
Abstract
Background
Knowing of perception of the illness, and cardiovascular risk factors in patients with myocardial infarction is crucial in engaging in effective secondary prevention. This study aimed to examine illness perception and cardiovascular risk factors in patients with myocardial infarction undergoing percutaneous coronary intervention.
Methods
The participants comprised 131 patients undergoing a first-time percutaneous coronary intervention at a metropolitan, tertiary referral hospital in Tabriz, Iran. The convenience sampling method was employed to select the research sample within a six-month period. The instruments used were as follows: (1) Demographic and health information form, (2) The Brief Illness Perception Questionnaire (3) The Health Risk Assessment framework developed by the Centers for Disease Control and Prevention. The design of the study was descriptive, cross sectional. The continuous variables were analyzed using Independent t-test and analysis of variance (ANOVA); and categorical variables were compared using the chi-square test.
Results
Most participants had a positive family history of cardiovascular disease (54.2%), with 66.4% of participants having at least one cardiovascular risk factor such as diabetes (36.6%) hypertension (32.8%) and dyslipidemia (16%). Most participants were physically inactive (78.6%), about 48.9% were overweight, 34.4% suffered from obesity and 26% were smokers. Illness perception in this study was seen to be high (6.21), with highest scores occurring in the illness control dimension (6.83) and lowest scores occurring in the understanding dimension (3.77). There was a significant relationship between illness perception and physical activity, nutrition, sleep and general health. Direct significant relationships between biometric values (cholesterol, glucose, blood pressure); psychological factors (depression, anxiety and stress) and illness perception were also found to exist.
Conclusions
Low scores in two dimensions of illness perception may lead to psychological consequences such as stress, anxiety, and depression. The relationship between illness perception and some risk factors of cardiovascular disease such as physical activity, diet and biometric values, reveal the need for more attention to patient education and counselling.
Similar content being viewed by others

Background
Characterized by an annual mortality rate of about 17.9 million people worldwide as at 2016 [1], cardiovascular diseases (CVDs) remain one of the commonest causes of death globally, accounting for 20% of worldwide deaths and 35% of deaths in Iran [2, 5]. Myocardial infraction (MI) has been known to cause more than four-fifths of deaths from cardiovascular diseases [3]. Compared to Western nations, most Asian countries have higher mortality rates of CVDs except for Japan, South Korea, Thailand, and Singapore [4]. Given the high costs of treatment for patients with MIs and the high burden of expenses on the healthcare system [5], an important but low-cost method of controlling CVDs that governments can adopt is to focus on mitigation of relevant risk factors, especially the modifiable factors [6, 7]. Several studies support the role of risk factor change on the quality of life of patients at high risk of cardiovascular events [8, 9], with several other studies revealing that people know little and do little about cardiovascular risk factors. These findings have spurred identification of modifiable CVDs risk factors in order to mitigate these medical conditions [10,11,12,13]. More than 70% of CVD cases globally are attributed to modifiable risk factors [14]. From the perspective of self-determination theory, positive human behaviors that are aligned with health-related goals are usually internalized by the patient in question, increasing motivation and making the patient feel more responsible for the outcomes, a situation that suggests more attention be given carefully to the patient’s experience and patient’s illness perception [27]. The importance of illness perception with respect to myocardial infarction has been demonstrated in the high attendance at rehabilitation by patients who feel they have a good grasp of the nature of the illness and that it can be controlled, a phenomenon related to patients’ compliance and relevant to patient-reported outcomes [28]. Thus, a patient who believes that nothing can change the course of the disease might be more prone to risk [29]. Patients can successfully adapt to CVDs only if they make long-term changes to their lifestyles and change their false beliefs regarding their conditions [21]. In addition, adherence of patients to secondary preventive measures may reduce the risk of progression of coronary heart disease (CHD) and speed up the recovery progress [1].
The concept of illness perception, a relevant factor in cardiovascular health behavior [1], is an organised belief model that predicts the patient’s future behavior toward the disease management and the correction of risk factors [15]. Based on several studies, a relationship has been established between illness perception and patients outcomes such as quality of life [16, 17], coping [18] and health care use [19]. This concept is derived from the Self-regulation Model of Leventhal [22] that states that in the face of an illness, an individual is moved to modify the health-related risks of that condition, according to how she/he perceives the illness. Also, there might even be different illness perceptions among patients with similar medical conditions and injuries [30]. Hence, a good perception or understanding of an illness leads to better adaptability, an improved general health status, ability to manage the illness more efficiently, a quicker return to work and reduced stress levels [20, 23, 24]. However, most patients with ischaemic heart diseases (IHDs) have insufficient information regarding the important role of this form of behavior plays in preventing the recurrence of IHDs, thus putting themselves at high risk of IHD recurrence [21]. Nicolai et al. indicate that changing lifestyle after an Acute Myocardial Infarction (AMI) is affected by a combination of physical, mental and social factors. They opine that such patients need more personalized information regarding causes of and risk factors for diseases as well as advantages of lifestyle change. They also advocate for involvement of friends and family members in the form of social support and participation during consultation and lifestyle training [22].
