
Abstract
Background
Intravenous lipid emulsions have been introduced for the management of patients with Local Anesthetic Systemic Toxicity (LAST). These emulsions have been stated as a first-line treatment in the guidelines of several international anesthesia organizations. Nevertheless, the adoption of lipid rescue therapy by Chinese practitioners remains unknown. We, therefore, evaluated the current approaches to treat LAST and the use of lipid rescue therapy among anesthesiologists in China.
Methods
In September 2013, a 23-question survey on regional anesthesia practice and availability of lipid emulsions was sent by e-mail to directors or designated individuals at 41 academic anesthesiology departments listed by the orthopedic anesthesia group of the Chinese Society of Anesthesiology.
Results
Responses were received from 36 of the 41 (88 %) anesthesiology departments. To simplify the analysis, responses were divided into two groups according to the annual percentage of patients who received regional anesthesia (RA) for orthopedic anesthesia: 14 departments (39 %) with high-utilization (≥50 %) and 22 departments (61 %) low-utilization (<50 %) of RA. Ropivacaine and bupivacaine were the common drugs used for RA, which were independent of RA utilization. Interestingly, ultrasound-guided techniques were much more frequently used in low-utilization institutions than in high-utilization institutions (P = 0.025). Lipid emulsion was readily available in 8 of the 36 (22 %) responding institutions, with 7 of the other 28 (25 %) institutions planning to stock lipid emulsion. No differences in lipid availability and storage plans were observed between high- and low-utilization institutions. Lipid resuscitation was performed in five of the eight departments that had lipid emulsion. Eleven patients were successfully resuscitated and one was not.
Conclusion
Lipid emulsion is not widely available in China to treat LAST resulted from RA for orthopedic patients. Efforts are required to promote lipid rescue therapy nationwide.
Trial registration
Chinese Clinical Trail Registry (Registration number # ChiCTR-EOR-15006960; Date of Retrospective Registration on August 23rd, 2015) http://www.chictr.org.cn/showproj.aspx?proj=11703.
Similar content being viewed by others


Background
The increased use of regional anesthesia (RA) have increased the incidence of local anesthetic systemic toxicity (LAST), which has been reported to range from 7.5 to 20 per 10,000 peripheral nerve blocks (PNBs) and at about 4 per 10,000 epidural blocks [1]. Although it is rare, LAST can be lethal. Many case reports [2–5] and animal studies [6, 7] have suggested that lipid emulsion infusion is effective in reversing LAST, resulting in the use of lipid rescue therapy (LRT) during resuscitation.
LRT has been explicitly supported by the Association of Anesthetists of Great Britain and Ireland (AAGBI), the American Society of Regional Anesthesia (ASRA), and the American Heart Association (AHA) guidelines on LAST treatment [8–10]. In addition, the American College of Medical Toxicology (ACMT) has issued interim aguidelines for the use of LRT in conditions other than LAST [11]. Similar national guidelines have not yet been introduced, but are under consideration, in China.
In 2006, a questionnaire study documented contemporary practice strategies among academic anesthesiology departments in the United States [12]. Two other national surveys, one in the United Kingdom in 2007 [13] and the other in the United States in 2011 [14], have assessed the availability of lipid emulsion in obstetric anesthesia units. Similarly, the availability of and use of lipid rescue therapy in England and Wales was also surveyed in 2009 [15]. To date, however, no comparable survey has been completed in China. The aim of this study was to evaluate the current status of RA practices and the adoption of LRT among anesthesiologists in China.
Methods
This study was approved by the independent ethical committee of Peking University Third Hospital, Beijing, China (Approval No. 2013046). It was also registered with Chinese Clinical Trial Registry under the number ChiCTR-EOR-15006960. The approved questionnaire was developed by three of the investigators (ZQL, MX and SLJ), based on previous research [12–15] and the guidelines published by the AAGBI and ASRA [8, 10]. The questionnaire consisted of 23 questions about the current RA practices and the availability of lipid emulsions in 2013. The survey responses were subsequently reviewed by four orthopedic anesthesiologists (XYG, XLW, LZ and ZGF) and an expert in LRT (XZX). The approved questionnaire is attached in Additional file 1.
