
Abstract
Background
The purpose of this study was to compare the efficacy and safety of dexmedetomidine versus remifentanil for sedation during awake intubation using a Shikani optical stylet (SOS).
Methods
Sixty-eight patients with cervical trauma or severe cervical spondylosis undergoing cervical spinal surgery were enrolled in this prospective study. They were randomly assigned to receive dexmedetomidine (Group D) or remifentanil (Group R). In Group D, the patients received an intravenous loading dose of dexmedetomidine 1 μg · kg−1 over 10 min followed by a continuous infusion of 0.7 μg · kg−1 · h−1. In Group R, a target-controlled infusion of remifentanil was administered to achieve a plasma concentration of 2.5 ng · ml−1, increased to 3 ng · ml−1 10 min later. An endotracheal tube was inserted using a SOS under dexmedetomidine or remifentanil sedation after topical anesthesia to the airway. Midazolam was given as rescue sedation. We recorded the first attempt intubation success rate, the dose of midazolam, duration of intubation, Ramsay Sedation Scale (RSS) score, tracheal tube tolerance score, duration of drug infusion, adverse events and patient satisfaction score.
Results
The RSS score was significantly higher in Group D than in Group R. First attempt success rate, rescue midazolam dose and the duration of intubation did not differ between the groups. Patients in Group R were significantly more tolerant of the tracheal tube. The incidence of hypoxia was significantly higher in Group R than Group D, but there was no significant difference in the incidence of other adverse events between the groups. The hemodynamic responses of the two groups were similar, but more patients in Group R were able to recall airway instrumentation.
Conclusions
Both dexmedetomidine and remifentanil are effective sedatives for awake intubation using an SOS. Although the first attempt success rates were similar, patients sedated with remifentanil tolerated the tracheal tube better after intubation with moderately increased risk of desaturation.
Trial registration
www.chictr.org.cn; ChiCTR-TRC-13003052 (February 4th, 2013).
Similar content being viewed by others


Background
The Shikani optical stylet™ (SOS; Clarus Medical, Minneapolis, MN, USA) is a rigid but malleable stylet with fiberoptic rods and a lens. The SOS is an effective means of managing patients with a difficult airway [1–6]. Compared with a Macintosh laryngoscope, use of a SOS reportedly reduces cervical spine movement during intubation [7], suggesting that it might reduce the risk of spinal cord injury during instrumentation of the airway in patients with a potential or documented cervical spine injury.
The SOS is most often used to intubate patients under general anesthesia. Awake intubation using the SOS in a patient with a difficult airway has been reported in two cases [3, 8]. The best means of providing sedation in awake SOS intubation has not yet been established. Sedation is one of the key elements for successful awake intubation. Intravenous midazolam, propofol and remifentanil are commonly used as sedatives for awake fiberoptic endoscope intubation (AFOI), and there have been recent reports of the safe and effective use of dexmedetomidine [9–14]. Dexmedetomidine is a highly selective α2 adrenoceptor agonist that acts as a sedative, analgesic and a moderate antisialagogue without respiratory depression, suggesting that it could be a suitable drug for facilitating awake intubation. Previous studies have demonstrated that dexmedetomidine is superior to midazolam [13], fentanyl [15], propofol [16] and sufentanil [17] in AFOI. Two studies compared dexmedetomidine with remifentanil for AFOI, but their results were contradictory [9, 10].
The sedation regimen for AFOI might not be suitable for awake intubation when a SOS is used instead of a fiberoptic bronchoscope (FOB), as the two devices have different characteristics and are manipulated differently. This study was designed to compare the efficacy and safety of dexmedetomidine with that of remifentanil during awake intubation with a SOS.
Methods
After institutional ethics committee approval (IRB00006761-2012045, Medical Ethics Committee of Peking University Third Hospital), informed written consent was obtained from all patients. We enrolled patients between December 2013 and December 2014. Inclusion criteria were: age 18–70 years; American Society of Anesthesiologists (ASA) physical status score I–III; requirement for preoperative neck immobilization with a hard plastic collar; planned urgent or elective cervical spine surgery for cervical trauma or severe cervical spondylosis. Exclusion criteria were: pregnancy; use of an α2 adrenoreceptor agonist or antagonist within the previous 14 days; known or admitted alcohol or drug misuse; uncontrolled seizure disorder; history of unstable angina or myocardial infarction; resting heart rate (HR) <50 min−1; and complete heart block.
