
Abstract
Background
Patients who call for emergency medical services (EMS) due to abdominal pain suffer from a broad spectrum of diseases, some of which are time sensitive. As a result of the introduction of the concept of ‘optimal level of care‘, some patients with abdominal pain are triaged to other levels of care than in an emergency department (ED). We hypothesised that it could be challenging in a patient safety perspective.
Aim
This study aims to describe consecutive patients who call for EMS due to abdominal pain and are triaged to self-care by EMS clinicians.
Methods
This was an observational study performed in an EMS organisation in Western Sweden during 2020. The triage tool Rapid Emergency Triage and Treatment System (RETTS), which included Emergency Signs and Symptom (ESS) codes, was used to find medical records where patients with abdominal pain have been triaged to self-care and 194 patients was included in the study.
Results
Of total 48,311 ambulance missions, A total of 1747 patients were labelled with ESS code six (abdominal pain), including 223 (12.8%) who were given the code for self-care and 194 who were further assessed by the research group. Of these patients, 32 (16.3%) had a return visit within 96 hours due to the same symptoms and 11 (5.6%) were hospitalised. In six of these patients, the EMS triage was evaluated retrospectively and assessed as inappropriate. These patients had a final diagnosis of ruptured abdominal aneurysm (n = 1), acute appendicitis with peritonitis (n = 2) and acute pancreatitis (n = 3). All these patients required extensive evaluation and different treatments, including acute surgery, antibiotics and fluid therapy.
Conclusion
Amongst the 1747 patients assessed by EMS due to abdominal pain, 223 (12.8%) were triaged to self-care. Of the 194 patients who were further assessed, 16.3% required a return visit to the ED within 96 hours and 5.6% were hospitalised. Six patients had obvious time-sensitive conditions. Our study highlights the difficulties in the early assessment of abdominal pain and the requirement for an accurate decision support tool.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
An increasing demand for emergency medical services (EMS) has been observed both nationally and internationally [1]. At the same time, a large proportion of EMS patients who have been assessed do not require further EMS interventions [2, 3]. There are several reasons why an increasing number of patients seek EMS help without an actual need for emergency care. Among others, growing health awareness, poor accessibility to primary care services, population growth, ageing and socio-demographic factors have been suggested as some of these reasons [4]. All these factors have changed EMS working routines. Instead of transporting most patients to the emergency department (ED), the concept of ‘the optimal level of care’ has been introduced. This means that EMS teams assess whether a patient can stay at home with self-care instructions, be referred to primary care, be transported to the ED or be transferred directly to specialist examination or treatment [3]. This places great demands on an EMS team’s ability to assess and triage a patient safely to alternative levels of care. A Finnish study revealed that triage to the optimal level of care is a patient-safe method used in EMS units with few adverse events and a very low rate of death related to self-care decisions [5]. EDs can also benefit from patient safety if EMS transport fewer patients to EDs, given that overcrowding is a known ED patient safety threat [6].
However, some symptoms can be connected to higher patient safety risks. For example, neurological symptoms, such as dizziness, are difficult to distinguish from stroke [7, 8]. Sepsis is another condition wherein prehospital identification is quite challenging [9]. Furthermore, chest pain is a symptom wherein the majority of EMS patients have a low-risk condition without the medical need for acute hospital treatment, although 16% have time-sensitive conditions in need of rapid transport to hospital care facilities [10].
When it comes to the concept of ‘the optimal level of care’, abdominal pain is another symptom with potential patient safety risks and hundreds of differential diagnoses, including some time-sensitive diagnoses [11]. Furthermore, abdominal pain is a top five dispatch symptom [12] and the second largest amongst patients triaged to self-care or primary care by EMS [2]. Compared to EDs, EMS have limited methods to distinguish non-urgent reasons for abdominal pain from those requiring urgent interventions in hospitals.
