
Abstract
Background
This study examines the socioeconomic differentials in trends in the prevalence of hypertension and pre-hypertension and hypertension awareness, treatment, and control in rural Southwestern China.
Methods
Two cross-sectional interviews and health examination surveys were administered in rural Yunnan Province, including 6,350 consenting participants in 2009 and 6,359 consenting participants in 2016 (aged ≥ 35 years). Participant demographics, socioeconomic status (SES), and ethnicity, along with information about hypertension awareness, treatment, and control, were collected using similar questionnaires in the two surveys. The participants’ blood pressure levels were also measured.
Results
From 2009 to 2016, the prevalence of hypertension substantially increased from 28.4% to 39.5% (P < 0.01), and awareness and control rose from 42.2 and 25.8% to 53.1 (P < 0.01) and 30.6% (P < 0.05), respectively. Although people with a higher education level also had higher awareness and control rates than the lower education level ones, there were no conspicuous differences in the improvement of awareness and control between publics with different education levels over the 7 years studied. Increases were observed in both rates of awareness and control in people with a high level of income (P < 0.01). However, only the awareness rate increased in participants with a low level of income. Furthermore, the prevalence (P < 0.01) and treatment (P < 0.05) of hypertension were higher in the Han people than in ethnic minorities.
Conclusions
Individual SES has clear associations with trends in the prevalence, awareness, and control of hypertension. Future interventions to improve hypertension prevention and control should be tailored to address individual SES.
Similar content being viewed by others


Background
Hypertension is a widespread and severe public health issue throughout the world. It is also a major independent, progressive hazard for chronic non-communicable diseases (NCDs), specifically for cardiovascular diseases (CVD) with substantial economic and health losses across the globe [1]. The growing prevalence of hypertension can be observed in countries of all income levels [2]. Globally, the prevalence of hypertension increased from 25.9% in 2000 to 31.1% in 2010 [3]. Pre-hypertension, a medium phase between normal blood pressure (BP) and hypertension, is also common in the world and varies by race and region [4]. Studies have shown that individuals with pre-hypertension, particularly the elderly, are prone to developing hypertension [5, 6]. In China, the state hypertension prevalence in people aged ≥ 18 years was 25.2% in 2016, a dramatically increase compared to the prevalence of 5.1% in 1959, 7.7% in 1980, 13.6% in 1991, and 17.6% in 2002 [7].
The global hypertension awareness, treatment, and control increased from 41.4%, 31.8% and 11.7% in 2000 to 46.5%, 36.9% and 13.8% in 2010 [3]. Generally, the rates in awareness, treatment, and control of hypertension are meaningfully higher in developed countries than in developing ones [8, 9]. China has improved hypertension management substantially over the past years. Nevertheless, the rates in awareness, treatment and control for hypertension are remain relatively low (28.9%, 35.3%, and 3.4%, respectively) related to those described in developed countries [10, 11]. Awareness and knowledge of pre-hypertension and hypertension are critical for the prevention and reduction of hypertension, particularly in rural regions where the levels of awareness and treatment are relatively lower [12].
Socioeconomic status (SES) has been found to be related to pre-hypertension and hypertension. Specifically, a lower SES is in connection with a higher risk of pre-hypertension and hypertension [13, 14], regardless of the indicators of SES that are used. However, little is known about the associations between SES and trends in prevalence, awareness, treatment, and control of hypertension all around the world, particularly in rural and ethnic minority areas in China.
China is a multi-ethnic state, in which 56 ethnicities were documented by nation. Yunnan Province was located in Southwestern China, with a population of 47.14 million in 2016. Twenty-five ethnicities dwelling in the area, and 15 are discovered only in Yunnan. The number of ethnic minorities accounts for one-third of the total population in this area. Previous study indicated hypertension prevalence, awareness, treatment, and control were associated with individual SES and varied by ethnic minority group in Yunnan [15]. However, SES differences in trends in hypertension prevalence, awareness, treatment, and control in this particular aim crowd have not been recognized. Hence, the purpose of our study was to uncover the trends in the change in hypertension and pre-hypertension prevalence, and in hypertension awareness, treatment, and control and to investigate their relationships with SES indicators among Southwestern China’s rural population (aged ≥ 35 years) from 2009 to 2016.
