
Abstract
Background
Although serum creatinine concentration has been traditionally used as an index of renal function in clinical practice, it is considered relatively inaccurate, especially in patients with mild renal dysfunction. This study investigated the usefulness of preoperative estimated glomerular filtration rate (eGFR) in predicting complications after cardiovascular surgery in patients with normal serum creatinine concentrations.
Methods
This study included 2208 adults undergoing elective cardiovascular surgery. Preoperative eGFR was calculated using Chronic Kidney Disease Epidemiology Collaboration equations. The relationships between preoperative eGFR and 90 day postoperative composite major complications were analyzed, including 90 day all-cause mortality, major adverse cardiac and cerebrovascular events, severe acute kidney injury, respiratory and gastrointestinal complications, wound infection, sepsis, and multi-organ failure.
Results
Of the 2208 included patients, 185 (8.4%) had preoperative eGFR < 60 mL/min/1.73 m2 and 328 (14.9%) experienced postoperative major complications. Multivariable logistic regression analyses showed that preoperatively decreased eGFR was independently associated with an increased risk of composite 90 day major postoperative complications (adjusted odds ratio: 1.232; 95% confidence interval [CI]: 1.148–1.322; P < 0.001). eGFR was a better discriminator of composite 90 day major postoperative complications than serum creatinine, with estimated c-statistics of 0.724 (95% CI: 0.694–0.754) for eGFR and 0.712 (95% CI: 0.680–0.744) for serum creatinine (P = 0.008).
Conclusions
Decreased eGFR was significantly associated with an increased risk of major complications after cardiovascular surgery in patients with preoperatively normal serum creatinine concentrations.
Similar content being viewed by others


Background
Several studies have demonstrated that the risk of postoperative complications and mortality is higher in patients with preoperative renal dysfunction than in those with normal renal function [1,2,3,4,5,6]. Thus, correct identification of preoperative renal function may be important in predicting the prognosis of patients undergoing cardiovascular surgery.
Serum creatinine (sCr) concentration has been regarded as an index of renal function in clinical practice [7], as well as being a component of several perioperative risk prediction models [8, 9]. However, because sCr level can be influenced not only by its renal excretion, but by other factors, including age, gender, ethnicity, muscle mass, and diet, it may remain within a normal range, even in patients with significant renal dysfunction [10, 11]. Estimated glomerular filtration rate (eGFR) has been reported to be a more useful measure than sCr in detecting and evaluating renal dysfunction and in predicting postoperative outcomes [1, 3, 4, 11,12,13,14]. Of several equations developed to calculate eGFR so far, the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is known to be more accurate and precise than the other equations in estimating GFR, especially in people with high GFR levels [15, 16]. Thus, the 2012 Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines recommend using the CKD-EPI equation to estimate GFR [17]. To our knowledge, however, no study to date has shown that eGFR calculated using the CKD-EPI equation can predict the prognosis of patients with normal sCr undergoing cardiovascular surgery. This study therefore assessed whether eGFR calculated using the CKD-EPI equation can predict major complications and mortality within 90 days after surgery in patients with normal sCr (< 1.4 mg/dl) undergoing cardiovascular surgery.
Methods
Study design, participants
All patients aged ≥20 years who underwent cardiovascular surgery in a tertiary hospital in South Korea between July 2012 and July 2015 were included. All baseline demographic and perioperative clinical information were obtained from the Asan Medical Center Cardiovascular Surgery and Anesthesia Database and from a retrospective review of the computerized patient record system (Asan Medical Center Information System Electronic Medical Record), as described [18]. Patients who had undergone preoperative dialysis, those without preoperative sCr measurements, and patients with preoperative sCr concentrations > 1.4 mg/dL (i.e., the upper limit of the normal range at our institution and considered abnormal) were excluded. Also excluded were patients who had undergone emergency or urgent surgery, those with a preoperative intra-aortic balloon pump or ventricular assist device support, and those who underwent endovascular aortic repair surgery. This retrospective study was performed according to the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology [19] and was approved by the Institutional Review Board of Asan Medical Center (AMC IRB 2017–0593), which waived the requirement for written informed consent because of the observational nature of the study.