To the best of our knowledge, no previous study has examined the safety of prehospital patients with abdominal pain triaged to self-care by EMS. We hypothesised that it is challenging to safely assess patients in the prehospital setting and to triage them to self care. Therefor the aims of our study were to:
-
1.
investigate requirement of hospitalisation and incidence of incorrect triage by mapping return visits within 4 days with the same symptoms amongst patients with abdominal pain who are triaged to self-care; and
-
2.
investigate which examinations are performed on site by EMS.
Methods
Study design
EMS and hospital medical records were examined in this retrospective observational study. The model for processes in chart review studies suggested by Kaji et al. [13] was used as a guide for the study’s design and methodology. The study proposes 10 important steps to avoid bias in chart review studies as for example systematic data collection and abstractor training.
Population and setting
The study was conducted in an EMS organisation in Western Sweden consisting of six ambulance stations serviced by 27 ambulance units. It has approximately 55,000 EMS missions annually. An ambulance is staffed by at least one registered nurse (RN) with or without 1 year of specialist education in prehospital care. The other crew member can also be an RN or an emergency medical technician (EMT) with an assistant nurse education and a one-year EMT education [14].
According to the local guidelines followed by the EMS organisation in this study, the ambulance team should triage a patient to the optimal level of care. First, all patients are assessed on site at home and then triaged to the optimal level of care (e.g. self-care at home, primary care or ED). The RN, who is responsible for the triage, refers to the clinical guidelines, a triage tool, a triage handbook and telephone contact with ED physicians.
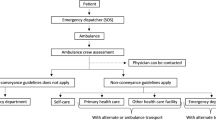
The EMS organisation is using the Rapid Emergency Triage and Treatment System (RETTS) [15] as a triage tool. The triage tool assigns each patient a triage colour that defines the priority designation related to waiting time for a doctor’s assessment at the hospital. The red triage colour stands for ‘life-threatening’, orange for ‘potentially life-threatening’, yellow for ‘non-life-threatening’, green for ‘non-life-threatening and not in need of immediate care’ and blue for ‘no need for triage’. Triage colour is based on two variables: vital signs and type of symptoms. The type of symptoms can be divided according to different Emergency Signs and Symptoms (ESS) codes (Fig. 1). Within this scheme, the ESS code for abdominal pain is ‘6’. Thus, RETTS and EES codes was described in this study in order to give information on how patients were prioritised and how reason for contact with EMS was assessed.

The RETTS triage process
The organisation also uses a symptom-based web decision support system (triage handbook). By clicking on a symptom, the EMS team can access suggestions of examination, diagnoses and advice for further processing. Except as described in guidelines, specific training of assessment in connection with abdominal pain has not been carried out in the included organisation.
The included EMS organisation has the following mandatory examinations and actions in connection to triage to self-care amongst patients with abdominal pain:
-
First survey with the assessment of airway, breathing, circulation and disability (ABCD)
-
Second survey with anamnesis according to Signs and symptoms, Allergies, Medications, Pertinent past history, Last oral intake, Events leading to the injury or illness, Onset, Provokes or Palliates, Quality, Radiates, Severity and Time [16]
-
Measurement of vital signs, including respiration rate, oxygen saturation, pulse rate, blood pressure, degree of consciousness and body temperature
-
Focused assessment in connection to abdominal pain, including inspection, palpation and auscultation of abdomen and blood test of serum glucose
-
RETTS colour blue, green or yellow
-
Contact with a physician
-
Use of triage handbook with descriptions of self-care advice
-
Written information to the patient
Inclusion and exclusion criteria
Data were abstracted from prehospital and hospital medical records. In all, there were 48311primary ambulance missions during the time of the survey. Among them did 1747 patients have ESS code six (abdominal pain) of which 223 patients had the assignment code A05 ‘triaged to self-care’. A total of 194 patients had no exclusion criteria and were therefor included in the study (Fig. 2).

Flow chart showing the inclusion process of medical records for review
The inclusion criteria included the following:
-
All patients were assessed by ambulance during the time period from 1 January to 31 December, 2020, with EES code six and assignment code A05
The exclusion criteria included the following:
-
The ambulance mission was categorised as assisting another ambulance.