Methods
Study area and population
In 2009 and 2016, two community-based, cross-sectional interviews and examination surveys were administered in two rural regions of Yunnan, China. In 2009, we employed a four-stage stratified random sampling method to choose the participants. In phase 1, all of the counties in Yunnan Province were classified into 2 groups, high and low, on the basis of per-capita gross domestic product (GDP). We randomly chosen one county from each of those two groups, for add up to 2 counties. In phase 2, each chosen county was also divided into 3 categories based on per-capita GDP: advantaged, average, or disadvantaged. From each of these 3 categories, one township was randomly chosen, for 6 townships in total. In phase 3, three villages were selected by probability proportional to size (PPS) method from each township. In phase 4 and ending, from the administration in each chosen village, a residents’ list aged 35 years and over was procured. Then, a simple random sampling method was employed to choose eligible persons from each chosen village. In 2016, we employed a uniform four-stage stratified random sampling technique to enable us to choose participants from the two rural regions.
Data collection and measurement
Similar pre-tested questionnaires were employed to assemble data from participants in the two surveys [16]. Both in 2009 and 2016, face-to-face interviews were conducted to each consenting participant by trained interviewers. Information about participants’ demographic characteristics (sex, age, ethnicity, education, and annual household income), diagnosis, treatment, and control of hypertension were converged. The measured BP was documented accompanied by those from the questionnaire.
BP was measured by trained interviewers using standardized mercury sphygmomanometers in 2009 and 2016, and taken from the individuals’ right arm after they rested for as a minimum 5 min in the sitting situation and had not eaten, smoked, or exercised. Three successive BP measurements were obtained following American Heart Association (AHA) recommendations [17]. In our study, we took the mean BP of three readings. To sustain the accuracy of BP results taken by mercury sphygmomanometer, an oscillometer device was used once a week.
Ethics approval
The Ethics Committee at Kunming Medical University authorized our study ahead of the start of the research.
Definition
Based on recommendations in the eighth Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) [18], pre-hypertension was defined in our study as a systolic blood pressure (SBP) of 120–139 mmHg, and/or diastolic blood pressure (DBP) of 80–89 mmHg. Hypertension was established when a person who has a mean SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, and/or currently being on antihypertensive therapy. A former diagnosis of hypertension by a qualified medical institution was also viewed hypertension in our study.
Among individuals with hypertension, awareness was established in our study when an individual had reported a former hypertension diagnosis in a health facility. Treatment was established when antihypertensive therapy in the last 14 days was reported by participants. Moreover, control was established when a person who has a mean SBP < 140 mmHg and DBP < 90 mmHg posttreatment.
Ethnicity was derived from China’s 56 state-recognized ethnicities, and was then classified into two groups in our study: Han Chinese or ethnic minority. Illiterate was defined as a person who has no capability to read with grasp or to write simple sentences. The level of education was then divided into two sets: illiterate and primary (grades 1–6) or higher. Approximate yearly household income was separated into two classifications (low and high), with the median value as the cut off point. Low referred to an approximate yearly household income < $945, and high referred to a yearly household income ≥ $945.
Statistical analysis
We employed SPSS 22.0 software to analyze all data double-entered into an EpiData 3.1. Descriptive analysis methods and the chi-squared test and t-test were computed in this study. The mean values of SBP and DBP were stated as the mean ± standard deviation (\(\overline{x}\) ± s). Counts and percentages were employed to express categorical variables in the study. A chi-squared test was applied to make a comparison on categorical variables between survey years and genders, and the t-test was analyzed continuous variables. We have adjusted the prevalence of hypertension and pre-hypertension, the rates in awareness, treatment, and control of hypertension, with age using a direct standardization technique for the 2010 population aged 35 years and over in China. All of the statistical significance determinations were grounded in two-tailed P values of < 0.05 in the study.
Results
In 2009 and 2016, a total of 6,600 people aged ≥ 35 years were invited in two surveys, of which 6,350 in 2009 and 6,359 in 2016 agreed to participate, yielding a total response rate of 96.2% and 96.3%, respectively.
