined according to [41]. In particular, interventional randomized and non-randomized clinical trials were assessed using the Cochrane Collaboration’s Risk-of-Bias Tool [42]. Observational studies with diagnostic aims were assessed using the Quality Assessment of Diagnostic Accuracy Studies tool – second version (QUADAS-2) [43]. Observational studies using predictive models with prognostic purposes were assessed through the Quality In Prognosis Studies (QUIPS) tool [44]. See Supplementary materials for details of the scales used.
Six blinded researchers (A.G., P.D.T., C.T., S.C., A.GR., F.R.G.) in pairs evaluated the studies’ quality. Conflicts were solved by consensus of authors in each pair or by the involvement of a third author in case of discrepancies.
Results
Review selection
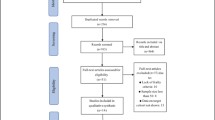
Based on our keywords we retrieved 2207 records. After removing duplicates, we screened the title and abstract of 1626 papers. According to our selection criteria and following the consensus on conflicts, 290 studies moved then to the full-text screening. Among the 290 full texts, 34 papers met our inclusion criteria and were included in the qualitative synthesis (Fig. 1).

PRISMA Flowchart of the screening process
Quality assessment
The quality and the risk of bias assessment of the retrieved studies are summarized in Figs. 2, 3 and 4. Considering the Cochrane Collaboration’s Risk-of-Bias Tool (Fig. 2), we evaluated 10 papers out of 34. Among these, six were randomized control trials [45,46,47,48,49,50], two were non-randomized control trials [51, 52], one was a pre-post design [53] and one was a cross-over randomized control trial [54]. The analysis of the risk of bias across studies revealed a high average quality with only two studies exposed to selection bias [52, 53] and two studies exposed to performance bias [45, 49].

Risk of bias evaluation with Cochrane tool

(a) Risk of bias evaluation with QUADAS-2 Risk tool. (b) (b)

Risk of bias evaluation with QUIPS tool
Based on the QUADAS-2 ratings (Fig. 3a), we assessed 15 [55,56,57,58,59,60,61,62,63,64,65,66,67,68,69] diagnostic accuracy studies, one retrospective cohort study [70], and one cross-sectional study [71]. The average quality of the included studies was intermediate to low as most of the analyzed items, in particular the tested index, the standard of reference, and timing of measurements, despite not totally at high risk of bias, were evaluated as unclear due to the lack of information in most of the retrieved papers. The item regarding the selection of patients was assessed as low risk by most of the papers, however, compared to the other items, it obtained the higher number of high risk ratings. Considering the evaluation of the applicability through QUADAS-2 (Fig. 3b), the quality of the retrieved observational studies was high.
We used the QUIPS tool to evaluate the quality of six observational studies describing a predictive model (Fig. 4). Among these, five papers were retrospective cohort studies [72,73,74,75,76] and one paper was a cross-sectional study [77]. The average quality was intermediate to low as the risk of attrition and confounding factors, as well as bias in patients’ section, were rated from moderate to high by most of the studies in this group.
Research methodology
The majority of the selected papers (24/34) reported observational studies, whereas only ten out of thirty-four studies were interventional researches (Table 1). Below we report the main results organizing the selected studies according to these two major methodological approaches.
Observational studies
Twenty-four out of thirty-four papers were observational studies and involved 923,319 patients affected by multimorbidity [70, 75, 78], 90,096 affected by frailty [55,56,57,58,59,60,61,62,63,64,65,66,67,68,69, 72,73,74, 76] and 1,765 patients affected by geriatric syndromes [71, 77]. The diagnostic accuracy study design was the most represented study typology, with fifteen out of twenty-four studies [55,56,57,58,59,60,61,62,63,64,65,66,67,68,69], and the general aim of all these studies was to assess a diagnostic methodology devoted to detect frailty. The second most represented study typology was the retrospective cohort study design, with six out of twenty-four studies. The general objective of five of these studies was to elaborate a predictive model for frailty [72,73,74, 76] or multimorbidity [75], whereas the general aim of the last one was to study the mortality rate of patients suffering from multimorbidity [70]. The typology of the remaining three papers refered to cross-sectional study design. The general aim of two of these was to study prevalence of geriatric syndromes [71, 77] and the third study aimed to elaborate a predictive model for multimorbidity [78].
