
Abstract
Background
Postpartum hemorrhage (PPH) is a serious obstetric emergency, and one of the top five causes of maternal mortality globally. The most common causes of PPH include uterine atony, placental disorders, birth trauma and coagulation defects. Timely diagnosis and early management are critical to reduce morbidity, the need for blood transfusion or even mortality. External, manual aortic compression (AC) has been suggested as an intervention that reduce PPH and extend time for control of bleeding or resuscitation. This procedure is not commonly utilized by healthcare personnel. The incidence of home-births is increasing, and competence in PPH assessment and management is essential in prehospital personnel. The objective was to explore prehospital personnel’s competence in PPH and AC, utilizing different tools.
Methods
The study was conducted in a county in South-eastern Norway, including five ambulance stations. All prehospital personnel (n = 250) were invited to participate in a questionnaire study. The questionnaire included the PPH self-efficacy (PPHSE) and PPH collective efficacy (PPHCE) tools, as well as tool developed utilizing the Delphi technique. Descriptive statistics were used to analyze the quantitative data, while quantitative content analysis was used to analyse free-text responses.
Results
A total of 87 prehospital personnel responded to the questionnaire, 57.5% male, mean age 37.9 years. In total, 80.4% were ambulance workers and/or paramedics, and 96.6 and 97.7% respectively reported to need more education or training in PPH. Moreover, 82.8% reported having managed patient(s) with PPH, but only 2.9% had performed AC. Prehospital personnels’ responses varied extensively regarding knowledge about what PPH is, how to estimate and handle PPH, and how to perform AC. Mean self-efficacy varied from 3.3 to 5.6, while collective efficacy varied from 1.9 to 3.8.
Conclusions
This study indicates that prehospital personnel lack knowledge about PPH and AC, due to various responses to the developed questionnaire. Even though AC is an acknowledged intervention in PPH, few participants reported that this was utilized. Our findings emphasize the need for education and training in PPH and PPH handling generally, and in AC specifically.
Similar content being viewed by others


Background
Postpartum hemorrhage (PPH) is a serious obstetric emergency, and one of the top five causes of maternal mortality globally [1]. Internationally, the prevalence of severe PPH appears to be rising, with increasing morbidity and need for transfusion therapy, and the mortality rates are high in low-income countries [2,3,4,5,6]. Maternal mortality rates (MMR) in the Nordic countries are among the lowest in the world, but women still die from complications of pregnancy or birth. In Norway, 168 maternal deaths were identified between 2005 and 2013 (Maternal Mortality Rate, MMR, 6.6 per 100,000), of whom 14 died due to severe PPH [7].
The incidence of PPH has been reported to vary between one to 5 %, depending upon the diagnostic criteria applied [2]. Although PPH is traditionally defined by the volume of blood loss observed, bleeding may not be visible externally or the blood may be mixed with amniotic fluid [4]. In 2017, the American College of Obstetricians and Gynecologists revised their definition of PPH to consist of the following criteria:
-
1.
Cumulative blood loss ≥1000 ml or
-
2.
Bleeding associated with signs or symptoms of hypovolemia within 24 h of the birth process, regardless of the route of delivery [8]
The most common causes of PPH include uterine atony, placental disorders, birth trauma and coagulation defects [9].
Timely diagnosis, appropriate resources and early management are critical to prevent death [9]. According to the World Health Organization, immediate solutions are needed to prevent women from dying of PPH [1]. Maternal mortality reviews have demonstrated that deaths caused by PPH are most likely to be preventable [10, 11]. The consistent application of a comprehensive protocol for management of PPH have been demonstrated to result in improved outcomes [12, 13]. Other potential interventions include tranexamic acid, fluid resuscitation, removal of the placenta, bimanual uterine compression, uterotonics, suturing of lower genital tract injury, blood product replacement, balloon tamponade, laparotomy, stepwise uterine de-vascularization, uterine compression sutures and hysterectomy. Emergency temporizing measures include application of the non-pneumatic anti-shock garment, uterine tourniquet application and aortic compression [14].