Table 1 indicates the general features of the participants. Among the study participants in 2009, 48.2% were male and 51.8% were female. In 2016, 49.4% were male and 50.6% were female. There were no valid changes in proportion of males (P = 0.204), mean age (P = 0.154), and proportion of people with a low approximate yearly household income (P = 0.128) between the two survey years. Nevertheless, the rate of illiteracy for females shortened from 50.9% in 2009 to 38.7% in 2016 (P = 0.001). Females had a higher illiteracy rate (P = 0.015) and a higher low approximate yearly household income rate (P = 0.023) than males both in 2009 and 2016.
Table 2 presents the prevalence of pre-hypertension and hypertension in two survey years and SES in rural Yunnan. Over the 7 years studied, from 2009 to 2016, although the prevalence of pre-hypertension did not differ, the hypertension prevalence boosted from 28.4 to 39.5% (P = 0.001), and among the subcategories, the increasing rates existed in sex, ethnicity, level of education, and approximate yearly household income. The prevalence of hypertension in males and in females increased from 27.6% and 28.8% to 39.5% and 39.8%, respectively (P = 0.001 and P = 0.001), and in the Han majority population, it rose from 27.9% to 40.3% (P = 0.001). Moreover, in the illiterate population, it increased from 26.5% to 54.7% (P = 0.001), and in participants with a low approximate yearly household income, it increased from 28.5 to 48.6% (P = 0.001). In both 2009 and 2016, the prevalence of pre-hypertension was higher in male participants than in female individuals (P = 0.012). In 2016, the hypertension prevalence was higher in Han majority population than in ethnicity minority population (P = 0.001), as well as in illiterate population than in their counterparts (P = 0.001). Moreover, the hypertension prevalence was higher in individuals with a low approximate yearly household income than in participants with a high approximate yearly household income (P = 0.001).
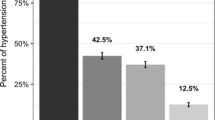
Table 3 shows the hypertension awareness, treatment, and control in two study years and SES in rural areas of Yunnan, China. The hypertension awareness increased from 42.2 to 53.1% (P = 0.001), and control rose from 25.8 to 30.6% (P = 0.026) over the 7 years studied. We found the trends of increase both in males and females, however, only observed in Han majority population and in people with a high level of income. Additionally, the awareness of hypertension also increased in those behind a low level of income. Although the hypertension awareness and control were higher in people who have a higher position in education level than in their counterparts, the improvement in awareness and control did not differ between groups of different education levels over the seven years studied. Further, there was no noteworthy change in treatment among the subcategories layered by sex (P = 0.272), education (P = 0.603), and income (P = 0.358) between in 2009 and in 2016. In both 2009 and 2016, the hypertension awareness and control were higher in females than in males (P = 0.017 and P = 0.033), and the ethnicity minority population had comparatively lower treatment rates than the Han people (P = 0.014).
Discussion
The findings indicated high rates in the prevalence of pre-hypertension and hypertension, relatively low levels in hypertension awareness, treatment, and control, and a total increase in the hypertension prevalence, awareness, and control in rural Southwestern China over the seven years studied. Moreover, the findings also indicated that ethnicity and individual SES have significant relationships with actual hypertension prevalence, awareness, and control, as well as the temporal trends in the hypertension prevalence, awareness, and control.
In the study, the prevalence of pre-hypertension (50.0%) in Yunnan Province was greater than that observed in China and other Asian and low- and middle-income countries [19,20,21,22,23]. The study did not show a growth in the prevalence of pre-hypertension over the 7 years studied. However, it revealed a substantially increasing trend in hypertension prevalence and indicated that hypertension is a chief and increasing public health issue in the regions under study. This possibly results from increasing prevalence rates of obesity (from 6.7% in 2009 to 9.0% in 2016), central obesity (from 43.5% in 2009 to 51.1% in 2016), and diabetes (from 7.7% in 2009 to 9.5% in 2016) in the regions under study, and obesity, central obesity, and diabetes are important contributors to hypertension. The findings suggested that more effective interventions are needed to avoid and control hypertension. Encouragingly, the hypertension awareness, treatment, and control rates (53.1%, 75.7%, and 30.6%, respectively) in 2016 were higher than those found in a national study of China (36.0%, 22.9%, and 5.7%) [24], indicating that hypertension health education programs and improving access to healthcare have helped achieve progress in rural Southwestern China.