Definitions of variables
The primary outcome was a composite of major complications within 90 days after surgery, including 1) death, 2) a major adverse cardiovascular or cerebrovascular event (MACCE), 3) pulmonary complications, 4) renal complications, 5) wound complications, 6) gastrointestinal complications, 7) sepsis, or 8) multi-organ failure. A patient who experienced more than one of these events was counted only once in the composite outcome. Major complications within 90 days after surgery were defined according to the European Perioperative Clinical Outcome definitions or as previously reported [20,21,22]. Mortality was defined as death from any cause within 90 days of primary cardiovascular surgery. Major adverse cardiovascular or cerebrovascular events included myocardial infarction, malignant ventricular arrhythmia, cardiac dysfunction, and ischemic or hemorrhagic stroke. Pulmonary complications included pneumonia of any cause, acute respiratory distress syndrome, and respiratory failure requiring mechanical ventilation for more than 48 h. Renal complications included severe acute kidney injury (KDIGO stage ≥ 2, i.e., an increase in sCr to ≥ 2.0 times that of the baseline value within 7 days of surgery) and the need for renal replacement therapy. For the diagnosis of severe acute kidney injury, urine output was not used due to incomplete recording and possible effects of diuretic use. Wound complications included surgical site infection, wound dehiscence, and mediastinitis. Gastrointestinal complications included gastrointestinal hemorrhage, mesenteric ischemia, pancreatitis, and hepatic failure. Secondary outcomes included the incidence of specific individual complications of the primary outcome and composite 30-day postoperative major complications. Data regarding postoperative morbidity and mortality were obtained from visiting outpatient clinics, by a detailed review of all medical records, by telephone interviews, or from the National Population Registry of the Korean National Statistical Office.
Preoperative renal function was assessed using both sCr and eGFR. sCr concentration was routinely checked preoperatively and daily until 3 days after surgery (upon arrival at the ICU, and at 1, 2, and 3 days after surgery); however, after 3 days postoperatively, sCr concentration was ordered at clinician (surgeon or intensive care physician) discretion until hospital discharge. The preoperative sCr concentration was defined as that measured closest to the time of surgery (but within 30 days of surgery). sCr concentration was measured using the kinetic Jaffe method (Cobas® 8000 modular analyzer series; Roche Diagnostics GmbH, Vienna, Austria) which was traceable to standardized reference method (isotope dilution mass spectrometry). Preoperative eGFR was calculated using the CKD-EPI equation (eGFR = 141 × min(sCr/κ, 1)α × max(sCr/κ, 1)− 1.209 × 0.993age × 1.018 (if female) × 1.159 (if black), where κ is 0.7 for females and 0.9 for males, α is − 0.329 for females and − 0.411 for males, min indicates the minimum of sCr/κ or 1, and max indicates the maximum of sCr/κ or 1) [15].
Statistical analysis
As this study was conducted for exploratory purposes, minimum sample size was not calculated and all included patients were analyzed. Categorical variables are presented as numbers and percentages, and continuous variables as mean ± standard deviation or median and interquartile range.
The unadjusted relationship between preoperative eGFR and composite 90-day postoperative major complications was analyzed using descriptive statistics, logistic regression, and receiver operating characteristic (ROC) curve analysis. Preoperative eGFR was analyzed as both a continuous variable and as a categorical variable, arbitrarily classified into groups with eGFR < 60, 60–74, 75–89, 90–104, and ≥ 105 mL/min/1.73 m2. Although categorization may be simple and attractive from the perspective of decision making, arbitrary classification may result in loss of information. Therefore, restricted cubic spines were adapted as an alternative for more flexible description of their relationship.