The electronic questionaire was e-mailed to the 41 committee members of the orthopedic anesthesia group of the Chinese Society of Anesthesiology (CSA) on September 1st, 2013. Two follow-up e-mail reminders at 1-month intervals were sent to non-responders. December 1st, 2013 was the deadline to receive the feedback e-mails. Participation in this study was voluntary. Completion of the survey indicated a consent to study participation.
The respondents were grouped by the number of RA performed in patients undergoing orthopedic anesthesia per year, and we arbitrarily defined high-utilization institutions as those performing ≥ 50 % each year, and low-utilization institutions as < 50 % each year. Descriptive statistics were calculated. Fisher’s exact t-test was used for between-group comparisons. All statistical analysis was performed with SPSS for Windows (version 16.0; SPSS, Chicago, IL). A p < 0.05 was considered statistically significant.
Results
Survey response and RA utilization
Responses were received from 36 out of the 41 (88 %) anesthesiology departments; their characteristics are shown in Table 1. Out of the 36 institutions, 14 (39 %) used RA for orthopedic anesthesia in ≥ 50 % of patients per year and 22 (61 %) used RA for < 50 % of these patients. RA included PNBs, epidural blocks and spinal anesthesia.
RA practice
RA was performed and monitored in the operating room of 29 (81 %) institutions, the RA induction area of 4 (11 %) institutions, and the postanesthesia care unit of 3 (8 %) institutions. With respect to the preferred local anesthetic when performing RA, 29 (81 %) respondents preferred ropivacaine and 6 (17 %) selected bupivacaine. There were 5 (14 %) responding departments selected multiple drugs as the preferred anesthetics. So the summation of all percentages exceeded 100 % (Fig. 1).

Long-acting local anesthetics preferred by responding institutions
When performing RA, especially PNBs, almost all of the institutions stated that monitoring consisted of pulse oxygen saturation, noninvasive arterial blood pressure, and electrocardiogram. Only one institution reported that only pulse oxygen saturation was monitored during regional blocking. The distribution of the average number of PNBs performed monthly was shown in Table 2. In addtion, PNBs was performed by attending anesthesiologists at 28 (78 %) institutions and by senior anesthesiology residents at only 8 (22 %) institutions.
Regional blocking was performed under ultrasound guidance at 7 (19 %) institutions, under nerve stimulator guidance at 12 (33 %) institutions, under both techniques at 10 (28 %) institutions, and using landmark-based techniques at 7 (19 %) institutions. Interestingly, the use of ultrasound guidance by high- and low-utilization institutions differed significantly (21 % vs. 64 %, P = 0.019, Fig. 2).

Techniques used by responding institutions for RA. The frequency of utilization of ultrasound differed significantly between high and low RA-utilization institutions (P = 0.019)
Incidence of LAST
Of the 36 responding institutions, 27 (75 %) reported an incident of LAST in 2013, among which, 14 respondents were high-utilization institutions while 13 respondents were low-utilization institutions. The incidence of LAST in the high-utilization institutions was much higher than that in the low-utilization institutions (100 % vs. 59 %, P = 0.006). The distribution of LAST among techniques used was: epidural anesthesia (31 %), brachial plexus block (50 %), cervical plexus block (23 %), lumbar plexus block (8 %), sciatic nerve block (4 %), combined lumbar and sciatic nerve block (31 %), and others (8 %).
Although 34 institutions (94 %) reported having an algorithm or guideline for the treatment of LAST, only the algorithms of 11 (31 %) of these institutions included lipid emulsions for treatment. All 36 responding institutions reported using lidocaine to detect intravascular epidural catheter placement, with five (14 %) adding epinephrine to the lidocaine.
Adoption of lipid rescue
When respondents were asked about the adoption of LRT for management of LAST, 22 (61 %) knew that lipid emulsion infusion was a treatment option and 13 (36 %) had heard of LRT but did not know the specifics of the regimen. Eight institutions (22 %) were aware of the 2007 and 2010 AAGBI guidelines for LAST management [16, 17], 19 (53 %) were aware of the 2010 ARSA guidelines [8], and two (6 %) were aware of the 2011 ACMT guidelines [11].