External, manual aortic compression (AC) is an emergency manoeuvre proposed to reduce postpartum haemorrhage and extend time for resuscitation and control of bleeding. The technique can be applied immediately to reduce bleeding from the uterus by reducing the blood supply. This again may prevent cardiac arrest from hypovolemia, and allow transfer to definitive care in-hospital. The Swedish obstetrician Bergstrom has been teaching this life-saving technique for many years in African countries, with great effect on maternal morbidity and mortality [15]. Nevertheless, in many countries, including Norway, manual AC is not actively used by healthcare personnel [16].
There is an increasing incidence of home births in Norway, as in Nordic countries [17, 18]. Hence, knowledge of PPH on competence in handling this condition is essential in prehospital personnel. Consequently, as researchers, healthcare personnel educators, nurse anesthetist and paramedic, our objective was to explore prehospital personnel’s knowledge about and self-assessed competence in PPH and AC, their experience with this condition, perceived need for more education and/or training, as well as their perceived self-efficacy and collective efficacy in PPH assessment and management.
Methods
The study had a cross-sectional design, utilizing a questionnaire to assess prehospital personnel’s knowledge, self-assessed competence, self-efficacy and team-efficacy. The study adheres to the STROBE (Strengthening the reporting of observational studies in epidemiology) guidelines (see additional file 1).
Setting and participants
The study was conducted in a county with approximately 317,000 inhabitants, within one hospital catchment area. There are five ambulance stations in this area. Prehospital personnel include ambulance assistants, ambulance workers (upper high school), bachelor in paramedicine or – nursing (180 European Credit Transfer and Accumulation System,
ECTs), and paramedics (further education, 60 ECTs). Utilizing a strategic sampling method, all prehospital personnel (n = 250) were invited to participate.
Questionnaire
The questionnaire consisted of three parts:
-
1)
a validated questionnaire in PPH self-efficacy (PPHSE) as well as PPH collective efficacy (PPHCE) [19]. The PPHSE includes eight items, using a continuous scale from 1 (never) to 8 (always). The items on self-efficacy focus on individual perception of control. The PPHCE includes 13 items (same scoring format as the PPHSE). In the current study, collective efficacy was defined as team-efficacy in the prehospital team, most commonly consisting of two healthcare personnel (see additional file 2.
-
2)
a questionnaire developed as part of this study (see additional file 3)
In this study, the Cronbach’s alpha was 0.89 on the PPHSE scale, and 0.96 on the PPHCE, which is assumed excellent.
Development of the questionnaire
Since no validated questionnaire to measure knowledge and self-assessed competence in PPH handling could be identified, we developed a questionnaire. Here, we used recommendations from the Delphi technique, which is suitable to obtain expert opinions in a systematic manner, and includes four steps: 1) expert input, 2) interaction with feedback, 3) statistical group responses, and 4) confidentiality [20, 21].
Experts were defined as specialists in their field, and included six anesthesiologists, three obstetricians and two midwives, knowledgeable in the field of obstetrics and obstetric anesthesia and recommended by other experts, four of them with prehospital experience [22]. The expert group consisted of four males, seven females, mean age was 53 years, and mean years of experience 15. In step 1 and 2, the expert group participated in the development of questions, and gave constructive inputs on clarity, wording, and contents of the whole questionnaire, as suggested by Streiner & Norman [23]. In these steps, experts received the questionnaire in two or three rounds depending on their inputs. In step 3, experts were asked to score the questionnaire regarding relevance, clarity and logic, on a scale from 1 = strongly disagree, to 5 = strongly agree. Table 1 presents the mean and range of responses to these scorings.
The experts were involved in several rounds until consensus was reached. The final version of the questionnaire consisted of a) 13 knowledge questions with free-text answers, and two questions with alternatives yes/no/undecided, b) two questions about perceived need for more education and/or simulation, and c) five questions about experience with PPH and the use of AC.
Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS 26.0) [24]. The descriptive statistics frequency, mean and Standard Deviation (SD) were used to analyse data. Internal consistency for the scales was tested by Cronbach’s alpha. There were no missing items in the validated questionnaires. The free-text responses were analyzed through a quantitative content analysis, reading through the responses and searching for similarities and code-words repeated throughout [25].
Results
A total of 87 prehospital healthcare personnel (34.8%) responded to the questionnaire. Table 2 gives an overview of respondents’ gender, age, educational background and years of experience.