The opinions of patients about diseases often differ from those of therapists, with medical staff being largely unaware of patients’ opinions about their diseases and rarely focusing on the latter’s beliefs. Lack of information, inadaptability to various treatments, and skepticism towards the positive effect of behavior change on the outcome of a disease are correlated with negative self-care behaviours of patients [23]. Knowing patients’ risk factors and their perception of CVDs can provide clinicians and health managers with realistic insights for the development and implementation of public health policies to promote patient education regarding the reduction of adjustable risk factors and prevention of IHDs. In illness perception, patients’ beliefs regarding lifestyle and disease risk can be adjusted in clinical interventions, giving nurses and other clinicians the opportunity to develop purposive interventions that will correct such beliefs in patients [3], especially as changes in illness perception over time has been shown to be useful in aiding the development of educational programs to bring about positive attitudes towards health beliefs in this subset of patients [1]. Hence, this study aimed to determine the IHD risk factors and their correlations with illness perception among the patients hospitalized and diagnosed with AMI at Shahid Madani Cardiovascular Center (Tabriz, Iran) who received the percutaneous coronary intervention (PCI).
Methods
Study design and participants
The statistical population of this cross-sectional descriptive study included 131 patients diagnosed with AMI who visited Shahid Madani Hospital and underwent first-time PCI. This study covered all the departments of surgery and cardiology and Cardiac Care Units (CCUs) of Shahid Madani Hospital in Tabriz, Northwest of Iran. This hospital is a CVD sub-specialty center with facilities for cardiac catheterization and is a referral centre for patients in need of angiography or PCI. After obtaining permission from Tabriz University of Medical Sciences, patients who met the inclusion criteria, were enrolled into the study at the discretion of clinicians in the CCU and departments of surgery and cardiology. The purpose of the research was explained to the participants, who filled out the written consent forms individually, completed the questionnaires and were interviewed. The convenience sampling method was employed to select the research sample within a six-month period (from December 2020 to May 2021).
In order to estimate the sample size, the formula for the estimation of a mean was employed. In the current study, the value of z with a 95% confidence level was 1.96, and total mean (standard deviation) of IP was 45.45 (9.33) based on the study of Allahbakhshian et al. [24] and considering d (precision) equal to 0.55, a sample size of 119 people was obtained. Regarding a possible attrition rate of 10%, the sample size was equal to 130 people. Continued enrollment of participants was conducted until the planned sample size was reached.
Inclusion criteria
-
Adult patients aged 18–65 years.
-
All patients experiencing their first myocardial infractions, receiving PCIs on an emergency basis for the first time at the hospital, who were in stable medical condition.
-
Persian, Turkish, or Kurdish-speaking Iranians conversing in either Turkish or Persian languages.
Exclusion criteria
-
Exclusion criteria are: unwillingness to continue participating in the study, and failure to complete the data collection tools.
Data collection
Data were collected by first author in order to minimise variability. The data were gathered via face-to-face interview using validated questionnaire. The Health Risk Assessments (HRAs) and Brief Illness Perception Questionnaire (IPQ-B) were used in this study.
Health risk assessments (HRAs) questionnaire
The framework proposed by the Centers for Disease Control and Prevention (CDC) and called Health Risk Assessments (HRAs) was employed to evaluate the IHD risk factors. The CDC developed this framework on the basis of three recently conducted systematic literature reviews and expert input from physicians, researchers, members of medical associations, wellness program developers, and CDC subject matter experts [25]. This framework includes 15 dimensions (with 37 indices): physical activity, tobacco use, alcohol use, nutrition, seat belt use, depression, anxiety, high stress, social/emotional support, pain, general health, activities of daily living, instrumental activities of daily living, sleep, and biometric measures (i.e., blood pressure, cholesterol, blood glucose, overweight/obesity). Among health risk assessment tools, the CDC’s HRAs framework may be completed through an interactive program before or as part of a visit and can identify chronic diseases, injury risks, modifiable risk factors, and urgent health needs. It assesses physical, psychological, and socioeconomic factors in addition to how these influence health and functional status [26].
All subjects were measured for their height, weight, body mass index (BMI), and blood pressure (BP) by first author. Height and weight were measured to the nearest 0.1 cm and 0.1 kg respectively using a pre-calibrated freestanding mounted to scales stadiometer (Seca, Germany) and height rod in light clothing and without shoes on. BMI (kg/m2) was calculated as weight (kg) divided by squared height (m2). Obesity is defined as BMI > 30 kg/m2 and overweight is defined as BMI of 25.1–30 kg/m2 [25]. An automated BP monitor (Citizen, Japan) was used to measure BP. Borderline high is defined as elevated BP with systolic BP (SBP) 120–139 mmHg and/or diastolic BP (DBP) 80–89 mmHg. High BP is defined as elevated BP with SBP ≥ 130 mmHg and/or DBP ≥ 90 mmHg [25]. Biochemical tests at the time of admission or the first day after hospitalization were requested for all patients by patient’s physician and their values were extracted from patients' electronic medical record. According to CDC’s HRAs framework, borderline high cholesterol is defined as elevated cholesterol 200–239 mg/dl and high cholesterol is defined as elevated cholesterol 240 mg/dl or higher. Borderline hyperglycemia is defined as elevated glucose 100–125 mg/dl and hyperglycemia as elevated glucose 126 mg/dl or higher. Also, according to this framework, those who have smoked in the last 30 days are defined as smokers [25].
