
Abstract
Background
Spinal cord injury (SCI) and spinal fracture are major complications in patients with ankylosing spondylitis (AS) who sustain spinal trauma. The purpose of this study was to investigate the incidence, predictors, and sequelae of spinal trauma in patients with AS.
Methods
This retrospective study included patients with AS who were admitted for spinal trauma between January 1, 2006, and June 30, 2016. The study compared clinical outcomes of patients between group 1: SCI alone, group 2: spinal fracture alone (no SCI), and group 3: both SCI and spinal fracture.
Results
Of the 6285 patients with AS admitted during the retrospective study period, only 105 suffered from spinal trauma and were enrolled in the study. Case number in group 1, 2, and 3 was 11(10.48%), 45(42.85%), and 49(46.67%), respectively. Among the patients with spinal fractures, 52.1% had SCI. Bamboo spine was significantly more prevalent in the fracture group than in the nonfracture group (78.7% vs. 36.4%; P = 0.006). Patients with SCI had more instances of subluxation or dislocation (48.3% vs. 8.9%; P < 0.001) and more cases of spinal epidural hematoma (SEH; 21.7% vs. 2.2%; P = 0.003) than patients without SCI. The rate of delayed diagnosis for spinal fracture was 31.4%, with one-third of patients developing delayed SCI. Among the patients with incomplete SCI, 58.3% achieved neurological improvement after treatment (P = 0.004).
Conclusions
Patients with AS and bamboo spine at radiograph had a higher rate of spinal fracture, which may be an important factor in SCI in patients with AS. Spinal fractures involving the C3–C7 region, subluxation or dislocation, severe spinal fracture, and SEH were found to be predictive of SCI, and SCI in patients with AS resulted in higher mortality and complication rates.
Similar content being viewed by others


Background
Ankylosing spondylitis (AS) is a chronic inflammatory disease that mainly affects the axial skeleton. AS is characterized by progressive bone loss, erosion, and syndesmophyte formation, all of which lead to progressive spinal rigidity and altered spinal biomechanics [1]. AS thus increases the risk of vertebral fractures from even minor injuries [2,3,4]. Patients with AS generally have marginal syndesmophyte formation, which presents as the classic “bamboo spine” in radiographic examinations [5]. An ankylosed spine is fragile due to the secondary osteoporosis and loss of mobility that accompany the disease [6], and the risk of fracture increases as the disease progresses over time. A severely ankylosed spine is more susceptible to injury and is relatively unstable compared with a normal spine [2, 7,8,9]. However, delayed diagnosis of spinal fractures in patients with AS after minor trauma is common. Patients with delayed diagnosis generally present with chronic pain, progressive neurologic deficits, and worsening spinal deformity [10,11,12].
Spinal trauma includes spinal cord injury (SCI), spinal fracture, or both.[1, 4, 11, 13, 14] Spinal trauma in the ankylosed spine greatly affects morbidity and mortality [3, 11, 13]. The mean prevalence of AS per 10,000 people has been found to be 23.8 in Europe, 16.7 in Asia, 31.9 in North America, 10.2 in Latin America, and 7.4 in Africa [15]. The reported prevalence of spinal fracture in patients with AS varied greatly between Europe and North America, with prevalences of 10% and 17%, respectively [6, 8, 16, 17], and rates of SCI of 19% and 91%, respectively [4, 11, 16, 18, 19]. Because AS is an uncommon disease, data on the predictors of this condition are scarce [4, 13], especially in Asia. The purpose of this study was to investigate the incidence, predictors, and sequelae of spinal trauma in patients with AS at a single tertiary center in Asia.