Responses to the developed questionnaire
Knowledge about PPH
On the question “How much is normal hemorrhage during birth, and when is it defined as postpartum hemorrhage?” most of the respondents assumed a hemorrhage of up to 500 ml as normal per-partum. Hemorrhage above 500 ml was interpreted as postpartum hemorrhage by 37 of the respondents. Other answers were ‘above 1 litre’ (n = 17), ‘2 l’ (n = 3), ‘1.5 l’ (n = 1) and ‘3–4 l’ (n = 1). The rest were undecided.
Regarding the question “How do you estimate the amount of hemorrhage during/after birth?” 39 respondents found this ‘difficult’. A total of 18 respondents reported to assess the sheets or diapers, how often they needed to be changed, or even to weigh them. In addition, 21 of the respondents reported to assess the patients´ vital parameters or level of consciousness.
Knowledge about interventions
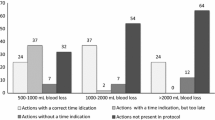
Table 3 gives an overview of responses to the questions “Which interventions should be initiated in postpartum hemorrhage?” and “When you observe a life threatening hemorrhage, what do you do first?».
Other suggestions interventions were ‘add pressure on the inguinal aorta’, ‘analgesia’, ‘tranexamacid’, ‘comfort the mother’, ‘compression’, ‘early warning to the hospital’.
Other “Clinical situations than postpartum hemorrhage where manual aortic compression can be lifesaving» reported were ‘hemorrhage in the lower extremities” (n = 7), ‘abdominal aorta aneurism’ (AAA) (n = 7), ‘other vaginal hemorrhage’ (n = 6), amputations (n = 4), other causes of massive hemorrhage such as extrauterine pregnancy (n = 2), and open wounds (n = 2).
Whether the ambulance had any drugs for use in situations of postpartum hemorrhage, most respondents reported ‘no’ (82.8%), while 11.5% were undecided, and 5.7% of the respondents reported ‘yes’. Drug reported accessible was oxytocin, and side-effects of this drug was reported to be ‘high blood-pressure’ (n = 1), and ‘nausea and vomiting’ (n = 1).
To the question “When is manual aortic compression (using a fist on aorta) appropriate?”, responses were ‘in massive hemorrhage’ (n = 32), ‘in PPH’ (n = 13), ‘in life-threatening hemorrhage’ (n = 5), ‘when the child is delivered’(n = 2), ‘when uterus massage does not have an effect’ (n = 2), and ‘AAA’(n = 1) (non-response, n = 32).
Contra-indications to AC reported were ‘limited hemorrhage’ (n = 28), ‘child not delivered’ (n = 6), ‘pain’(n = 1), and ‘patient awake’ (n = 1) (non-response, n = 51).
Knowledge about performance of AC
When asked «How would you provide manual aortic compression?» 12 of the respondents reported ‘establish pulse in arteria femoralis, add pressure above the uterus until absence of pulse’. And 20 respondents reported to ‘add pressure on the abdomen’, but location of pressure varied from ‘under the diaphragm’, ‘umbilical area’, or ‘in the middle’. Ten respondents answered ‘add pressure on the aorta’, four respondents reported ‘add pressure both from the inside and outside’, and three ‘add vaginal pressure’.
When asked what the purpose of AC is, 71 respondents reported ‘to stop the hemorrhage’. On the question “How do you assess whether the maneuver is conducted correct?”, 35 responded ‘when the hemorrhage stops’, and 18 responded ‘when the pulse in arteria femoralis is absent’. Regarding considerations during drug administration and ongoing AC, five respondents reported ‘side-effects’, and one reported ‘that drugs are not transported beyond the location of pressure’. A total of 82.8% of the respondents reported ‘no’, 11.5% reported ‘undecided’ and 5.7% reported ‘yes’, to the question about whether there are potential complications related to AC. Suggested complications were ‘damage due to ischemia’ (n = 4), ‘reduced blood pressure’(n = 3), ‘damage to inner organs’(n = 1), and ‘pain’ (n = 1).
No relation between educational background and level of knowledge could be identified.