The study also showed ethnic differences in temporal trends in hypertension prevalence, and hypertension awareness, treatment, and control in rural Southwestern China. Specifically, the Han people had higher prevalence of hypertension than ethnic minority populations over the seven years studied. One of the reasons might be that ethnic minorities have healthier lifestyles, such as plain food and more activities [25]. In both 2009 and 2016, the treatment rate of hypertension in ethnic minority populations was significantly lower than which in the Han people, which may be attributed to the economically disadvantaged status of the ethnic minority population [26]. Furthermore, only the Han majority population improved the rates in hypertension awareness and control. Thus, specific efforts must be taken in the ethnic minority groups to advance the awareness, treatment, and control of hypertension as well as to improve their economic status and their access to medical services.
In the study population, less educated and low-income individuals were more likely to suffer from hypertension than their more educated and high-income counterparts. This result is consistent with that from previous studies [14, 15, 27]. This possibly due to the fact that less educated individuals had higher prevalence of obesity, central obesity, and diabetes than their more educated counterparts (13.0% vs. 7.0%, 56.4% vs. 43.5%, and 9.7% vs. 6.5%, P < 0.05), while prevalence of obesity and central obesity was higher in low-income individuals than in high-income counterparts (9.5% vs. 8.6% and 51.1% vs. 37.3%, P < 0.05) in this study, and diabetes and being obese or central obese are well recognized established major risk factors for CVD in previous studies. Furthermore, over the seven years we studied, the hypertension prevalence markedly increased in both less educated and low-income people. The interactions of SES and multiple CVD risk factors thereby underscore an urgent need for improving community-based hypertension prevention strategies focused particularly on individuals with low levels of education and income.
In this study, higher rates in awareness and control were found in more educated people than less educated participants in both 2009 and 2016. However, there was no remarkable change in the increase of awareness, treatment, and control between different education levels groups. In particular, the study showed stable treatment rates of hypertension between the two survey years, suggesting that the treatment of hypertension had entered a bottleneck stage in the study region, and novel effective measures should be taken to continue to improve the treatment rate. Although the treatment of hypertension did not differ in groups with diverse education level, the control of hypertension was significantly lower in illiterate groups than in educated groups. The specific reasons need further study.
Although there was a significant increase in awareness between different income groups over the 7 years studied, it only appeared in the high-income group for control. Encouragingly, the study revealed a similar treatment rate of hypertension between low-income participants and their higher-income counterparts both in 2009 and in 2016. Although the low-income participants had equivalent awareness and treatment of hypertension as their higher-income counterparts, the rate of control was dramatically lower in the low-income participants than their counterparts over the 7 years studied. The reasons might be low-income people use incorrect treatment methods or do not adhere to their treatment for a long time [28]. The findings underline an urgent need to improve the control of hypertension for the low-income population.
There were some limitations in the study. First, as the data were collected using a cross-sectional design, we were unable to determine causal relationships. Second, the trends in prevalence, awareness, treatment, and control of hypertension were analyzed based on a seven years study period, which is a relatively short-range time period; to determine whether the trends will persist over a longer time frame, more data will be needed. Third, the study lacked lipid, diet, alcohol, and physical inactivity -related data, and lipid, diet, alcohol and physical inactivity may be important factors influencing hypertension. So the full range of risk factors attributable to hypertension was not captured. Further research is needed to examine the contribution of other risk factors to hypertension in rural southwestern China. Fourth, due to the lack of data on pharmacological treatment/care for multiple cardiovascular risk factors, we did not analyze their interactions with SES.
Conclusions
In conclusion, the study displayed that the prevalence of hypertension as well as hypertension awareness and control significantly increased in rural Southwestern China from 2009 to 2016, with ethnicity and individual SES having clear associations with the trends in prevalence, awareness, and control of hypertension. However, the hypertension treatment did not differ over the 7 years studied. The findings indicated that the policymakers should increase levels of awareness and control to promote the hypertension prevention and management, as well as employ effective interventions that consider socioeconomic disparities.
