
Abstract
Background
There is a need for improving cohort retention in longitudinal studies. Our objective was to identify cohort retention strategies and implementation approaches used in studies with high retention rates.
Methods
Longitudinal studies with ≥200 participants, ≥80% retention rates over ≥1 year of follow-up were queried from an Institutional Review Board database at a large research-intensive U.S. university; additional studies were identified through networking. Nineteen (86%) of 22 eligible studies agreed to participate. Through in-depth semi-structured interviews, participants provided retention strategies based on themes identified from previous literature reviews. Synthesis of data was completed by a multidisciplinary team.
Results
The most commonly used retention strategies were: study reminders, study visit characteristics, emphasizing study benefits, and contact/scheduling strategies. The research teams were well-functioning, organized, and persistent. Additionally, teams tailored their strategies to their participants, often adapting and innovating their approaches.
Conclusions
These studies included specialized and persistent teams and utilized tailored strategies specific to their cohort and individual participants. Studies’ written protocols and published manuscripts often did not reflect the varied strategies employed and adapted through the duration of study. Appropriate retention strategy use requires cultural sensitivity and more research is needed to identify how strategy use varies globally.
Similar content being viewed by others

Background
Retention of study participants is vital to ensure the power and internal validity of longitudinal research [1–3]. A high attrition rate increases the risk of bias, particularly if those lost to follow-up differ from those retained in the study or if there is differential attrition between the intervention and control groups in a randomized controlled trial (RCT) [1].
Investigation to identify effective retention strategies has increased over recent years [4]. The following retention strategy themes were identified in two systematic reviews: (1) contact and scheduling methods, (2) visit characteristics, (3) study personnel, (4) nonfinancial incentives, (5) financial incentives, (6) reminders, (7) special tracking methods, (8) study description, (9) benefits of study, (10) reimbursement, (11) study identity, and (12) community involvement [4, 5]. Studies that used multiple retention strategies had higher retention rates [4]. Despite the knowledge gained from these systematic reviews, an inherent limitation is that they were limited to published data and did not allow for in-depth exploration of retention strategies and their implementation. They potentially overlooked other retention strategies or themes that may have been effective in existing research.
The objective of this study was to identify, via survey and in-depth, semi-structured interviews, cohort retention strategies and implementation approaches used in longitudinal clinical research studies that achieved high retention rates. We intentionally focused the research question on studies that had success with high retention rates, with the goal of learning from their experience and establishing a template and tools for successful retention practices. Findings from this study augment existing information on retention strategies from previous research and systematic reviews [3–9], and inform researchers designing studies and cohort retention tools.
Methods
A naturalistic inquiry approach was utilized to increase our understanding of retention practices in longitudinal studies that achieved high retention rates. The Johns Hopkins Medicine Institutional Review Board (IRB) database, which consists of the protocols from 7 separate IRBs with over 6500 active protocols, was queried to identify a convenience sample of studies that met the following inclusion criteria: 1) recruited ≥200 adult participants, 2) followed the participants for ≥1 year, and 3) retained ≥80% of participants using the following search: “Outcomes OR Cohort OR Longitudinal OR Long-term OR Long term OR Chronic OR Follow-up OR Follow AND Brain injury OR Chronic Obstructive Pulmonary Disease (COPD) OR Congestive Heart Failure (CHF) OR Hypertension OR “Kidney disease” OR Leukemia OR End-Stage Liver Disease (ESLD) OR Cancer OR Oncology OR Oncological OR Tumor OR End-Stage Renal Disease (ESRD) OR “Renal failure” OR Dialysis”.
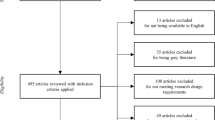
Principal investigators of identified studies were contacted via an email with a description of this study and were asked to confirm study eligibility. For eligible studies, principal investigators were then asked for agreement to participate in this study and to provide contact information for a study team member who could answer detailed questions regarding the study’s retention strategies. In addition, investigators contacted members of their professional networks known to have conducted longitudinal studies within the institution. Six additional principal investigators were identified, four of whom were eligible and provided interviews. Of the 139 total studies identified through IRB query and related enquiries to established principal investigators, 22 met the inclusion criteria and 19 (86%) semi-structured interviews were completed. Reasons for not providing interviews included study completion >5 years prior, change in principal investigator, and departure of study staff responsible for retention efforts. Participants did not receive any financial incentive for participation. The Johns Hopkins Medicine Institutional Review Board approved this study with a waiver of informed consent.