Need for education and/or training
When asked “Do you want more education in handling postpartum hemorrhage?”, 96.6% responded ‘yes’, 1.1% responded ‘no’, and 2.3% responded ‘undecided’.
Among the respondents, 97.7% answered ‘yes’ that they want more training/simulation in handling postpartum hemorrhage.
Participants that responded ‘no’ or ‘undecided’ that they needed more education or training were all assistants or ambulance workers.
Experience
Prehospital personnel’s experience with PPH and AC is shown in Table 4.
Reasons for not using AC were ‘lack of education’ (74.7%), ‘lack of training’ (10.3%), ‘feel unsecure on the procedure’ (10.3%), and ‘difficult to cause the patient pain’ (4.6%) (fixed response alternatives).
Self-efficacy in PPH
Table 5 gives an overview of the responses to the PPH self-efficacy questionnaire (PPHSE).
Table 6 gives an overview of the responses to the PPH collective efficacy questionnaire (PPHCE).
Discussion
Our findings indicate that prehospital personnel lack knowledge about postpartum hemorrhage (PPH) and manual aortic compression (AC). As much as 82.8% had experienced PPH, but only 2.3% had utilized AC. Participants scored lower on self-efficacy than on collective efficacy in PPH handling. 96.6 and 97.7% respectively reported a need for more education or training in PPH/PPH handling.
Our findings enlighten the knowledge gap in prehospital personnel regarding PPH and AC. This indicates a need to include this topic in educational programs regardless of educational level. Studies have indicated a need to develop and implement robust clinical research regarding treatment of PPH, to establish an international knowledge platform [26]. Senthiles et al. [27] emphasize a need to reach a broad consensus about the most efficient interventions to prevent and treat PPH. This include PPH prevention initiatives, estimation of blood loss, when and which uterotonica to administer, and use of blood products. Nevertheless, consensus has been reached regarding the main steps for the initial management of PPH: manual exploration of the uterus, visual assessment of genital tract, bladder indwelling catheter, measures to maintain maternal temperature, supplemental oxygen, uterine massage, maintenance of venous access, infusion of crystalloids rather than colloids, continuous monitoring of pulse, blood pressure and respiratory rate, and use of a uterotonic [27].
The participants’ self-efficacy was scored lowest on the items «I have experienced being able to act in situations with PPH” (mean score 2.6, SD = 1.5) and “I am confident in how to treat PPH” (mean score 3.5, SD = 2.6), while the highest score was on the item “I remain calm when handling PPH” (mean score 5.5, SD = 2.1). In contrast, the mean score on the item “I am able to stay calm in emergency situations” was 4.1 (SD 2.2). This may indicate that prehospital personnel feel self-efficient when handling more stable PPH-patients, but not in emergency PPH. Prehospital personnel is used to handling acute and unpredictable situations, hence this question has to be seen in relation to PPH-handling, and not as a general approach to emergency situations. The lowest score regarding collective efficacy was on the item “I think that every member of the team will express themselves clearly during PPH” (mean score 4.8, SD = 2.0), and the highest score on the item “As a team, we help each other prevent excessive PPH” (mean score 6.9, SD = 1.4). This may mostly reflect the nature of prehospital personnel’s work, rather than PPH itself [28]. In contrast, a recent study including pre- and post-simulation scores of self- and collective efficacy in PPH in intra-hospital personnel, participants scored 5.9 (SD = 1.1) on self-efficacy before the simulations, and 6.5 (SD = 0.9) after. Scores on collective efficacy in PPH handling increased from 5.8 (SD = 0.9) to 6.3 (SD = 0.8) [19]. This may indicate that personnel working in obstetric/resuscitation teams in hospital are more trained in this obstetric emergency, which is also natural.
