
Abstract
This study investigated whether endurance training attenuates orchiectomy (ORX)-induced metabolic alterations. At 7 days of recovery after sham operation or ORX surgery, the mice were randomized to remain sedentary or undergo 5 weeks of treadmill running training (15–20 m/min, 60 min, 5 days/week). ORX decreased glycogen concentration in the gastrocnemius muscle, enhanced phosphofructokinase activity in the plantaris muscle, and decreased lactate dehydrogenase activity in the plantaris and soleus muscles. Mitochondrial enzyme activities and protein content in the plantaris and soleus muscles were also decreased after ORX, but preserved, in part, by endurance training. In the treadmill running test (15 m/min, 60 min) after 4 weeks of training, orchiectomized sedentary mice showed impaired exercise performance, which was restored by endurance training. Thus, endurance training could be a potential therapeutic strategy to prevent the hypoandrogenism-induced decline in muscle mitochondrial content and physical performance.
Similar content being viewed by others


Background
Androgens are male sex hormones that are secreted predominantly from the testes. Androgen deficiency or insufficiency occurs under several conditions, such as aging and disease [1], leading to negative health consequences [2]. Circulating testosterone levels are positively correlated with insulin sensitivity, maximal oxygen uptake, and mitochondrial gene expression [3], suggesting that bioavailable androgen levels are closely associated with metabolic homeostasis, whole-body metabolism, and physical performance.
Although androgen restoration is a treatment option for men with hypogonadism, several adverse effects have been reported. For example, a study conducted in old frail men with a high prevalence of cardiovascular diseases was halted prematurely due to high rates of cardiac, respiratory, and dermatologic events in the treatment group [4]. Therefore, an alternative approach to hypoandrogenism is warranted. Exercise training prevents several metabolic disorders, by potentially improving the metabolic capacity of skeletal muscles [5, 6]. However, it remains unclear whether endurance training is a viable strategy to alleviate androgen deficiency-induced metabolic impairments, and whether loss of androgens impedes skeletal muscle adaptation to endurance training.
In this study, we examined the effects of endurance training on glycolytic and oxidative enzyme activities in the skeletal muscles of mice that underwent orchiectomy (ORX) surgery, which is a prevailing model of androgen deficiency. Since substrate metabolism is regulated by transport activity at the plasma membrane, we also determined the protein levels of key metabolite transporters. Given that androgen sensitivity is likely to differ depending on the muscle phenotype [7,8,9], we analyzed the plantaris (glycolytic phenotype) and soleus (oxidative phenotype) muscles. Moreover, we performed respiratory gas analysis during exercise to evaluate whole-body metabolism. Given that androgen level is reported to associate with metabolic function [3], we hypothesized that enzyme activity and transport protein levels are declined by ORX, but restored by endurance training.
Methods
Animals
All experiments were approved by the Animal Experimental Committee of The University of Tokyo (No. 2021-1). Ten-week-old male Institute of Cancer Research (ICR) mice bred in the animal care facility at The University of Tokyo were used in this study. The animals were housed individually on a 12:12 h light/dark cycle (dark: 7:00 to 19:00) in an air-conditioned room (23 °C). All mice had ad libitum access to standard chow diet (Oriental Yeast, Tokyo, Japan) and water during the experimental period.
Experimental design
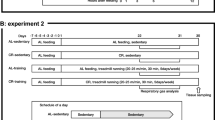
Figure 1 shows the schematic of the experiment. Before the experiment, all animals were familiarized with running on a treadmill (MK-680; Muromachi Kikai Co., Inc., Tokyo, Japan) at a speed of 20 m/min for 5 min for 3 days. At 10 weeks of age, the animals underwent a sham operation or ORX surgery, as described below. Following a 7-day post-surgery recovery, animals were subdivided into sedentary and training groups as follows: sham-sedentary group (n = 9), ORX-sedentary group (n = 10), sham-training group (n = 8), and ORX-training group (n = 11). Animals in the training groups performed 60 min of treadmill running 5 days a week for 5 weeks. According to a previous study, the critical speed, where the greatest metabolic rate that results in wholly oxidative energy provision is represented [10], for ICR mice is 24.1 ± 4.6 m/min [11]. In our previous study, we used treadmill running at 20 m/min for 60 min as endurance training for ICR mice [12]. In our preliminary study, however, we observed that animals were unable to complete 60 min of exercise at 20 m/min, while they were able to complete it at 15 m/min after a 7-day post-surgery. Therefore, the running speed for the initial five training sessions was set at 15 m/min, followed by 20 m/min for subsequent training sessions. The treadmill running test was performed 4–7 days before tissue sampling to avoid exercise effects on the sedentary groups, as described below. Twenty-four hours after the last training session, the animals were anesthetized using isoflurane and euthanized by removing blood from the inferior vena cava. The gastrocnemius, plantaris, and soleus muscles were collected, rapidly frozen in liquid nitrogen, and stored at − 80 °C until analysis.