-
Inaccurate ESS code
-
Inaccurate assignment code
-
Incomplete patient identification
Data collection
A data collection protocol was developed and pilot-tested before the data search. The protocol comprised data on on-scene assessments according to first and second surveys, measurements of vital parameters (executed and values), focused assessment, triage colour, contact with physician, use of triage handbook, written information to the patient and time on scene. These data were searched for in the EMS organisation’s prehospital medical record system (Ambulink). After conducting individual reviews in Ambulink, the respective prehospital medical records were followed up in the hospital’s medical record system (Melior), from which data on return visit to ED within 96 hours, hospitalisation, care time and ICD code were sampled.
Two of the authors (EO and PH) performed the data collection. They manually screened the medical records together. Both free text and fixed data were used. The relevant data were then transferred to a database where the data was de-anonymised and personal data linked to serial numbers were transferred to a separate codebook stored apart from the dataset. No inter-rater reliability test was performed, as the data collection was executed by two persons together.
Data analysis
The outcome data were summarised using descriptive statistics. A univariate logistical regression analysis was used for predictors of return visits within 96 hours on binary (sex) and continuous variables (age and vital parameters). Significant variables in the univariate regression were considered eligible for inclusion in the multivariate model. A P-value of ≤0.05 was considered significant in the regression. All analyses were performed using SPSS 21.0 (SPSS Inc., Chicago, IL).
Ethical issues
The study was accepted by the research ethics board of Stockholm, Sweden (Dnr 2021–03440) and conducted in agreement with the ethical references of the Swedish Research Council [17].
Results
Amongst patients with abdominal pain who were triaged to self-care, 109 (55.6%) were females. The mean age of the patients was 56.3 years. On average, EMS teams spent a total of 28.0 minutes on the scene with each patient. The patients had normal vital signs (mean) and only three patients were assigned a RETTS colour of orange or red (Table 1).
Prehospital assessment
Compliance to 21 mandatory examinations was at 60.7%, with the greatest compliance attributed to the measurement of vital signs. Three patients had RETTS colours of orange and red, both of which are beyond the recommended triage colour for self-care. Contact with physicians at the EDs and the use of triage handbook had low compliance rates of 28.1 and 12.2%, respectively (Table 2).
Patient outcome
Return visits with the same symptoms within 96 hours were observed in 32 cases (16.3%), whilst 11 (5.6%) were hospitalised. Fourteen patients (7.1%) were transported to a hospital by ambulance and 18 (9.2%) by other transport modes (Table 3). There were 19 different diagnoses amongst the patients required to have return visits, and all corresponded to abdominal pain as a symptom (Table 4). Of 6 patients (3.1%) who were diagnosed, the assessment of prehospital triage to self-care was considered inappropriate. One of the patients, suffering from a ruptured abdominal aortic aneurysm, died within 2 hours after the EMS assessment. The remaining patients were hospitalised from 3 to 120 hours and received surgical interventions, antibiotic therapy or fluid therapy (Table 4).
Predictor for return visits
In the univariate logistic regression, there was only one significant variable that predicted outcome; thus, a multivariate logistic regression was not performed. A lower prehospital oxygen saturation level was a predictor for return visits, with an odds ratio of 0.68 (0.53–0.88) (Table 5). As shown in Fig. 3, the probability for return visits increased from 8% with a saturation of 100–55% to a saturation of 93%.

Predicted probability for return visits 96 hours/hospitalisation in relation to prehospital oxygen saturation
Discussion
The results of this retrospective observational study confirm the hypothesis that, within the prehospital setting, it is challenging to safely assess patients with abdominal pain and triage them to self-care. The revisit rate was 16.3%. Furthermore, 6 patients (3.1%) were assessed to be incorrectly triaged to self-care by the EMS team, thereby endangering patient safety. This statement is made despite the fact that the EMS team’s compliance with guidelines can be considered relatively high.