Aronson and Bergström’s research [15] indicates that AC may effectively reduce need for blood transfusion, morbidity and mortality. Nevertheless, our participants rarely used this technique. This study, as well as earlier research enlighten the challenges in distributing knowledge to larger groups of personnel, and from high-income to low-income countries. Hence, a PPH digital learning program was developed, in addition to a simulator that enables participants to evaluate the pressure, placement and effect of AC. After the conduction of this study, prehospital personnel attended the course and were given a demonstration and opportunity to apply AC. In addition, a new PPH handling guideline has been implemented in hospital, resulting in that midwives and obstetricians now often arrive to the operating room in the patient’s bed, adding AC. In Tanzania, a structured inter-professional simulation program on PPH handling lead to a significant reduction in the use of ≥5 units of blood products related to severe bleeding after birth [19]. Moreover, training that included all levels of maternity staff, repeated sessions with realistic scenarios, and debriefing contributed to reduced blood transfusion rates in this high-risk maternity settings [29]. The same research team conducted a study on the effect of inter-professional simulations to reduce PPH, in a Norwegian university hospital. The researchers emphasized the importance of team training as a learning feature, and that inter-professional simulation enhanced self-efficacy and reduced perception of stress. Here, personnel also experienced an improved competence to provide efficient PPH management [30].
It may be argued that research conducted in low-income countries (LIC) are not transferable to high-income countries (HIC) similar to the setting for this study. Moreover, it may be argued that the study presented here is not as relevant due to the low incidence of PPH in HIC settings. Still, there is an increasing incidence of home births in Norway, as in Nordic countries [17, 18], and we argue that knowledge of PPH on competence in handling this condition is essential in prehospital personnel. Self-assessment of knowledge, experiences, teamwork and need for more education and training provide possibilities to provide tailored training and education of healthcare personnel, also in rare conditions.
Limitations
Due to the small sample size, findings here may not be generalizable to other countries or settings. Nevertheless, research support our findings, stating a need for more knowledge and competence in PPH and PPH handling internationally. Two validated tools were used to measure self-efficacy and collective efficacy, which increase the reliability of the study. Moreover, the new questionnaire was developed in-line with recommendations from the Delphi technique, and face- and content validity were high. The eight point scale may fail to measure the true attitudes of respondents. Also, it is not unlikely that responses will be influenced by previous questions. In the current study, there may have been some mis-interpretations of items on the PPHSE and PPHCE due to that the PPH reference was not included on all items.
Conclusion
Our findings indicate that prehospital personnel lack knowledge about postpartum hemorrhage (PPH) and manual aortic compression (AC). Hence, this study indicates a need for more education and training in PPH and PPH handling in prehospital personnel, to be able to assess and manage PPH.
Implications for further research
Responses on the free-text questionnaire in this study will be used to develop a tool with fixed response alternatives, for assessment of healthcare personnel’s knowledge about PPH and AC that can be used in other settings to assess knowledge gaps and what to focus on in quality improvement initiatives.
Availability of data and materials
All data generated or analyzed during this study are included in this published article, and is attached as a supplementary information file (see additional file 4).
Abbreviations
- AAA:
-
abdominal aorta aneurism
- AC:
-
aortic compression
- ECT:
-
European Credit Transfer and Accumulation System
- PPH:
-
postpartum haemorrhage
- PPHCE:
-
postpartum haemorrhage collective efficacy
- PPHSE:
-
postpartum haemorrhage self-efficacy
- SD:
-
standard deviation
References
WHO Recommendations on prevention and treatment of postpartum haemorrhage and the WOMAN trial. https://www.who.int/reproductivehealth/topics/maternal_perinatal/pph-woman-trail/en/. Accessed Nov 20 2020.
Kramer M, Berg C, Abenhaim H. Incidence, risk factors, and temporal trends in severe postpartum hemorrhage. Am J Obstet Gynecol. 2013;209:441–7. https://doi.org/10.1016/j.ajog.2013.07.007.
Bateman B, Berman M, Riley L, Leffert L. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesth Analg. 2010;110:1368–73. https://doi.org/10.1213/ANE.0b013e3181d74898.
Oyolese Y, Ananth C. Postpartum hemorrhage: epidemiology, risk factors and causes. Clin Obstet Gynecol. 2010;53:147–56. https://doi.org/10.1097/GRF.0b013e3181cc406d.
Fleischer A, Meirowitz N. Care bundles for management of obstetrical hemorrhage. Semin Perinatol. 2016;40:99–108. https://doi.org/10.1053/j.semperi.2015.11.015.
