
Abstract
Background
This study aimed to investigate whether awareness of being monitored by an accelerometer has an effect on physical activity in young people.
Methods
Eighty healthy participants aged 10–18 years were randomized between blinded and nonblinded groups. The blinded participants were informed that we were testing the reliability of a new device for body posture assessment and these participants did not receive any information about physical activity. In contrast, the nonblinded participants were informed that the device was an accelerometer that assessed physical activity levels and patterns. The participants were instructed to wear the accelerometer for 4 consecutive days (2 school days and 2 school-free days).
Results
Missing data led to the exclusion of 2 participants assigned to the blinded group. When data from the blinded group were compared with these from the nonblinded group, no differences were found in the duration of any of the following items: (i) wearing the accelerometer, (ii) total physical activity, (iii) sedentary activity, and (iv) moderate-to-vigorous activity.
Conclusions
Our study shows that the awareness of wearing an accelerometer has no influence on physical activity patterns in young people. This study improves the understanding of physical activity assessment and underlines the objectivity of this method.
Trial registration
NCT02844101 (retrospectively registered at July 13th 2016).
Similar content being viewed by others
Background
Physical activity (PA), especially moderate-to-vigorous PA (MVPA), is widely recognized as an important determinant of health in children and adolescents [1, 2]. Thus, accurate measurement of PA is essential for developing intervention strategies in epidemiological studies. PA questionnaires, diaries, pedometers, and accelerometers have been used widely to assess PA in free-living conditions [3].
Accelerometry is frequently used in PA studies and it is recognized as a reliable, valid, and objective measurement [4]. A major concern regarding the objective assessment of PA is the Hawthorne effect, i.e. the change in PA behavior related to the participant’s awareness of being monitored to actually assess their PA pattern [3, 5]. The term reactivity has been used to describe the action of modifying PA behaviors when wearing a measurement device [3, 6, 7]. In other words, participants in PA studies may increase their daily and routine activities when they know that they are wearing a device to assess their habitual PA.
Findings on the reactivity measured with a pedometer in children and adolescents are controversial; however, few studies have assessed reactivity using accelerometer devices in youth [6, 8,9,10,11,12]. One study showed no reactivity to accelerometers in young adults in contrast to another study in teenagers who were all well-informed about the nature and purpose of the device (i.e. it measured their PA patterns), which may have elicited some degree of reactivity [6, 13]. Recently, Davis and Loprinzi did not observe sufficient evidence of accelerometer reactivity among United States (US) children and adolescents [8].
The conflicting results of the previous studies on accelerometer reactivity in youth create difficulties in the interpretations and understanding of accelerometer reactivity in young people [6, 8]. Moreover, the authors used an indirect methodology (i.e. a nonexperimental design) that could lead to a potential bias in their results.
Therefore, the aim of this study was to assess reactivity to an accelerometer in young people by comparing PA measured in teenagers wearing the device who were randomized into 2 groups: 1 group was aware of the real nature of the device, but the second group was informed only that the device aimed to assess body posture.
Methods
Participants
Eighty healthy participants (44 boys, 36 girls) from several primary care pediatrician offices in northern France volunteered for the study. The inclusion criteria were: (i) subjects were aged between 10 and 18 years old; (ii) informed consent was signed by the participant as well as his/her parents; (iii) absence of medical contraindication for daily PA (e.g. cardiovascular diseases, musculoskeletal pain); and (iv) no simultaneous inclusion in other biomedical studies. All participants underwent a medical examination to exclude potential contraindications for the study.
Before the study began, the aims and objectives were explained carefully to each adolescent and their parents. Written informed consent was obtained from the adolescent and the parents. Written informed consent was obtained from the adolescent and the parents. The study was approved by the Research Ethics Committee of the University of Lille (Comité Protection des Personnes, Nord Ouest IV, Lille, France). All procedures were performed according to the ethical standards of the Helsinki Declaration of 1975, as revised in 2008, and European Good Clinical Practice.