The twenty-four observational studies selected implemented different ICT technologies. Among the fifteen diagnostic accuracy studies, wearable sensors were the most common ICT technologies used and were mainly proposed to analyze postural and movement variables [55, 59,60,61, 67]. Four studies proposed to exploit widely diffuse technologies (smartphone or tablet) to analyze movement parameters during sit-to-stand tasks [64,65,66] or handwriting [63]. Two studies implemented virtual reality technologies, one to propose serious games [58] and the other to implement movement analysis [57]. The remaining four studies were based on different technologies: one study implemented a social robot to administer clinical questionnaires [62], another one assessed motion and walking parameters using commercial motion capture sensors like Kinect [68], a third one implemented a home monitoring platform with ambient sensors to analyze patient daily habits [69], and the last study used machine learning to identify frailty from administrative data [56]. Among the six retrospective cohort studies selected, five exploited different machine learning methods to develop predictive models for frailty [72,73,74, 76] or multimorbidity [75], whereas one study analyzed data from a telemonitoring experience to assess mortality according to multimorbidity and telemonitoring status [70]. The remaining three cross sectional studies implemented, in two cases, machine learning algorithms to generate predictive models for multimorbidity [78] or to detect patterns of medication combinations according to geriatric syndrome status [77], and in one case a mobile iPad application was used to study the prevalence of geriatric syndromes [71].
Interventional studies
Ten out thirty-four papers were interventional studies and involved 1912 patients affected by multimorbidity [46,47,48,49, 52], 170 affected by frailty [45, 50, 51, 54] and 53 with comorbidity [53].
Seven studies were randomized controlled trials, four devoted to study interventions for multimorbidity [46,47,48,49] and three for frailty [45, 50, 54]. The remaining three studies were two non-randomized trials, one for frailty [51] and one for multimorbidity [52], and one a pre-post study design which analyzes an intervention for comorbidity [53].
The seven randomized controlled trials selected used different ICT technologies. Three studies promoted physical activity (PA) or motivation toward PA through virtual reality [50], robot [54] or a web-based motivational program [49]; two studies analysed Ambient Assisted Living (AAL) interventions [45, 48], one study used telemonitoring [47] and another one a video consultation intervention [46]. The three further non-randomized trials proposed a smart-phone based PA program [51], a telemonitoring system [53] or an integrated care intervention [52].
Discussion
The present review first aimed to systematically describe research designs implemented by studies about technologies applications to clinical assessment and treatment of aging-related syndromes. Overall, the results showed a clear imbalance toward a more represented amount of observational studies compared to interventional ones. This result reflects the well-known limits of applying only standard Randomized Clinical Trials (RCTs) in the research field of technology-based interventions for rehabilitation purposes [79]. Moreover, the quality assessment revealed that interventional studies were of higher quality, whereas observational studies were mainly of intermediate to low quality. Taken together, these findings may suggest that the field is still seminal as emerged in a previous review [4].
Our second aim was to propose a step model to standardize studies’ methods and improve the research quality in this field. This is in line with the actions of the European Network for Health Technology Assessment. This network on technology research recommends: a clear assessment of previous studies’ results; the disclosure of the rationale for using technology; the clinical indication of the population, the kind of intervention and comparators; the evidence about safety and effectiveness; the definition of study design (see https://www.eunethta.eu/methodology-guidelines/). Based on these recommendations, we hypothesize that one possible interpretation of our results could be the absence of a strong frame of reference describing all the steps useful to obtain a technology of good quality to be used for diagnostic or interventional purposes in a real-world setting. Considering the field of new drugs development, suggestions on how to formulate a canonized frame helping to overcome the emerged limitations could be found. Indeed, we propose that the development of a new technology to be used for diagnostic or interventional purposes has to pass several steps similar to those of the process to develop a new drug, as shown in Table 2.