Material and methods
Patient sample
Between January 1, 2006, and June 30, 2016, 6285 patients were treated for spinal fractures or SCI following a spinal injury at our institution. Of the 6285, only 110 patients with AS with spinal trauma were identified. The patients’ charts and images were reviewed by 3 experienced neurosurgeons. A rheumatologist confirmed the diagnosis of AS based on the criteria of the Assessment of Spondyloarthritis International Society [20,21,22,23], and 105 patients who had a minimum 2-year follow-up or who died over the course of follow-up were included. This study excluded 4 patients who had a follow-up of less than 1 year and 1 patient for whom key image data were missing. This study was approved by the institution’s institutional review board (IRB No.: 201700858B0).
Variables
Predefined and generally accepted parameters (listed in Table 1) were used to extract data from electronic medical records, including patient age at the time of injury, patient sex, the initial neurological grading on the American Spinal Injury Association Impairment Scale (AIS), the presence of high-energy trauma [24], the presence of bamboo spine, the presence of subluxation or dislocation, the presence and level of SCI, the presence and level of spinal fracture, the presence and level of spinal epidural hematoma (SEH), the fracture classification, the treatment administered, the outcome at discharge and 2 years after trauma, and the presence and type of complications.
Outcome measures
The degree of SCI was manually graded for each patient according to the AIS at the time of the initial SCI diagnosis, at the time of discharge, and at the 2-year follow-up. Patients with a decline in AIS grade of 1 or more (such as a decline from E to D) at any point after injury were considered patients with SCI. We categorized SCI as either complete (AIS grade A) or incomplete (AIS grades B–D). Patients with SCI who demonstrated an improvement of at least 1 AIS grade (such as from D to E) during follow-up were considered neurologically improved.
Statistical methods
Data were presented as frequency and percentage for continuous variables and as mean and standard deviation for categorical variables. The patients included in the study were divided into 3 groups (group 1: SCI alone, group 2: spinal fracture alone (no SCI), and group 3: both SCI and spinal fracture). The characteristics of patients among the groups were compared using one-way analysis of variance for continuous variables or Fisher’s exact test for categorical variables. The improvement in AIS grade from the time of the first symptoms to the last follow-up in the patients with SCI was tested using the McNemar test. All tests were 2-tailed, and P < 0.05 was considered statistically significant. No adjustment for multiple testing (multiplicity) was made in this study. Data analyses were conducted using SPSS 25 (IBM SPSS, Chicago, Illinois).
Results
Of the 105 patients included in the study, 11 patients (10.48%) were in group 1, 45 patients (42.85%) in group 2 (Fig. 1), and 49 (46.67%) in group 3 (Fig. 2). A small percentage of the patients were female (4.8%; 5/105). Fifty-three patients (50.5%) had low-energy trauma alone, 33 (31.4%) had subluxation or dislocation, and 94 (89.5%) had spinal fractures. Spinal fracture involving the C3–C7 region occurred most frequently in patients with both SCI and spinal fracture (65.3%), whereas the thoracic spine was the most frequently fractured region in patients without SCI (44.4%). Of the 105 patients, 60 (57.1%) had SCI, including 12 with complete SCI. Of the 12 cases of complete SCI, C3–7 SCI accounted for 43.8%. Forty-nine patients (52.1%) had both SCI and spinal fracture, and 78 patients (74.3%) presented with bamboo spine in X-ray images (Table 2).

Demonstration of a patient in group 2 (spinal fracture alone). A 63-year-old man with AS presented to the hospital after a falling down accident, without neurological deficit (ASIA Grade E). CT showed a Type B2 fracture (A) and the fracture with mild displacement of T11 vertebral body and the fracture line involving and left pedicle (B). The patient underwent internal fixation as schedule

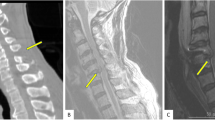
Demonstration of a patient in group 3 (both spinal fracture and cord injury). A 52-year-old man with AS presented to the hospital after a high-energy trauma, with neurological deficit (ASIA Grade A). CT showed a Type B3 fracture (A) and the fracture involving C5–6 and left facet (B). cervical MRI showed severe cord compression with cord edema (C.D). The patient underwent reduction, internal fixation and decompression immediately
Delayed diagnosis was made in 33 patients (31.4%). Among these patients, all had spinal fracture; 6 of the patients were placed in the “doctor delay” group. Two of the 6 patients developed SCI at 5 days, and another 2 of the 6 developed SCI at 15 days after the trauma. The remaining 27 patients were placed in the “patient delay” group; 9 of the patients developed delayed SCI within 2 to 90 days after the trauma. The average time between trauma and a confirmed diagnosis for all the patients was 19.8 days (SD = 20.4 days), with a range of 2 to 90 days (Table 2).