The original version of HRAs questionnaire was translated from English into Persian. This was done by a faculty member with good command of the Persian language. The translated version was reviewed by the research team. Then, two faculty member familiar with measured concept and with good command of both languages reviewed the translated version and a final version was obtained. Intra-class correlation coefficient was between 0.78 and 1 for 15 dimensions of HRAs questionnaire in a pilot study, in which the questionnaire was completed for 10 patients by two members of the research team independently.
Brief illness perception questionnaire (IPQ-B)
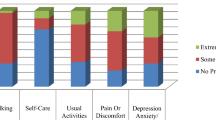
The IPQ-B is a nine-item scale that has each item rated on a scale from 0 (minimum) to 10 (maximum) and which assesses the emotional and cognitive aspects of individual’s illness [27]. Each of the terms of this questionnaire examines a dimension of understanding of the disease as follows: item 1: consequences, item 2: timeline, item 3: Personal control, item 4: treatment Control, item 5: identity, item 6: concern, item 7: illness comprehensibility and item 8: emotions, and item 9 is a question that is answered by the patient about one’s opinion regarding the cause of illness. Items 1–5 assess the cognitive dimensions which relate to understanding of illness, its causes, effect of treatment while items 6 to 8 evaluate the emotional dimensions that relate to emotions such as mood, fear, anxiety or anger. The total score of illness perception is calculated by inverting the score for items 3, 4 and 8 and added to the score of the other items. The maximum total score is 80 and the minimum total score is 0. A higher score indicates a more threatening view of the patient, while a lower score indicates a more optimistic view of the disease [28].
The reliability and validity of the Farsi version of this questionnaire has been verified and localized by Bazzazian and Besharat [29]. Their results showed that the scale has cross- cultural validity. In the present study, the internal consistency reliability (Cronbach’s alpha) of questionnaire’s subscales were between 0.76 and 0.82. According to the criteria (at least 0.65) indicated by Devellis [30], most subscales demonstrated good internal consistency reliability.
Statistical data analysis
All data were analyzed using SPSS 21.0 (IBM, Armonk, NY, USA). The continuous data for normal distribution were tested using the Kolmogorov–Smirnov test, which showed the normal distribution of variables. The continuous variables are presented as means ± standard deviation and were analyzed using Independent t-test and analysis of variance (ANOVA) and the Least Significant Difference (LSD) post hoc test. Categorical variables are presented using n (%) and were compared using the chi-square test.
Results
Characteristics of patients
Of the 131 study participants, 72 patients (55%) were male, and 130 patients (99.2%) were married. They were aged 36–65 with a mean age (± standard deviation) of 55.06 (± 7.72) years old. The mean age of male patients was 53.25, whereas that of female patients was 57.28, and most of them were illiterate (57; 43.5%). A positive family history of CVDs was seen in 71 patients (54.2%), and 87 (66.4%) of them had at least one co-morbid medical condition, the most common being hypertension (HTN) (32.8%), diabetes mellitus (DM) (36.6%), and HPL (16%). The co-morbid entities of DM and HTN were jointly observed in 12.2% of participants, whereas 8.39% had all three comorbid conditions. All patients were presenting for PCI for the first time.
Analysis of health risk assessment
Regarding IHD risk factors based on the HRA questionnaire, research results showed that 78.6% of patients reported no sports activities. The average weekly duration for engagement in sporting activity was 0.82 days, with the average time duration for their sports activities being 7.59 min. Moreover, 26% of them reported smoking in the past 30 days, and 24.43% of them reported eating fatty and fried foods twice a week or more frequently. Finally, 13.74% of participants reported drinking sweet beverages twice a week or more. Majority of participants stated that they had experience some sort of depression (41.22%) and anxiety (35.88%). The highest stress level (within the 0–3 score range) was related to their health with an average of 1.60, whereas the blood pressure, cholesterol, and blood sugar values above 140/90, 240 mg/dl, and 126 mg/dl respectively were observed in 25.95%, 16.03%, and 35.88% of participants, respectively. Moreover, 48.9% and 34.4% of the participants were overweight and obese, respectively (Table 1).
Analysis of illness perception
The mean of the illness perception was reported to be 43.49% (9.56) within the 0–80 range. Table 2 demonstrates the mean of each expression. The highest mean was related to the dimension of treatment control (6.83), whereas the lowest mean came from the understanding dimension (3.77). In addition, a good number of participants stated that the causes of illness were stress (36; 27.5%) and family issues (30; 22.9%).