Patients were assigned by a computer-generated randomization schedule to receive sedation with dexmedetomidine (Group D) or remifentanil (Group R). A research nurse generated the allocation sequence, enrolled participants and assigned them to their groups. While one anesthesiologist prepared and infused the study drug, another anesthesiologist experienced in the use of the SOS was in charge of airway anesthesia and intubation. Another research nurse assessed the patients, recorded intubation time and followed up the patients postoperatively. The participants, the intubating anesthesiologist and the nurse who was responsible for assessment and follow up were blinded to the group allocation.
All patients received a bolus of intravenous scopolamine 0.3 mg as premedication and oxygen by nasal cannula (3 L · min−1). Vital signs, including systolic blood pressure (SBP), diastolic blood pressure (DBP), HR and pulse oxygen saturation (SpO2) were recorded at baseline and every 2 min until the completion of intubation. The time required for intubation (from the first insertion of the SOS to confirming intubation with capnography) and the number of attempts was also recorded.
All patients received the study drug via an Alaris PK Syringe Pump (Care Fusion, Becton Dickinson, Franklin Lakes, NJ). The study drug was diluted to 50 mL with a 0.9 % NaCl solution, and the infusion was started 10 min before airway anesthesia and continued throughout airway management and intubation. Group D received a loading dose of 1.0 μg · kg−1 dexmedetomidine over 10 min followed by a continuous infusion of 0.7 μg · kg−1 · h−1 [12]. Group R received a target-controlled infusion of remifentanil using the Minto three compartment model. The initial target was set at 2.5 ng · ml−1 and increased to 3 ng · ml−1 10 min later. In both groups, the drug infusion was continued until confirmation of successful intubation.
During application of topical airway anesthesia and intubation, the cervical collar was not released. Airway anesthesia began 10 min after the start of sedative drug infusion. Lidocaine 200 mg was administered through a laryngotracheal mucosa atomization device (LMA MADgic, Teleflex Medical, Athlone, Republic of Ireland) to the mouth, larynx and glottis.
The application of topical anesthesia to the upper airway took no less than 10 min. The patient’s sedation level was assessed using the Ramsay Sedation Scale (RSS) at baseline, 10 min after the drug infusion had started, and every 3 min during airway anesthesia. Any patient with an RSS <2 was given a rescue bolus of intravenous midazolam 0.5 mg until an RSS of 2 was achieved [12].
A SOS preloaded with an endotracheal tube (ETT) was inserted over the tongue. The supine patient was asked to take deep breaths. The epiglottis and the glottic opening were identified via the eyepiece. Once the vocal cords were visualized, the tip of the ETT was advanced during inspiration. After the tip of ETT had entered the trachea, the SOS was withdrawn. Intubation score was assessed using a 5-point scale during SOS endoscopy and intubation (1, no movement; 2, grimacing; 3, mild cough; 4, major limb movement; 5, prolonged coughing) [13]. If the intubation score was >2 during endoscopy, the SOS was withdrawn and 3 mL 2 % lidocaine was sprayed on to the glottis via the LMA MADgic. The patient’s sedation level was reassessed and rescue midazolam 0.5 mg was given repeatedly in 1-min intervals until RSS ≥2.
The SOS was withdrawn if the patient’s SpO2 was ≤92 % during endoscopy. Oxygen was given via facemask (5 L · min−1) and the patient was instructed to take deep breaths. When SpO2 recovered to ≥95 %, another intubation attempt was made.
Immediately after intubation, end tidal CO2 concentration (first breath) was recorded. Tolerance of the ETT was assessed using a 3-point scale (1, well tolerated and cooperative; 2, mild coughing and/or grimacing but still cooperative; 3, severe coughing and/or agitated and not cooperative) [15]. General anesthesia was induced immediately after assessment of ETT tolerance. Infusion of the study drug was discontinued upon completion of induction of general anesthesia.
At the 24-h postoperative follow-up visit, patients were interviewed to assess their recall of pre-anesthesia events, administration of topical anesthesia, endoscopy and intubation, and whether there had been complications (for example, injury to the teeth, lip or oral mucosa, sore throat or hoarseness). Patient satisfaction with the whole procedure was assessed on an 11-point numeric rating scale (0, completely dissatisfied; 10, completely satisfied).
The primary efficacy endpoint of this study was the proportion of patients intubated successfully at the first attempt. Based on the findings of a previous study, in which the first attempt success rates using dexmedetomidine versus remifentanil in AFOI were 38 and 76 % respectively [10], we calculated that a sample size of 64 patients would be sufficient to detect a difference between the treatment groups with a power of 0.8 and a significance level of 0.05. Considering possible 5 % dropout, the sample size was set at 68.