Procedure
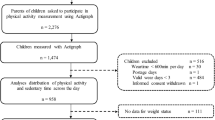
The study started in September 2013 and ended in June 2015. Participants were referred to the Clinical Research Centre of the Lille University Hospital. Body mass index was measured to the nearest 0.1 kg using an electronic scale (Seca, Hamburg, Germany) after removal of shoes or heavy outer garments. Height was measured to the nearest 0.1 cm using a stadiometer (Seca). The included participants were randomized using sealed envelopes between the blinded group (n = 40) and the nonblinded group (n = 40). The randomization was centralized in the study center using a 1:1 ratio of blinded to nonblinded participants, which was divided into height blocks to obtain 4 blinded participants and 4 nonblinded participants per block. Participants assigned to the blinded group were informed that the study targeted the reliability of a new device assessing body posture. However, participants assigned to the nonblinded group were aware of the device being an accelerometer for PA assessment. The participants in the nonblinded group were given full information about the device, i.e. how the device detects body movements, measures sedentary behaviors (e.g. sleeping, lying before the TV, playing video games) as well as vigorous activities (e.g. playing soccer, cycling, running). The explanations were given by the same researcher, who was not blinded about the randomization of the groups. Participants wore the accelerometer on their lower back under their clothing using an elastic belt and adjustable buckle. All participants were instructed to remove the device during contact sports, water-based activities (swimming, showering, and bathing), and overnight. To fairly assess PA patterns in both groups, the participants were asked to keep a log diary of when and why the device was removed (Fig. 1) [14]. The sport activities performed after removal of the device were classified in agreement with the Compendium of Energy Expenditures for Youth and time spent in moderate or vigorous PA was added. Activities between 4 and 6 metabolic equivalents of task (MET) were defined as moderate PA and activities with 6 or more MET were defined as vigorous PA [15]. According to consensus recommendations for assessing PA in youth, a minimum of 2 or 3 days measured is needed to estimate weekly usual PA behavior in children and adolescents [16,17,18]. We a priori decided to record 4 days of PA behavior to ensure that our data reflected weekly PA, including leisure time. The accelerometers recorded activity for 4 consecutive days (2 school days and 2 school-free days) in free-living conditions. The devices were collected after the 4-day monitoring and the data were transferred from the device to a computer. To ensure the compliance of the subjects of the blinded group, the following 3 questions were asked: (i) Did you search online for any information regarding the device? (ii) Did you receive any information about this device by your peers? If so, which? (iii) Are you aware of the use or utility of this device?

The log diary used in this study
Materials
The triaxial accelerometer used was the ActiGraph® Monitor (Model GT3X; ActiGraph, Pensacola, CA, USA) (46 × 33 × 15 mm; weight 19 g, additional technical features) [19]. The accelerometer measures acceleration and deceleration in 3 spatial dimensions according to a vertical vector (x), an anteroposterior vector (y), and a mediolateral vector (z). The vector magnitude (VM) was calculated as follows: VM = √(×2+y2+z2). The epoch interval for the accelerometer was set at 1 s. A computer was used to initialize and synchronize the accelerometer. Participants who recorded less than 10 h of activity per day were excluded from the analyses [18]. PA levels were categorized as follows: sedentary activity, 0–180 counts.15 s−1; light activity, 181–757 counts.15 s−1; moderate activity, 758–1112 counts.15 s−1; and vigorous activity, >1112 counts.15 s−1 [20]. The interinstrument reliability of this device is reported to be better for moderate and vigorous activities than for sedentary activity [19, 21]. Data were averaged and expressed in counts.min−1.
Outcomes
The primary outcome was the overall total counts per minute over the 4 day-period. The secondary outcome was the daily time spent at each PA level (sedentary, light, moderate, vigorous, and moderate to vigorous) calculated over the 4 day-period. All outcomes were also analyzed over the 4-day period, and school days were separated from school-free days.