The independent associations between preoperative eGFR and composite 90-day postoperative major complications were evaluated using multivariable logistic regression analyses. In addition to preoperative renal function, all preoperative variables in Table 1 were assessed independently, and variables with a P value < 0.20 in the univariate analyses were entered into the multivariable analyses. A backward elimination process with a P value cutoff of 0.05 was used to develop the final multivariable models. Additionally, univariate and multivariate analyses were conducted to evaluate the relationships between preoperative eGFR and the secondary outcome variables. Adjusted odds ratio (OR) with 95% confidence interval (CI) for the logistic regression were calculated. Model discrimination and calibration were measured using c-statistics and Hosmer-Lemeshow statistics, respectively.
The abilities of preoperative eGFR and preoperative sCr, both assessed as continuous variables, to predict composite 90-day postoperative major complications were compared. For this, c-statistics (equivalent to the area under the ROC curve [AUC]) for each final multivariable logistic regression model, each with eGFR or sCr separately, were calculated. To evaluate the discrimination ability of preoperative eGFR and sCr for predicting composite 90-day postoperative major complications, the adjusted AUCs (i.e., the c-statistics) with 95% CIs were compared using method of comparing areas based on correlated U statistics described by Delong et al. [23].
All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and IBM SPSS Statistics 21.0 (IBM Corp., Armonk, NY, USA) software. All reported P values were two-sided, with P < 0.05 considered statistically significant.
Results
During the study period, 2818 patients underwent cardiovascular surgery. After excluding 610 patients who met exclusion criteria, a total of 2208 patients were analyzed (Fig. 1). The baseline and intraoperative characteristics of the study population are shown in Table 1. Mean patient age was 60.0 ± 12.8 years, 59.1% were male, and mean preoperative sCr was 0.9 ± 0.2 mg/dL and mean preoperative eGFR was 86.3 ± 17.6 mL/min/1.73 m2 (Additional file 1: Table S1). Of the 2208 patients, 185 (8.4%) were found to have occult renal dysfunction (eGFR < 60 mL/min/1.73 m2), with the latter more likely in elderly than in younger patients and in women than in men. Despite strong negative correlations between sCr and eGFR in both males (Pearson correlation coefficient R = − 0.860; P < 0.001) and females (R = − 0.892; P < 0.001), the range of eGFR values among patients with low sCr was wide (Additional file 1: Figure S1).

Flow diagram of the study, showing patients included and excluded. sCr = serum creatinine, IABP = intra-aortic balloon pump, VAD = ventricular assist device
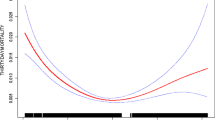
Composite 30-day and 90-day postoperative major complications occurred in 296 (13.4%) and 328 patients (14.9%), respectively (Additional file 1: Table S2). Classification of the study population into five eGFR categories showed that the incidence of composite 90-day postoperative major complications increased from higher to lower eGFR categories (Fig. 2a). Similarly, when restricted cubic splines and logistic regression were used to analyze the relationship between eGFR as a continuous variable and composite 90-day postoperative major complications, an inverse relationship was observed (Fig. 2b). In addition, the 30-day and 90-day mortality, major adverse cardiovascular or cerebrovascular event, pulmonary, and renal complication rates increased from higher to lower eGFR categories, with all being particularly high in patients with eGFR < 60 mL/min/1.73 m2 (Fig. 3 and Additional file 1: Figure S2).