We used SPSS 13.0 software (SPSS, Chicago, IL) for statistical analyses. Continuous variables are expressed as mean ± standard deviation, and were compared within groups using the paired t-test and between groups using the independent t-test. The chi-squared test or Fisher’s exact test were used to compare categorical data between the groups. Intubation conditions and tolerance score were analyzed using the independent samples Mann–Whitney U test. Blood pressure and HR at different time points were compared using two-way repeated-measures analysis of variance. A P value <0.05 was regarded as statistically significant.
Results
A total of 70 patients were assessed for eligibility, and 68 patients were enrolled. The enrolled patients were randomized and all of them completed this study (Fig. 1). Patients’ demographic and clinical characteristics did not differ between the groups (Table 1).

Study flow diagram. Group D, group Dexmedetomidine; Group R, group remifentanil
The baseline RSS of the two groups were similar (Table 2), but RSS was significantly higher in Group D than in Group R 10 min after drug infusion (Table 2, P = 0.001).
All patients were successfully intubated with the SOS. The first intubation attempt success rates and the need for rescue midazolam were similar between the groups (Table 2). In first-time SOS insertions, the intubation scores of the two groups were broadly comparable. After intubation, mild coughing was observed in 12 patients in Group R, compared with 24 patients in Group D (and one case of severe coughing), resulting in significantly different tube tolerance scores (P = 0.001). The duration of drug infusion was 26.0 ± 4.5 versus 24.8 ± 4.0 min in Groups D and R, respectively (P = 0.247).
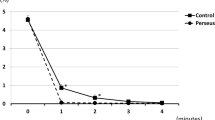
Nine patients in Group R and two in Group D developed hypoxia during intubation. The incidence of hypoxia (defined as SpO2 ≤ 90 % or a decrease of 10 % below baseline saturation, with the number of desaturation episodes measured on a per patient basis) in Group R was significantly higher than Group D (26 % versus 6 %, P = 0.021). The lowest SpO2, observed in a patient in Group R, was 85 %. All patients who developed hypoxia recovered to an SpO2 ≥ 95 % within 2 min after administration of supplementary oxygen by face mask. The hemodynamic changes observed in both groups were similar (Table 3). There were no significant differences in the occurrence of hemodynamic adverse events between the groups from the beginning of drug infusion until 10 min after intubation (Table 4). Significantly more patients in Group R recalled airway management than Group D (Table 2). There were no significant differences in patient satisfaction (Table 2) or intubation complications between the two groups (Table 4).
Discussion
We found that remifentanil and dexmedetomidine are both suitable for use as sedatives for awake SOS intubation. Although the first attempt success rates were similar between the groups, patients sedated with remifentanil tolerated the tracheal tube better after intubation, but at the expense of a greater risk of mild desaturation.
We selected the dose of the sedative according to previous studies of AFOI. The loading dose of 1 μg · kg−1 over 10 min followed by a continuous infusion at 0.5–0.7 μg · kg−1 · h−1 is a standard regime for intraoperative use of dexmedetomidine, and is most widely reported in use for dexmedetomidine sedation for AFOI [12, 16–21]. A higher dose may cause hypertension [22], while a lower one may not achieve adequate sedation. The reported target concentrations of remifentanil for AFOI vary [9, 10, 23–30]; in most studies the target effect site concentration of remifentanil at the time of endotracheal intubation was 2–4 ng · ml−1 [9, 10, 23–28, 30]. This informed our choice of 3 ng · ml−1.
We found that the main differences between the groups were sedation level and ETT tolerance. The patients in Group D were more deeply sedated, but patients in both groups were able to cooperate with the operator during airway anesthesia. There were no significant differences in the first intubation attempt success rates or the overall score for intubation conditions at the first attempt between the groups. After intubation, the proportion of patients who coughed mildly in Group D was twice that of Group R. Although patients in Group D were significantly less likely to tolerate the ETT, there was nonetheless no difference in the proportion with hypertension or tachycardia compared with Group R. The apparent lack of a profound hemodynamic response to coughing and the higher incidence of bradycardia in Group D may be explained by the anti-sympathetic effect of dexmedetomidine.
