
Abstract
Background
Various papers have addressed pros and cons of the stepped wedge cluster randomized trial design (SWD). However, some issues have not or only limitedly been addressed. Our aim was to provide a comprehensive overview of all merits and limitations of the SWD to assist researchers, reviewers and medical ethics committees when deciding on the appropriateness of the SWD for a particular study.
Methods
We performed an initial search to identify articles with a methodological focus on the SWD, and categorized and discussed all reported advantages and disadvantages of the SWD. Additional aspects were identified during multidisciplinary meetings in which ethicists, biostatisticians, clinical epidemiologists and health economists participated. All aspects of the SWD were compared to the parallel group cluster randomized design. We categorized the merits and limitations of the SWD to distinct phases in the design and conduct of such studies, highlighting that their impact may vary depending on the context of the study or that benefits may be offset by drawbacks across study phases. Furthermore, a real-life illustration is provided.
Results
New aspects are identified within all disciplines. Examples of newly identified aspects of an SWD are: the possibility to measure a treatment effect in each cluster to examine the (in)consistency in effects across clusters, the detrimental effect of lower than expected inclusion rates, deviation from the ordinary informed consent process and the question whether studies using the SWD are likely to have sufficient social value. Discussions are provided on e.g. clinical equipoise, social value, health economical decision making, number of study arms, and interim analyses.
Conclusions
Deciding on the use of the SWD involves aspects and considerations from different disciplines not all of which have been discussed before. Pros and cons of this design should be balanced in comparison to other feasible design options as to choose the optimal design for a particular intervention study.
Similar content being viewed by others
Background
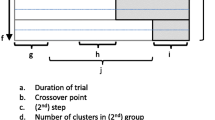
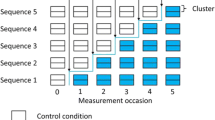
The cluster randomized trial design (CRT), in which (existing) groups of individuals are being randomized, may be considered when randomization of individual participants is not feasible or desirable [1]. Standard CRTs typically use a parallel design where clusters are randomized to either a control or an experimental intervention for the entire study. Alternatively, CRTs may use a crossover design where at a fixed point in time clusters which started with the control treatment switch to the experimental intervention and clusters which started with the experimental intervention switch to the control treatment [1, 2]. The stepped wedge design (SWD), also called phased or staggered implementation and multiple baseline design [3–5] (though not perceived as exactly the same as SWD [6, 7]), is a special type of the CRT crossover design in which clusters cross over in one direction only [6, 8, 9]. All clusters start with the control treatment after which, at pre-specified time points, one or more clusters switch sequentially to the experimental intervention until eventually all clusters have received the new intervention (see Fig. 1). Within this design, clusters are randomized with respect to the time point at which they cross over (referred to as step), not with respect to a treatment condition or order of treatments as in parallel group or usual crossover designs, respectively. Measurements of the endpoints and other variables of interest are being taken in all clusters during the entire study period. A differentiation can be made between the cohort (longitudinal) and cross-sectional SWD [6, 10, 11]. In a cohort SWD, the same subjects within the clusters are being followed over time, hence the crossover between treatments is then not only at the cluster level but also at the subject level. In the cross-sectional SWD, new subjects are being included after each step, which means that the crossover of treatments is only at the cluster level.

Illustration of the stepped wedge design, where different (groups of) clusters switch from control to intervention at different time points
The interest in the application of the SWD in intervention research has sharply increased over the last couple of years [6, 12]. This design was applied in particular to study community level public health interventions that have been proven effective in individual level trials, in so-called phase IV effectiveness trials [6, 9, 12–14], and seems useful for the evaluation of complex healthcare interventions [6, 7, 9, 12, 14–17]. Yet, there is also extensive debate about whether and when the SWD is actually useful for intervention studies [14, 16–22]. The SWD seems to have some natural attractiveness, i.e. the stepwise implementation of the new intervention in each cluster is logistically advantageous [6, 8, 12] and may increase the willingness of clusters to participate [6, 13, 23]. However, this may cause overuse of the SWD, especially when awareness of all potential benefits and drawbacks of this design as compared to feasible alternative designs is fragmented and incomplete.
Previous papers [6, 12, 13] have provided an overview of several perceived pros and cons of the SWD. However, various aspects of the SWD have not yet or only limitedly been addressed, such as considerations related to health economic evaluations of interventions and study ethics. Moreover, discussions of the statistical aspects of the SWD have been limited to sample size and analysis approaches, but do not include interim analyses for example. Furthermore, some pros and cons of the SWD mentioned vary depending on specific characteristics of the study at hand.
Hence, we aim to provide a comprehensive, multidisciplinary overview of the viewpoints on the merits and limitations of the SWD within the CRT setting. We used a set of several methodological papers on the SWD as our starting point to discuss the potential impact of the various features of the SWD in our multidisciplinary team, and to identify features that have not yet been discussed. We set off all identified aspects to the standard parallel group CRT to show which of them are specific to the SWD CRT. Finally, we illustrated several issues by an actual study that applied the SWD. Our overview can assist researchers, reviewers and ethical committees when deciding on the appropriateness of the SWD CRT for a specific intervention study.