Relationship between preoperative eGFR and composite 90 day postoperative major complications as evaluated by (a) descriptive statistics and (b) logistic regression analysis. The 95% confidence intervals are denoted by error bars in a and bands around the regression line in b. eGFR = estimated glomerular filtration rate

Effects of preoperative eGFR on the rates of 90-day (a) mortality, (b) MACCE, (c) pulmonary complications, and (d) renal complications after cardiovascular surgery. eGFR = estimated glomerular filtration rate; MACCE = major adverse cardiovascular and cerebrovascular event
Unadjusted univariate analyses showed that factors significantly associated with composite 90-day postoperative major complication rates included patient age; body mass index; logistic EuroSCORE; sCr concentration; eGFR; hematocrit; concentrations of total bilirubin, serum albumin, uric acid, and C-reactive protein; left ventricular ejection fraction; congestive heart failure; peripheral vascular disease; liver disease; dyslipidemia; current smoker; and preoperative use of an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and of diuretics and insulin. All these variables were incorporated into full multivariable logistic regression model (Table 2). Using the backward elimination method of multivariable logistic regression model, with the pre-specified significance level for removing and keeping factors in the model set to 0.05, the following parameters showed independent and significant associations with an increased risk of developing composite 90-day postoperative major complications (Table 2): peripheral vascular disease, current smoker, preoperative eGFR, hematocrit levels, serum total bilirubin levels, albumin levels, and preoperative use of diuretics.
Multivariable logistic regression analyses showed that preoperatively decreased eGFR was independently associated with increased risk of composite 90-day postoperative major complications, with a 23% increased risk for each 10 mL/min/1.73 m2 reduction in eGFR (OR: 1.232; 95% CI: 1.148–1.322; P < 0.001). Compared with patients with preoperative eGFR ≥105 mL/min/1.73 m2, those in the lower eGFR categories, with eGFR < 60 mL/min/1.73 m2 (OR: 4.476; 95% CI: 2.542–7.883; P < 0.001), eGFR 60–74 mL/min/1.73 m2 (OR: 2.514; 95% CI: 1.482–4.264; P = 0.001), eGFR 75–89 mL/min/1.73 m2 (OR: 2.225; 95% CI: 1.336–3.706; P = 0.002), and eGFR 90–104 mL/min/1.73 m2 (OR: 1.687; 95% CI: 1.011–2.815; P = 0.045), were at significantly increased risk of composite 90-day postoperative major complications. In additional analyses with secondary outcome variables, similar results were obtained (Table 3).
Although sCr was also effective for the prediction of composite 90-day postoperative major complications (OR: 3.871; 95% CI: 2.147–6.979; P < 0.001), eGFR was more accurate, as shown by their adjusted AUCs of 0.724 (95% CI: 0.694–0.754) for eGFR and 0.712 (95% CI: 0.680–0.744) for sCr (P = 0.008).
Discussion
This retrospective observational study of 2208 patients who underwent cardiovascular surgery found that, even if sCr concentration is normal, GFR estimated by the CKD-EPI equation is a significant predictor of composite 90-day postoperative major complications and that this relationship is maintained despite adjustment for potential confounding variables. Furthermore, eGFR as a measure of renal function showed greater accuracy than sCr concentrations in multivariable risk models predicting composite 90-day postoperative major complications.
Regardless of how it is measured, renal dysfunction is an important predictor of postoperative adverse outcomes [3, 5, 7]. Previous studies, however, have found that assessing renal function only by dichotomized sCr levels may underestimate renal dysfunction, as sCr can be normal in patients with impaired renal function [10, 11]. Indeed, studies have shown that patients with normal sCr levels may have renal dysfunction that may affect postoperative outcome [1, 2, 12, 13]. For example, a study of 4603 patients with normal sCr undergoing cardiac surgery found that 565 (12.3%) had creatinine clearance, as estimated by the Cockroft-Gault equation, of < 60 mL/min/1.73 m2, which was related to increased risks of renal failure requiring dialysis, mortality, and major morbidity [1]. Another study showed that 13% of patients with normal sCr had estimated creatinine clearance < 60 mL/min/1.73 m2, which was associated with a nearly 3-fold increase in the risk of renal replacement therapy after cardiac surgery [12]. A third report found that 706 (8.2%) of 8562 patients with normal sCr had estimated creatinine clearance < 60 mL/min/1.73 m2, which was associated with higher risks for mortality and prolonged hospital stay after coronary artery bypass surgery [13]. More recently, a study found that approximately 40% of 9159 patients with normal sCr levels undergoing coronary artery bypass surgery had estimated creatinine clearance < 60 mL/min/1.73 m2 and that this factor was an independent predictor of mortality, renal dysfunction, dialysis, stroke, arrhythmia, and prolonged hospital stay [2]. Consistent with these previous reports, our study found that 8.4% of patients with normal sCr levels had eGFR < 60 mL/min/1.73 m2 and that this factor was significantly associated with an increased risk of composite 90-day postoperative major complications.