In contrast, Hu and colleagues found that dexmedetomidine and remifentanil were both effective in patients undergoing awake fiberoptic nasotracheal intubation, and there were no significant differences in intubation or post-intubation scores between those sedated with dexmedetomidine versus remifentanil [9]. Unlike a flexible FOB, the SOS is a more rigid rod with limited degrees of freedom. This difference makes the manipulation of the SOS more stimulating than a FOB. Additionally, the SOS does not have a working channel though which local anesthetic can be administered in a ‘spray-as-you-go’ manner. Although the vocal cords and the airway above the vocal cords can be adequately anesthetized through an LMA MADgic, local anesthetic could not be sprayed into the trachea. The suppression of the cough reflex after intubation relied mainly on the analgesic properties of the sedative.
There have been several reports of the use of dexmedetomidine or remifentanil for AFOI without topical anesthesia. In one case report, a loading dose of 1.0 μg · kg−1 dexmedetomidine followed by an infusion of 0.6 μg · kg−1 · h−1 was used as the sole agent for AFIO in a patient with local anesthetic allergy [18]. The authors reported that the patient tolerated the procedure well with minimal discomfort despite the lack of topical anesthesia. Our findings suggest that for awake SOS intubation a combination of dexmedetomidine with a more potent analgesic drug should be considered to achieve better ETT tolerance. A recent study showed that for AFOI, the use of dexmedetomidine (1 μg · kg−1 loading dose followed by an infusion of 0.5 μg · kg−1 · h−1) plus ketamine (15 mg loading dose and a 20 mg · h−1 continuous infusion) provided better hemodynamic stability and sedation than dexmedetomidine alone [31].
The proportion of patients in our study who experienced mild or prolonged coughing after intubation was significantly lower in Group R than Group D. In a previous study, Song and colleagues used ‘no sustained and repetitive coughing with head lift’ as the indicator of suitable sedation conditions for AFIO in patients undergoing cervical spine surgery [28]. Although in our study,all patients in Group R met Song’s criteria, a higher plasma remifentanil concentration might reduce the incidence of mild coughing further. Vennila and colleagues used a target controlled infusion of remifentanil as the sole agent for AFIO without ‘spray-as-you-go’ local anesthesia [29]. The higher mean remifentanil concentration that they adopted (6.3 ng · ml−1 at nasal endoscopy, and 8.06 ng · ml−1 during tracheal intubation) was shown to be safe. Although in the present study, Group R had a higher incidence of hypoxia, the degree of hypoxia was modest—the lowest SpO2 was 85 % in one patient. Hypoxia was successfully addressed within 2 min in all patients who desaturated. The majority of patients who developed desaturation in both groups had a history of smoking or pulmonary disease, or a BMI >30 kg · m−2. Caution should be exercised when administering sedation in such patients.
We found that the proportion of patients who recalled airway management was higher in the remifentanil group than the dexmedetomidine group. This finding chimes with those of previous studies, which have reported that dexmedetomidine has a stronger amnesic effect than remifentanil [9, 10]. Although the recall rate was higher in Group R, most patients did not find the experience unpleasant, reflected in broadly comparable patient satisfaction scores. Although no dental injuries were reported in our study, there was a high incidence of sore throat in both groups (47.1 % versus 52.9 %, P = 0.628), which may have been a consequence of surgery rather than airway instrumentation. It has previously been reported that the incidence of sore throat was as high as 51–74 % in patients undergoing cervical spine surgery [32].
Our study had some limitations. First, the sample size in each group was 34 and the primary endpoint was first-attempt intubation success rate. These were 79.4 and 85.3 % in each group, meaning that the risk of a statistical type II error was 0.88. Therefore, further larger samples studies will be needed to confirm our results. Second, there was also a relatively high chance that our sample size was inadequate to detect intergroup differences for uncommon adverse events (e.g., lip or teeth injuries, complications associated with oxygen desaturation events, etc.). Finally, our results cannot be extrapolated to settings where target-controlled infusion of remifentanil is not available.
Conclusions
Dexmedetomidine and remifentanil are effective sedatives for awake intubation using the SOS. Although the first-attempt success rates were similar between the two groups, patients sedated with remifentanil tolerated the ETT better at the expense of an increased risk of mild hypoxia.
Abbreviations
AFOI, awake fiberoptic endoscope intubation; DBP, diastolic blood pressure; ETT, endotracheal tube; FOB, fiberoptic endoscope; HR, heart rate; RSS, Ramsay Sedation Scale; SBP, systolic blood pressure; SOS, Shikani optical stylet; TCI, target controlled infusion
References
Lin N, Li M, Shi S, Li TZ, Zhang BX. Shikani seeing optical stylet-aided tracheal intubation in patients with a large epiglottic cyst. Chin Med J (Engl). 2011;124:2795–8.