In our model, the two phases of the “Clinical research” step represent the attempt to exploit the power of “Efficacy” studies, which are intended to assess the performance of an intervention under ideal circumstances, as well as “Effectiveness” studies, which are intended to produce evidence of therapeutic effectiveness in real-world practice settings [80, 81]. Usually “Efficacy” studies are the classical RCTs that, even though represent the gold standard for evaluating the efficacy of an intervention, require highly controlled conditions to avoid biases and confounding factors [81]. On the other hand, “Effectiveness” studies are retrospective or prospective real-world observational studies that, by using a less strict methodology and examining interventions under circumstances closer to real-world practice, lead to complementary evidence to that provided by RCTs, even if they are more prone to several sources of bias and risk of uncontrolled confounders [80].
Considering these characteristics and the concerns of limiting the research on technologies for disabilities only to RCTs [79], we think that both these types of studies should contribute to the research field of technologies applications for the diagnosis and intervention of age-related pathologies. Indeed, the results of this review, coherently with previous works [4, 5], show that studies in which technological solutions are tested in samples of frail, comorbid, and multimorbid old patients frequently describe technical aspects of technologies through laboratory experimentations, with only empirical applications on pilot samples. In other cases, they are large but methodologically poor observational studies aiming at improving the assessment or at providing predictive models. Sometimes, they are clinical trials that, despite the good quality, lack usability and acceptability considerations and are underpowered to generalize the results or to run cost-effectiveness analyses. Therefore, we first suggest that systematizing “Efficacy” and “Effectiveness” study designs in the “Clinical research” phase of our model could enhance the methodological rigor of randomized trials and observational studies, both conducted on small selected samples as well as on heterogeneous and large groups of patients. Following the methodological requirements of “Efficacy” and “Effectiveness” research designs, RCTs could indeed rightly test technologies efficacy, while observational studies could strictly explore aging-related syndromes prevalence, technologies applications’ validity, reliability, sensitivity, and their role in predicting long-term outcomes of chronic conditions. Second, considering the proposed model as a whole, we are confident that applying such a rigorous framework could help scholars to dialogue with clinicians, to effectively investigate technologies’ usability, acceptability, and safety based on clinical population characteristics and strata. This, in turn, could prepare the stage for well-designed clinical studies that could provide solid results, even regarding cost-effectiveness analysis, to be used for revision and approval by a recognized Institution and finally for post-market monitoring of long-term effects and large-scale use.
In conclusion, the results of the present systematic review seem to suggest that research in the field of the development and use of technological tools for aging-related syndromes is, at the moment, mostly oriented toward observational studies devoted to diagnostic tools to be used in the assessment of geriatric conditions (e.g. frailty). The field suffers from some limitations related to the research quality and poor attention to interventional studies of efficacy and effectiveness. We propose that a structured and shared methodological approach, like that followed in pharmaceutical studies, could help the field to increase the research quality and more adequately respond to the needs of patients and their caregivers.
Data Availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Change history
01 August 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12874-023-01996-4
References
Palmer K, Marengoni A, Forjaz MJ, Jureviciene E, Laatikainen T, Mammarella F et al. Multimorbidity care model: recommendations from the consensus meeting of the Joint Action on Chronic Diseases and promoting healthy ageing across the life cycle (JA-CHRODIS). In: Health Policy. 2018.
Tinetti ME, Fried T. The end of the disease era. Am J Med. 2004.
Cesari M, Calvani R, Marzetti E. Frailty in Older Persons. Clinics in Geriatric Medicine. 2017.
Gallucci A, Trimarchi PD, Abbate C, Tuena C, Pedroli E, Lattanzio F, et al. ICT technologies as new promising tools for the managing of frailty: a systematic review. Aging Clinical and Experimental Research; 2021.