Schematic overview of the experiment
ORX surgery
The animals were anesthetized via an intraperitoneal injection of a cocktail (5 µL/g body weight) of medetomidine hydrochloride (0.3 µg/g body weight), midazolam (4.0 µg/g body weight), and butorphanol (5.0 µg/g body weight). Small incisions (~ 0.5 cm) were made on both sides of the scrotum. The bilateral testes were removed from the incisions and excised, leaving the epididymal fat pad and seminal vesicles in place. An identical procedure was performed in the sham-operated groups, except that the testes were left intact. The incisions were closed using a surgical needle and a 3–0 absorbable suture. After all surgical procedures were completed within 10 min, atipamezole hydrochloride (3.0 µg/g body weight, 5 µL/g body weight) was intraperitoneally administered to negate anesthesia.
Treadmill running test
The animals performed treadmill running at a speed of 15 m/min for 60 min in an airtight metabolic chamber equipped with a treadmill (MK-680AT/02M; Muromachi Kikai). This treadmill running speed is considered lower than the critical speed for typical ICR mice [11]. O2 consumption (VO2) and CO2 production (VCO2) were measured every 5 min using a metabolism-measuring system (MK-5000RQ; Muromachi Kikai) with an airflow rate of 1.5 L/min. The respiratory exchange ratio (RER) was calculated as VCO2/VO2. The measurement was terminated when the animals reached exhaustion before 60 min of exercise. Exhaustion was defined as the inability of the animals to maintain the running speed despite contacting the electrical grid for more than 5 consecutive seconds. Before and after exercise, the tail vein blood glucose and lactate levels were measured using GLUCOCARD Plus Care (Arkray, Kyoto, Japan) and Lactate Pro 2 (Arkray), respectively.
Muscle glycogen
The glycogen content in the gastrocnemius muscle was measured as previously described [13]. Briefly, the whole gastrocnemius muscle was heated at 100 °C in 30% (w/v) KOH solution saturated with Na2SO4 until completely dissolved. Glycogen in the solution was precipitated on ice for 30 min after the addition of 99% (v/v) ethanol. The solution was then centrifuged at 10,000×g for 10 min at 4 °C. After the supernatant was discarded, the glycogen precipitate was dissolved in 1 N HCl and heated at 100 °C for 2 h to hydrolyze glycogen to glucose. After neutralization with 1 N NaOH, glucose concentration was determined using a glucose CII kit (Fujifilm Wako, Osaka, Japan).
Muscle triglyceride (TG)
Whole gastrocnemius muscle was homogenized using a µT-01 bead crusher (TAITEC, Saitama, Japan) in a buffer containing 5% (v/v) NP-40 substitute (145-09701; Fujifilm Wako). The homogenate was subjected to two cycles of heating (100 °C for 5 min) and cooling (room temperature) to solubilize the lipids. After centrifugation at 10,000×g for 2 min, the TG content in the supernatant was determined using a LabAssay Triglyceride kit (Fujifilm Wako).
Determination of enzyme activity
Whole soleus and plantaris muscles were homogenized in 100 times (vol/wt) of phosphate buffer (100 mM, pH 7.6) using a μT-01 bead crusher (TAITEC). The homogenates were freeze-thawed twice using liquid nitrogen to disrupt the plasma and mitochondrial membranes. After centrifugation at 1000×g for 10 min at 4 °C, the supernatant was recovered for the enzyme assay.