Phua DS, Mah CL, Wang CF. The Shikani optical stylet as an alternative to the GlideScope® videolaryngoscope in simulated difficult intubations--a randomised controlled trial. Anaesthesia. 2012;67:402–6.
Shukry M, Hanson RD, Koveleskie JR, Ramadhyani U. Management of the difficult pediatric airway with Shikani Optical Stylet. Paediatr Anaesth. 2005;15:342–5.
Stricker P, Fiadjoe JE, McGinnis S. Intubation of an infant with Pierre Robin sequence under dexmedetomidine sedation using the Shikani Optical Stylet. Acta Anaesthesiol Scand. 2008;52:866–7.
Agro F, Cataldo R, Carassiti M, Costa F. The seeing stylet: a new device for tracheal intubation. Resuscitation. 2000;44:177–80.
Yang D, Tong SY, Jin JH, Tang GZ, Sui JH, Wei LX, Deng XM. Shikani optical stylet-guided intubation via the intubating laryngeal airway in patients with scar contracture of the face and neck. Chin Med Sci J. 2013;28:195–200.
Turkstra TP, Pelz DM, Shaikh AA, Craen RA. Cervical spine motion: a fluoroscopic comparison of Shikani Optical Stylet vs Macintosh laryngoscope. Can J Anaesth. 2007;54:441–7.
Kovacs G, Law AJ, Petrie D. Awake fiberoptic intubation using an optical stylet in an anticipated difficult airway. Ann Emerg Med. 2007;49:81–3.
Hu R, Liu JX, Jiang H. Dexmedetomidine versus remifentanil sedation during awake fiberoptic nasotracheal intubation: a double-blinded randomized controlled trial. J Anesth. 2013;27:211–7.
Cattano D, Lam NC, Ferrario L, Seitan C, Vahdat K, Wilcox DW, Hagberg CA. Dexmedetomidine versus remifentanil for sedation during awake fiberoptic intubation. Anesthesiol Res Pract. 2012;2012:753107.
Boyd BC, Sutter SJ. Dexmedetomidine sedation for awake fiberoptic intubation of patients with difficult airways due to severe odontogenic cervicofacial infections. J Oral Maxillofac Surg. 2011;69:1608–12.
Bergese SD, Candiotti KA, Bokesch PM, Zura A, Wisemandle W, Bekker AY, Group AS. A Phase IIIb, randomized, double-blind, placebo-controlled, multicenter study evaluating the safety and efficacy of dexmedetomidine for sedation during awake fiberoptic intubation. Am J Ther. 2010;17:586–95.
Bergese SD, Patrick Bender S, McSweeney TD, Fernandez S, Dzwonczyk R, Sage K. A comparative study of dexmedetomidine with midazolam and midazolam alone for sedation during elective awake fiberoptic intubation. J Clin Anesth. 2010;22:35–40.
Kunisawa T, Nagashima M, Hanada S, Suzuki A, Takahata O, Iwasaki H. Awake intubation under sedation using target-controlled infusion of dexmedetomidine: five case reports. J Anesth. 2010;24:789–92.
Chu KS, Wang FY, Hsu HT, Lu IC, Wang HM, Tsai CJ. The effectiveness of dexmedetomidine infusion for sedating oral cancer patients undergoing awake fibreoptic nasal intubation. Eur J Anaesthesiol. 2010;27:36–40.
Tsai CJ, Chu KS, Chen TI, Lu DV, Wang HM, Lu IC. A comparison of the effectiveness of dexmedetomidine versus propofol target-controlled infusion for sedation during fibreoptic nasotracheal intubation. Anaesthesia. 2010;65:254–9.
Shen SL, Xie Y, Wang WY, Hu SF, Zhang YL. Comparison of dexmedetomidine and sufentanil for conscious sedation in patients undergoing awake fibreoptic nasotracheal intubation: a prospective, randomised and controlled clinical trial. Clin Respir J. 2014;8:100–7.
Madhere M, Vangura D, Saidov A. Dexmedetomidine as sole agent for awake fiberoptic intubation in a patient with local anesthetic allergy. J Anesth. 2011;25:592–4.
Abdelmalak B, Makary L, Hoban J, Doyle DJ. Dexmedetomidine as sole sedative for awake intubation in management of the critical airway. J Clin Anesth. 2007;19:370–3.
Gaszynski T, Gaszynska E, Szewczyk T. Dexmedetomidine for awake intubation and an opioid-free general anesthesia in a superobese patient with suspected difficult intubation. Drug Des Devel Ther. 2014;8:909–12.