Relationship between risk factors and illness perception
Table 3 shows the correlations between IHD risk factors (continuous variables) and the illness perception. Accordingly, the number of days of physical activities (r = − 0.21, p = 0.014) and the duration of sports activities (r = − 0.28, p = 0.001) had inverse significant correlations with illness perception. This meant that the less often participants engaged in physical activities, the higher the illness perception score; thus, they regarded the illness more threatening. Furthermore, the use of fatty foods (r = − 0.17, p < 0.048) and sugar sweetened drinks (r = − 0.22, p < 0.011) had inverse significant correlations with illness perception. In other words, when patients perceive the illness as more threatening, the total score of illness perception increases and the use of fatty foods and sugary drinks will decrease. There was also an inverse significant correlation between sleep and the total score of illness perception (r = − 0.24, p = 0.005). In other words, the less sleep the patients reported, the higher the total score of illness perception; thus, the illness became more threatening. Also, the total score of the illness perception had direct significant correlations with cholesterol (r = 0.23, p = 0.006), glucose (r = 0.19, p = 0.025), systolic blood pressure (r = 0.37, p < 0.001), and diastolic blood pressure (r = 0.26, p = 0.002). In other words, the total score of illness perception increased as these biometric values increased, with patients perceiving the illness as more threatening. The findings reported no significant relationships between the total score of illness perception and other IHD factors or BMI (p > 0.05) (Table 3). Table 4 depicts the correlations between IHD risks (categorical variables) and illness perception. Participants’ total illness perception score had significant correlations with depression (p < 0.001), anxiety (p = 0.001), health-related stress (p < 0.001), financial issues (p < 0.001), family or social relationships (p = 0.003), and general health (p < 0.001). The subgroups of each of these variables were compared in terms of the total scores of illness perception by the LSD post hoc test. Results showed the total score of illness perception to be significantly higher in patients who felt more depressed, anxious, and stressed about their health, financial problems and family or social relations. Therefore, these patients were seen to perceive the illness as more threatening. At the same time, patients who perceived their general health as weaker had significantly higher scores of the illness perception. In other words, these patients also considered the illness more threatening. Other variables such as age, sex, and level of education did not influence on the illness perception.
Discussion
This study aimed to determine heart disease risk factors and their correlations with illness perception among patients with an initial diagnosis of AMI who were undergoing PCI. The mean age of patients was low, with male and female patients averaging 53.25 and 57.28 years old, respectively. This finding is consistent with findings reported in a meta-analysis by Poorzand et al. [31]. The history of smoking over the past 30 days and history of familial heart diseases were positive in more than one-fourth and more than half of the participants, respectively. The familial history of positive CVDs is known to increase the chance of early emergence of heart disease by 2.35 [31]. In study of Gharios and colleagues [32], also a parental history of CHD, especially before 60 years, best predicted cardiovascular mortality. Findings of this study which include a positive history of co-morbid conditions such as HTN, DM, and HPL in most of the participants with a history of familial heart diseases, some of whom had two or three of those conditions simultaneously, lend credence to the fact that, CVD is a major cause of mortality in diabetic patients and that many other factors (e.g., hypertension) play a key role in the high prevalence of CVDs [33]. Blood pressure increases in diabetic patients are known to be twice more than in non-diabetic patients and patients with hypertension are often resistant to insulin and are more prone to the risk of diabetes than normal people [34]. A high percentage of CVDs and CVD-caused deaths is attributed to the adjustable risk factors, the most important of which are metabolic factors [14]. The findings from this study that most participants engaged in no physical activities, nearly half of them were overweight and more than one-third of them were obese, point to the fact that they are prone to metabolic syndrome, the latter been seen as an important factor seen in several similar studies from Iran and all over the globe [35, 36]. Mirzaei et al. conducted a study in Yazd, Iran and reported that lack of physical activities and unhealthy eating habits were among the most prominent risk factors of CVDs in a healthy society [37]. They also reported that 26.5% of Iran’s healthy population would be prone to the high risk of CVDs based on the Framingham risk score (FRS) [38]. The onset age of CVDs is ten years earlier in Iran than in the developed countries [39]. The growing CVD epidemic of the recent 40 years in Iran might be correlated with socioeconomic developments, changes in diets, insufficient physical activities, industrialization and urbanization, increased life expectancy, increased metabolic and physical risk factors, insufficient and less cost-effective access to early care and treatment, and low adaptability for economic reasons and psychological problems [40]. According to the findings of this meta-analysis, the most prevalent and strongest risk factors of premature coronary artery disease (PCAD) in the Iranian population are type 2 DM, dyslipidemia, familial history of CAD, smoking, hypertension and higher values of BMI were reported for patients diagnosed with PCAD [31]. These findings indicate the important roles that high BMI and a positive familial history of CAD play in the development of atherosclerotic CAD, especially with respect to the mean age of about 55 years as seen in more than half of study participants who experienced AMI for the first time. The results of one systematic review reveal that diabetes mellitus type 2, familial history of CAD, dyslipidemia, smoking, and hypertension are significantly and positively correlated with CAD in young adults compared with the healthy population of Iran [34] while in other studies, the prevalence of IHD risk factors was subject to change depending on the people’s lifestyle habits, income and health systems of countries [41, 42]. A similar study in Greece reported the prevalence of hypertension, hyperlipidemia, obesity, and severe diabetes [43] while another study in Poland reported that a history of current or previous habit of smoking was associated with a high prevalence rate of CVD and CV risk factors [44]. Moo-Sik et al. evaluated the scores of CVD risk factors in patients under PCI with no history of CVDs through the FRS and concluded that some of the conventional risk factors (e.g., high BMI) increased within a 17-year period. They also demonstrates that although traditional FRS and its associated predicted 10-year cardiovascular risk declined over time, the prevalence of risk factors increased in patients undergoing PCI. The study suggests the need for a new risk-factor assessment in this patient population [45]. Apparently, the HRA framework can be employed to evaluate the IHD risks and provide caregivers with more information regarding risks and corrective measures.