Thus, the results of our analyses confirm and extend the observations of previous studies that using eGFR with sCr rather than sCr alone may be more beneficial in clinical practice. Our study suggests that clinicians should use eGFR for evaluating preoperative renal function in patients undergoing cardiovascular surgery instead of relying on sCr value alone and that patients with occult renal dysfunction (eGFR < 60 mL/min/1.73 m2 despite having normal sCr values) should be considered as having clinically significant renal dysfunction linked to poor postoperative outcomes. In addition, the incorporation of this strategy in the preoperative assessment would facilitate the identification of high-risk patients who could remain unrecognized by clinicians when relying on sCr abnormalities alone to identify renal dysfunction and would provide better risk stratification that can help optimize monitoring and care strategies during the perioperative period.
In contrast to previous studies, which used the Cockroft-Gault equation to calculate eGFR, our study used the CKD-EPI equation. Although the Cockroft-Gault equation has been still used to determine the level of renal function, the CKD-EPI equation has been reported to be superior to the Cockroft-Gault equation in terms of eGFR accuracy and classification in several populations, particularly those with preserved renal function [24]. Moreover, the KDIGO clinical practice guidelines recommend using the sCr-based CKD-EPI equation for detecting and determining the severity of renal dysfunction, and for assessing the effects of treatment [17]. Because most of our patients had high eGFR levels, the use of the CKD-EPI equation to estimate GFR may strengthen the reliability of our findings. Our study also showed an inverse relationship between eGFR and the incidence of composite 90-day postoperative major complications, even when eGFR was greater than 60 mL/min/1.73 m2. Additionally, in agreement with previous studies [1, 12,13,14], our study showed that eGFR had a greater sensitivity than sCr in predicting postoperative outcomes. Taken together, these findings suggest that GFR estimated by the CKD-EPI equation may be useful for identifying patients with renal dysfunction undergoing cardiovascular surgery among patients thought to have preoperative normal renal function based on low sCr alone.
There are several limitations to be considered in the interpretation of our results. First, although our analyses included many variables, the retrospective and observational nature of this study may have masked hidden or unknown factors that may have influenced our results. Second, although the CKD-EPI equation has the highest accuracy in estimating GFR, GFR was not directly measured using any reference method or markers of kidney damage, including albuminuria. Thus, we cannot definitively conclude that actual preoperative renal function is directly associated with postoperative outcomes. Third, even though strenuous efforts have been made to achieve complete follow-up for all patients and to make our database as complete as possible, it is almost impossible to achieve 100% follow-up of all eligible subjects in a large-cohort study. Thus, in this study, we cannot completely rule out the possibility that complications suffered after discharge that were managed in primary care or local hospitals were missed, which may weaken the validity of our study. Accordingly, our results should be interpreted with caution. Finally, this was a single-center study and almost exclusively included Korean patients. Indeed, the CKD-EPI equation used to estimate GFR in this study was developed in a population comprising 99% Westerners (62% Caucasians, 32% African–Americans, and 5% Hispanics) and only 1% Asians [15], and its validity in Koreans and other Asian populations needs to be established. However, recent studies conducted in Asia on validating or establishing GFR estimating equations showed that the original CKD-EPI equation could be valid for evaluating the Korean and multiethnic Asian populations [25,26,27]. However, because we cannot completely exclude the possibility that the effect of race and ethnicity on estimating GFR could have influenced the results of this study, caution should be exercised in generalizing these results to centers with different patient populations.