Interview and data analysis procedures
The interview guide was created, reviewed and revised by four team members with expertise in longitudinal, patient-centered outcomes research (CDH, DMN, VDD, MNE). The interview guide included collection of background information on the eligible study’s design and methodology, followed by a detailed exploration of domains of inquiry related to retention strategies. Interviews were conducted in-person or by phone by two research assistants (MA, MC), who received training on the interview guide and data collection practices prior to initiation of the study. Interview questions were provided, upon request, via an online survey before the interviews to help the interviewee gather necessary information. Two study coordinators initially responded via the online survey (Active Surveillance of Prostate Cancer, and the Longitudinal Study of Alzheimer's Disease and Other Memory Disorders), then completed the remainder of interview by phone. Prior to the interviews, the research assistants performed an online search for any study-related publications and websites that provided information on the study aims, longitudinal research visits, retention strategies and retention rates to help focus the interview. In addition, study teams were asked to provide any additional study publications or written protocols that specifically outlined retention strategies. The team of investigators reviewed the data from each interview to explore emerging common findings. According to established qualitative research methods [10], the interview guide was iteratively refined and adapted to ask subsequent study participants about additional strategies that emerged in initial interviews. Then, the data was reviewed and independently coded by four investigators (MAA, MC, MNE, CDH), using a priori themes established in prior systematic reviews (Table 1) [4, 5]. After 19 interviews, data saturation was reached. A final review of the data was performed to synthesize overarching findings from the interviews.
Results
Of the 19 participating studies, 13 were prospective cohort studies, 5 were RCTs, and 1 was a quasi-experimental study (Table 2). Included studies had diverse patient populations, including victims of intimate partner violence, persons living with human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS), survivors of critical illness and other serious illnesses. The target sample size for studies ranged from 255-10,000. Actual sample recruitment at the time of interview ranged from 205 for the Community Aging in Place – Advancing Better Living for Elders (CAPABLE) study [11] with older adults aging in place to 2528 for the Alzheimer’s Disease Anti-Inflammatory Prevention Trial (ADAPT) [12]. Though each of the studies retained at least 80% of participants, 10 (53%) of the 19 studies achieved >90% retention. Five of the participating studies had published articles describing the study protocol, including some reference to retention protocols [11, 13–16]. However, none of the studies empirically tested retention strategies within their study.
Table 3 provides a distribution of retention strategies employed across studies. The most commonly used strategies were from the following themes: reminders, visit characteristics, benefits of the study, and contact and scheduling. The strategy themes of study description and non-financial incentives were least reported by the participating studies. Some of the studies (Active Surveillance of Prostate Cancer study and Early Detection and Predicting Recurrence in Non Small Cell Lung Cancer study) embedded their research data collection in regular clinic visits to reduce patient burden, using the clinic protocols to serve as patient reminders. This group of clinic-based studies embedded within routine clinical care used very few strategies for recruitment and retention.
Based on the interviews, the following were key findings associated with success in achieving high cohort retention rates: 1) cohort research staff are specialized, organized, persistent, and communicate well; 2) “personal touches” matter: tailoring retention strategies to individuals; and 3) written protocols do not reflect the many details of retention strategies employed during conduct of the study. Findings related to each of these three key messages are described below.