Lipid emulsion: availability and choice
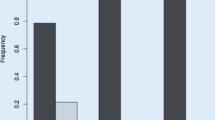
Lipid emulsion was readily available in 8 of the 36 (22 %) responding institutions (Fig. 3a). This availability was not associated with RA utilization (Fig. 3b). These eight institutions began to stock lipid emulsion between 2008 and 2012, with all eight institutions reporting storing lipid emulsion according to AAGBI [16, 17] and ASRA guidelines [8].

Adoption of lipid rescue therapy by responding institutions in China in 2013. a Current and future planned availability of lipid emulsion; b Current availability of lipid emulsion by high and low RA- utilization institutions (P = 1.0); c Future planned availability of lipid emulsion by high and low RA-utilization institutions (P = 0.394)
Of the 28 departments that did not currently stock lipid emulsion, seven (25 %) planned to stock it. The reasons for the remaining 21 departments that did not plan to stock lipid emulsion are shown in Table 3, with some departments citing more than one reason. In addition, high- and low-utilization institutions were similarly unlikely in planning to store lipid emulsion (Fig. 3c).
The most common storage locations for lipid emulsion were anesthesia preparation rooms (4/8, 50 %) and a pharmacy within the department (3/8, 38 %). One respondent reported storing lipid emulsion in the postanesthesia care unit. All eight, however, reported that they could obtain the emulsion within 5 min for emergency treatment of LAST.
Of the eight units, five stocked lipid emulsions containing long-chain triglycerides (e.g. Intralipid; Huarui Pharmaceuticals Co., Ltd., Wuxi, China), two stocked lipid emulsions containing long- and medium-chain triglycerides (e.g. Lipovenoes; Huarui Pharmaceuticals Co., Ltd.); and one stocked both. Five of the eight units (63 %) reported using lipid emulsion to treat LAST within their departments. Of the 12 patients treated, 11 were successfully resuscitated; whereas one was not, making the overall failure rate of lipid resuscitation for LAST at 8.3 %.
Resuscitation practice
When asked about treatment of ventricular tachycardia from presumed toxicity by local anesthetics, only five departments (14 %) reported they would use lipid emulsion. Of the remaining departments, 22 (61 %) would use amiodarone, five (14 %) would use lidocaine, and four (11 %) would use esmolol. Unfortunately, no data about the use of electrical cardioversion and its relation to the use of lipid emulsion in this questionnaire.
In response to convulsions secondary to LAST, only one respondent (3 %) reported that lipid emulsion would be the first-line treatment; whereas 25 (69 %) would choose a benzodiazepine, six (17 %) would use propofol, three (8 %) would use thiopental, and one (3 %) would use a muscle relaxant.
None of the 36 respondents reported using lipid emulsion for severe hypotension (MAP < 60 mmHg). In contrast, 20 (56 %) would consider epinephrine, 6 (17 %) would choose norepinephrine, five (14 %) would use dopamine and/or dobutamine, three (8 %) would use ephedrine, and two (6 %) would choose phenylephrine.
Discussion
This survey showed that, from September to November 2013, lipid emulsion was available in only 22 % of academic anesthesiology departments listed by the orthopedic anesthesia group of the CSA. Of the remaining departments, only 25 % reported intention to stock lipid emulsion in the near future. The most common reason for not stocking lipid emulsion by the other 21 departments was “availability in the central pharmacy” within the hospital.
The long acting RA preferred by most departments was ropivacaine, followed by bupivacaine. However, bupivacaine is more cardiotoxic than similar agents. Thus, the greater safety of ropivacaine [18] may explain its widespread and, in some case, exclusive use by anesthesiologists in many institutions of China. Other factors, such as the cost of the agent and its duration of action, may also influence the choice by anesthesiologists. However, these factors were not evaluated in our study. Giving a test dose is a safety step to reduce LAST and was used by all institutions with 14 % of them using epinephrine-containing test solutions. Because other safety steps may not prevent intravascular injection, test dosing with an epinephrine-containing solution may have value. Any significant changes in heart rate and blood pressure may alert the anesthesiologist to intravascular injection of both epinephrine and anesthetic.