Tuena C, Pedroli E, Trimarchi PD, Gallucci A, Chiappini M, Goulene K et al. Usability issues of clinical and research applications of virtual reality in older people: a systematic review. Front Hum Neurosci. 2020.
Cesari M, Pérez-Zepeda MU, Marzetti E. Frailty and Multimorbidity: different Ways of thinking about Geriatrics. J Am Med Dir Assoc. 2017.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J et al. Frailty in older adults: evidence for a phenotype. Journals Gerontol Ser A Biol Sci Med Sci. 2001.
Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. Journals of Gerontology - Series A Biological Sciences and Medical Sciences. 2004.
Bergman H, Ferrucci L, Guralnik J, Hogan DB, Hummel S, Karunananthan S et al. Frailty: An emerging research and clinical paradigm - Issues and controversies. Journals of Gerontology - Series A Biological Sciences and Medical Sciences. 2007.
Villacampa-Fernández P, Navarro-Pardo E, Tarín JJ, Cano A. Frailty and multimorbidity: two related yet different concepts. Maturitas. 2017.
Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005.
World Health Organization (WHO). World Health Organization World Report on Ageing and Health. World Health Organization; 2015.
Belloni G, Cesari M. Frailty and intrinsic capacity: two distinct but related constructs. Front Med. 2019.
Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009.
Yancik R, Ershler W, Satariano W, Hazzard W, Cohen HJ, Ferrucci L. Report of the National Institute on Aging Task Force on Comorbidity. Journals of Gerontology - Series A Biological Sciences and Medical Sciences. 2007.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012.
Onder G, Cesari M, Maggio M, Palmer K. Defining a care pathway for patients with multimorbidity or frailty. Eur J Intern Med. 2017.
Shamliyan T, Talley KMC, Ramakrishnan R, Kane RL. Association of frailty with survival: a systematic literature review. Ageing Res Rev. 2013.
Vaupel JW. Biodemography of human ageing. Nature. 2010.
Yang Z, Norton EC, Stearns SC. Longevity and health care expenditures: the real reasons older people spend more. Journals Gerontol - Ser B Psychol Sci Soc Sci. 2003.
Boult C, Green AF, Boult LB, Pacala JT, Snyder C, Leff B. Successful models of comprehensive care for older adults with chronic conditions: evidence for the institute of medicine’s “retooling for an Aging America” report. J Am Geriatr Soc. 2009.
Goodwin N, Dixon A, Anderson G, Wodchis W. Providing integrated care for older people with complex needs: Lessons from seven international case studies. Kings Fund. 2014.
Nuño R, Coleman K, Bengoa R, Sauto R. Integrated care for chronic conditions: the contribution of the ICCC Framework. Health Policy. 2012.
Carter M, Grover V. Me, my self, and I(T): conceptualizing information technology identity and its implications. MIS Quarterly: Management Information Systems. 2015.
Gorini A, Riva G. Virtual reality in anxiety disorders: the past and the future. Expert Rev Neurother. 2008.
Mujber TS, Szecsi T, Hashmi MSJ. Virtual reality applications in manufacturing process simulation. J Mater Process Technol. 2004.
Beard JR, Bloom DE. Towards a comprehensive public health response to population ageing. The Lancet. 2015.
Garçon L, Khasnabis C, Walker L, Nakatani Y, Lapitan J, Borg J et al. Medical and assistive health technology: meeting the needs of aging populations. Gerontologist. 2016.
Dasenbrock L, Heinks A, Schwenk M, Bauer JM. Technology-based measurements for screening, monitoring and preventing frailtyScreening, monitoring und Prävention von (Pre-)Frailty mit technologiebasierten assessments. Z Gerontol Geriatr. 2016.
Barlow J, Singh D, Bayer S, Curry R. A systematic review of the benefits of home telecare for frail elderly people and those with long-term conditions. J Telemed Telecare. 2007.