Research staff are specialized, organized, persistent, and communicate well
The majority of studies (n = 11) used a team approach to retain study participants, employing several staff members to collect data and manage retention. Two of these studies employed a full-time staff member dedicated to implementing retention strategies and focused on optimizing participant follow up. Five of 11 studies allocated a specific number of participants to one team member who served as the study’s primary point of contact for that group of participants. This person was given strategic support at team meetings, which included adapting or developing new approaches to overcome retention barriers when standard methods of contacting a participant had been exhausted. Other features of these successful teams included selecting appropriate individuals with responsibility for participant contact and providing intensive training and support on study protocols, including retention techniques. In recruiting research staff for cohort retention activities, study teams often screened applicants for experience, communication skills, cultural-competence and specialized knowledge of the population (e.g. Spanish-speaking, domestic violence advocate). One research team provided training focused on providing staff with a common understanding of empathy and sensitivity, including mock interviews to prepare new staff prior to contacting participants on their own [13, 17–19].
In most study teams, participant data tracking was complex; tracking methods were used to inform retention efforts and facilitate communication among team members. Rigorous monitoring, often using spreadsheets or databases, enabled team evaluation of the success of retention strategies or conversely the need to adapt or innovate for the most difficult-to-reach participants. Detailed records were kept for the participant and at least one additional contact person. These records were updated at every participant contact. Study staff used phone numbers, email, texting, social media (e.g., Facebook) and internet searches to locate participants. Studies visited participants’ homes, used personal delivery of reminders and searched obituaries, court documents and incarceration records to locate participants. One highly experienced study coordinator developed a checklist of techniques used to search for participants to help ensure a complete and systematic search process was consistently undertaken.
Study teams ensured regular internal communication regarding cohort retention issues through meetings involving research assistants, study coordinators, data managers and principal investigators. During these meetings, study teams examined their latest recruitment and retention rates, discussed strategies for participants who were difficult to contact and provided each other support and ideas. One study mentioned the importance of setting daily participant contact goals for each team member; another study used friendly competition as a way to engage team members.
“Personal touches” matter: tailoring retention strategies to individuals
To facilitate study visits, studies used tools and strategies tailored to the characteristics of individual participants or specific study requirements. For example, one study that required fasting prior to the visit provided snacks after the test was completed [20]. Some encouraged participants to bring items from home to make themselves comfortable, such as a blanket or pillow. Others provided meals or coffee. Two studies involving victims of intimate partner violence arranged for a safe meeting place and transportation as well as childcare [15, 21]. In many of the studies, parking and transportation were reimbursed. Studies also used financial compensation as a retention strategy, with amounts ranging from $10 for 1 h of survey response to $200 for a full day of data collection with invasive testing.
To help keep participants engaged throughout the study’s follow-up period, studies employed various methods. For instance, studies sent regular newsletters and cards for holidays, birthdays and even condolences. Many studies sent reminder letters about the study and upcoming visits at regular intervals. Lastly, many teams sought to develop strong staff-participant relationships by having the same staff throughout the follow-up period, which created long-standing relationships (e.g., decade-long) between study staff and participants. However, some studies, such as the CAPABLE study [11], did not require the same staff member to perform follow-up and yet were able to maintain a high retention rate throughout the study.
When appropriate, some studies sought to engage participants in groups, instead of individually, fostering a sense of community. For example, some studies hosted educational discussion forums where physicians or nurses led small group discussions related to disease management. Participants with Fuch’s corneal dystrophy were encouraged to invite the study team to family gatherings and reunions to provide education and testing for this genetic disorder. Other studies engaged participants through annual events, often held at entertainment venues (e.g., a dinner theater, horse racing) [20], using these events to encourage camaraderie among participants and study staff. Finally, one study invited participants to send in artwork created by the participant or their grandchildren to be used in future study correspondence and a calendar that featured different artwork for each month that was sent to each participant [20].
Protocols do not reflect the many details of retention strategies employed
Only 3 (16%) of 19 studies provided written cohort retention protocols. Recognizing this pattern after the initial interviews, we added interview questions to explore the lack of written protocols to delineate retention strategies. Interviews revealed that existing study protocols were not detailed regarding techniques to locate and retain participants or were out of date. Since strategies were frequently adapted to reflect new or revised retention strategies tailored to individual participant’s circumstances, with many of the changes verbally discussed during team meetings, revised retention strategies were noted but not updated in the actual protocol. Notably, principal investigators (PIs) and study coordinators agreed that IRB review and approval is an important process and that they developed study protocols recognizing IRB and ethical issues. In some studies, retention protocols submitted to the IRB included general principles for follow-up, rather than a detailed protocol, due to concern that a detailed protocol would require frequent IRB submissions with amendments and not be practicable to implement. Moreover, there were conflicting perceptions regarding whether or not the IRB would be supportive of cohort retention approaches that include internet or social media searches and persistence when trying to locate hard-to-find participants.