Of the 105 patients in this study, 32 received surgical treatment for spinal fracture alone at 13 ± 93.7 days after trauma, and 45 patients received surgical treatment for SCI that consisted of decompression, open reduction, and fixation at 1.8 ± 3.2 days. Of the patients with both SCI and spinal fracture, 6, including 3 patients with AIS grade A, received closed reduction and halo-jacket fixation; 3 patients with mild SCI (initial AIS grade: D) with mild spinal fracture (AO spine fracture classification: A) received conservative treatment. Thirteen patients with mild spinal fractures (AO spine fracture classification: A) without SCI received conservative treatment. Of the 11 patients with SCI alone, 10 were cases of central cord syndrome, and they achieved recovery to AIS grade E; 1 case was a severe head injury with consciousness no recovery to clear. One, 4, 2, 3, and 1 injuries occurred at C3, C4, C5, C6, and C7, respectively. Anterior microdiscectomy with interbody fusion and fixation was performed in 2 cases; the 8 patients with mild SCI (initial AIS grade: D) and the 1 who initially presented with a deep coma received conservative treatment.
SEH was observed in 14 patients (13.3%). Over the course of follow-up, 32 patients (30.5%) experienced complications, with infection being the most common (22.9%). Four patients (3.8%) died during the 2-year follow-up period; 3 of these deaths were due to pneumonia-related septic shock, and 1 was due to pulmonary embolism and cardiac failure with acute respiratory distress syndrome (Table 2).
Among the SCI patients, the AIS grade significantly improved from the time of the first symptoms to the follow-up at 2 years (P = 0.004). Among all 60 patients with SCI, 35 achieved an improvement in AIS grade. However, the AIS grades in 4 patients worsened due to the patients who died (n = 4) having been given an AIS grade A at the 2-year follow-up (Table 3). Excluding patients with mild SCI (initial AIS grade: D) who did not undergo surgery, 53.3% of the 45 patients who received surgical treatment experienced long-term neurological recovery.
For patients with and without spinal fracture, bamboo spine appeared significantly more frequently in the fracture group (78.7% vs. 36.4%; P = 0.006). Demographic and clinical characteristics were not significantly different, however, between the fracture and nonfracture groups or between the SCI and non-SCI groups. The results revealed that compared with the non-SCI group, more cases involving subluxation or dislocation (48.3% vs. 8.9%; P < 0.001), spinal fractures involving the C3–C7 region (53.3% vs. 11.1%; P < 0.001), spinal fracture in general (P < 0.001), and SEH occurred in the SCI group (21.7% vs. 2.2%; P = 0.003; Table 4).
Discussion
Among patients with AS, SCI is a major complication regardless of spinal fracture occurrence. Our results revealed that the SCI rate after spinal trauma in patients with AS was 57.1% (60/105) and the SCI rate in cases also involving spinal fractures was 52.1% (49/94), which are similar to the rates in Europe and North America, which range from 19.7% to 67.2% [3, 4, 11, 13, 14, 18]. Variation in the rate of SCI after spinal fractures in patients with AS may be due to differences in medical referral standards, severity of trauma, and severity of AS.