Merriam A, Bateman B, Ananth C, Wright J, Siddiq Z, D'Alton M, et al. Risk for postpartum hemorrhage, transfusion and hemorrhage-related morbidity at low, moderate and high volume hospitals. J Matern Fetal Neonatal Med. 2018;31(8):1025–34. https://doi.org/10.1080/14767058.2017.1306050.
Vangen S, Bødker B, Ellingsen L, Saltvedt S, Gissler M, Gerisson R, Nyfløt L. Maternal deaths in the Nordic countries. Acta Obstet Gynecol Scand. 2017; 96(9):1112–1119. Vhttps://doi.org/10.1111/aogs.13172.
Committee on Practice Bulletins-Obstetrics. Postpartum Hemorrhage. Practice Bulletin No. 183. Obstet Gynecol. 2017;130(4):168. https://doi.org/10.1097/AOG.0000000000002351.
Belfort M. Overview of postpartum hemorrhage. UptoDate 2019. https://www.uptodate.com/contents/overview-of-postpartum-hemorrhage. Accessed Nov 18 2020.
Clark S, Belfor M, Dildy G, Herbst M, Meyers J, Hankins G. Maternal death in the 21st century: causes, prevention and relationship to cesarean delivery. Am J Obstet Gynecol. 2008;199:e1–5. https://doi.org/10.1016/j.ajog.2008.05.009.
Berg C, Harler H, Atkinson S. Preventability of pregnancy-related deaths: results of a state-wide review. Obstet Gynecol. 2005;106:1228–34. https://doi.org/10.1097/01.AOG.0000187894.71913.e8.
Shields L, Wiesner S, Fulton J, Pelletreau B. Comprehensive maternal hemorrhage protocols reduce the use of blood products and improve patient safety. Am J Obstet Gynecol. 2015;212(3):272–80. https://doi.org/10.1016/j.ajog.2014.07.012.
Skupski D, Brady D, Lowenwirt I, Sample J, Lin S, Lohana R, et al. Improvement in outcomes of major obstetric hemorrhage through systematic change. Obstet Gynecol. 2017;130(4):770. https://doi.org/10.1097/AOG.0000000000002207.
Hofmeyr G, Quereshi Z. Preventing deaths due to hameorrhage. Best Pract Res Clin Obst Gynaecol. 2016;36:68–82. https://doi.org/10.1016/j.bpobgyn.2016.05.004.
Aronsson A, Bergstrom S. Abdominal compression of the aorta effective in severe postpartum hemorrhage. Läkartidningen. 2012;109(34–35):1478–80.
Mousa H, Blum J, El Senoun G, Shakur H, Alfirevic Z. Treatment for primary postpartum hemorrhage. Cochrane Database Syst Rev. 2014;2(CD0003249). https://doi.org/10.1002/14651858.CD003249.pub3.
Medical birth registry. 2019. https://www.fhi.no/en/hn/health-registries/medical-birth-registry-of-norway/. Accessed Nov 01 2020.
Blix E, Kumle M, Ingversen K, Huitfeldt A, Hegaard H, Olafsdottir O, et al. Transfers to hospital in planned home birth in four Nordic countries- a prospective cohort study. Acta Anesthesiol Gynecol Scand. 2016;95(4):420–8. https://doi.org/10.1111/aogs.12858.
Egenberg S, Øian P, Eggebø T, Arsenovic M, Bru L. Changes in self-efficacy, collective efficacy and patint outcome following interprofessional simulation training on postpartum haemorrhage. J Clin Nurs. 2016;26:3174–87. https://doi.org/10.1111/jocn.13666.
Jirwe M, Gerrish K, Keeney S. Identifying the core components of cultural competence: findings from a Delphi study. J Clin Nurs. 2009;18:2622–34. https://doi.org/10.1111/j.1365-2702.2008.02734.x.
Keeney S, Hasson F, McKenna H. The Delphi technique in nursing and health research. West Sussex: Wiley-Blackwell; 2011.
Bing-Jonsson P, Bjørk I, Hofoss D, Kirkevold M, Foss C. Competence in advanced older people nursing: development of 'Nursing older people- competence evaluation tool'. Int J Older People Nursing. 2014;10:59–72. https://doi.org/10.1111/opn.12057.