Hexokinase (HK) assay
Maximal HK activity was measured as previously described, with slight modifications [14]. The aliquots were mixed with the reaction mixture (50 mM triethanolamine, 5 mM EDTA, 10 mM MgCl2, 0.35 mM NADH, 2.8 mM ATP, 2.8 mM glucose, and 2.5 U glucose-6-phosphatase, pH 7.6) in a 96-well microplate (195-96F; Watson Bio Lab, Tokyo, Japan). The changes in absorbance at 340 nm were determined using a microplate spectrophotometer (Epoch Microplate Spectrophotometer, BioTek Instruments, Inc.).
Phosphofructokinase (PFK) assay
Maximal PFK activity was measured as previously described, with slight modifications [14]. The aliquots were mixed with the reaction mixture (50 mM triethanolamine, 5 mM EDTA, 10 mM MgCl2, 0.3 mM NADH, 2.8 mM ATP, 2.8 mM F-6-P, 2.5 U GPDH-TPI, and 1.0 U aldolase, pH 7.6) in a 96-well microplate. The changes in absorbance at 340 nm were determined.
Lactate dehydrogenase (LDH, pyruvate-to-lactate) assay
The activity of LDH, which involved the conversion of pyruvate to lactate, was measured as previously described, with slight modifications [15]. The aliquots were mixed with the reaction mixture (50 mM imidazole, 5 mM DTT, 150 μM NADH, 4.0 mM pyruvate, pH 7.4) in a 96-well microplate. The changes in absorbance at 340 nm were determined.
Citrate synthase (CS) assay
Maximal CS activity was measured as previously described, with slight modifications [16]. The aliquots were mixed with the reaction mixture (100 mM Tris, 100 μM DTNB, 300 μM acetyl-CoA, and 50 μM oxaloacetate, pH 8.3) in a 96-well microplate. The changes in absorbance at 412 nm/min were determined.
Cytochrome c oxidase (COX) assay
Maximal COX activity was measured as previously described, with slight modifications [17]. The aliquots were mixed with the reaction mixture (10 mM phosphate and 50 μM cytochrome c reduced with sodium hydrosulfite, pH 7.0) in a 96-well microplate. The changes in absorbance at 550 nm/min were determined.
β-Hydroxyacyl-CoA dehydrogenase (β-HAD) assay
The maximal β-HAD activity was measured as previously described, with slight modifications [18]. The aliquots were mixed with the reaction mixture (1 M Tris, 5 mM EDTA, 450 µM NADH, and 100 µM acetoacetyl-CoA, pH 7.0) in a 96-well microplate. The changes in absorbance at 340 nm/min were determined.
Total carnitine palmitoyltransferase (CPT) assay
The maximal activity of CPT (CPT-I and CPT-II) was measured as described previously, with slight modifications [19]. The aliquots were mixed with the reaction mixture (60 mM Tris, 1.5 mM EDTA, 0.25 mM DTNB, 1.67 mM l-carnitine, and 0.025 mM palmitoyl-CoA, pH 8.0) in a 96-well microplate. The changes in absorbance at 412 nm/min were determined.
Western blotting
Whole soleus and plantaris muscles were homogenized 20 times (vol/wt) in ice-cold radioimmunoprecipitation assay buffer (25 mM Tris-HCl, pH 7.6, 150 mM NaCl, and 1% NP-40) supplemented with a protease inhibitor cocktail (cOmplete Mini, ETDA-free; Roche Applied Science, Indianapolis, IN, USA) using a μT-01 bead crusher (TAITEC). The homogenates were rotated on ice for 60 min and centrifuged at 1500×g at 4 °C for 20 min. The total protein content of the samples was determined using a BCA protein assay kit (TaKaRa BIO Inc., Shiga, Japan). Equal amounts of proteins were loaded onto sodium dodecyl sulfate–polyacrylamide gels and separated via electrophoresis. Proteins were transferred onto polyvinylidene difluoride membranes and western blotting was performed using the standard procedure, as previously described [20]. The primary and secondary antibodies used in this study are mentioned below. Blots were scanned and quantified using ChemiDoc XRS (Bio-Rad Laboratories, Hercules, CA, USA) and Quantity One (version 4.5.2; Bio-Rad). Ponceau staining was used to verify the consistent loading.