The prehospital compliance to guidelines has been shown [18] to vary between 7.8–95%. Compliance with examination and treatment recommendations is generally lower compared to compliance with monitoring recommendations. This could also be observed in the present study. There are several reasons for the low guideline compliance in the prehospital setting, including the low evidence level in the guidelines that are being used, prevailing attitudes and workplace culture, and the physical format of the guidelines [18]. Accordingly, this can be an explanation for the poor use of the triage handbook in the present study. One study [19] has shown that paper-based guidelines can be cumbersome to use effectively in connection to patient assessment in the prehospital context.
The EMS team in this study had low compliance when it came to conducting focused examinations, such as abdominal auscultation, inspection and palpation. These are important examinations in the management of patients with abdominal pain. However, even properly performed examinations cannot rule out serious conditions. For example, one study showed that half of patients with peritonitis had normal bowel sounds and that palpation had low sensitivity and specificity for peritonitis [20]. In more than two-thirds of the cases examined, a physician was not contacted for advice; thus, there might be room for improvement to decide the right level of care. A previous study has reported decreased ambulance transport to the ED for patients with low priority conditions when ambulance nurses and physicians collaborate concerning the right level of care [21]. It is important to highlight that the consequences of inferior training in patient assessment already at the internship level of ambulance training. Incomplete assessments and anamnesis in the hospital field might be less dangerous when the patient is under observation for a longer time, the same shortcomings in patient assessment is more dangerous when “treat and release” in the prehospital setting.
The population in the current study is relatively young compared to patients with abdominal pain who are typically admitted to EDs [22]. This is a positive finding, as it probably means that most elderly patients are transported to hospitals. Elderly patients are more likely than younger patients to have severe aetiologies behind their abdominal pain. It has been shown that both mortality and misdiagnosis increase exponentially with each decade of age past 50 [20, 23].
Furthermore, EMS teams have limited opportunities to safely assess and examine patients with abdominal pain. For example, point-of-care blood tests are unusual, and it is impossible to have a patient undergo an X-ray examination on the spot. The common examination methods available are inspection, palpation and auscultation. It is also possible to measure ECG and vital parameters. Anamnesis is also a very important aspect of the examination done in the prehospital setting. At the same time, patients with abdominal pain are also difficult to assess at the ED, despite opportunities for more advanced examinations. Patient history and physical examinations have a sensitivity of 0.25 and a specificity of 0.92 compared to patient history, physical examination, laboratory analysis, acute abdominal series radiographs and non-enhanced helical computed tomography, with a sensitivity of 0.92 and a specificity of 0.90 [24]. Thus, overall, it is difficult to achieve a good assessment of patients with abdominal pain in a prehospital setting.
Meanwhile, we found that oxygen saturation is a critical clinical predictor associated with the risk of a return visit within 96 hours after the initial assessment, with a lower oxygen saturation indicating an increased risk of a return visit. The risk increased even above 90%. Previous studies have indicated that low oxygen saturation in the early phase is associated with an increased risk of adverse events amongst patients with acute myocardial infarction [25] and an increased risk of death amongst patients suffering from stroke [26]. The mechanisms behind these findings can only be speculated upon. A reasonable hypothesis is that when diseases in other organs are so severe that they influence respiration, it can be considered a serious sign.
Furthermore, our findings indicate the need for an accurate decision support tool so that not all patients have to be transported to an ED for evaluation. In developing such a tool, the definition of time-sensitive conditions must be carefully considered. Diseases, such as appendicitis and cholecystitis, should most likely be included in such a definition, regardless of any complication.
Limitations
The main limitation of the present study is the low number of included patients. A study with a larger population could provide a better picture of the prehospital assessment and triage of patients with abdominal pain. Nevertheless, even though generalisability is limited by the small number of patients, the total number from 1 year of ambulance assignments is relatively large enough to highlight potential medical risks amongst patients triaged to self-care. Transferability to other ambulance organisations with similar guidelines should be approached with some caution.
Another limitation is the retrospective study design, which does not allow subsequent analyses of patients’ conditions or diagnoses when they are asked to remain at home. It has been suggested that there is a lack of a clear definition of what constitutes time-sensitive conditions [11]. The current study found that certain diseases could be included in further discussions to improve the precision of prehospital assessment and avoid delayed treatments for patients who require acute hospital care.