Sample calculation and statistical analysis
Based on the data of Martinez-Gomez and colleagues, we hypothesized that the mean of total counts.min−1 would be reduced by 20% in the blinded group compared with the nonblinded group (corresponding to an absolute difference of 100 counts counts.min−1) [22]. With a standard deviation of 150 counts.min−1, a power of 80% and an alpha risk of 5%, 37 adolescents per group were required to detect this effect size (effect size of −0.67 considered as medium to large according to Cohen) [23]. To compensate for the potential missing data, inclusion of 40 subjects per group was required. Data were analyzed using SAS software (version 9.3; SAS Institute, Cary, NC). Statistical testing was conducted at the 2-tailed α-level of 0.05. Data were expressed as mean ± standard deviation (SD) or percentages as appropriate. Normality of distributions was assessed using histograms and the Shapiro–Wilk test. Data between groups were compared using Student’s t test. Cohen’s d effect sizes (standardized mean differences between nonblinded vs. blinded groups) were calculated and interpreted as small for absolute value = 0.2, medium for value = 0.5, large for value = 0.8 and very large effect for value = 1.3 [23].
Results
Eighty participants were enrolled in the study and equally randomized into 2 groups. Two teenagers (aged 14 and 16 years old) assigned to the blinded group were excluded because of missing data in PA assessment (monitoring failure). The 38 participants from the blinded group remained unaware of the true nature of the device (according to data from the ad hoc questionnaire) and their main characteristics (Table 1) overlapped with those of the nonblinded group (n = 40).
The duration of wearing the accelerometer did not differ between the 2 groups for the overall 4-day-period, nor did it differ after separating school days from school-free days. Similarly, total counts per day over the 4 day-period did not vary significantly between the nonblinded and blinded groups (mean ± SD, 178.8 ± 57.9 vs. 201.8 ± 69.5; effect size, −0.36, p = 0.12) (Table 2). Only 3 participants performed PA during sports (i.e. swimming, contact sports) after removal of the accelerometer, as reported in their log diaries. This accounted for 180 min out of the 60,366 min of the total recording (0.02%). This small amount of time was considered irrelevant. Table 2 details the PA patterns, including all activities. No difference was observed between school days and school-free days on any of the PA parameters between the 2 groups (Table 2).
Discussion
The present study is the first to examine whether children and adolescents changed their PA behavior when wearing motion sensors using an experimental design. Our findings clearly showed that there was no difference in PA patterns (school days and school-free days) between the young people in the blinded vs. the nonblinded groups, which contrasted with what we had hypothesized initially.
Two previous studies addressing this question arrived at contrasting results, but the authors used an indirect methodology [6, 8]. Instead of randomizing the children into different groups according to their awareness of the accelerometer, the researchers compared the measurements of the first day to the 6 following days [6, 8]. In the first study, the authors observed a 3–7% reduction in PA over the 6 remaining days compared to the first day, which evoked the presence of reactivity to the accelerometer in children [6]. In the second study, Davis and Loprinzi showed no evidence of reactivity in US children and adolescents when considering the total activity counts per day or the time spent in MVPA [8]. Davis and Loprinzi described the reasons for the discrepancy using results from Dösseger et al., i.e. the population differences and the structure of the built environment that may elicit more engagement in free-play situations for Swiss children than that for their American counterparts [6, 8]. The methodological differences and biases induced by the awareness of the nature of the device by all patients can justify the disagreement in findings between these 2 studies and ours [6, 8].
Other studies using a pedometer in adults mostly suggest reactivity [24,25,26]. However, several factors should be considered. Firstly, adults are more sensitive to the current PA recommendation and their own PA compared to children and adolescents [27, 28]. Secondly, some teenagers cannot do PA when they wish because of their family constraints, lifestyles, and/or school rhythms [29, 30]. Another interesting difference can be observed in the direct and continuous view of the results; adults could observe the digital screen of their pedometer, which contrasts with the measurement of PA by the accelerometer in our study, where all subjects remained blind to their individual counts throughout the study. In addition, when PA was assessed by use of a pedometer, the participants were asked to file a daily step log, which may have further affected their motivation for PA. Wearing a pedometer has been reported to be a simple, noninvasive way to increase awareness of daily activity, which led to an increase in PA by adult women [31].