Availability of data and materials
The datasets used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- AHA:
-
American Heart Association;
- BP:
-
Blood pressure;
- CVD:
-
Cardiovascular diseases;
- DBP:
-
Diastolic blood pressure;
- GDP:
-
Gross domestic product;
- NCDs:
-
Non-communicable diseases;
- PPS:
-
Probability proportional to size;
- SBP:
-
Systolic blood pressure;
- SES:
-
Socioeconomic status
References
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Executive summary: heart disease and stroke statistics–2013 update: a report from the American Heart Association. Circulation. 2013;127:143–52.
Zhou B, Bentham J, Di Cesare M, Bixby H, Danaei G, Cowan MJ, Cho B. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 191 million participants. The Lancet. 2017;389(10064):37–55.
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, Chen J, He J. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–50.
Guo X, Zou L, Zhang X, Li J, Zheng L, Sun Z, Hu J, Wong ND, Sun Y. Prehypertension: a meta-analysis of the epidemiology, risk factors, and predictors of progression. Tex Heart Inst J. 2011;38:643–52.
Kim SJ, Lee J, Nam CM, Jee SH, Park IS, Lee KJ, Lee SY. Progression rate from new-onset pre-hypertension to hypertension in Korean adults. Circ J. 2011;75:135–40.
Zheng L, Sun Z, Zhang X, Xu C, Li J, Hu D, Sun Y. Predictors of progression from prehypertension to hypertension among rural Chinese adults: results from Liaoning Province. Eur J Cardiovasc Prev Rehabil. 2010;17:217–22.
Wang J, Sun W, Wells GA, Li Z, Li T, Wu J, Zhang Y, Liu Y, Li L, Yu Y, Liu Y, Qi C, Lu Y, Liu N, Yan Y, Liu L, Hui G, Liu B. Differences in prevalence of hypertension and associated risk factors in urban and rural residents of the northeastern region of the People’s Republic of China: a cross-sectional study. PLoS ONE. 2018;13:e195340.
Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief. 2013:1–8.
Abdul-Razak S, Daher AM, Ramli AS, Ariffin F, Mazapuspavina MY, Ambigga KS, Miskan M, Abdul-Hamid H, Mat-Nasir N, Nor-Ashikin MN, Ng KK, Nawawi H, Yusoff K. Prevalence, awareness, treatment, control and socio demographic determinants of hypertension in Malaysian adults. BMC Public Health. 2016;16:351.
Zhao L, Sun W, Wang J, Wu J, Zhang Y, Liu Y, Liu B. Differences in the treatment and control of hypertension in urban and rural residents of the northeastern region of the People’s Republic of China: a cross-sectional study. Clin Exp Hypertens. 2019;41:366–72.
Wang Y, Peng X, Nie X, Chen L, Weldon R, Zhang W, Xiao D, Cai J. Burden of hypertension in China over the past decades: Systematic analysis of prevalence, treatment and control of hypertension. Eur J Prev Cardiol. 2016;23:792–800.
Htet AS, Bjertness MB, Oo WM, Kjøllesdal MK, Sherpa LY, Zaw KK, Ko K, Stigum H, Meyer HE, Bjertness E. Changes in prevalence, awareness, treatment and control of hypertension from 2004 to 2014 among 25–74-year-old citizens in the Yangon Region. Myanmar BMC Public Health. 2017;17:847.
Zhang R, Deng R, Shen P, Fan M, Leng B, Zhou Y, Cui Y, Li G. Prehypertension and socioeconomic status: a cross-sectional study in Chongqing. China Clin Exp Hypertens. 2017;39:774–80.
Leng B, Jin Y, Li G, Chen L, Jin N. Socioeconomic status and hypertension: a meta-analysis. J Hypertens. 2015;33:221–9.