Discussion
The 19 studies with high cohort retention evaluated via in-depth interviews were heterogeneous in terms of design, sample size, target population and length of follow up. This heterogeneity allowed for exploration of a variety of approaches to cohort retention strategies and confirmed the 12 categories of retention strategies previously established. However, this study does provide further insight through the thematic analysis of in-depth interviews. These studies had research staff members who are specialized, persistent and collaborate well to accomplish their retention goals teams. They utilized personalized approaches and tailored retention strategies specific to participants in the study cohorts. This tailoring of strategies that are not formally documented in written form is an iterative process based largely on the experience and persistence of study coordinators. Cultural acceptability and feasibility of study and retention practices was evaluated by the expertise and experience of the study staff. This tailoring was facilitated by an understanding of social, cultural and environmental norms particular to the population studied.
Previous systematic reviews identified over 900 retention strategies across 88 studies, with higher retention attained in studies using more retention strategies [4, 5]. The present study suggests the importance of having a well-functioning research team that is organized, persistent, adaptable, and innovative. Prior studies focused on financial incentives to recruit and retain participants, finding a positive correlation between magnitude of incentive and retention rates [4, 5]. In our study, the use of financial incentives varied, yet all studies had high rates of retention, suggesting that participants also respond to additional strategies, such as facilitating visits and emphasizing other potential benefits of participating in the study. The in-depth interviews from this study confirm prior empirical analyses that demonstrated that achieving high retention rates requires use of multiple retention strategies and often many contact attempts by highly skilled staff [4, 22]. However, it is not clear which strategies are the most effective for study teams with limited budgets to implement. Though budget allocation for retention-specific activities was not assessed, most of these high retention studies were federally funded and adequately resourced; 15 of 19 studies had personnel that were trained and specialized, contributing to the high retention. Future studies should conduct comparative effectiveness evaluations regarding different budget allocations for retention to inform financial budget planning and prioritization among potential retention strategies.
While most research teams indicated that they have a retention protocol, after in-depth interviews, it became evident that the protocols were generally non-specific, often not reflecting all detailed aspects of retention practices. Moreover, the most successful study teams iteratively refined their retention processes in practice without updating protocols, and individualized them to specific participants. Maintaining updated retention protocols may be valuable for staff training and for maintaining high retention rates throughout the study, especially in the event of staff turnover. In addition, social media is in constant evolution and investigators should consider using technologies available to provide high quality longitudinal data. A recent article examined feasibility of using websites and social media for recruitment and demonstrated that a young female urban population is more likely to respond to these methods than traditional methods such as flyers and health fairs [23]. These recruitment strategies also use a small amount of study team resources, however it is unclear if this would be true for the purposes of retention.
Certain retention strategies are likely to have culturally-specific considerations. The question of appropriate methods and frequency for contact attempts is an important area for further exploration and may have variation in acceptability depending on the population. Likewise, the ethics of financial incentives have been widely discussed and remain an important ethical consideration. In addition, ethical regulation and oversight of studies has great variation within large academic centers, between institutions, and globally. In addition, IRB policies continue to evolve, particularly in response to new strategies such as digital and social media-based approaches for participant contact. Research practices and policies must ensure cultural-sensitivity and the protection of subjects while facilitating efficient and effective longitudinal research.