The main strength of the study is the use of the random assignment of treatment condition vs. real covert condition, which provides confidence in our findings. However, our results have to be interpreted with caution because we only included healthy young people. Therefore, our conclusions cannot be extended to pathologic conditions. It would be judicious to investigate the reactivity in subpopulations including overweight or obese children and other chronic diseases such as respiratory diseases or diabetes. Finally, we did not collect the parents’ education level or socioeconomic status. These parameters may influence attitudes to healthy lifestyles, PA, and the motivation to wear a monitor.
Conclusions
Our findings show that the awareness of wearing an accelerometer does not influence PA and PA patterns in healthy youth people. Therefore, the study confirms that accelerometry is an objective method that accurately reflects habitual PA and can be used for monitoring PA in children and adolescents.
Abbreviations
- MVPA:
-
Moderate-to-vigorous physical activity
- PA:
-
Physical activity
References
Hallal PC, Victora CG, Azevedo MR, Wells JC. Adolescent physical activity and health: a systematic review. Sports Med. 2006;36:1019–30.
Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports. 2006;16:3–63.
Welk GJ, Corbin CB, Dale D. Measurement issues in the assessment of physical activity in children. Res Q Exerc Sport. 2000;71:S59–73.
Vanhelst J, Hardy L, Gottrand F, Béghin L. Technical aspects and relevance of physical activity assessment in children and adolescents in free-living conditions. Arch Pediatr. 2012;19:1219–25.
Wickström G, Bendix T. The “Hawthorne effect”—what did the original Hawthorne studies actually show? Scand J Work Environ Health. 2000;26:363–7.
Dössegger A, Ruch N, Jimmy G, Braun-Fahrländer C, Mäder U, Hänggi J, et al. Reactivity to accelerometer measurement of children and adolescents. Med Sci Sports Exerc. 2014;46:1140–6.
Intille SS, Lester J, Sallis JF, Duncan G. New horizons in sensor development. Med Sci Sports Exerc. 2012;44:S24–31.
Davis R, Loprinzi PD. Examination of accelerometer reactivity among a population sample of children, adolescents, and adults. J Phys Act Health. 2016;24:1–27.
Ozdoba R, Corbin C, Le Masurier G. Does reactivity exist in children when measuring activity levels with unsealed pedometers? Pediatr Exerc Sci. 2004;16:158–66.
Rowe D, Mahar M, Raedeke T, Lore J. Measuring physical activity in children with pedometers: reliability, reactivity, and replacement of missing data. Pediatr Exerc Sci. 2004;16:343–54.
Vincent SD, Pangrazi RP. Does reactivity exist in children when measuring activity levels with pedometers? Pediatr Exerc Sci. 2002;14:56–63.
Wickel E, Eisenmann J, Pangrazi R, Graser SV, Raustorp A, Tomson LM, et al. Do children take the same number of steps every day? Am J Hum Biol. 2007;19:537–43.
Behrens TK, Dinger MK. Motion sensor reactivity in physically active young adults. Res Q Exerc Sport. 2007;78:1–8.
Ottevaere C, Huybrechts I, De Meester F, De Bourdeaudhuij I, Cuenca-Garcia M, De Henauw S. The use of accelerometry in adolescents and its implementation with non-wear time activity diaries in free-living conditions. J Sports Sci. 2011;29:103–13.
Ridley K, Ainsworth BE, Olds TS. Development of a compendium of energy expenditures for youth. Int J Behav Nutr Phys Act. 2008;10:45.
Ruiz JR, Ortega FB, Martínez-Gómez D, Labayen I, Moreno LA, De Bourdeaudhuij I, et al. Objectively measured physical activity and sedentary time in European adolescents: the HELENA study. Am J Epidemiol. 2011;174:173–84.
Trost SG, Pate RR, Freedson PS, Sallis JF, Taylor WC. Using objective physical activity measures with youth: how many days of monitoring are needed? Med Sci Sports Exerc. 2000;32:426–31.