Bergese SD, Khabiri B, Roberts WD, Howie MB, McSweeney TD, Gerhardt MA. Dexmedetomidine for conscious sedation in difficult awake fiberoptic intubation cases. J Clin Anesth. 2007;19:141–4.
Bloor BC, Ward DS, Belleville JP, Maze M. Effects of intravenous dexmedetomidine in humans. II. Hemodynamic changes. Anesthesiology. 1992;77:1134–42.
Lallo A, Billard V, Bourgain JL. A comparison of propofol and remifentanil target-controlled infusions to facilitate fiberoptic nasotracheal intubation. Anesth Analg. 2009;108:852–7.
Lee HM, Sakong J, Jee DL. The comparison of feasibility and safety on fiberoptic guided intubation under conscious sedation with remifentanil and propofol. Korean J Anesthesiol. 2013;65:215–20.
Rai MR, Parry TM, Dombrovskis A, Warner OJ. Remifentanil target-controlled infusion vs propofol target-controlled infusion for conscious sedation for awake fibreoptic intubation: a double-blinded randomized controlled trial. Br J Anaesth. 2008;100:125–30.
Cafiero T, Esposito F, Fraioli G, Gargiulo G, Frangiosa A, Cavallo LM, Mennella N, Cappabianca P. Remifentanil-TCI and propofol-TCI for conscious sedation during fibreoptic intubation in the acromegalic patient. Eur J Anaesthesiol. 2008;25:670–4.
Zhang X, He W, Wu X, Zhou X, Huang W, Feng X. TCI remifentanil vs. TCI propofol for awake fiber-optic intubation with limited topical anesthesia. Int J Clin Pharmacol Ther. 2012;50:10–6.
Song JW, Kwak YL, Lee JW, Chang CH, Kim HS, Shim YH. The optimal effect site concentration of remifentanil in combination with intravenous midazolam and topical lidocaine for awake fibreoptic nasotracheal intubation in patients undergoing cervical spine surgery. Minerva Anestesiol. 2012;78:521–6.
Vennila R, Hall A, Ali M, Bhuiyan N, Pirotta D, Raw DA. Remifentanil as single agent to facilitate awake fibreoptic intubation in the absence of premedication. Anaesthesia. 2011;66:368–72.
Yeganeh N, Roshani B, Azizi B, Almasi A. Target-controlled infusion of remifentanil to provide analgesia for awake nasotracheal fiberoptic intubations in cervical trauma patients. J Trauma. 2010;69:1185–90.
Sinha SK, Joshiraj B, Chaudhary L, Hayaran N, Kaur M, Jain A. A comparison of dexmedetomidine plus ketamine combination with dexmedetomidine alone for awake fiberoptic nasotracheal intubation: a randomized controlled study. J Anaesthesiol Clin Pharmacol. 2014;30:514.
Ratnaraj J, Todorov A, McHugh T, Cheng MA, Lauryssen C. Effects of decreasing endotracheal tube cuff pressures during neck retraction for anterior cervical spine surgery. J Neurosurg. 2002;97:176–9.
Acknowledgments
We sincerely thank all the staff of the Anesthesiology Department of Peking university third hospital for their help in this research.
Funding
Not applicable.
Availability of data and materials
The data during this study are available from the corresponding author on reasonable request.
Authors’ contributions
All authors have made substantive intellectual contributions to the manuscript. ML and TX designed the study. TX and CN were responsible for conducting the study and analyzing the data. ML, TX and CN wrote the manuscript. XG participated in study design and revised the manuscript. All authors have seen the original study data, reviewed the data analysis and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written informed consent was obtained from the patient for publication of the Fig. 2c in this article.

Shikani Optical Stylet larygngoscope and its application in a male patient with hard plastic collar. a A Shikani Optical Stylet larygngoscope; (b) The Shikani Optical Stylet larygngoscope was inserted into an endotracheal tube; (c) Manipulation of tracheal intubation by a Shikani Optical Stylet larygngoscope
Ethics approval and consent to participate
The study was approved by Peking university third hospital medical ethics committee and each participant provided written informed consent.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Xu, T., Li, M., Ni, C. et al. Dexmedetomidine versus remifentanil for sedation during awake intubation using a Shikani optical stylet: a randomized, double-blinded, controlled trial. BMC Anesthesiol 16, 52 (2015). https://doi.org/10.1186/s12871-016-0219-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-016-0219-9