Findings from this study should be considered in light of several strengths and potential limitations. This study’s strength is the novelty of using in-depth interviews to obtain unpublished data from research teams to explore successful retention strategies for following large cohorts for at least one year. Moreover, a heterogeneous mix of high retention studies were included, with varying cohort sizes (205–2528 participants) and types of study population, including a national cohort study (ARDS Network Long Term Outcome Study – ALTOS) that enrolled over 900 acute respiratory distress syndrome (ARDS) survivors from more than 40 sites [17, 19]. However, this study also has potential limitations. First, only studies with ≥200 participants and retention rates ≥80% were considered; thereby, potentially limiting the comprehensiveness and generalizability of the data collected. However, all retention strategies from a prior systematic review [4] were exemplified through the interviews, offering some replication of findings. Future studies may examine how studies with low retention have used retention strategies and if practical resources can support study teams to improve retention rates. Also, in this study a convenience sample of studies were screened for eligibility from only one institution; hence additional retention strategies may be uncovered if conducted with a larger number of studies from other research centers. Social, cultural and regulatory body acceptance of the retention strategies described may vary by institution and internationally. As these retention strategies are used outside of the US, additional cultural tailoring of retention strategies may be required and should be studied empirically. Finally, the design of our study allowed us to identify strategies that were used together with a high degree of success. However, since these research teams applied multiple strategies we were not able to identify which individual strategies were superior. Given our insights regarding the need to tailor strategies to the context of the target population and other study factors, it is possible that each strategy identified could be implemented and yet retention goals still may not be met in a given study. To move the science of cohort retention forward, studies that compare retention strategies to identify best practices are needed.
There is need and ongoing effort to address the lack of attention and resources focused on cohort retention in longitudinal studies, including increasing number of studies reporting on retention strategies [4, 5]. To ensure validity and generalizability of results, future studies must consider and allocate resources for retention activities. This includes judiciously composing an effective research team specialized in implementing retention strategies. This project, undertaken as part of a National Heart, Lung, and Blood Institute-funded grant (R24HL111895) to create a national research infrastructure, aims to assist clinical researchers in achieving high retention rates by providing practical resources (see Tables 3, 4 and http://www.improvelto.com/).
Conclusions
In-depth interviews with research staff from longitudinal studies with high cohort retention are instructive in complimenting existing empirical literature in understanding successful strategies for cohort retention. Our findings emphasize the importance of creating and sustaining well-functioning research teams focused on cohort retention, applying personalized approaches and tailored retention strategies, and continually evaluating, refining and documenting retention strategies through the duration of the study.
Abbreviations
- AIDS:
-
Acquired immunodeficiency syndrome
- ARDS:
-
Acute respiratory distress syndrome
- HIV:
-
Human immunodeficiency virus
- IRB:
-
Institutional Review Board
- RCT:
-
Randomized controlled trial
References
Fewtrell MS, Kennedy K, Singhal A, Martin RM, Ness A, Hadders-Algra M, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch Dis Child. 2008;93(6):458–61.
Siddiqi AE, Sikorskii A, Given CW, Given B. Early participant attrition from clinical trials: role of trial design and logistics. Clin Trials. 2008;5(4):328–35.
Gupta A, Calfas KJ, Marshall SJ, Robinson TN, Rock CL, Huang JS, et al. Clinical trial management of participant recruitment, enrollment, engagement, and retention in the SMART study using a Marketing and Information Technology (MARKIT) model. Contemp Clin Trials. 2015;42:185–95.
Robinson KA, Dinglas VD, Sukrithan V, Yalamanchili R, Mendez-Tellez PA, Dennison-Himmelfarb CR, et al. Updated systematic review identifies substantial number of retention strategies: using more strategies retains more study participants. J Clin Epidemiol. 2015;68(12):1481–7.
Robinson KA, Dennison CR, Wayman DM, Pronovost PJ, Needham DM. Systematic review identifies number of strategies important for retaining study participants. J Clin Epidemiol. 2007;60(8):757–65.
Hindmarch P, Hawkins A, McColl E, Hayes M, Majsak-Newman G, Ablewhite J, et al. Recruitment and retention strategies and the examination of attrition bias in a randomised controlled trial in children’s centres serving families in disadvantaged areas of England. Trials. 2015;16:79.
Taylor RM, Mohain J, Gibson F, Solanki A, Whelan J, Fern LA. Novel participatory methods of involving patients in research: naming and branding a longitudinal cohort study, BRIGHTLIGHT. BMC Med Res Methodol. 2015;15:20.