D SDS. G. K. Evaluating the evidence base for the use of home telehealth remote monitoring in elderly with heart failure. Telemed J E Health. 2009.
Keränen NS, Kangas M, Immonen M, Similä H, Enwald H, Korpelainen R et al. Use of information and communication technologies among older people with and without frailty: a population-based survey. J Med Internet Res. 2017.
Carretero S. Technology-enabled services for older people living at home independently: lessons for public long-term care authorities in the EU Member States. JRC Work Pap. 2015.
Stroetmann KA, Kubitschke L, Robinson S, Stroetmann V, Cullen K, McDaid D. How can telehealth help in the provision of integrated care? World Heal Organ. 2010.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009.
Carreto S, Stewart J, Centeno C, Barbabella F, Schmidt A, Lamontagne-godwin F et al. Can Technology-based Services support Long-term Care Challenges in Home Care ? An. alysis of Evidence from Social Innovation Good Practices across the EU: CARICT Projet Summary Report. 2012.
Antonopoulos I, Robu V, Couraud B, Kirli D, Norbu S, Kiprakis A et al. Artificial intelligence and machine learning approaches to energy demand-side response: a systematic review. Renew Sustain Energy Rev. 2020.
Das S, Dey A, Pal A, Roy N. Applications of Artificial Intelligence in Machine Learning: review and Prospect. Int J Comput Appl. 2015.
Muhanna MA. Virtual reality and the CAVE: Taxonomy, interaction challenges and research directions. Journal of King Saud University - Computer and Information Sciences. 2015.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016.
Thiese MS. Observational and interventional study design types; an overview. Biochem Med. 2014.
Higgins J, Green S. Cochrane Handbook for systematic reviews of Interventions Version 5.1.0 [updated March 2011]. Colloids Surf B Biointerfaces. 2011.
Whiting PF, Rutjes AWS, Westwood ME, Mallett S, Deeks JJ, Reitsma JB et al. Quadas-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011.
Hayden JA, Côté P, Bombardier C. Evaluation of the quality of prognosis studies in systematic reviews. Ann Intern Med. 2006.
Dupuy L, Froger C, Consel C, Sauzéon H. Everyday functioning benefits from an assisted living platform amongst frail older adults and their caregivers. Front Aging Neurosci. 2017.
Orlandoni P, Jukic Peladic N, Spazzafumo L, Venturini C, Cola C, Sparvoli D et al. Utility of video consultation to improve the outcomes of home enteral nutrition in a population of frail older patients. Geriatr Gerontol Int. 2016.
Takahashi PY, Pecina JL, Upatising B, Chaudhry R, Shah ND, Van Houten H et al. A randomized controlled trial of telemonitoring in older adults with multiple health issues to prevent hospitalizations and emergency department visits. Arch Intern Med. 2012.
Tomita MR, Mann WC, Stanton K, Tomita AD, Sundar V. Use of currently available smart home technology by frail elders: process and outcomes. Top Geriatr Rehabil. 2007.
Volders E, Bolman CAW, De Groot RHM, Verboon P, Lechner L. The effect of active plus, a computer-tailored physical activity intervention, on the physical activity of older adults with chronic illness(es)-A cluster randomized controlled trial. Int J Environ Res Public Health. 2020.
Kubicki A, Bonnetblanc F, Petrement G, Mourey F. Motor-prediction improvements after virtual rehabilitation in geriatrics: frail patients reveal different learning curves for movement and postural control. Neurophysiol Clin. 2014.
Lee SC, Tsai JM, Tsai LY, Liang LJ, Wu CP. Promoting physical activity and reducing frailty of middle-aged and older adults in community: the effects of a health promotion program combining smart phone learning and exercise. Int J Gerontol. 2019.
Mateo-Abad M, Fullaondo A, Merino M, Gris S, Marchet F, Avolio F et al. Impact assessment of an innovative integrated care model for older complex patients with multimorbidity: the carewell project. Int J Integr Care. 2020.