Methods
Within a project team consisting of ethicists, biostatisticians, clinical epidemiologists and health economists (all at assistant, associate, or full professor level), we started off by reading and discussing landmark papers describing the stepped wedge design methodology, and systematic reviews describing in which fields and for which reasons the stepped wedge design has been applied. We performed cross-reference checks to find other papers discussing the merits and drawbacks of this design. Finally, we performed a screen search to assure that we did not miss any key papers discussing the stepped wedge methodology. For this purpose we searched Medline, Embase, Pubmed and Web of Science, using the following phrases: step* wedge*, step* wedge* design, and step* wedge* AND research design. The final search was performed on February 2, 2015 without date restrictions. Articles with didactic purposes or reporting best practice guidelines were also included. Articles only reporting the results of an SWD evaluating a specific intervention, without a methodological focus, were excluded.
Based on the resulting set of articles we identified, categorized and discussed all reported advantages and disadvantages of the SWD in the CRT setting. These served as a starting point for the identification of new, additional benefits, viewpoints, challenges and problems, during a series of informal multidisciplinary meetings. All articles were screened by EH, IT, RG, JR and HK, and decisions on eligibility of articles were made by these authors as well. All found and mentioned aspects of the SWD were discussed and set off to the parallel group CRT to identify which of these aspects are indeed unique for the SWD and whether each aspect is an advantage (+) or disadvantage (−) in comparison to the parallel group CRT. If the consequences of an aspect may be similar for the two designs or their impact may be context dependent this was indicated as (~). The results were categorized into three study phases: 1) the study design and preparation phase, 2) the study execution phase, and 3) the data analysis and interpretation phase.
Results and discussion
An overview of all identified SWD characteristics and their potential impact is provided in Tables 1, 2, 3 and 4. Table 1 provides key aspects of the SWD. Tables 2, 3 and 4 contain aspects of the SWD in comparison to the parallel group CRT, where Table 2 contains aspects related to the study design and preparation phase, Table 3 those related to the study execution phase, and Table 4 those related to the data analysis and interpretation phase. We will explain certain aspects (indicated with * in the tables) in more detail below.
Study design and preparation phase (Table 2)
In comparison to the parallel group CRT design, the SWD raises two ethical challenges. Although clinical equipoise and social value are ethical requirements for both designs, the content of these requirements may substantially differ in the two designs, as we will explain below.
Clinical equipoise (2a)
It has been argued that there should be “genuine uncertainty in the expert medical community about the preferred treatment” before a randomized trial is allowed to be conducted [24]. Ensuring this uncertainty balances the duties of physicians as caregivers and researchers. If there is clinical equipoise among two (or more) treatments, physicians who are researchers do not violate their therapeutic duties by withholding a (possibly superior) treatment from their patients.
The SWD is frequently used in situations where the intervention under study has “shown to be effective in more controlled research settings” or may not have shown to be effective yet but is strongly believed to do more good than harm [6, 12]. At first sight, clinical equipoise seems to be absent in these situations. At the same time, one may argue that in spite of the lack of equipoise all participating clusters will receive the seemingly superior experimental intervention at some point during the study. This assumption can be questioned: one should note that although all clusters will receive the experimental intervention, it does not always mean that all participating subjects will receive the experimental intervention. In a cohort design this is the case, but in a cross-sectional SWD only half of the participants will receive the experimental intervention just as in a parallel group CRT [16]. Thus the SWD cannot always prevent that some participants are withheld from the seemingly superior intervention.
Yet it still remains to be proven whether the experimental intervention that is felt superior is actually better. An intervention might have shown efficacy (i.e. work under controlled settings), though still really needs to be evaluated for effectiveness (i.e. does it work in practice). Moreover, when both the experimental intervention and the control arm are established effective interventions participants are in principle not withheld from care as usual, even when one of these arms is felt to be slightly superior before the start of the study. At the same time, when the risks of the arms substantially differ this must be disclosed to research participants [25].
Social value and health care decision making (2b and 2c)
Social value implies that research should be conducted with the aim to produce generalizable health knowledge that will ultimately improve the health of individuals and/or the public [26]. This is an important ethical requirement for human subjects research since the resources for research are limited, so should be well-spent, and people should not be put at risk for the benefit of science and society if there is no social value to be expected [26]. Although results obtained from a singular study using an SWD may lead to health benefits, the social value of SWD studies may be limited compared to parallel group CRTs, in particular from a health economic perspective. Given a limited research budget, performing one study effectively prohibits the execution of another study. This is known as the opportunity cost of a study and represents the “cost” incurred by not enjoying the benefits (i.e. social value) from the best, alternative research activity with similar resource costs [27]. The benefits of performing a study can be defined as the additional insight gained into the health effects, costs and cost-effectiveness of the experimental intervention compared with the control treatment. However, this insight is only valuable when it actually improves decision making on whether to adopt the experimental intervention immediately, to adopt it while also requiring additional evidence collection, to adopt it only in research settings in order to collect more evidence, or to reject the experimental intervention [28]. Such policy decisions are partially based on the balance between the monetary costs and the resulting health benefits of the experimental intervention, i.e. cost-effectiveness. Therefore, the social value of studies is largest when the cost-effectiveness of an experimental intervention is highly uncertain, such that additional evidence may largely reduce the risk of making wrong policy decisions.