Conclusion
In conclusion, eGFR calculated using the CKD-EPI equation was significantly associated with composite 90-day postoperative major complications and has a significant advantage over sCr as a predictor of major complications after cardiovascular surgery in patients with normal sCr. These findings suggest that accurately assessing preoperative renal function by calculating eGFR in addition to measuring sCr may better identify patients at high risk for major complications after cardiovascular surgery and may be better for risk stratification.
Availability of data and materials
All data are available from the corresponding author upon reasonable request.
Abbreviations
- AUC:
-
Areas under the ROC curve
- CI:
-
Confidence interval
- CKD-EPI:
-
Chronic Kidney Disease Epidemiology Collaboration
- eGFR:
-
Estimated glomerular filtration rate
- KDIGO:
-
Kidney Disease Improving Global Outcomes
- OR:
-
Odds ratio
- ROC:
-
Receiver operating characteristic
- sCr:
-
Serum creatinine
References
Wang F, Dupuis JY, Nathan H, Williams K. An analysis of the association between preoperative renal dysfunction and outcome in cardiac surgery: estimated creatinine clearance or plasma creatinine level as measures of renal function. Chest. 2003;124:1852–62.
Miceli A, Bruno VD, Capoun R, Romeo F, Angelini GD, Caputo M. Occult renal dysfunction: a mortality and morbidity risk factor in coronary artery bypass grafting surgery. J Thorac Cardiovasc Surg. 2011;141:771–6.
Mooney JF, Ranasinghe I, Chow CK, et al. Preoperative estimates of glomerular filtration rate as predictors of outcome after surgery: a systematic review and meta-analysis. Anesthesiology. 2013;118:809–24.
AbuRahma AF, Alhalbouni S, Abu-Halimah S, Dean LS, Stone PA. Impact of chronic renal insufficiency on the early and late clinical outcomes of carotid artery stenting using serum creatinine vs glomerular filtration rate. J Am Coll Surg. 2014;218:797–805.
Prowle JR, Kam EP, Ahmad T, Smith NC, Protopapa K, Pearse RM. Preoperative renal dysfunction and mortality after non-cardiac surgery. Br J Surg. 2016;103:1316–25.
Cohen JS, Gu A, Wei C, et al. Preoperative estimated glomerular filtration rate is a marker for postoperative complications following revision total knee arthroplasty. J Arthroplast. 2018.
Bernardi MH, Schmidlin D, Schiferer A, et al. Impact of preoperative serum creatinine on short- and long-term mortality after cardiac surgery: a cohort study. Br J Anaesth. 2015;114:53–62.
Roques F, Michel P, Goldstone AR, Nashef SA. The logistic EuroSCORE. Eur Heart J. 2003;24:881–2.
Gupta PK, Gupta H, Sundaram A, et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation. 2011;124:381–7.
Duncan L, Heathcote J, Djurdjev O, Levin A. Screening for renal disease using serum creatinine: who are we missing? Nephrol Dial Transplant. 2001;16:1042–6.
Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function--measured and estimated glomerular filtration rate. N Engl J Med. 2006;354:2473–83.
Wijeysundera DN, Karkouti K, Beattie WS, Rao V, Ivanov J. Improving the identification of patients at risk of postoperative renal failure after cardiac surgery. Anesthesiology. 2006;104:65–72.
Najafi M, Goodarzynejad H, Karimi A, et al. Is preoperative serum creatinine a reliable indicator of outcome in patients undergoing coronary artery bypass surgery? J Thorac Cardiovasc Surg. 2009;137:304–8.
Cywinski JB, Mascha EJ, Kurz A, Sessler DI. Estimated glomerular filtration rate better predicts 30-day mortality after non-cardiac surgery than serum creatinine: a retrospective analysis of 92,888 patients. Can J Anaesth. 2015;62:745–52.
Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12.