Brueton VC, Tierney JF, Stenning S, Meredith S, Harding S, Nazareth I, et al. Strategies to improve retention in randomised trials: a Cochrane systematic review and meta-analysis. BMJ Open. 2014;4(2):e003821.
Booker CL, Harding S, Benzeval M. A systematic review of the effect of retention methods in population-based cohort studies. BMC Public Health. 2011;11:249.
Flick U. An introduction to qualitative research. Berlin: SAGE Publications; 2009.
Szanton SL, Wolff JW, Leff B, Thorpe RJ, Tanner EK, Boyd C, et al. CAPABLE trial: a randomized controlled trial of nurse, occupational therapist and handyman to reduce disability among older adults: rationale and design. Contemp Clin Trials. 2014;38(1):102–12.
Meinert CL, McCaffrey LD, Breitner JC. Alzheimer’s disease anti-inflammatory prevention trial: design, methods, and baseline results. Alzheimers Dement. 2009;5(2):93–104.
Needham DM, Dennison CR, Dowdy DW, Mendez-Tellez PA, Ciesla N, Desai SV, et al. Study protocol: the Improving Care of Acute Lung Injury Patients (ICAP) study. Crit Care. 2005;10(1):R9. http://ccforum.com/content/10/1/R9.
Sabbagh MN, Thompson N, Tweedy D, Stipho-Majeed S, Kawas C, Connor DJ. Recruitment and retention strategies for clinical trials in Alzheimer’s disease. Pharm Dev Regul. 2003;1(4):269–76.
Clough A, Wagman J, Rollins C, Barnes J, Connor-Smith J, Holditch-Niolon P, et al. The SHARE project: maximizing participant retention in a logitudinal study with victims of intimate partner violence. Field Methods. 2011;23(1):86–101.
Tosoian JJ, Trock BJ, Landis P, Feng Z, Epstein JI, Partin AW, et al. Active surveillance program for prostate cancer: an update of the Johns Hopkins experience. J Clin Oncol. 2011;29(16):2185–90.
Dinglas VD, Hopkins RO, Wozniak AW, Hough CL, Morris PE, Jackson JC, et al. One-year outcomes of rosuvastatin versus placebo in sepsis-associated acute respiratory distress syndrome: prospective follow-up of SAILS randomised trial. Thorax. 2016;71:401–10.
Ruhl AP, Huang M, Colantuoni E, Lord RK, Dinglas VD, Chong A, et al. Health care resource use and costs in long-term survivors of ARDS: a 5-year longitudinal cohort study. Crit Care Med. 2017;45(2):196–204.
Needham DM, Dinglas VD, Bienvenu OJ, Colantuoni E, Wozniak A, Rice TW, et al. One year outcomes of initial trophic vs full enteral feeding in acute lung injury patients: prospective follow-up ofthe EDEN randomized trial. BMJ. 2013;346:f1532.
Denker M, Boyle S, Anderson AH, Appel LJ, Chen J, Fink JC, et al. Chronic Renal Insufficiency Cohort Study (CRIC): overview and summary of selected findings. Clin J Am Soc Nephrol. 2015;10(11):2073–83.
Eden KB, Perrin NA, Hanson GC, Messing JT, Bloom TL, Campbell JC, et al. Use of online safety decision aid by abused women: effect on decisional conflict in a randomized controlled trial. Am J Prev Med. 2015;48(4):372–83.
Dinglas VD, Huang M, Sepulveda KA, Pinedo M, Hopkins RO, Colantuoni E, et al. Personalized contact strategies and predictors of time to survey completion: analysis of two sequential randomized trials. BMC Med Res Methodol. 2015;15:5.
Staffileno BA, Zschunke J, Weber M, Gross LE, Fogg L, Tangney CC. The feasibility of using Facebook, craigslist, and other online strategies to recruit young African American Women for a web-based healthy lifestyle behavior change intervention. J Cardiovasc Nurs. 2016.
Jabs DA, Van Natta ML, Holbrook JT, Kempen JH, Meinert CL, Davis MD. Longitudinal study of the ocular complications of AIDS: 1. Ocular diagnoses at enrollment. Ophthalmology. 2007;114(4):780–6.