The total mean score of illness perception was high among participants of this study, something which indicates that they considered the illness a threat. Other findings of this study included the low score of illness perception in the dimensions of personal control and understanding. By contrast, the participants had high illness perception scores in the dimensions of concern and treatment control. Lotfi et al. reported a similarly high total mean score of illness perception [20] as did another study from Indonesia which reported a high total mean score of illness perception and the score of understanding and personal control to be average and low, respectively, which is consistent with findings from this present study [46]. In a study by Petriček et al., the dimension of understanding had the lowest mean score and was a significant predictor of BMI [47]. In related studies, the threatening perception of the illness was associated with the numerous outcomes of patients such as a reduced quality of life, lower levels of health and higher levels of emotional distress [48], less frequent presence in cardiac rehabilitation programs [49], low adherence to prescribed medications, sports, and recommended diets [50], and high mortality [51]. Thus, training and counselling programs are required to modify and improve the illness perception of participants in this current study. Ashour et al. reported that the low perception of personal control and the high perception of disease symptoms could predict the highly perceived learning needs in patients after a PCI [52].
With the findings of this study, it is seen that the total mean score of the illness perception had inverse correlations with physical activity, use of fatty and fried foods, sugar sweetened drinks, sleep, and general health. In other words, patients who perceived the disease as more threatening reported fewer physical activities as well as less use of fatty and fried foods and sugary drinks. Consistent with the findings of this present study is another study which reported that a more threatening view of an illness was correlated with the better diet management [46]. However, findings of some previous studies indicate contradictory results regarding this relationship between illness perception and healthy behavior. For instance, Mosleh et al. predicted better illness perception, better adherence to physical activities, and better adherence to treatment [50]. Nonetheless, Gauro et al. in Nepal reported an inverse correlation between illness perception and cardiovascular health behavior [21], which show that opinions about an illness require psychological training intervention to improve disease management methods and enhance adherence to healthy behaviors [50]. Patients with more threatening views of their diseases reported fewer sleep hours, higher levels of anxiety, stress, and depression, and lower levels of general health. Yeom and Shin reported that the illness perception could be correlated with sleep hours and disease-caused stress and that stress could have a mediating role in the correlation between the illness perception and sleep [53]. In other words, the negative effect of illness perception on sleep can be mitigated by regulating stress. It is also necessary to develop intervention programs that can reduce the stress related with illness perception among patients. Doi-Kanno and H. Fuahori reported that negative opinions about illness and other factors such as the physical activity patterns, use of fat, smoking, stress, and anxiety after the PCI could predict depression in patients after an MI [54]. According to the findings of this study, the total score of the illness perception had direct correlation with biometric values such as cholesterol, blood glucose, and blood pressure. In other words, increasing each of these biometric values would make the illness more threatening. Brewer et al. found a correlation between the better identification of an illness and the better control of cholesterol as well as adherence to drugs [55]. Other studies have reported that illness perception was correlated with the self-care behaviors aimed at improving health and moderating lifestyle [56, 57]. In a study by Goldman, participants believed that use of anti-hypertensive drugs would be preferable to cholesterol-lowering drugs and considered cholesterol levels less important than hypertension [58]. Therefore, in the light of these study findings, it is necessary to develop national training and health checkup programs aimed at teaching patients, providing them with lifestyle modification strategies [59], and improving the patient–clinician relationship [60] by enhancing patients’ knowledge about the role of biometric values and other risk factors in the development of CVD.
Conclusion
In this study, participants experienced most of the IHD risk factors and had high mean scores of concern about the illness and its outcomes in terms of the illness perception. This might lead to psychological outcomes such as stress, anxiety, and depression. The correlations of the illness perception with some lifestyle components such as physical activity and diet as well as with biometric values indicate the necessity of paying more attention to training patients and providing them with consultation to improve the perception of CVDs as a manageable illness. As far as it is known, this is the first study to employ the CVD risk assessment framework published by the CDC, USA in Iran. The positive familial history of CVDs, diabetes, and hypertension depicts the necessity to paying more attention to these patients in terms of screening for hypertension, diabetes, and dyslipidemia. Health policies in Iran and similar climes should be focused on the risk factors having major roles in preventing CVDs and mortality with further emphasis on the most important factors in specific groups such as patients with positive familial history, diabetes, and hypertension. Doctors, nurses and other clinicians should be trained to execute the crucial role of ensuring that patients are educated properly on managing lifestyles in a bid to mitigate the psychological outcomes resulting from myocardial infraction and its treatments. Evidence from this study about the relationship between illness perception and some psychological, and modifiable lifestyle factors can provide ideas for other studies. In other words, our results suggest that the design of an educational intervention study and its consequences in the disease follow-up phase be done.
One of the limitations of this study is the cross-sectional nature of it, the relationships shown between HRA questionnaire’s dimensions with illness perception cannot accurately reflect the causal relationship. Another limitation of the study was convenience of the sampling that reduces the generalizability of the results. In addition, in current study, patients who experienced first myocardial infractions, received PCIs for the first time could recruit in the study. Therefore, as a limitation, this study may not be the representative of patients with AMI in Iran in general.