Persson HL, Lyth J, Lind L. The health diary telemonitoring and hospital-based home care improve quality of life among elderly multimorbid copd and chronic heart failure subjects. Int J COPD. 2020.
Ozaki K, Kondo I, Hirano S, Kagaya H, Saitoh E, Osawa A et al. Training with a balance exercise assist robot is more effective than conventional training for frail older adults. Geriatr Gerontol Int. 2017.
Alqahtani BA, Ferchak MA, Huppert TJ, Sejdic E, Perera S, Greenspan SL et al. Standing balance and strength measurements in older adults living in residential care communities. Aging Clin Exp Res. 2017.
Ambagtsheer RC, Shafiabady N, Dent E, Seiboth C, Beilby J. The application of artificial intelligence (AI) techniques to identify frailty within a residential aged care administrative data set. Int J Med Inform. 2020.
Kubicki A. Functional assessment in older adults: should we use timed up and go or gait speed test? Neurosci Lett. 2014.
Paliokas I, Kalamaras E, Votis K, Doumpoulakis S, Lakka E, Kotsani M et al. Using a Virtual Reality Serious Game to Assess the Performance of Older Adults with Frailty. In: Advances in Experimental Medicine and Biology. 2020.
Parvaneh S, Mohler J, Toosizadeh N, Grewal GS, Najafi B. Postural Transitions during Activities of Daily Living Could Identify Frailty Status: Application of Wearable Technology to Identify Frailty during Unsupervised Condition. Gerontology. 2017.
Ritt M, Schülein S, Lubrich H, Bollheimer LC, Sieber CC, Gassmann KG. High-technology based gait assessment in frail people: Associations between spatio-temporal and three-dimensional gait characteristics with frailty status across four different frailty measures. J Nutr Heal Aging. 2017.
Tsipouras MG, Giannakeas N, Tegou T, Kalamaras I, Votis K, Tzovaras D. Assessing the Frailty of Older People using Bluetooth Beacons Data. In: International Conference on Wireless and Mobile Computing, Networking and Communications. 2018.
Boumans R, Van Meulen F, Hindriks K, Neerincx M, Rikkert MGMO. Robot for health data acquisition among older adults: a pilot randomised controlled cross-over trial. BMJ Qual Saf. 2019.
Camicioli R, Mizrahi S, Spagnoli J, Büla C, Demonet JF, Vingerhoets F et al. Handwriting and pre-frailty in the Lausanne cohort 65+ (Lc65+) study. Arch Gerontol Geriatr. 2015.
Galán-Mercant A, Cuesta-Vargas AI. Differences in trunk accelerometry between frail and nonfrail elderly persons in sit-to-stand and stand-to-sit transitions based on a mobile inertial sensor. JMIR mHealth uHealth; 2013.
Galán-Mercant A, Cuesta-Vargas AI. Mobile Romberg test assessment (mRomberg). BMC Res Notes. 2014.
Galán-Mercant A, Cuesta-Vargas AI. Clinical frailty syndrome assessment using inertial sensors embedded in smartphones. Physiol Meas. 2015.
Garcia-Moreno FM, Bermudez-Edo M, Garrido JL, Rodríguez-García E, Pérez-Mármol JM. Rodríguez-Fórtiz MJ. A microservices e-health system for ecological frailty assessment using wearables. Sens (Switzerland). 2020.
Gianaria E, Grangetto M, Roppolo M, Mulasso A, Rabaglietti E. Kinect-based gait analysis for automatic frailty syndrome assessment. In: Proceedings - International Conference on Image Processing, ICIP. 2016.
Gokalp H, De Folter J, Verma V, Fursse J, Jones R, Clarke M. Integrated Telehealth and Telecare for Monitoring Frail Elderly with Chronic Disease. Telemedicine and e-Health. 2018.
Martín-Lesende I, Recalde E, Viviane-Wunderling P, Pinar T, Borghesi F, Aguirre T et al. Mortality in a cohort of complex patients with chronic illnesses and multimorbidity: a descriptive longitudinal study. BMC Palliat Care. 2016.