The following two situations illustrate the limited usefulness of the SWD from a health economic perspective. First, if the cost-effectiveness of the experimental intervention is highly uncertain, new and unfavourable evidence on health outcomes and costs may lead to the rejection of the experimental intervention. Such a rejection decision might be costly since all clusters will have implemented the intervention by the end of the SWD study. Indeed, all clusters have invested but now need to disinvest while the investment costs may be irrecoverable. On the other hand, if the decision to implement will not be affected by new findings, collecting additional evidence on health outcomes and costs within an SWD is inefficient because this evidence will not influence policy decisions anymore and therefore will have no social value. Although this holds irrespective of whether a parallel group CRT or SWD design is being used, the higher disinvestment costs makes this situation more likely for SWD studies.
Health economic methods have been developed to estimate the social value of a study [29, 30]. These, so-called, value-of-information methods quantify the expected improvement in health outcomes and expected changes in health care costs when the adoption decision can also include evidence from the new study instead of including existing evidence only [31]. The expected social value of a new study increases when the additional evidence it collects will benefit more individuals in the future (that is, when many individuals are eligible for the experimental intervention) and when the study rapidly delivers evidence that remains valuable for a long period of time. Conversely, when some individuals would already receive the experimental intervention the social value of a new study decreases because treatment would change for fewer individuals. In particular, only those future individuals that would have received the control treatment might benefit from a switch to the experimental intervention. In general, these issues might lead to a lower social value of an SWD study as compared to a parallel group CRT, as the SWD study may take longer to complete which reduces the number of future individuals eligible for the experimental intervention. This reduction could, however, be compensated by a faster total implementation process in the entire region of interest (e.g. country or state) following study completion for SWD studies as compared to parallel group CRTs. This advantage depends on the number of clusters included in the SWD or parallel group CRT and the number of not included clusters in the region of interest. If the experimental intervention is accepted for use in clinical practice, the number of clusters in which it still needs to be implemented can be substantially lower after SWD studies than after parallel group CRTs.
Study design (2h)
In a parallel group CRT more than two treatment arms can be included rather easily. For example, usual care can be compared with two experimental interventions within the same study, as illustrated by de Smet et al. [32]. Within the SWD however, this is more difficult. One question that arises is how the clusters will cross over from control to the experimental interventions since there are two possibilities to do so. First, the experimental interventions can be implemented sequentially, that is, clusters cross over from control to one experimental intervention first and at a later time point (step) cross over from this intervention to the other experimental intervention. Secondly, the cross over to one of the experimental interventions can take place at the same time, that is at one step some clusters cross over from control to the first experimental intervention while other clusters cross over to the other experimental intervention. In case of the first situation a (much) longer study period may be required than in the latter situation. In addition to this practical question, it is unclear what the appropriate methods are to calculate the required sample size and to analyse the data resulting from such a three-arm design. Moreover, the question is whether the SWD is a suitable design given the aim of a three-armed study. If there is no practical need to implement the treatments sequentially in clusters over time, other designs will probably provide results in a shorter period of time than the SWD and will therefore be preferable. If, on the other hand, the experimental treatments consist of training of professionals for example, the sequential implementation within the SWD may be very attractive upfront. However, in this example the question is whether the effects of the experimental interventions do not carry over within a cluster from one period to another (given that the trainings are substantially different from each other). One exception to this proposed situation is when one intervention is an add-on to another intervention. For example, in the Helping Hands study [33] one intervention targeted the individual professionals and included education, reminders and feedback. The other intervention extended this by targeting the team level as well and focussed on social influence in groups and leadership. In this example, sequential implementation could be a reasonable choice and carry-over effects would not be an issue. However, since all clusters will be trained for one or both of the experimental interventions, the SWD will probably be more expensive than other design options. Given these issues, it seems questionable whether an SWD is useful if more than two treatment arms are to be included in one study.
Sample size (2i and 2j)
The SWD is often thought to be more efficient than the parallel group CRT since it uses both within- and between-cluster comparisons to estimate a treatment effect [9]. However, in the comparison of designs a difference should be made whether efficiency is in terms of the number of clusters, the number of participants or the total number of measurements required. Furthermore, a difference should be made between a cohort and a cross-sectional design. At the moment, only sample size and power formulae are available for the cross-sectional setting, hence the following discussion will be limited to this setting. Finally, a clear definition of what the parallel group CRT entails should be taken into account. If the parallel group CRT includes only one follow-up measurement of each participant in the analysis (i.e. one measurement period of m participants per cluster), then given an equal cluster size m per measurement period for the SWD, the SWD always requires fewer clusters than the parallel design [34, 35]. However, whether in this case the SWD is also more efficient in terms of the number of participants (which equals the number of measurements in a cross-sectional setting) depends on the cluster size, intracluster correlation coefficient (ICC), and the number of steps [34, 36]. In general, if the ICC is small, the parallel group CRT will have more power, whereas the SWD will have more power in case of a large ICC [37].