Over the past two decades, ultrasound-guided RA has been increasingly used by anesthesiologists worldwide. Compared with non-ultrasound techniques, ultrasound guided RA has been associated with reduced rates of inadvertent vascular puncture [19] and reduced LA requirements [20], resulting in reduction in the risk and severity of LAST [21]. Half of the respondents to our survey reported using ultrasound guidance and combined ultrasound and nerve stimulator guidance. Interestingly, ultrasound guided methods were more frequently used in low than in high RA-utilization institutions. The reasons for this difference remain unclear. Furthermore, the lower use of ultrasound guidance and higher incidence of LAST in high-utilization institutions may pointed to the clinical efficacy and safety of the performance of ultrasound-guided RA. Nevertheless, wether there is a negative correlation between use of ultrasound guidance and LAST or not is not presented in the current study and requires further research.
As LAST is a rare but devastating complication of RA, the availability of lipid emulsion is a patient-safety issue [14]. The AAGBI guidelines recommend that 20 % lipid emulsion should be “immediately available in all areas where potentially toxic doses of local anesthetics are administered.” All eight departments stocking lipid emulsion reported that they could obtain the drug within 5 min. However, many respondents that did not stock lipid emulsion reported that it was available at their central pharmacies. Thus, lipid emulsion was unlikely to be immediately available to those departments. Because AAGBI guidelines were not followed, increased physician awareness and education are warranted.
Our survey also assessed the effectiveness of lipid rescue in patients with LAST. Lipid resuscitation was successful in 11 of 12 events in the eight departments that store lipid emulsion. Although we did not assess the circumstances in which lipid emulsion was used, clinical and experimental reports have shown failure of lipid rescue in LAST management [22–24]. Failures may be due to the physicochemical properties of local anesthetics, an inadequate dose of lipid emulsion and/or interaction between the lipid emulsion and local anesthetics [25]. Optimal methods of administering lipid emulsion have not yet been determined.
The adoption of LRT in the United Kingdom was assessed in 2005–2008 by surveying 66 National Health Service hospitals within London and its surrounding areas [26]. Following the publication of the 2007 AAGBI guidelines [16], there was a sharp increase in the number of departments adopting these guidelines. By 2009, LRT was available in 95.1 % of institutions in England and Wales [15]. Moreover, two similar national surveys found that LRT was adopted in 2007 by 49 % of obstetric anesthesia units in the UK [13] and in 2011 by 88 % of obstetric anesthesia units in the United States [14]. Our survey found that the overall level of lipid emulsion availability was much lower, indicating the need to increase the awareness of LRT throughout China. Establishing Chinese national guidelines would likely contribute to this process.
This study had several limitations. As with any survey, it is subject to responder bias. However, we surveyed 41 academic hospitals that are distributed in all provinces and major municipalities in mainland China. In addition, our response rate was 88 %, suggesting that our results are as representative as possible. Also, we did not report incidents of local anesthetic toxicity with other fields as obstetric and peripheral vascular surgeries, in which lipid emulsion may be more available. However, orthopedic surgery in our study is the major indication for RA, with the utilization of PNBs in orthopedic surgery paralleling the increased number of ambulatory surgeries [27]. Thus, findings in hospitals performing orthopedic surgery likely reflect the adoption of LRT by academic anesthesiology departments. Finally, our results may not reflect the much broader practice of RA in non-academic departments throughout China.
Conclusion
The survey found that LRT was available at few academic anesthesiology departments in China. The safety of perioperative RA can be optimized by increasing awareness of LAST and techniques for reducing and treating this condition. We encourage storage of lipid emulsion in specified locations, with current guidelines readily available. To date, no comparable survey has been reported in other developing countries. Our survey results may have been somewhat representative, thereby supporting efforts to globally promote LRT among practitioners.
Abbreviations
- RA:
-
Regional anesthesia
- LAST:
-
Local anesthetic systemic toxicity
- PNBs:
-
Peripheral nerve blocks
- LRT:
-
Lipid rescue therapy
- AAGBI:
-
Association of anesthetists of Great Britain and Ireland
- ASRA:
-
American society of regional anesthesia
- AHA:
-
American heart association
- ACMT:
-
American college of medical toxicology
- CSA:
-
Chinese society of anesthesiology
References
Mulroy MF. Systemic toxicity and cardiotoxicity from local anesthetics: incidence and preventive measures. Reg Anesth Pain Med. 2002;27(6):556–61.