Streiner D, Norman G. Health measurement scales: a practical guide to their development and use. Oxford: Oxford Scholarship; 2008. https://doi.org/10.1093/acprof:oso/9780199231881.001.0001.
IBM Corporation. IBM SPSS Statistics for Windows, Version 25.0. Armonk, New York; 2017.
White M, Marsh E. Content analysis: a flexible methodology. Libr Trends. 2006;55(1):22–45. https://doi.org/10.1353/lib.2006.0053.
Dahlke J, Mendez-Figueroa H, Maggio L, Hauspurg A, Sperling J, Chauhan S, et al. Prevention and management of postpartum hemorrhage: a comparison of 4 national guidelines. Am J Obstet Gynecol. 2015;213:1–10. https://doi.org/10.1016/j.ajog.2015.02.023.
Senthiles L, Goffinet F, Vayssiere C, Deneux-Tharaux C. Comparison of postpartum haemorrhage guidelines: discrepancies underline our lack of knowledge. Int J Obstet Gynaecol. 2016;124(5):718–22. https://doi.org/10.1111/1471-0528.14305.
Patterson P, Arnold R, Abebe K, Lave J, Krackhardt D, Carr M, et al. Variation in emergency medical technician partner familiarity. Health Serv Res. 2011;46(4):1319–31. https://doi.org/10.1111/j.1475-6773.2011.01241.x.
Egenberg S, Masenga G, Bru L, Eggebø T, Mushi C, Massay D, et al. Impact of multi-professional, scenario-based training on postpartum hemorrhage in Tanzania: a quasi-experimental, pre- vs. post-intervention study. BMC Pregnancy and Childbirth. 2017; 17(287). https://doi.org/10.1186/s12884-017-1478-2.
Egenberg S, Karlsen B, Massay D, Kimaro H, Bru L. "No patient should die of PPH just for the lack of training!" Experiences from multi-professional simulation training on postpartum hemorrhage in northern Tanzania: a qualitative study. BMC Medical Education. 2017;17(119). https://doi.org/10.1186/s12909-017-0957-5.
Declaration of Helsinki- Ethical Principles for Medical Research Involving Human Subjects. http://www.wma.net/en/30publications/10policies/b3. Accessed Nov 20 2020.
Acknowledgements
Participants in the expert group are acknowledged for their thorough work with the development of the questionnaire. Grethe Heitmann is acknowledged for taking the initiative to this quality improvement initiative both intra- and prehospital, development of a local guideline and the digital course in PPH, as well as training in AC. Heitmann was not involved in the research project.
Funding
The study was funded by Østfold University College. The funding body did not take part in design of the study, collection, analysis, and interpretation of data or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
ACL participated in planning the study, facilitated the expert-group inputs, development of the questionnaire, data collection, analysis, and writing and approval of the whole draft of the manuscript. LEU participated in planning the study, facilitating the intervention, data collection, and critical revisions of the manuscript, and approval of the final version of the manuscript. AKH participated in planning the study, development of the questionnaire, data collection, analysis, and writing and approval of the whole draft of the manuscript. VAG participated in planning the study, development of the questionnaire, data collection, analysis, and writing and approval of the whole draft of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Norwegian Centre for Research Data (NSD) (project no.740937). The study was based on the research ethical principles in the Declaration of Helsinki [31], on willing participation, consent to participate implicated by completion and submission of questionnaire, anonymity and confidentiality. The study was presented for the Regional ethics committee for medical and healthcare research (REK), and judged not needing an ethical approval (reference no. 202781).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary informations
Additional file 1.
The STROBE (Strengthening the reporting of observational studies in epidemiology) checklist.
Additional file 2.
The postpartum haemorrhage self-efficacy (PPHSE) and -collective efficacy (PPHCE) items.
Additional file 3.
The questionnaire developed as part of the study, assessing knowledge and self-assessed competence in PPH handling.
Additional file 4.
Anonymized data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Leonardsen, AC.L., Helgesen, A.K., Ulvøy, L. et al. Prehospital assessment and management of postpartum haemorrhage- healthcare personnel’s experiences and perspectives. BMC Emerg Med 21, 98 (2021). https://doi.org/10.1186/s12873-021-00490-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12873-021-00490-8