Jabs DA, Van Natta ML, Holbrook JT, Kempen JH, Meinert CL, Davis MD. Longitudinal study of the ocular complications of AIDS: 2. Ocular examination results at enrollment. Ophthalmology. 2007;114(4):787–93.
Morris JC, Weintraub S, Chui HC, Cummings J, DeCarli C, Ferris S, et al. The Uniform Data Set (UDS): clinical and cognitive variables and descriptive data from Alzheimer Disease Centers. Alzheimer Dis Assoc Disord. 2006;20(4):210–6.
Enroll-HD: a worldwide observational study for Huntington’s disease families. 2016. Available from: https://www.enroll-hd.org/ Accessed 8-3-2016.
Bhasin B, Lau B, Atta MG, Fine DM, Estrella MM, Schwartz GJ, et al. HIV viremia and T-cell activation differentially affect the performance of glomerular filtration rate equations based on creatinine and cystatin C. PLoS One. 2013;8(12):e82028.
Ryan DH, Espeland MA, Foster GD, Haffner SM, Hubbard VS, Johnson KC, et al. Look AHEAD (Action for Health in Diabetes): design and methods for a clinical trial of weight loss for the prevention of cardiovascular disease in type 2 diabetes. Control Clin Trials. 2003;24(5):610–28.
Vasanth S, Eghrari AO, Gapsis BC, Wang J, Haller NF, Stark WJ, et al. Expansion of CTG18.1 Trinucleotide repeat in TCF4 is a potent driver of Fuchs’ corneal dystrophy. Invest Ophthalmol Vis Sci. 2015;56(8):4531–6.
Drummond MB, Merlo CA, Astemborski J, Kalmin MM, Kisalu A, Mcdyer JF, et al. The effect of HIV infection on longitudinal lung function decline among IDUs: a prospective cohort. AIDS. 2013;27(8):1303–11.
Brock MV, Hooker CM, Ota-Machida E, Han Y, Guo M, Ames S, et al. DNA methylation markers and early recurrence in stage I lung cancer. N Engl J Med. 2008;358(11):1118–28.
Chuang YF, An Y, Bilgel M, Wong DF, Troncoso JC, O’Brien RJ, et al. Midlife adiposity predicts earlier onset of Alzheimer’s dementia, neuropathology and presymptomatic cerebral amyloid accumulation. Mol Psychiatry. 2016;21(7):910–5.
O’Neal WK, Anderson W, Basta PV, Carretta EE, Doerschuk CM, Barr RG, et al. Comparison of serum, EDTA plasma and P100 plasma for luminex-based biomarker multiplex assays in patients with chronic obstructive pulmonary disease in the SPIROMICS study. J Transl Med. 2014;12:9.
Acknowledgements
Not applicable.
Funding
This research was supported by the National Heart, Lung, and Blood Institute [R24HL111895] and the Johns Hopkins Institute for Clinical and Translational Research which is funded in part by the National Center for Advancing Translational Sciences [UL1TR001079]. The funding bodies had no role in the design and conduct of the study.
Availability of data and material
The dataset for the current study is available from the corresponding author on reasonable request.
Authors’ contributions
DMN, MNE, VDD and CDH contributed to the conception and/or design of this study. MAA and MIAC contributed to the acquisition of data. All authors contributed to the analysis and interpretation of data. MAA drafted the manuscript, and CDH and VDD critically revised it for important intellectual content. All authors reviewed and approved the final version to be submitted.
Competing interests
MNE received an honorarium from Praxis Pharmaceuticals and Boehringer Ingelheim, unrelated to this project.
Consent for publication
Not Applicable.
Ethics approval and consent to participate
Ethics approval was obtained from the Johns Hopkins Medicine Institutional Review Board (NA_00087504) with a waiver of informed consent.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Abshire, M., Dinglas, V.D., Cajita, M.I.A. et al. Participant retention practices in longitudinal clinical research studies with high retention rates. BMC Med Res Methodol 17, 30 (2017). https://doi.org/10.1186/s12874-017-0310-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-017-0310-z