Rosenblatt MA, Abel M, Fischer GW, Itzkovich CJ, Eisenkraft JB. Successful use of a 20 % lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiol. 2006;105(1):217–8.
Ludot H, Tharin JY, Belouadah M, Mazoit JX, Malinovsky JM. Successful resuscitation after ropivacaine and lidocaine-induced ventricular arrhythmia following posterior lumbar plexus block in a child. Anesth Analg. 2008;106(5):1572–4.
Foxall G, McCahon R, Lamb J, Hardman JG, Bedforth NM. Levobupivacaine-induced seizures and cardiovascular collapse treated with Intralipid. Anaesthesia. 2007;62(5):516–8.
Warren JA, Thoma RB, Georgescu A, Shah SJ. Intravenous lipid infusion in the successful resuscitation of local anesthetic-induced cardiovascular collapse after supraclavicular brachial plexus block. Anesth Analg. 2008;106(5):1578–80.
Li Z, Xia Y, Dong X, Chen H, Xia F, Wang X, et al. Lipid resuscitation of bupivacaine toxicity: long-chain triglyceride emulsion provides benefits over long- and medium-chain triglyceride emulsion. Anesthesiol. 2011;115(6):1219–28.
Weinberg GL, VadeBoncouer T, Ramaraju GA, Garcia-Amaro MF, Cwik MJ. Pretreatment or resuscitation with a lipid infusion shifts the dose–response to bupivacaine-induced asystole in rats. Anesthesiol. 1998;88(4):1071–5.
Neal JM, Bernards CM, Butterworth JF, Di Gregorio G, Drasner K, Hejtmanek MR, et al. ASRA practice advisory on local anesthetic systemic toxicity. Reg Anesth Pain Med. 2010;35(2):152–61.
Vanden Hoek TL, Morrison LJ, Shuster M, Donnino M, Sinz E, Lavonas EJ, et al. Part 12: cardiac arrest in special situations: 2010 american heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circ. 2010;122(18 Suppl 3):S829–61.
Cave G, Harvey MG, Winterbottom T. Evaluation of the Association of Anaesthetists of Great Britain and Ireland lipid infusion protocol in bupivacaine induced cardiac arrest in rabbits. Anaesth. 2009;64(7):732–7.
American College of Medical T. ACMT position statement: interim guidance for the use of lipid resuscitation therapy. J Med Toxicol. 2011;7(1):81–2.
Corcoran W, Butterworth J, Weller RS, Beck JC, Gerancher JC, Houle TT, et al. Local anesthetic-induced cardiac toxicity: a survey of contemporary practice strategies among academic anesthesiology departments. Anesth Analg. 2006;103(5):1322–6.
Williamson RM, Haines J. Availability of lipid emulsion in obstetric anaesthesia in the UK: a national questionnaire survey. Anaesth. 2008;63(4):385–8.
Toledo P, Nixon HC, Mhyre JM, Wong CA, Weinberg G. Brief report: availability of lipid emulsion in United States obstetric units. Anesth Analg. 2013;116(2):406–8.
Hamann P, Dargan PI, Parbat N, Ovaska H, Wood DM. Availability of and use of Intralipid (lipid rescue therapy, lipid emulsion) in England and Wales. Emerg Med J. 2010;27(8):590–2.
The Association of Anaesthetists of Great Britain and Ireland. Guidelines for the Management of Severe Local Anaesthetic Toxicity. August 2007. Available from: http://www.aagbiorg/publications/guidelines/docs/latoxicity07pdf. Accessed October 2015.
The Association of Anaesthetists of Great Britain and Ireland. Management of Severe Local Anaesthetic Toxicity 2. December 2010. Available from: http://www.aagbiorg/sites/default/files/latoxicity_2010_0pdf. Accessed September 2015.
Groban L, Deal DD, Vernon JC, James RL, Butterworth J. Cardiac resuscitation after incremental overdosage with lidocaine, bupivacaine, levobupivacaine, and ropivacaine in anesthetized dogs. Anesth Analg. 2001;92(1):37–43.