Diagnoses of fractures in patients with AS are frequently delayed at a rate of 17.1% to 65.4%[2, 4, 11, 14] due to the frequent presence of chronic pain in patients with AS, even in the absence of trauma. Therefore, aggravating pain following minor trauma may be overlooked. Due to alterations in bone density resulting from AS, radiological assessment of fracture in patients with AS can be difficult, with fractures difficult to identify and easily misinterpreted, especially in cases involving fractures at the thoracic spine and thoracolumbar junction. In our study, the rate of delayed diagnosis of spinal fracture was 31.4% (33/105), with 69.7% (23/33) of those cases involving fractures between the T8 and L1 vertebrae. Delay in 6 of the 33 cases was attributed to oversight by a doctor, and delay in the remaining cases was due to patients delaying visits. Oversight may put patients with AS at higher risk of delayed SCI. In our study, one-third of the 33 patients with a delayed diagnosis of spinal fracture developed delayed SCI. Within the initial posttrauma period, 90.9% of these patients had axial pain, such as neck or back pain, and 33.3% had limb numbness. Attending physicians should remain aware of the consequences of delayed diagnosis in patients with AS, even in cases of low-energy trauma. We suggest routine radiographic examination for all patients with AS after trauma and additional computed tomography imaging if axial pain progresses. Magnetic resonance imaging is a viable option for assessing spinal cord injuries and for detecting potential occult fractures [12, 29,30,31].
Bamboo spine is a radiographic feature in AS that occurs as a result of vertebral body fusion by marginal syndesmophytes. The resulting radiographic appearance is of radiopaque spicules that completely bridge the adjoining vertebral bodies. In our study, 74.3% (78/105) of patients with AS exhibited this feature. We also observed that the patients with bamboo spine had a higher rate of spinal fracture than those without bamboo spine (P = 0.006; Table 4). However, the results revealed no significant correlation between bamboo spine and SCI (P = 0.367; Table 4). This contradicted our finding that AS with spinal fracture was significantly related to SCI (P < 0.001). To clarify this discrepancy, we analyzed the relationship between bamboo spine and spinal fracture in the 60 patients with SCI. Four of the 11 patients who had SCI without spinal fracture presented with bamboo spine, and 43 of the 49 patients with both SCI and spinal fracture had bamboo spine. A comparison of these 2 groups revealed a significant difference (P = 0.001; Table 2). Patients with noncomplex compression fractures with intact posterior ligamentous complex (PLC) (AOSpine—Spine Trauma Classification System type A) [32] had a lower rate of SCI than those with complex fractures, which include tension band injuries in cervical spine, and distraction injuries in thoracolumbar spine (type B), or translation injuries (type C) (P < 0.001). Subluxation or dislocation was also a risk factor for patients with AS developing SCI (P < 0.001). The severity of disruption to the spinal structure is, thus, predictive of SCI in patients with AS. In cases involving a complex fracture, SCI is not only caused by the damage from direct impact but also by further compression from bone fragments, hematoma, or disk material [33]. Therefore, we hypothesize that patients with AS with bamboo spine have a high probability of experiencing spinal fracture. Mild fractures, however, do not necessarily cause SCI in patients with AS.
No universal guidelines have been developed for the management of spinal trauma in patients with AS [31]. Nonoperative treatment, including bed rest, skeletal traction, bracing, or immobilization with a halo-vest, has long been recommended for nondisplaced or minimally displaced fractures of ankylosed spines [31, 34, 35]. However, the inherent instability of these fractures and their high potential for acute displacement may cause severe damage [36]. Therefore, surgical fixation with long segmental instrumentation combined with fusion is recommended [36]. Furthermore, the compression of neurological elements often requires surgical evacuation. Recent studies have demonstrated a trend of higher complication rates in nonoperative patients—for instance, finding higher rates of pulmonary complications and a risk of neurological deterioration [3, 4, 35]. Surgical stabilization usually includes anterior, posterior, or combined fixation, often accompanied by decompression with laminectomy and several osteotomy techniques for deformity correction [37, 38]. In our study, 3 patients with an initial AIS grade A received closed reduction and halo-jacket fixation, and all 3 patients (100%) experienced complications: 1 patient experienced screw loosening and 2 developed pneumonia. By contrast, 7 of 9 patients (77.8%) with an initial AIS grade A experienced complications after surgery, suggesting a trend of lower complication rates in severe SCI.