If the analysis of a parallel group CRT includes a baseline measurement as a covariate (resulting in an analysis of covariance), then the SWD does not necessarily require fewer clusters in comparison to a parallel group CRT with three measurement periods (one baseline and two follow-up) as shown by Rhoda et al. [5]. They showed that, given a cluster size of 100 participants per group per measurement period, if the ICC is rather small (<0.005) and the number of steps is up to three, the SWD requires more clusters. In case of four steps and ICC ≥ 0.005 or at least five steps and ICC ≥ 0.0001, the SWD requires fewer clusters. However, the total number of measurements (and hence participants in a cross-sectional setting) is higher for the SWD in most cases, except for situations where the ICC ≥ 0.05 and the number of steps is between five and eight. Note that when the cluster size changes the cut-offs in ICCs and numbers of steps will change as well since all of these factors affect the required number of clusters.
Although the numbers might change slightly when the third measurement would not be taken into account as in [5], it can still be expected that the SWD will not always require fewer clusters nor participants depending on cluster size, ICC and number of steps. Yet, Hemming et al. [37] showed that irrespective of the value of the ICC, an SWD with four or more steps will have more power than a parallel group CRT that includes a baseline period (i.e. a two measurement periods design).
Since the SWD requires fewer clusters than the parallel group CRT in many cases as described above, the SWD is especially advantageous when the number of available clusters is limited [12, 14, 16, 21, 22, 34]. Yet, one should be aware that this may come at the cost of a higher number of required participants/measurements.
Study execution phase (Table 3)
Informed consent (3a)
Thus far only Zhan et al. [13] have identified informed consent as a key issue in SWDs by noting that the timing of the informed consent procedure can be difficult. In their trial, the Research Ethics Committee considered it unethical to ask patients informed consent at the start of the study (when care as usual was delivered). Unfortunately, it remained unclear what the exact reasoning was for this judgement but some possible reasons can be listed.
In individual randomized trials, informed consent is given at once for data collection, randomization and administering the experimental intervention, whereas in CRTs participants have to give separate informed consent for these three elements [38]. In particular the latter two elements may raise ethical issues. In CRTs, often the randomization of the clusters has taken place before participants enter the cluster, for example, a hospital has been randomized to one of the treatment arms before a patient enters. Besides, it is usually impossible for participants to move to another cluster and therefore it is then almost virtually impossible for a patient to opt-out (for instance in an emergency situation as in the example of the HEART study described below). This means that participants in CRTs need to consent that they have already been randomized rather than going to be randomized to one of the treatments. These issues are true irrespective of the design choice (parallel group or SWD).
Yet, the informed consent for randomization in an SWD differs from the parallel group CRT in the sense that in a parallel group CRT a cluster is either randomized to the control or the experimental intervention whereas in an SWD all clusters will start providing the control intervention but will switch to the experimental intervention at some point during the study. In a cross-sectional SWD new participants are included after each step leading to half of the participants being exposed to the intervention and the other half to the control. Then the informed consent process is not different from a parallel group CRT. However, if the same participants are being followed over time (a cohort SWD) participants must understand that they are not randomized to one of the treatment arms but that the time point at which they will switch from the control to the experimental treatment is being randomized. So, although participants in this situation will receive the experimental treatment at some time during the study, they should understand that it could be shortly after the start of the study but that it could also be almost at the end of the study. Disclosure of this information may increase the risk of contamination.
Study participation (3b)
Although it is likely that clusters are more willing to participate in an SWD than in a parallel group CRT (because they know they will receive the experimental intervention somewhere during the study) [6, 13, 23], drop out of clusters could be more likely as well. Especially when clusters are being randomized to later steps (which they should not know in advance), they might drop out just because of this delay (clusters may lose interest [21]) or because a similar kind of intervention as the experimental one becomes available during the study. Drop-out of participants will not be an issue if new participants are being included after each step (cross-sectional design). However when the same participants are being followed over time (cohort design) there will be an increased risk of drop-out similar to other longitudinal research designs.
On the other hand, drop-ins may also be more likely in SWDs than in parallel group CRTs [18]. Drop-ins may occur at the participant level in two ways: a participant may already receive the experimental treatment from his caregiver while this caregiver should give the control treatment by design, or the participant may move to another cluster that has already switched to the experimental treatment. The first type of drop-in could be considered a non-adherent cluster, which could lead to biased (contaminated) results if such a participant would be included in the analysis as if he were in the control intervention. The effects of the second type of drop-in may have only limited effect on the results since such a patient then becomes a member of a different cluster and his outcomes would be considered to belong to the ‘new’ cluster. Only if this patient would still report outcomes to his initial cluster as if he received the control intervention, bias may occur. These types of drop-ins can occur in parallel group CRTs as well, but are more likely in SWD studies because they often take more time to complete. Drop-ins at the cluster level are less likely, since clusters agreed with the stepwise implementation within the study upfront.