Availability of data and materials
The data that support the findings of this study are available from the authors upon reasonable request.
Abbreviations
- ADL:
-
Activities of daily living
- AMI:
-
Acute myocardial infarction
- ANOVA:
-
Analysis of variance
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- CCU:
-
Cardiac care unit
- CDC:
-
Centers for disease control and prevention
- CHD:
-
Coronary heart disease
- CVD:
-
Cardiovascular disease
- DBP:
-
Diastolic blood pressure
- DM:
-
Diabetes mellitus
- HPL:
-
Hyperlipidemia
- HRA:
-
Health risk assessments
- HTN:
-
Hypertension
- IHD:
-
Ischaemic heart diseases
- IPQ:
-
Illness perception questionnaire
- IPQ-B:
-
Brief illness perception questionnaire
- LSD:
-
Least significant difference
- MI:
-
Myocardial infraction
- PCI:
-
Percutaneous coronary intervention
- SBP:
-
Systolic blood pressure
References
Ashour A, Al-Smadi A, Shajrawi A, Al-Rawashdeh S, Alshraifeen A, Abed M. Changes in illness perception among patients’ undergoing percutaneous coronary intervention. Heart Lung. 2020;49(6):836–41.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021.
Lerdal A, Hofoss D, Gay CL, Fagermoen MS. Perception of illness among patients with heart failure is related to their general health independently of their mood and functional capacity. J Patient Rep Outcomes. 2019;3(1):1–7.
Ohira T, Iso H. Cardiovascular disease epidemiology in Asia: an overview. Circ J. 2013;77(7):1646–52.
Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health. 2018;18(1):975.
Rezaei Hachesu V, Naderyan Feli S, Zare Sakhvidi MJ. Prevalence of cardiovascular risk factors among taxi drivers in Yazd, Iran. J Community Health Res. 2017;6(4):200–6.
World Health Organization. World health assembly update 25 may 2019: international statistical classification of diseases and related health problems (ICD‐11). https://www.who.int/news-room/detail/25-05-2019-world-health-assembly-update. Accessed March 24, 2021.
Cesaro A, Gragnano F, Fimiani F, Moscarella E, Diana V, Pariggiano I, Concilio C, Natale F, Limongelli G, Bossone E, et al. Impact of PCSK9 inhibitors on the quality of life of patients at high cardiovascular risk. Eur J Prevent Cardiol. 2020;27(5):556–8.
Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Internal Med. 2005;143(9):659–72.
Baghernezhad Hesary F, Vahdaninia V, Vahdaninia Z, Sadeghi R. Level of knowledge, attitude and practice of clients of rural health centers in relation to some risk factors for cardiovascular disease. J Health Adm. 2020;23(3):66–74.
Alanazi A, Alghanim MH, Alamer AJ, Alshaqaqiq MA, Busaeed MMA, Alahmed AH, Alali AI, Almazyadi H, Alharbi WF, Nasser IA, et al. Acute myocardial infarction patients’ knowledge regarding the modifiable risk factors of heart disease. Int J Pharm Res Allied Sci. 2020;9(2):210–6.
Khan NS, Shehnaz SI, Guruswami GK, Ibrahim SAM, Mustafa SAJ. Knowledge of warning signs, presenting symptoms and risk factors of coronary heart disease among the population of Dubai and Northern Emirates in UAE: a cross-sectional study. Nepal J Epidemiol. 2017;7(2):670–80.
Saengsuwan J, Suangpho P, Tiamkao S. Knowledge of stroke risk factors and warning signs in patients with recurrent stroke or recurrent transient ischaemic attack in Thailand. Neurol Res Int. 2017;2017:8215726.
Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, Brauer M, Kutty VR, Gupta R, Wielgosz A. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395(10226):795–808.
Hoving JL, van der Meer M, Volkova AY, Frings-Dresen MH. Illness perceptions and work participation: a systematic review. Int Arch Occup Environ Health. 2010;83(6):595–605.
Yaraghchi A, Rezaei O, Mandegar MH, Bagherian R. The relationship between Illness perception and quality of life in Iranian patients with coronary artery bypass graft. Procedia-Soc Behav Sci. 2012;46:3329–34.
Thomson P, Rushworth GF, Andreis F, Angus NJ, Mohan AR, Leslie SJ. Longitudinal study of the relationship between patients’ medication adherence and quality of life outcomes and illness perceptions and beliefs about cardiac rehabilitation. BMC Cardiovasc Disord. 2020;20(1):71.
Tiemensma J, Gaab E, Voorhaar M, Asijee G, Kaptein AA. Illness perceptions and coping determine quality of life in COPD patients. Int J Chronic Obstr Pulm Dis. 2001;2016:11.
Schwille-Kiuntke J, Rüdlin SL, Junne F, Enck P, Brenk-Franz K, Zipfel S, Rieger MA. Illness perception and health care use in individuals with irritable bowel syndrome: results from an online survey. BMC Fam Pract. 2021;22(1):1–14.