Cai L, Dong J, Cui WL, You DY, Golden AR. Socioeconomic differences in prevalence, awareness, control and self-management of hypertension among four minority ethnic groups, Na Xi, Li Shu, Dai and Jing Po, in rural southwest China. J Hum Hypertens. 2017;31:388–94.
Li HF, Cai L, Golden AR. Short-term trends in economic burden and catastrophic costs of type 2 diabetes mellitus in rural southwest China. J Diabetes Res. 2019;2019:9626413.
Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Jones DW, Kurtz T, Sheps SG, Roccella EJ. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension. 2005;45:142–61.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SJ, Svetkey LP, Taler SJ, Townsend RR, Wright JJ, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–20.
Chen C, Yuan Z. Prevalence and risk factors for prehypertension and hypertension among adults in Central China from 2000–2011. Clin Exp Hypertens. 2018;40:734–43.
Afsargharehbagh R, Rezaie-Keikhaie K, Rafiemanesh H, Balouchi A, Bouya S, Dehghan B. Hypertension and pre-hypertension among iranian adults population: a meta-analysis of prevalence, awareness, treatment, and control. Curr Hypertens Rep. 2019;21:27.
Wu J, Li T, Song X, Sun W, Zhang Y, Liu Y, Li L, Yu Y, Liu Y, Qi C, Liu B. Prevalence and distribution of hypertension and related risk factors in Jilin Province, China 2015: a cross-sectional study. BMJ Open. 2018;8:e20126.
Meiqari L, Essink D, Wright P, Scheele F. Prevalence of hypertension in vietnam: a systematic review and meta-analysis. Asia Pac J Public Health. 2019;31:101–12.
Sarki AM, Nduka CU, Stranges S, Kandala NB, Uthman OA. Prevalence of hypertension in low- and middle-income countries: a systematic review and meta-analysis. Medicine (Baltimore). 2015;94:e1959.
Lu J, Lu Y, Wang X, Li X, Linderman GC, Wu C, Cheng X, Mu L, Zhang H, Liu J, Su M, Zhao H, Spatz ES, Spertus JA, Masoudi FA, Krumholz HM, Jiang L. Prevalence, awareness, treatment, and control of hypertension in China: data from 1·7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet. 2017;390:2549–58.
Ruixing Y, Qiming F, Dezhai Y, Shuquan L, Weixiong L, Shangling P, Hai W, Yongzhong Y, Feng H, Shuming Q. Comparison of demography, diet, lifestyle, and serum lipid levels between the Guangxi Bai Ku Yao and Han populations. J Lipid Res. 2007;48:2673–81.
Cai L, Wang XM, Fan LM, Shen JR, Liu YN, Golden AR. Socioeconomic variations in chronic obstructive pulmonary disease prevalence, diagnosis, and treatment in rural Southwest China. BMC Public Health. 2020;20:536.
Wang Q, Shen JJ, Frakes K. Limited contribution of health behaviours to expanding income-related chronic disease disparities based on a nationwide cross-sectional study in China. Sci Rep. 2018;8:12485.
Kunz M, Lauder L, Ewen S, Bohm M, Mahfoud F. The current status of devices for the treatment of resistant hypertension. Am J Hypertens. 2020;33:10–8.
Acknowledgements
None.
Funding
The present study was supported by grant from the National Natural Science Fund of China (Grant numbers: 72064026, 71663035), Program for Innovative Research Team of Yunnan Province (202005AE160002), and Program for Innovative Research Team (in Science and Technology) in University of Yunnan Province ((2018)134). The funders had no role in study design, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
LC conceptualized the research idea and revised the manuscript. LMF participated in the study and drafted the manuscript. FW, MZ, and WLC contributed to the study design, collected the data, and provided comments on the paper during the writing process. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee at Kunming Medical University prior to the start of the research. Written informed consent was obtained from all participants in our study, and the Ethics Committee at Kunming Medical University approved this consent procedure.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fan, LM., Wang, F., Zhao, M. et al. Socioeconomic differentials in trends in the prevalence of hypertension and pre-hypertension and hypertension awareness, treatment, and control in rural Southwestern China. BMC Cardiovasc Disord 21, 259 (2021). https://doi.org/10.1186/s12872-021-02062-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-021-02062-x