Inclusion rate (3c)
The effect of lower than expected inclusion rates can be very detrimental in SWDs, because it will disturb the balance in the design and will cause a loss of power. Whereas in parallel group CRTs the inclusion period can be extended rather easily, this is not straightforward in SWDs since it would mean that the time between steps needs to be prolonged which may result in a much longer study period than planned beforehand. This may not be feasible due to financial or other constraints. Furthermore, such a change during the study will result in different lengths of time and different numbers of measurements between steps. If, and how, this may affect the results and validity of the study is not clear yet. Moreover, if the inclusion rate lags behind and it is therefore decided to prolong the time between steps, the risk of drop-out may increase due to further delays for clusters not yet receiving the experimental intervention.
Data analysis and interpretation phase (Table 4)
Measure of effect in each cluster (4b)
Because each cluster in an SWD will switch from control to intervention, it is possible to calculate the effect measure of interest (e.g. difference in means, relative risk, odds ratio) in each cluster and examine the consistency in effect across clusters [37]. Tools applied in meta-analysis can be used to visualize (forest plot) and quantify the inconsistency (τ2 and I2 as heterogeneity measures). Consistency in effect across clusters may increase the strength of the overall finding, whereas inconsistency may complicate the interpretation of the overall finding [39]. Reasons for inconsistency may be explored. Even though the design is often not powered for these analyses, they may still provide additional insights [37].
Interim analyses (4d)
Cumulative monitoring of a study might be warranted to detect potential harmful effects or early dramatic benefits of a new intervention. Several group sequential methods are available and extensively studied for individual randomized trials, but little is known about the application of these methods in the CRT setting. It has been shown that the Pocock and O’Brien-Fleming boundaries can be applied to parallel group CRTs with a binary outcome in order to control the type I error rate, given that all clusters are recruited simultaneously (i.e. start the trial at the same time) and individuals are recruited from those cluster sequentially [40]. However, the aspect of adjustment of the effect estimates following a group sequential CRT has not been studied.
Given that the SWD is most often used when the intervention is thought to do more good than harm and in implementation research, stopping early for harmful effects is unlikely. However, beneficial effects may lead to early stopping and speeding up implementation in the clusters which were allocated to switch treatments at later.
The cross-sectional SWD will use the same recruitment pattern as described for the parallel group CRT. Hence, the results presented above can be expected to apply to SWDs as well. However, within the SWD unequal numbers of measurements are available for each condition after each step (with exception of the last period). That is, at the start of an SWD only measurements under the control condition are available. Then from the first step onwards, the inequality between the number of control and experimental intervention measurements becomes smaller, until at the end of the study the number of measurements under each intervention is similar. The effects of these inequalities on the statistical analysis and power at interim time points are yet unclear, though the unequal numbers of measurements under each treatment over time will generally result in a loss of efficiency [5, 41].
Example: the HEART impact study
Several aspects of the SWD will be illustrated by assessing the HEART Impact study [42–44]. This study uses a cross-sectional SWD and the inclusion of this study has recently completed. Patients presenting at an emergency department with chest pain pose a challenge to physicians since chest pain can be the symptom of an acute coronary syndrome (i.e. acute myocardial infarction or unstable angina) requiring prompt treatment. However, in up to 80 % of the patients it is caused by another, usually non-life-threatening condition. The HEART score has been specifically developed to stratify patients with chest pain according to their risk for cardiac events. Previous studies have shown that this score can adequately identify patients with low, medium or high risk for developing cardiac events [43, 44]. A few hospitals in the Netherlands already apply the HEART score, though other clinical prediction rules [45–47] are being used as well. Yet, the majority of hospitals (or treating physicians) do not use any of the formal prediction rules.
The aim of the HEART Impact study is to quantify the impact of the active use of the HEART score in daily practice on clinical decision making, patient outcomes (incidence of major adverse cardiac events within 6 weeks and quality of life), use of health care resources and costs. The hypotheses are that the use of the HEART score will be safe (comparable incidence of major adverse cardiac events when using the HEART score compared to usual care), will improve the management of the patients presenting with chest pain (in particular fewer hospital admissions and additional testing in low risk patients when using the HEART score), and will reduce overall healthcare costs in this group of patients.
Table 5 shows which aspects of the SWD are relevant in this study. Some of these aspects will be explained in further detail below.
Implementation decisions (5a and 5b)
Collecting data on health outcomes and costs in the HEART Impact study will allow assessment of the cost-effectiveness of the HEART score compared to usual care in clinical practice. Cost-effectiveness results are likely to provide crucial input to a subsequent formal decision on whether to implement the HEART score in the entire Netherlands. Indeed, the HEART-Impact study is expected to provide definitive evidence on the (favourable) cost-effectiveness of the HEART score, meaning that additional studies would have no social value. In the (unlikely) event that the collected evidence would contradict the expected safety and cost savings, de-implementation of this specific intervention in all participating hospitals is very straightforward and virtually costless. Consequently, the collected data on cost-effectiveness is valuable and likely to be used in decision making on (further) implementation of the HEART score.