Lotfi-Tokaldany M, Shahmansouri N, Karimi A, Sadeghian S, Saadat S, Abbasi SH, Jalali A. Association between illness perception and health-related quality of life in patients with preexisting premature coronary artery disease. J Psychosom Res. 2019;120:118–23.
Gauro P, Thaniwattananon P, Kritpracha C. Illness perception predicting cardiovascular health behaviors among patients with ischemic heart disease in Nepal: a descriptive cross-sectional study. JNMA J Nepal Med Assoc. 2020;58(231):884–8.
Nicolai J, Müller N, Noest S, Wilke S, Schultz JH, Gleißner CA, Eich W, Bieber C. To change or not to change - That is the question: A qualitative study of lifestyle changes following acute myocardial infarction. Chronic Illn. 2018;14(1):25–41.
Najafi Ghezeljeh T. eydi m, Haghani S: Illness perception in patients with heart failure admitted to selected centers of iran university of medical sciences. Nurs Midw J. 2019;17(2):91–101.
Allahbakhshian A, Ghahramanian A, Tabrizi FJ, Shirazy S. Examining the relationship between illness perception, adherence to medication regimen and readmission in patients with heart failure. J Adv Pharm Educ Res. 2019;9(S2):143.
Goetzel RZ, Staley P, Ogden L, Stange PV, Fox J, Spangler J, Tabrizi M, Beckowski M, Kowlessar N, Glasgow RE. A framework for patient-centered health risk assessments: providing health promotion and disease prevention services to Medicare beneficiaries. US Department of Health and Human Services, Centers for Disease Control and Prevention, Atlanta, GA (2011). http://www.cdc.gov/policy/opth/hra/.
Krist AH, Phillips SM, Sabo RT, Balasubramanian BA, Heurtin-Roberts S, Ory MG, Johnson SB, Sheinfeld-Gorin SN, Estabrooks PA, Ritzwoller DP. Adoption, reach, implementation, and maintenance of a behavioral and mental health assessment in primary care. Ann Fam Med. 2014;12(6):525–33.
Basu S, Poole J. The brief illness perception questionnaire. Occup Med. 2016;66(5):419–20.
Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–7.
Bazzazian S, Besharat MA. Reliability and validity of a Farsi version of the brief illness perception questionnaire. Procedia Soc Behav Sci. 2010;5:962–5.
DeVellis RF, Thorpe CT. Scale development: theory and applications. London: Sage Publications; 2021.
Poorzand H, Tsarouhas K, Hozhabrossadati SA, Khorrampazhouh N, Bondarsahebi Y, Bacopoulou F, Rezaee R, Jafarzadeh Esfehani R, Morovatdar N. Risk factors of premature coronary artery disease in Iran: a systematic review and meta-analysis. Eur J Clin Invest. 2019;49(7):e13124.
Gharios C, Leblebjian M, Mora S, Blumenthal RS, Jaffa MA, Refaat MM. The association of cardiovascular mortality with a first-degree family member history of different cardiovascular diseases. J Geriatr Cardiol JGC. 2021;18(10):816.
Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):1–19.
Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–84.
Poorzand H, Tsarouhas K, Hozhabrossadati SA, Khorrampazhouh N, Bondarsahebi Y, Bacopoulou F, Rezaee R, Jafarzadeh Esfehani R, Morovatdar N. Risk factors of premature coronary artery disease in Iran: a systematic review and meta-analysis. Eur J Clin Investig. 2019;49(7):e13124.
Alshammary AF, Alharbi KK, Alshehri NJ, Vennu V, Ali KI. Metabolic syndrome and coronary artery disease risk: a meta-analysis of observational studies. Int J Environ Res Public Health. 2021;18(4):1773.
Mirzaei M, Mirzaei M, Sarsangi AR, Bagheri N. Prevalence of modifiable cardiovascular risk factors in Yazd inner-city municipalities. BMC Public Health. 2020;20(1):134.
Mirzaei M, Mirzaei M. Agreement between Framingham, IraPEN and non-laboratory WHO-EMR risk score calculators for cardiovascular risk prediction in a large Iranian population. J Cardiovasc Thorac Res. 2020;12(1):20–6.
Mohseni J, Kazemi T, Maleki MH, Beydokhti H. A systematic review on the prevalence of acute myocardial infarction in Iran. Heart Views. 2017;18(4):125–32.
Sarrafzadegan N, Mohammmadifard N. Cardiovascular disease in iran in the last 40 years: prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. Arch Iran Med. 2019;22(4):204–10.
World Health Organization. Cardiovascular diseases (CVDs). https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds). Accessed March 24, 2021.
Lüscher TF. Epidemiology of cardiovascular disease: the new ESC Atlas and beyond, vol. 39. Oxford: Oxford University Press; 2018. p. 489–92.
Touloumi G, Karakosta A, Kalpourtzi N, Gavana M, Vantarakis A, Kantzanou M, Hajichristodoulou C, Chlouverakis G, Trypsianis G, Voulgari PV, et al. High prevalence of cardiovascular risk factors in adults living in Greece: the EMENO National Health Examination Survey. BMC Public Health. 2020;20(1):1665.