Primary and secondary antibodies
Commercially available primary antibodies were used to detect hypoxia-inducible factor 1-α (HIF-1α; #20960-1-AP; Proteintech Japan, Tokyo, Japan), peroxisome proliferator-activated receptor γ coactivator 1-α (PGC-1α; #516557; Merck Millipore), mitochondrial electron transport proteins (NADH:ubiquinone oxidoreductase subunit B8 [NDUFB8], succinate dehydrogenase complex iron sulfur subunit B [SDHB], ubiquinol–cytochrome c reductase core protein 2 [UQCRC2], mitochondrially encoded cytochrome c oxidase 1 [MTCO1], and ATP synthase F1 subunit alpha [ATP5F1A/ATP5A]; #ab110413; Abcam, Cambridge, UK), cytochrome c oxidase subunit 4I1 (COX4I1/COXIV; #ab14744; Abcam), glucose transporter 1 (GLUT1; #sc-377228; Santa Cruz Biotechnology, Santa Cruz, CA, USA), glucose transporter 4 (GLUT4; #07-1404; Merck Millipore, Tokyo, Japan), and fatty acid translocase/cluster of differentiation 36 (FAT/CD36; #18836-1-AP; Proteintech Japan). Antibodies against monocarboxylate transporter (MCT)-1 and MCT-4 were raised in rabbits against the C-terminal region of the respective MCT (Qiagen, Tokyo, Japan), and have been used in our previous studies [13, 21,22,23]. Rabbit anti-goat IgG (H&L) (#A102PT; American Qualex, San Clemente, CA, USA) and mouse anti-goat IgG (H&L) (#A106PU; American Qualex) were used as secondary antibodies.
Statistical analysis
All data are presented as the mean ± standard error of the mean. Two-way analysis of variance (ANOVA) was applied to determine the interaction and main effects of training and ORX on mice. When an interaction was significant, a comparison was made using the Tukey–Kramer multiple comparison test to identify differences among the groups. The running proportion curves in the treadmill running test were compared using the log-rank (Mantel–Cox) test. For the time course changes in RER, two-way ANOVA (time × group) followed by the Tukey–Kramer multiple comparison test was performed. All statistical analyses were performed using the GraphPad Prism software (Ver. 9.0, Macintosh; GraphPad Software, La Jolla, CA). Statistical significance was defined as p < 0.05. All results within the range of 0.05 ≤ p ≤ 0.1 were shown as tendencies.
Results
Body and tissue weights, and food intake
There were no differences in the initial body weights among the groups (Fig. 2A); however, ORX resulted in the lower final body weight (p < 0.05, Fig. 2B). We also found that ORX (p < 0.05) and training (p < 0.01) reduced the body weight during the experimental period (Fig. 2C). ORX decreased food intake during the experimental period (p < 0.01, Fig. 2D), suggesting that the lower final body weight was, in part, due to a decline in food consumption. ORX dramatically decreased seminal vesicle weight (p < 0.01, Fig. 3A), suggesting the successful removal of testes and a reduction in bioavailable testosterone after ORX. There was a trend for lower epididymal fat weight after ORX administration (p = 0.10, Fig. 3B). The plantaris, soleus, and gastrocnemius muscle weights did not differ significantly among the groups (Fig. 3C–E). These observations suggest that the decline in body weight after ORX is likely to result from a reduction in body fat mass caused by decreased food intake. Moreover, ORX-induced atrophy of androgen-sensitive tissues may partially account for body weight loss, as evidenced by the significant decrease in the seminal vesicle weight.