Conclusion
Amongst the 1747 patients assessed by EMS due to abdominal pain, 223 (12.8%) were triaged to self-care of which 194 (87%) did not have any exclusion criteria. Among them 16.3% required return visits to EDs within 96 hours and 5.6% were hospitalised. Six patients had obvious time-sensitive conditions. Our study highlights the difficulties involved in the early assessment of patients with abdominal pain and the requirement for an accurate decision support tool.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due the dataset is written in Swedish and needs to be translated to be useful for non-Swedish speakers, but are available from the corresponding author on reasonable request.
Abbreviations
- ED:
-
Emergency Department
- EMS:
-
Emergency Medical Service
- RETTS:
-
Rapid Emergency Triage and Treatment System
- VP:
-
Vital Parameters
- ESS codes:
-
Emergency Signs and Symptoms
- ECG:
-
Electrocardiogram
- AMLS:
-
Advanced Medical Life Support
- ABCDE:
-
Airway, Breathing, Circulation, Disability and Exposure
References
Andrew E, Nehme Z, Cameron P, Smith K. Drivers of increasing emergency ambulance demand. Prehosp Emerg Care. 2020;24:385–90.
Höglund E, Andersson-Hagiwara M, Schröder A, Möller M, Ohlsson-Nevo E. Characteristics of non-conveyed patients in emergency medical services (EMS): a one-year prospective descriptive and comparative study in a region of Sweden. BMC Emerg Med. 2020;20:61.
Paulin J, Kurola J, Salanterä S, Moen H, Guragain N, Koivisto M, et al. Changing role of EMS –analyses of non-conveyed and conveyed patients in Finland. Scand J Trauma, Resusc. 2020;28:45.
Booker MJ, Shaw ARG, Purdy S. Why do patients with ‘primary care sensitive’ problems access ambulance services? A systematic mapping review of the literature. BMJ Open. 2015;5:e007726.
Paulin J, Kurola J, Koivisto M, Iirola T. EMS non-conveyance: a safe practice to decrease ED crowding or a threat to patient safety? BMC Emerg Med. 2021;21:115.
Berg LM, Ehrenberg A, Florin J, Östergren J, Discacciati A, Göransson KE. Associations between crowding and ten-day mortality among patients allocated lower triage acuity levels without need of acute hospital care on departure from the emergency department. Ann Emerg Med. 2019;74:345–56.
Alsholm L, Axelsson C, Andersson Hagiwara M, Niva M, Claesson L, Herlitz J, Magnusson C, Rosengren L, Jood K. Interrupted transport by the emergency medical service in stroke/transitory ischemic attack: A consequence of changed treatment routines in prehospital emergency care. Brain Behav. 2019;9(5):e01266. https://doi.org/10.1002/brb3.1266. Epub 2019 Apr 13.
Magnusson C, Gärskog J, Lökholm E, Stenström J, Wetter R, Axelsson C, et al. Prediction of a time-sensitive condition among patients with dizziness assessed by the emergency medical services. BMC Emerg Med. 2021;21:38.
Sjösten O, Nilsson J, Herlitz J, Axelsson C, Jiménez-Herrera M, Andersson HM. The prehospital assessment of patients with a final hospital diagnosis of sepsis: results of an observational study. Australas Emerg Care. 2019;22:187–92. https://doi.org/10.1016/j.auec.2019.02.002.
Wibring K, Lingman M, Herlitz J, Amin S, Bång A. Prehospital stratification in acute chest pain patient into high risk and low risk by emergency medical service: a prospective cohort study. BMJ Open. 2021;11:e044938.
Wibring K, Magnusson C, Axelsson C, Lundgren P, Herlitz J, Andersson HM. Towards definitions of time-sensitive conditions in prehospital care. Scand J Trauma Resusc Emerg Med. 2020;28:7. https://doi.org/10.1186/s13049-020-0706-3.
Magnusson C, Herlitz J, Axelsson C. Patient characteristics, triage utilisation, level of care, and outcomes in an unselected adult patient population seen by the emergency medical services: a prospective observational study. BMC Emerg Med. 2020;20:7.