Merchant RA, Hui RJY, Kwek SC, Sundram M, Tay A, Jayasundram J et al. Rapid Geriatric Assessment using Mobile App in Primary Care: prevalence of geriatric Syndromes and Review of its feasibility. Front Med. 2020.
Hassler AP, Menasalvas E, García-García FJ, Rodríguez-Mañas L, Holzinger A. Importance of medical data preprocessing in predictive modeling and risk factor discovery for the frailty syndrome. BMC Med Inform Decis Mak. 2019.
Peng LN, Hsiao FY, Lee WJ, Huang ST, Chen LK. Comparisons between hypothesis- and data-driven approaches for multimorbidity frailty index:a machine learning approach. J Med Internet Res. 2020.
Sargent L, Nalls M, Amella EJ, Slattum PW, Mueller M, Bandinelli S et al. Shared mechanisms for cognitive impairment and physical frailty: a model for complex systems. Alzheimer’s Dement Transl Res Clin Interv. 2020.
Schiltz NK, Dolansky MA, Warner DF, Stange KC, Gravenstein S, Koroukian SM. Impact of Instrumental Activities of Daily Living Limitations on Hospital Readmission: an observational study using machine learning. J Gen Intern Med. 2020.
Graña M, Lopez-Guede JM, Irazusta J, Labayen I, Besga A. Modelling hospital readmissions under frailty conditions for healthy aging. In: Expert Systems. 2020.
Held F, Le Couteur DG, Blyth FM, Hirani V, Naganathan V, Waite LM et al. Polypharmacy in older adults: Association rule and frequent-set analysis to evaluate concomitant medication use. Pharmacol Res. 2017.
Violán C, Foguet-Boreu Q, Fernández-Bertolín S, Guisado-Clavero M, Cabrera-Bean M, Formiga F et al. Soft clustering using real-world data for the identification of multimorbidity patterns in an elderly population: cross-sectional study in a Mediterranean population. BMJ Open. 2019.
Wang RH, Kenyon LK, McGilton KS, Miller WC, Hovanec N, Boger J, et al. The time is now: a FASTER Approach to Generate Research evidence for technology-based interventions in the field of disability and Rehabilitation. Archives of Physical Medicine and Rehabilitation; 2021.
Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and impact of real-world Clinical Data for the practicing clinician. Advances in Therapy; 2018.
Singal AG, Higgins PDR, Waljee AK. A primer on effectiveness and efficacy trials. Clin Transl Gastroenterol. 2014.
Acknowledgements
Alessia Gallucci wishes to thank all the authors for providing useful ideas and supervision during the conceptualization, writing, and revisionof the manuscript.
Funding
The work reported in this publication was granted by the Italian Ministry of Health, under the Aging Network of Italian Research Hospitals (IRCCS) (Project: “Next Generation Promising (NGP): a new network approach to frailty, multimorbidity and age-related disease in the Era of Precision Medicine” RCR-202-223682286).
Author information
Authors and Affiliations
Contributions
All authors contributed significantly to the study conception and design. Material preparation, data collection and analysis were performed by Alessia Gallucci, Pietro Davide Trimarchi, CosimoTuena, Silvia Cavedoni, Francesca Romana Greco and Antonio Greco. The first draft of the manuscript was written by Alessia Gallucci and Pietro Davide Trimarchi and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. No other contributors assisted the authors in this work.
Corresponding author
Ethics declarations
Competing interests
All Author have not conflict of interests to declare.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: the authors requested to correct Dr. Cosimo Tuena’s affiliation to “Applied Technology for Neuro-Psychology Lab, IRCCS Istituto Auxologico Italiano, Milan, Italy”.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gallucci, A., Trimarchi, P.D., Tuena, C. et al. Technologies for frailty, comorbidity, and multimorbidity in older adults: a systematic review of research designs. BMC Med Res Methodol 23, 166 (2023). https://doi.org/10.1186/s12874-023-01971-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-023-01971-z