Informed consent procedure (5f)
In general, informed consent procedures in CRTs, whether parallel cluster or stepped wedge, are ethically complex (see above). Obtaining informed consent also raised ethical issues in the HEART Impact study, in particular because the intervention under evaluation consists of two steps. The first step is to determine the HEART score based on routinely collected information directly after presentation. The researchers of the HEART study received a waiver of informed consent from the research ethics committee for calculating the HEART score since this score is evidence-based, part of the medical professional standard, and determining the score does not involve additional, invasive procedures. The second step of the HEART intervention is the link between the height of the HEART score and certain management options, for example the suggested management for patients with a low HEART score is discharge to home. In practice, there was a time interval between the first and second step of the intervention. During this time interval, the purpose of the study was explained and informed consent for additional data collection and follow-up was obtained. In theory, there were two ways in which patients could opt out: (a) patients refuse consent for data collection and for using the HEART score to guide further treatment decisions; (b) patients refuse consent for data collection but not for using the HEART score to determine further treatments. At first sight, the latter situation seems unproblematic since physicians do not have to consider alternative strategies to guide further treatment decisions. However, the information that is present is essentially the same as in the first situation. Patients who are given the opportunity to opt out are in a situation where it is almost impossible to meaningfully opt out, as we set out earlier in the ethics section since they cannot go to another hospital. Moreover, if they choose to opt out and hence to receive care as usual, this care as usual will be based on the clinician’s professional judgment, which could be guided by the HEART score, by an alternative risk score that the physician used to apply previously, or by his or her overall risk assessment without formal prediction rules.
Conclusions
Our aim was to provide a comprehensive overview of the pros and cons of the SWD from a multidisciplinary viewpoint, moving beyond a systematic review only reiterating previously discussed aspects. We showed that many aspects from different disciplines need to be considered when deciding on a SWD, not all of which have been discussed before. If researchers consider using an SWD for their intervention study all these aspects should be taken into account since seemingly attractive aspects may be outweighed by negative or yet unclear effects of other aspects.
Whether the SWD is the best design option for a specific intervention study needs to be decided by considering all, multidisciplinary (statistical, methodological, ethical and health economical) aspects in comparison to other feasible designs. We agree with Hemming et al. [37] that the SWD is likely to be preferable for studies where some evidence of effectiveness of the experimental intervention is already available, or in cases where the intervention is a service delivery or policy change that does not need individual informed consent to be implemented and where the outcome is preferably available from routinely collected data. However, the SWD may not be a good choice in case of a high risk intervention for which effectiveness has not been shown yet, or in case of an intervention unlikely or unfeasible to be de-implemented when proven ineffective.
Several variations on both the simple SWD and parallel group CRT are possible, such as the staggered parallel group CRT and incomplete SWDs [18, 48]. Although we did not take these variations into consideration explicitly, many of the addressed aspects will still be an issue, though possibly to a different extent.
We distinguished between cross-sectional and cohort designs throughout this paper. For many aspects one can easily see the potential differences. However, for power and sample size calculations this is not straightforward. The available approaches all rely on the cross-sectional design [5, 9, 35, 48, 49]. If a cohort or a mixture of the cross-sectional and cohort design is to be used, both sample size calculations and analyses need to take into account the correlation over time not only at the cluster but also at the individual level. Furthermore, changes over time at both levels should be taken into account. However, it is not clear yet how to incorporate these factors into the design and analysis of SWD studies. Although cohort designs are more efficient than cross-sectional designs in general [50–52], future research is required to see whether this also holds for the SWD (given variations in ICC, number of clusters, cluster size and number of steps) before further comparisons can be made with other designs in this respect.
Several other aspects have been noted to require further research. For example, methods for sample size and power calculations so far have been limited to cross-sectional designs and assumed equal cluster sizes between both clusters and steps. Besides, the possibility of including more than two treatment arms is questionable. Finally, little is known about the use of interim analyses in CRTs altogether [40]. Given that one might expect to be able to stop early for effectiveness within an SWD in situations where there is already an indication of superiority of the new intervention, it is important to know how to perform the interim analyses properly.
In summary, we have provided an overview of all aspects of the SWD that should be taken into consideration when a choice will be made between this design and other valid design options. The SWD is a relatively new design and therefore further research is warranted in order to inform researchers, reviewers and ethical committees better with respect to the question which design to prefer for the study question at hand.
Abbreviations
- CRT:
-
Cluster randomized trial
- SWD:
-
Stepped wedge design
- ICC:
-
Intracluster correlation coefficient
References
Donner A, Klar N. Design and analysis of cluster randomization trials in health research. 1st ed. London: Arnold; 2000.
Rietbergen C, Moerbeek M. The design of cluster randomized crossover trials. J Educ Behav Stat. 2011;36:472–90.
Baer DM, Wolf MM, Risley TR. Some current dimensions of applied behavior analysis. J Appl Behav Anal. 1968;1:91–7.
Hawkins NG, Sanson-Fisher RW, Shakeshaft A, D’Este C, Green LW. The multiple baseline design for evaluating population-based research. Am J Prev Med. 2007;33:162–8.
Rhoda DA, Murray DM, Andridge RR, Pennell ML, Hade EM. Studies with staggered starts: multiple baseline designs and group-randomized trials. Am J Public Health. 2011;101:2164–9.
Brown CA, Lilford RJ. The stepped wedge trial design: a systematic review. BMC Med Res Methodol. 2006;6:54.