Rich C, Geraci M, Griffiths L, Sera F, Dezateux C, Cortina-Borja M. Quality control methods in accelerometer data processing: defining minimum wear time. PLoS One. 2013;8:e67206.
Santos-Lozano A, Marín PJ, Torres-Luque G, Ruiz JR, Lucía A, Garatachea N. Technical variability of the GT3X accelerometer. Med Eng Phys. 2012;34:787–90.
Romanzini M, Petroski EL, Ohara D, Dourado AC, Reichert FF. Calibration of ActiGraph GT3X, Actical and RT3 accelerometers in adolescents. Eur J Sport Sci. 2014;14:91–9.
Santos-Lozano A, Torres-Luque G, Marín PJ, Ruiz JR, Lucia A, Garatachea N. Intermonitor variability of GT3X accelerometer. Int J Sports Med. 2012;33:994–9.
Martínez-Gómez D, Welk GJ, Calle ME, Marcos A, Veiga OL, AFINOS Study Group. Preliminary evidence of physical activity levels measured by accelerometer in Spanish adolescents: the AFINOS study. Nutr Hosp. 2009;24:226–32.
Cohen J. Statistical power analysis for the Behavioral sciences. 2nd ed. Hillsdale: Lawrence Erlbaum Associates; 1988. p. 455.
Clemes SA, Deans NK. Presence and duration of reactivity to pedometers in adults. Med Sci Sports Exerc. 2012;44:1097–101.
Clemes SA, Matchett N, Wane SL. Reactivity: an issue for short-term pedometer studies? Br J Sports Med. 2008;42:68–70.
Clemes SA, Parker RA. Increasing our understanding of reactivity to pedometers in adults. Med Sci Sports Exerc. 2009;41:674–80.
Corder K, van Sluijs EM, Goodyer I, Ridgway CL, Steele RM, Bamber D, et al. Physical activity awareness of British adolescents. Arch Pediatr Adolesc Med. 2011;165:603–9.
Corder K, van Sluijs EM, McMinn AM, Ekelund U, Cassidy A, Griffin SJ. Perception versus reality awareness of physical activity levels of British children. Am J Prev Med. 2010;38:1–8.
Gorely T, Atkin AJ, Biddle SJ, Marshall SJ. Family circumstance, sedentary behaviour and physical activity in adolescents living in England: project STIL. Int J Behav Nutr Phys Act. 2009;11:33.
Story M, Nanney MS, Schwartz MB. Schools and obesity prevention: creating school environments and policies to promote healthy eating and physical activity. The Milbank Quarterly. 2009;87:71–100.
Rooney B, Smalley K, Larson J, Havens S. Is knowing enough? Increasing physical activity by wearing a pedometer. WMJ. 2003;102:31–6.
Acknowledgements
The authors thank the participants for enrolling in the study. The authors recognize Dr. Ravasi for English editing the manuscript, on behalf of the University of Lille, France.
Funding
There is no funding to support this study.
Availability of data and materials
The dataset supporting the conclusions of this article and the full protocol of the study are available upon request from JV.
Author information
Authors and Affiliations
Contributions
Each author of this article significantly contributed to the study, especially: JV, LB and FG designed research; JV, LB, SC and FG conducted research; JV analyzed data; JV, LB, and FG wrote the paper; ED analyzed data and performed statistical analysis; FG had primary responsibility for final content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Research Ethics Committee of the University of Lille (Comité Protection des Personnes, Nord Ouest IV, Lille, France). All procedures were performed according to the ethical standards of the Helsinki Declaration of 1975, as revised in 2008, and European Good Clinical Practice.
Consent for publication
The aims and objectives were explained carefully to each adolescent and their parents. Written informed consent was obtained from the adolescent and the parents.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Vanhelst, J., Béghin, L., Drumez, E. et al. Awareness of wearing an accelerometer does not affect physical activity in youth. BMC Med Res Methodol 17, 99 (2017). https://doi.org/10.1186/s12874-017-0378-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-017-0378-5