All 14 patients with SEH developed SCI; SCI thus became a key predictive factor for SCI (P = 0.003). SEH occurred in 13.3% of the patients with AS, which is a much higher rate than that of the general population (range: 0.5% to 7.5%) [39, 40]. Compared with fractures that cause SCI immediately, SEH may lead to subacute SCI hours after trauma. The mechanisms underpinning cervical SEH formation are not fully understood; disruption of the posterior longitudinal ligament and spinal epidural vessel rupture, however, may play a vital role [25, 40]. Symptomatic SEH is generally considered a neurosurgical emergency. In the general population, better long-term neurological recovery has been noted after early surgical intervention. However, no major case study has reported the effects of early surgical intervention in patients with AS. In our study, the patients with SCI received surgical treatment 1.8 ± 3.2 days after trauma. Several of these patients had delayed surgical treatment due to delayed diagnosis, old age, comorbidity, or polytrauma that required additional treatments.
None of the patients who had complete SCI at admission exhibited improvement in AIS grade after 2 years. By contrast, 58.3% (35/60) of patients in the incomplete SCI group demonstrated improvement. Overall, patients with AS with incomplete SCI had better long-term neurological recovery. Complication rates were significantly higher (P = 0.001) in patients with SCI. The 4 patients who died within 1 year were significantly older (with an average age of 69.2 years). This echoes previous findings of higher mortality in older patients with AS after spinal fracture [11, 13]. Of the patients with AS with different complexities of fracture and varying degrees of SCI in our study, more than 53% of patients achieved long-term neurological recovery after surgical treatment.
Limitation
This is a single-center study thus obviating patient selection bias. Besides, most subjects achieved long-term follow-up. Meanwhile, this study was limited for its retrospective design, as well as the non-feasibility of analysis on cervical, thoracic and lumbar cohorts separately due to insufficient case number. Thus, further well-designed prospective randomized studies are needed.
Conclusions
SCI is a major complication of spinal trauma in patients with AS. After spinal trauma, patients with AS with bamboo spine have relatively high rates of spinal fracture. Cervical fracture involving the C3–C7 region, subluxation or dislocation, high severity, and SEH are predictive of SCI. In patients with AS, even low-energy trauma has the potential to cause spinal trauma, including SCI or fracture. Although the prevalence of AS differs across continents, the rate and predictors of SCI after spinal trauma in AS exhibit no obvious differences. Delayed diagnosis of fracture and SCI occur in approximately 30% and 10% of cases of spinal trauma, respectively. Therefore, attending physicians should be aware of their potential effects on patients with AS.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SCI:
-
Spinal cord injury
- AS:
-
Ankylosing spondylitis
- SEH:
-
Spinal epidural hematoma
- ASAS:
-
Assessment of Spondyloarthritis International Society
- AIS:
-
American Spinal Injury Association Impairment Scale
References
Bot SD, Caspers M, Van Royen BJ, Toussaint HM, Kingma I. Biomechanical analysis of posture in patients with spinal kyphosis due to ankylosing spondylitis: a pilot study. Rheumatology (Oxford). 1999;38(5):441–3.
Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999;37(6):444–7.
Jacobs WB, Fehlings MG. Ankylosing spondylitis and spinal cord injury: origin, incidence, management, and avoidance. Neurosurg Focus. 2008;24(1):E12.
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and complications. Eur Spine J. 2009;18(2):145–56.
Whang PG, Goldberg G, Lawrence JP, Hong J, Harrop JS, Anderson DG, Albert TJ, Vaccaro AR. The management of spinal injuries in patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis: a comparison of treatment methods and clinical outcomes. J Spinal Disord Tech. 2009;22(2):77–85.
Donnelly S, Doyle DV, Denton A, Rolfe I, McCloskey EV, Spector TD. Bone mineral density and vertebral compression fracture rates in ankylosing spondylitis. Ann Rheum Dis. 1994;53(2):117–21.