Sanson-Fisher RW, D’Este CA, Carey ML, Noble N, Paul CL. Evaluation of systems-oriented public health interventions: alternative research designs. Annu Rev Public Health. 2014;35:9–27.
The Gambia Hepatitis Study Group. The Gambia hepatitis intervention study. Cancer Res. 1987;47:5782–7.
Hussey MA, Hughes JP. Design and analysis of stepped wedge cluster randomized trials. Contemp Clin Trials. 2007;28:182–91.
Ukoumunne O, Gulliford M, Chinn S, Sterne J, Burney P. Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review. Health Technol Assess. 1999;3:98.
Brown C, Hofer T, Johal A, Thomson R, Nicholl J, Franklin BD, et al. An epistemology of patient safety research: a framework for study design and interpretation. Part 2. Study design. Qual Saf Health Care. 2008;17:163–9.
Mdege ND, Man MS, Brown CA T n, Torgerson DJ. Systematic review of stepped wedge cluster randomized trials shows that design is particularly used to evaluate interventions during routine implementation. J Clin Epidemiol. 2011;64:936–48.
Zhan Z, van den Heuvel ER, Doornbos PM, Burger H, Verberne CJ, Wiggers T, et al. Strengths and weaknesses of a stepped wedge cluster randomized design: its application in a colorectal cancer follow-up study. J Clin Epidemiol. 2014;67:454–61.
Mdege ND, Man MS, Taylor nee Brown CA, Torgerson DJ. There are some circumstances where the stepped-wedge cluster randomized trial is preferable to the alternative: no randomized trial at all. Response to the commentary by Kotz and colleagues. J Clin Epidemiol. 2012;65:1253–4.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. Br Med J. 2008;337:a1655.
Keriel-Gascou M, Buchet-Poyau K, Rabilloud M, Duclos A, Colin C. A stepped wedge cluster randomized trial is preferable for assessing complex health interventions. J Clin Epidemiol. 2014;67:831–3.
Mdege ND, Kanaan M. Response to Keriel-Gascou et al. Addressing assumptions on the stepped wedge randomized trial design. J Clin Epidemiol. 2014;67:833–4.
Kotz D, Spigt M, Arts IC, Crutzen R, Viechtbauer W. Use of the stepped wedge design cannot be recommended: a critical appraisal and comparison with the classic cluster randomized controlled trial design. J Clin Epidemiol. 2012;65:1249–52.
Hemming K, Girling A, Martin J, Bond SJ. Stepped wedge cluster randomized trials are efficient and provide a method of evaluation without which some interventions would not be evaluated. J Clin Epidemiol. 2013;66:1058–9.
Kotz D, Spigt M, Arts IC, Crutzen R, Viechtbauer W. The stepped wedge design does not inherently have more power than a cluster randomized controlled trial. J Clin Epidemiol. 2013;66:1059–60.
Viechtbauer W, Kotz D, Spigt M, Arts IC, Crutzen R. Response to Keriel-Gascou et al.: Higher efficiency and other alleged advantages are not inherent to the stepped wedge design. J Clin Epidemiol. 2014;67:834–6.
Kotz D, Spigt M, Arts IC, Crutzen R, Viechtbauer W. Researchers should convince policy makers to perform a classic cluster randomized controlled trial instead of a stepped wedge design when an intervention is rolled out. J Clin Epidemiol. 2012;65:1255–6.
Hutson AD, Reid ME. The utility of partial cross-over designs in early phase randomized prevention trials. Control Clin Trials. 2004;25:493–501.
Freedman B. Equipoise and the ethics of clinical research. N Engl J Med. 1987;317:141–5.
Macklin R, Shepherd L. Informed consent and standard of care: what must be disclosed. Am J Bioeth. 2013;13:9–13.
Emanuel EJ, Wendler D, Grady C. What makes clinical research ethical? JAMA. 2000;283:2701–11.
Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, Stoddart GL. Methods for the economic evaluation of health care programmes. Oxford: Oxford University Press; 2005.
Claxton K, Palmer S, Longworth L, Bojke L, Griffin S, McKenna C, et al. Informing a decision framework for when NICE should recommend the use of health technologies only in the context of an appropriately designed programme of evidence development. Health Technol Assess. 2012;16:1–323.
Eckermann S, Willan AR. Expected value of information and decision making in HTA. Health Econ. 2007;16:195–209.
Claxton KP, Sculpher MJ. Using value of information analysis to prioritise health research: some lessons from recent UK experience. Pharmacoeconomics. 2006;24:1055–68.
Claxton K, Griffin S, Koffijberg H, McKenna C. Expected health benefits of additional evidence: principles, methods and applications. York: Center for Health Economics, University of York; 2013.
de Smet AM, Kluytmans JA, Cooper BS, Mascini EM, Benus RF, van der Werf TS, et al. Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med. 2009;360:20–31.
Huis A, Schoonhoven L, Grol R, Borm G, Adang E, Hulscher M, et al. Helping hands: a cluster randomised trial to evaluate the effectiveness of two different strategies for promoting hand hygiene in hospital nurses. Implement Sci. 2011;6:101.
de Hoop E, Woertman W, Teerenstra S. The stepped wedge cluster randomized trial always requires fewer clusters but not always fewer measurements, that is, participants than a parallel cluster randomized trial in a cross-sectional design. J Clin Epidemiol. 2013;66:1428.