Barrington MJ, Watts SA, Gledhill SR, Thomas RD, Said SA, Snyder GL, et al. Preliminary results of the Australasian Regional Anaesthesia Collaboration: a prospective audit of more than 7000 peripheral nerve and plexus blocks for neurologic and other complications. Reg Anesth Pain Med. 2009;34(6):534–41.
Renes SH, van Geffen GJ, Rettig HC, Gielen MJ, Scheffer GJ. Minimum effective volume of local anesthetic for shoulder analgesia by ultrasound-guided block at root C7 with assessment of pulmonary function. Reg Anesth Pain Med. 2010;35(6):529–34.
Barrington MJ, Kluger R. Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med. 2013;38(4):289–97.
Marwick PC, Levin AI, Coetzee AR. Recurrence of cardiotoxicity after lipid rescue from bupivacaine-induced cardiac arrest. Anesth Analg. 2009;108(4):1344–6.
Aveline C, Cognet F, Bonnet F. Ineffectiveness of intralipid infusion for central nervous toxicity following ultrasound-guided sciatic nerve block with lidocaine-ropivacaine solution: interaction between carbamazepine, local anaesthetic and intralipid? Eur J Anaesthesiol. 2010;27(12):1070–2.
Calenda E, Dinescu SA. Failure of lipid emulsion to reverse neurotoxicity after an ultrasound-guided axillary block with ropivacaine and mepivacaine. J Anesth. 2009;23(3):472–3.
Zausig YA, Zink W, Graf BM. What limits the effect of lipid emulsion therapy? Eur J Anaesthesiol. 2012;29(3):159–60.
Picard J, Ward SC, Zumpe R, Meek T, Barlow J, Harrop-Griffiths W. Guidelines and the adoption of 'lipid rescue' therapy for local anaesthetic toxicity. Anaesth. 2009;64(2):122–5.
Stein BE, Srikumaran U, Tan EW, Freehill MT, Wilckens JH. Lower-extremity peripheral nerve blocks in the perioperative pain management of orthopaedic patients: AAOS exhibit selection. J Bone Joint Surg Am. 2012;94(22):e167.
Acknowledgements
We would like to thank the following committee members of the orthopedic anesthesia group of the Chinese Society of Anesthesiology for providing the original data from their hospitals: Dr. Shaohui Chen, Dr. Jing Yang, Dr. Ting Ma, Dr. Geng Wang, Dr. Hongda Cai, Dr. Zhouping Guo, Dr. Haihua Shu, Dr. Chengxin Lin, Dr. Fangxiang Zhang, Dr. Yinglin Wang, Dr. Wei Zhang, Dr. Wengang Ding, Dr. Weike Mao, Dr. Yi Zhang, Dr. Longyun Li, Dr. Xiaoping Gu, Dr. Shi Xiao, Dr. Hongtao Liu, Dr. Yi Qiu, Dr. Liqin Deng, Dr. Jiuhui Li, Dr. Jishun Ning, Dr. Jianxin Yang, Dr. Buhuai Dong, Dr. Hao Fang, Dr. Zhijie Lu, Dr. Wei Jiang, Dr. Talaiti Ailaiti, Dr. Furong Zhang, Dr. Fan Tao, and Dr. Ke Wei.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MX, SLJ, and ZQL helped to design the study, sent the questionnaires to participations, analyze the data, and drafted the original manuscript; XZX, XLW, LZ, and ZGF contributed the study design and questionnaire revision; BWY, JL, and XYG designed the survey and edited the manuscript critically. All authors read and approved the final manuscript.
Mao Xu, Shanliang Jin and Zhengqian Li contributed equally to this work.
Additional file
Additional file 1:
Survey questionnaire. (DOC 53 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Xu, M., Jin, S., Li, Z. et al. Regional anesthesia and lipid resuscitation for local anesthetic systemic toxicity in China: results of a survey by the orthopedic anesthesia group of the chinese society of anesthesiology. BMC Anesthesiol 16, 1 (2015). https://doi.org/10.1186/s12871-015-0163-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-015-0163-0