Feldtkeller E, Vosse D, Geusens P, van der Linden S. Prevalence and annual incidence of vertebral fractures in patients with ankylosing spondylitis. Rheumatol Int. 2006;26(3):234–9.
Cooper C, Carbone L, Michet CJ, Atkinson EJ, O’Fallon WM, Melton LJ 3rd. Fracture risk in patients with ankylosing spondylitis: a population based study. J Rheumatol. 1994;21(10):1877–82.
Chaudhary SB, Hullinger H, Vives MJ. Management of acute spinal fractures in ankylosing spondylitis. ISRN Rheumatol. 2011;2011:150484.
Thumbikat P, Hariharan RP, Ravichandran G, McClelland MR, Mathew KM. Spinal cord injury in patients with ankylosing spondylitis: a 10-year review. Spine (Phila Pa 1976). 2007;32(26):2989–95.
Schiefer TK, Milligan BD, Bracken CD, Jacob JT, Krauss WE, Pichelmann MA, Clarke MJ. In-hospital neurologic deterioration following fractures of the ankylosed spine: a single-institution experience. World Neurosurg. 2015;83(5):775–83.
Anwar F, Al-Khayer A, Joseph G, Fraser MH, Jigajinni MV, Allan DB. Delayed presentation and diagnosis of cervical spine injuries in long-standing ankylosing spondylitis. Eur Spine J. 2011;20(3):403–7.
Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010;35(11):E458-464.
Teunissen FR, Verbeek BM, Cha TD, Schwab JH. Spinal cord injury after traumatic spine fracture in patients with ankylosing spinal disorders. J Neurosurg Spine. 2017;27(6):709–16.
Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ. Global prevalence of ankylosing spondylitis. Rheumatology (Oxford). 2014;53(4):650–7.
Vosse D, Feldtkeller E, Erlendsson J, Geusens P, van der Linden S. Clinical vertebral fractures in patients with ankylosing spondylitis. J Rheumatol. 2004;31(10):1981–5.
Hunter T, Dubo HI. Spinal fractures complicating ankylosing spondylitis. A long-term followup study Arthritis Rheum. 1983;26(6):751–9.
Lukasiewicz AM, Bohl DD, Varthi AG, Basques BA, Webb ML, Samuel AM, Grauer JN. Spinal fracture in patients with ankylosing spondylitis: cohort definition, distribution of injuries, and hospital outcomes. Spine (Phila Pa 1976). 2016;41(3):191–6.
Einsiedel T, Schmelz A, Arand M, Wilke HJ, Gebhard F, Hartwig E, Kramer M, Neugebauer R, Kinzl L, Schultheiss M. Injuries of the cervical spine in patients with ankylosing spondylitis: experience at two trauma centers. J Neurosurg Spine. 2006;5(1):33–45.
Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369(9570):1379–90.
Dillon CF, Hirsch R. The United States National Health and Nutrition Examination Survey and the epidemiology of ankylosing spondylitis. Am J Med Sci. 2011;341(4):281–3.
Reveille JD. Epidemiology of spondyloarthritis in North America. Am J Med Sci. 2011;341(4):284–6.
Rudwaleit M, van der Heijde D, Landewe R, Listing J, Akkoc N, Brandt J, Braun J, Chou CT, Collantes-Estevez E, Dougados M, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009;68(6):777–83.
Sulter G, Steen C, De Keyser J. Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke. 1999;30(8):1538–41.
Garza-Mercado R. Traumatic extradural hematoma of the cervical spine. Neurosurgery. 1989;24(3):410–4.
Chicago IACoS. American College of Surgeons. Advanced trauma life support for doctors, student course manual. 1997.
Levine AM, Edwards CC. Fractures of the atlas. J Bone Joint Surg Am. 1991;73(5):680–91.
Anderson LD, D’Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974;56(8):1663–74.
Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005;30(14):E417-419.
Tavolaro C, Ghaffar S, Zhou H, Nguyen QT, Bellabarba C, Bransford RJ. Is routine MRI of the spine necessary in trauma patients with ankylosing spinal disorders or is a CT scan sufficient? Spine J. 2019;19(8):1331–9.
Leone A, Marino M, Dell’Atti C, Zecchi V, Magarelli N, Colosimo C. Spinal fractures in patients with ankylosing spondylitis. Rheumatol Int. 2016;36(10):1335–46.
Divi SN, Schroeder GD, Oner FC, Kandziora F, Schnake KJ, Dvorak MF, Benneker LM, Chapman JR, Vaccaro AR. AOSpine-Spine Trauma Classification System: The Value of Modifiers: A Narrative Review With Commentary on Evolving Descriptive Principles. Global Spine J. 2019;9(1 Suppl):77S-88S.
Volarevic V, Erceg S, Bhattacharya SS, Stojkovic P, Horner P, Stojkovic M. Stem cell-based therapy for spinal cord injury. Cell Transplant. 2013;22(8):1309–23.
Graham B, Van Peteghem PK. Fractures of the spine in ankylosing spondylitis. Diagnosis, treatment, and complications. Spine (Phila Pa 1976). 1989;14(8):803–7.
Kouyoumdjian P, Guerin P, Schaelderle C, Asencio G, Gille O. Fracture of the lower cervical spine in patients with ankylosing spondylitis: Retrospective study of 19 cases. Orthop Traumatol Surg Res. 2012;98(5):543–51.
Fox MW, Onofrio BM, Kilgore JE. Neurological complications of ankylosing spondylitis. J Neurosurg. 1993;78(6):871–8.
Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002;97(2 Suppl):218–22.
Taggard DA, Traynelis VC. Management of cervical spinal fractures in ankylosing spondylitis with posterior fixation. Spine (Phila Pa 1976). 2000;25(16):2035–9.
Pan G, Kulkarni M, MacDougall DJ, Miner ME. Traumatic epidural hematoma of the cervical spine: diagnosis with magnetic resonance imaging. Case report J Neurosurg. 1988;68(5):798–801.
Lin TC, Liu ZH, Bowes AL, Lee ST, Tu PH. Effective Steroid Treatment in Traumatic Cervical Spinal Epidural Hematoma Presenting with Delayed Tetraparesis: Two Case Reports and Literature Review. World Neurosurg. 2016;91(673):e675-679.
Acknowledgements
The authors thank Chen-Ying Liu for assisting in the surgical procedures. We also acknowledge Wallace Academic Editing Services Co. for editing the manuscript.
Funding
This work was not supported by any grants.
Author information
Authors and Affiliations
Contributions
PH performed the conception and design of the study, analysis and Interpretation of data, grant funder, and drafting the article. ZH contributed to the design of the study, acquisition of data, analysis and interpretation of data, critically revising the article, approved the final version of the manuscript. MC contributed to the interpretation of data, drafting the article, and study supervision. YT contributed to the acquisition and analysis of data, technical and material support of procedures. YCL analyzed, interpreted, and reviews the images. YCH contributed to the acquisition of data and technical support of procedures. TM contributed to the acquisition of data and technical support of procedures. CC critically revised the article, approved the final version of the manuscript, statistical analysis, and study supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained in writing from every patient after a detailed consultation, during which the risks and benefits of the procedures and alternatives were delineated. The database of all patients and procedures was retrospectively reviewed to identify the patients, and the study was approved by our institute’s institutional review board (IRB No.: 201700858B0).
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
All authors certify that there is no actual or potential conflict of interest in relation to this article, and there are no financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tu, PH., Liu, ZH., Yeap, MC. et al. Spinal cord injury and spinal fracture in patients with ankylosing spondylitis. BMC Emerg Med 22, 73 (2022). https://doi.org/10.1186/s12873-022-00635-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12873-022-00635-3