Woertman W, de Hoop E, Moerbeek M, Zuidema SU, Gerritsen DL, Teerenstra S. Stepped wedge designs could reduce the required sample size in cluster randomized trials. J Clin Epidemiol. 2013;66:752–8.
Hemming K, Girling A. The efficiency of stepped wedge vs. cluster randomized trials: Stepped wedge studies do not always require a smaller sample size. J Clin Epidemiol. 2013;66:1427–8.
Hemming K, Haines TP, Chilton PJ, Girling AJ, Lilford RJ. The stepped wedge cluster randomised trial: rationale, design, analysis, and reporting. Br Med J. 2015;350:h391.
Weijer C, Grimshaw JM, Eccles MP, McRae AD, White A, Brehaut JC, et al. The Ottawa statement on the ethical design and conduct of cluster randomized trials. PLoS Med. 2012;9:e1001346.
Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. Rating the quality of evidence-inconsistency. J Clin Epidemiol. 2011;64:1294–302.
Zou GY, Donner A, Klar N. Group sequential methods for cluster randomization trials with binary outcomes. Clin Trials. 2005;2:479–87.
Hayes RJ, Moulton LH. Cluster randomised trials. Boca Raton: CRC Press; 2009.
Poldervaart JM, Reitsma JB, Koffijberg H, Backus BE, Six AJ, Doevendans PA, et al. The impact of the HEART risk score in the early assessment of patients with acute chest pain: design of a stepped wedge, cluster randomised trial. BMC Cardiovasc Disord. 2013;13:77.
Six AJ, Cullen L, Backus BE, Greenslade J, Parsonage W, Aldous S, et al. The HEART score for the assessment of patients with chest pain in the emergency department: a multinational validation study. Crit Pathw Cardiol. 2013;12:121–6.
Backus BE, Six AJ, Kelder JC, Mast TP, van den Akker F, Mast EG, et al. Chest pain in the emergency room: a multicenter validation of the HEART Score. Crit Pathw Cardiol. 2010;9:164–9.
de Araujo GP, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur Heart J. 2005;26:865–72.
Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, Papuchis G, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835–42.
Fox KA, Dabbous OH, Goldberg RJ, Pieper KS, Eagle KA, Van de WF, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). Br Med J. 2006;333:1091.
Hemming K, Lilford R, Girling AJ. Stepped-wedge cluster randomised controlled trials: a generic framework including parallel and multiple-level designs. Stat Med. 2015;34:181–96.
Hemming K, Girling A. A menu-driven facility for power and detectable-difference calculations in stepped-wedge cluster-randomized trials. Stata J. 2014;14:363–80.
Duncan GJ, Kalton G. Issues of design and analysis of surveys across time. Int Stat Rev. 1987;55:97–117.
Feldman HA, Mckinlay SM. Cohort versus cross-sectional design in large field trials - precision, sample-size, and a unifying model. Stat Med. 1994;13:61–78.
Frison L, Pocock SJ. Repeated measures in clinical-trials - analysis using mean summary statistics and its implications for design. Stat Med. 1992;11:1685–704.
van der Tweel I, van der Graaf R. Issues in the use of stepped wedge cluster and alternative designs in the case of pandemics. Am J Bioeth. 2013;13:23–4.
Handley MA, Schillinger D, Shiboski S. Quasi-experimental designs in practice-based research settings: design and implementation considerations. J Am Board Fam Med. 2011;24:589–96.
Fatemi Y, Jacobson RM. The stepped wedge cluster randomized trial and its potential for child health services research: a narrative review. Acad Pediatr. 2015;15:128–33.
Pearson D, Torgerson D, McDougall C, Bowles R. Parable of two agencies, one of which randomizes. An Am Acad Polit Soc Sci. 2010;628:11–29.
van der Graaf R, Koffijberg H, Grobbee DE, de Hoop E, Moons KGM, van Thiel GJMW, et al. Rethinking the ethics of cluster randomized trials: a refinement of the Ottawa statement. J Clin Epidemiol. 2015;68:1108–14.
Acknowledgements
We would like to thank M.J.C. Eijkemans, C.B. Roes, G.A. de Wit, H.F. van Stel, and R.H.H. Groenwold for their input on this manuscript as members of the MultiFaCT project. This project, hence all authors and contributors, was funded by an internal grant from the Julius Center, University Medical Center Utrecht. The funding body had no role in any part of the manuscript nor the decision to submit it for publication.
Funding
Internal grant Julius Center, University Medical Center Utrecht.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
EH drafted most of the manuscript. IT, RG, JR and HK conceived of and designed the study, and participated in drafting the manuscript. KM and JD helped to revise the manuscript and supervised the study. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
de Hoop, E., van der Tweel, I., van der Graaf, R. et al. The need to balance merits and limitations from different disciplines when considering the stepped wedge cluster randomized trial design. BMC Med Res Methodol 15, 93 (2015). https://doi.org/10.1186/s12874-015-0090-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-015-0090-2