Jozwiak J, Studzinski K, Tomasik T, Windak A, Banach M, Investigators L. The prevalence of cardiovascular risk factors and cardiovascular disease among primary care patients in Poland: results from the LIPIDOGRAM2015 study. Eur Heart J. 2020; 41(Supplement_2).
Lee MS, Flammer AJ, Li J, Lennon RJ, Singh M, Holmes DR Jr, Rihal CS, Lerman A. Time-trend analysis on the Framingham risk score and prevalence of cardiovascular risk factors in patients undergoing percutaneous coronary intervention without prior history of coronary vascular disease over the last 17 years: a study from the Mayo Clinic PCI registry. Clin Cardiol. 2014;37(7):408–16.
Nur KRM. Illness perception and cardiovascular health behaviour among persons with ischemic heart disease in Indonesia. Int J Nurs Sci. 2018;5(2):174–80.
Petricek G, Vrcic-Keglevic M, Vuletic GCV, Ozvacic Z, Murgić L. Illness perception and cardiovascular risk factors in patients with type 2 diabetes: cross-sectional questionnaire study. Croat Med J. 2009;50(6):583–93.
Sararoudi R, Motmaen M, Maracy M, Pishghadam E, Kheirabadi G. Efficacy of illness perception focused intervention on quality of life, anxiety, and depression in patients with myocardial infarction. J Res Med Sci. 2016;21(1):125–125.
French DP, Cooper A, Weinman J. Illness perceptions predict attendance at cardiac rehabilitation following acute myocardial infarction: a systematic review with meta-analysis. J Psychosom Res. 2006;61(6):757–67.
Mosleh SM, Almalik MM. Illness perception and adherence to healthy behaviour in Jordanian coronary heart disease patients. Eur J Cardiovasc Nurs. 2016;15(4):223–30.
Parfeni M, Nistor I, Covic A. A systematic review regarding the association of illness perception and survival among end-stage renal disease patients. Nephrol Dial Transpl. 2013;28(10):2407–14.
Ashour A, Al-Smadi A, Tawalbeh L, Alshraifeen A, Al-Rawashdeh S, Gharaibeh B. Do illness perception predict perceived learning needs among patients treated with percutaneous coronary intervention. Dimens Crit Care Nurs. 2020;39(5):251–8.
Yeom H-E, Shin J-W. Mediating effect of stress on the relationship between illness perception and sleep in patients at risk of metabolic syndrome. Korean J Adult Nurs. 2019;31(4):449–59.
Doi-Kanno M, Fukahori H. Predictors of depression in patients diagnosed with myocardial infarction after undergoing percutaneous coronary intervention: a literature review. J Med Dent Sci. 2016;63(2–3):37–43.
Brewer NT, Chapman GB, Brownlee S, Leventhal EA. Cholesterol control, medication adherence and illness cognition. Br J Health Psychol. 2002;7(4):433–47.
Zelber-Sagi S, Bord S, Dror-Lavi G, Smith ML, Towne SD Jr, Buch A, Webb M, Yeshua H, Nimer A, Shibolet O. Role of illness perception and self-efficacy in lifestyle modification among non-alcoholic fatty liver disease patients. World J Gastroenterol. 2017;23(10):1881.
Nie R, Han Y, Xu J, Huang Q, Mao J. Illness perception, risk perception and health promotion self-care behaviors among Chinese patient with type 2 diabetes: a cross-sectional survey. Appl Nurs Res. 2018;39:89–96.
Goldman RE, Parker DR, Eaton CB, Borkan JM, Gramling R, Cover RT, Ahern DK. Patients’ perceptions of cholesterol, cardiovascular disease risk, and risk communication strategies. Ann Fam Med. 2006;4(3):205–12.
Zhou B, Danaei G, Stevens GA, Bixby H, Taddei C, Carrillo-Larco RM, Solomon B, Riley LM, Di Cesare M, Iurilli MLC. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet. 2019;394(10199):639–51.
Peimani M, Nasli-Esfahani E, Sadeghi R. Patients’ perceptions of patient–provider communication and diabetes care: a systematic review of quantitative and qualitative studies. Chronic Illn. 2020;16(1):3–22.
Acknowledgements
This study was financially supported by the Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences (No. 64546). This article was written based on an MS dissertation, registered in Tabriz University of Medical Sciences.
Funding
This study was supported by a fund from the Tabriz University of Medical Sciences. The funding bodies played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
AG and VZ conceived the idea, performed the statistical analysis. AT and NR performed data collection and drafted the manuscript. TO, NA, and VZ contributed their clinical knowledge and reviewed the manuscript. AG reviewed and revised the idea and study design, received the grant. TO helped to edit the manuscript. AG and AT are the guarantors of this work and take all responsibility for this study. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All the participants voluntarily participated in this study and provided written informed consent. The Ethics Committee of the Tabriz University of Medical Sciences approved this study (IR.TBZMED.REC.1399.483). We confirm that all experiments were performed in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Thagizadeh, A., Ghahramanian, A., Zamanzadeh, V. et al. Illness perception and cardiovascular risk factors in patients with myocardial infarction undergoing percutaneous coronary intervention in Iran. BMC Cardiovasc Disord 22, 245 (2022). https://doi.org/10.1186/s12872-022-02684-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02684-9