Levey AS, Stevens LA. Estimating GFR using the CKD epidemiology collaboration (CKD-EPI) creatinine equation: more accurate GFR estimates, lower CKD prevalence estimates, and better risk predictions. Am J Kidney Dis. 2010;55:622–7.
Levin A, Stevens PE. Summary of KDIGO 2012 CKD guideline: behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014;85:49–61.
Joung KW, Jo JY, Kim WJ, et al. Association of preoperative uric acid and acute kidney injury following cardiovascular surgery. J Cardiothorac Vasc Anesth. 2014;28:1440–7.
von Elm E, Altman DG, Egger M, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335:806–8.
Lee EH, Chin JH, Choi DK, et al. Postoperative hypoalbuminemia is associated with outcome in patients undergoing off-pump coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth. 2011;25:462–8.
Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European perioperative clinical outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32:88–105.
Hansen MS, Petersen EE, Dahl JB, Wetterslev J. Post-operative serious adverse events in a mixed surgical population - a retrospective register study. Acta Anaesthesiol Scand. 2016;60:1209–21.
Delong ER, Delong DM, Clarkepearson DI. Comparing the areas under 2 or more correlated receiver operating characteristic curves - a nonparametric approach. Biometrics. 1988;44:837–45.
Botev R, Mallie JP, Wetzels JF, Couchoud C, Schuck O. The clinician and estimation of glomerular filtration rate by creatinine-based formulas: current limitations and quo vadis. Clin J Am Soc Nephrol. 2011;6:937–50.
Teo BW, Koh YY, Toh QC, et al. Performance of the CKD-EPI creatinine-cystatin C glomerular filtration rate estimation equations in a multiethnic Asian population. Singap Med J. 2014;55:656–9.
Jeong TD, Lee W, Yun YM, Chun S, Song J, Min WK. Development and validation of the Korean version of CKD-EPI equation to estimate glomerular filtration rate. Clin Biochem. 2016;49:713–9.
Teo BW, Zhang L, Guh JY, et al. Glomerular filtration rates in Asians. Adv Chronic Kidney Dis. 2018;25:41–8.
Acknowledgements
We would like to thank Hwa Jung Kim, PhD, from the Department of Clinical Epidemiology and Biostatistics of Asan Medical Center for professional help with the statistical analyses.
Funding
This study was supported by a grant (Grant Number: 2016–7023) from the Asan Institute for Life Sciences, Asan Medical Centre, Seoul, Korea.
Author information
Authors and Affiliations
Contributions
MSJ participated in data selection, data analysis, and drafting of the manuscript. JSN participated in data analysis and drafting of the manuscript. JYJ contributed to the interpretation of data and drafting of the manuscript. CHK performed the statistical analyses and contributed to drafting of the manuscript. SAR participated in the design of the study and revising the manuscript. EHL participated in the design of the study, the statistical analysis, and revising the manuscript. ICC participated in the design of the study and revising the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Asan Medical Center (AMC IRB 2017–0593). Informed consent was waived by the AMC IRB.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Baseline and perioperative characteristics of the patient population. Table S2. Postoperative 30-day and 90-day complications. Figure S1. Correlation between preoperative serum creatinine concentration and eGFR calculated by the Chronic Kidney Disease Epidemiology Collaboration equation (R = –0.860, P < 0.001 in males; R= –0.892, P < 0.001 in females). eGFR = estimated glomerular filtration rate. Figure S2. Effects of preoperative eGFR on rates of 90 day (A) mortality, (B) MACCE, (C) pulmonary complications, and (D) renal complications (D) after cardiovascular surgery. eGFR = estimated glomerular filtration rate; MACCE = major adverse cardiovascular and cerebrovascular event. (PDF 464 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Jang, MS., Nam, JS., Jo, JY. et al. The relationship of preoperative estimated glomerular filtration rate and outcomes after cardiovascular surgery in patients with normal serum creatinine: a retrospective cohort study. BMC Anesthesiol 19, 88 (2019). https://doi.org/10.1186/s12871-019-0763-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-019-0763-1