Kaji AH, Schriger D, Green S. Looking through the retrospectoscope: reducing bias in emergency medicine chart review studies. Ann Emerg Med. 2014;64:292–8.
Lindström V, Bohm K, Kurland L. Prehospital care in Sweden. Notf Rett Med. 2015;18:107–9.
Widgren BR, Jourak M. Medical emergency triage and treatment system (METTS): a new protocol in primary triage and secondary priority decision in emergency medicine. J Emerg Med. 2011;40:623–8.
National Association of emergency medical technicians (U.S.). Advanced medical life support committee. Advanced medical life support: an assessment-based approach. Burlington: Jones & Bartlett Learning; 2017.
Hermerén G. Good research practice. Stockholm: The Swedish Research Council; 2011.
Ebben R, Vloet L, Verhofstad M, Meijer S, Groot J, van Achterberg T. Adherence to guidelines and protocols in the prehospital and emergency care setting: a systematic review. Scand. J. Trauma, Resusc. 2013;21:9.
Hagiwara M, Suserud B-O, Jonsson A, Henricson M. Exclusion of context knowledge in the development of prehospital guidelines: results produced by realistic evaluation. Scand J Trauma, Resusc. 2013;21:46.
American College of Emergency Physicians. Clinical policy: critical issues for the initial evaluation and management of patients presenting with a chief complaint of nontraumatic acute abdominal pain. Ann Emerg Med. 2000;36:406–15.
Larsson G, Holmén A, Ziegert K. Early assessment of patient’s medical condition in ambulance care affects the level of care of non-urgent patients. Stud Health Technol Inform. 2016;225:893–4.
Osterwalder I, Özkan M, Malinovska A, Nickel CH, Bingisser R. Acute abdominal pain: missed diagnoses, extra-abdominal conditions, and outcomes. J Clin Med. 2020;9:899.
Velissaris D, Karanikolas M, Pantzaris N, Kipourgos G, Bampalis V, Karanikola K, et al. Acute abdominal pain assessment in the emergency department: the experience of a Greek university hospital. J Clin Med Res. 2017;9:987–93.
Gerhardt RT, Nelson BK, Keenan S, Kernan L, MacKersie A, Lane MS. Derivation of a clinical guideline for the assessment of nonspecific abdominal pain: the guideline for abdominal pain in the ED setting (GAPEDS) phase 1 study. Am J Emerg Med. 2005;23:709–17.
James SK, Erlinge D, Herlitz J, Alfredsson J, Koul S, Fröbert O, et al. Effect of oxygen therapy on cardiovascular outcomes in relation to baseline oxygen saturation. JACC Cardiovasc Interv. 2020;13:502–13.
Hansson PO, Andersson Hagiwara M, Brink P, Herlitz J, Wireklint SB. Prehospital identification of factors associated with death during one-year follow-up after acute stroke. Brain Behav. 2018;8:e00987.
Acknowledgements
We like to thank the participant EMS organizations for kindly support in data collection.
Funding
Open access funding provided by University of Boras. No funding was received.
Author information
Authors and Affiliations
Contributions
All authors design and planed the study. PH and EO performed all data collection and analysis. MH supervised the data analysis. All authors was participated in preparation of the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Regional Ethics Committee, Stockholm, Sweden (Dnr 2021–03440). Before the journal review, approval was obtained from the operations manager in the included organisation. The project has received an approved ethics review without the informed consent of patients whose medical records have been reviewed. The motivation is that record review is a common method for healthcare organizations to measure patient safety and quality of care. The approach in this research project does not differ from the journal review that normally takes place in healthcare organizations. Persons employed in the included organization have performed the journal reviews. The study ensured strict compliance with Swedish research ethics guidelines [17].
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Larsson, G., Hansson, P., Olsson, E. et al. Prehospital assessment of patients with abdominal pain triaged to self-care at home: an observation study. BMC Emerg Med 22, 92 (2022). https://doi.org/10.1186/s12873-022-00649-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12873-022-00649-x