Body weight and food intake. Initial (A) and final (B) body weights. Body weight change (C) and food intake (D) during the experimental period. Data are expressed as the mean ± standard error of the mean (SEM) (n = 8–11). Two-way analysis of variance (ANOVA) was performed to determine the interactions and main effects of training and ORX. *p < 0.05: main effect of training. ††p < 0.01, †p < 0.05: main effect of ORX

Tissue weights after the experimental period. A Seminal vesicle and B epididymal fat weights. Plantaris (C), soleus (D), and gastrocnemius (E) muscle weights. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. ††p < 0.01, (†)p ≤ 0.10: main effect of ORX
Treadmill running test
To elucidate the impact of ORX on whole-body metabolism during exercise, we performed gas analysis during treadmill running 5 weeks after surgery. During this test, one mouse in the sham-sedentary group and five mice in the ORX-sedentary group reached exhaustion before 60 min, generating significant differences in the running proportion curves (p < 0.01, Fig. 4A). As they could not complete 60 min of exercise, we excluded their respiratory and blood metabolite data from the statistical analysis. Although the RER at 5 min of treadmill running was significantly higher in the ORX-sedentary group than in the sham-training group (p < 0.05, Fig. 4B), no significant differences were observed in the average RER (Fig. 4C). VO2/bodyweight at 55 min was significantly higher in the ORX-sedentary group than in the sham-training (p < 0.05) and ORX-training groups (p < 0.01, Fig. 4D). In the time course changes in VCO2/bodyweight, we observed a main effect of time (p < 0.01), but not a main effect of ORX or significant interaction (p = 0.09; Fig. 4F). Endurance training tended to decrease average VO2/bodyweight (p = 0.05, Fig. 4E), and significantly decreased VCO2/bodyweight (p < 0.01, Fig. 4G). The blood lactate and glucose levels before exercise were not significantly different (Fig. 4H, J). There was no significant difference in the post-exercise glucose concentration (Fig. 4I). Blood lactate levels after 60 min of exercise were significantly higher in the ORX-sedentary group than in the other groups (p < 0.01; Fig. 4K). These observations suggest that ORX impairs the endurance exercise performance. However, this impairment is likely to be restored by endurance training.

Respiratory exchange ratio and blood metabolite levels in the treadmill running test. Running proportions (A), time-course changes in the respiratory exchange ratio (RER) (B), and average RER (C) during 60 min of treadmill running. Time-course changes in O2 consumption (VO2)/bodyweight (D), and average VO2/bodyweight (E) during 60 min of treadmill running. Average RER (C) during 60 min of treadmill running. Time-course changes in CO2 production (VCO2)/bodyweight (F), and average VCO2/bodyweight (G) during 60 min of treadmill running. Blood glucose concentrations before (H) and after (I) exercise. Blood lactate concentrations before (J) and after (K) exercise. Data are expressed as the mean ± SEM (n = 5–11). The running proportion curves in the treadmill running test were compared using the log-rank (Mantel–Cox) test. For the time course changes in RER, two-way ANOVA (time × group) followed by the Tukey–Kramer multiple comparison test was performed. To determine the interactions and main effects of training and ORX, two-way ANOVA followed by the Tukey–Kramer multiple comparison test was performed. #p < 0.05: ORX-sedentary group vs. sham-training group. ‡p < 0.05: sham-sedentary group vs. ORX-training group. ¶¶p < 0.01: ORX-sedentary group vs. ORX-training group. **p < 0.01, (*)p ≤ 0.10: effect of training. §§p < 0.01: significantly different from other groups
Glycogen and TG levels
Given the impaired exercise performance of ORX-sedentary animals, we evaluated the basal level of muscle glycogen, which is a determinant factor of prolonged exercise performance [24]. We found that ORX reduced glycogen concentration in the gastrocnemius muscle at rest (p < 0.05, Fig. 5A), suggesting that a lower abundance of muscle glycogen was partially responsible for the compromised performance. We also determined the level of TG, which is another energy deposit stored in the skeletal muscle. No significant effect was detected on the TG concentration in the gastrocnemius muscle (Fig. 5B).

Muscle glycogen and triglyceride (TG) concentrations. Glycogen (A) and TG (B) concentrations in the gastrocnemius muscle at rest. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. †p < 0.05: main effect of ORX
Glycolytic enzyme activity
To clarify the metabolic characteristics of skeletal muscles, we first evaluated the glycolytic enzyme activity. Endurance training significantly enhanced HK activity in the plantaris (p < 0.01, Fig. 6A) and soleus (p < 0.01, Fig. 6D) muscles and PFK activity in the soleus muscle (p < 0.01, Fig. 6E). In addition, endurance training decreased LDH activity in the plantaris (p < 0.01, Fig. 6C) and soleus (p < 0.01, Fig. 6F) muscles. ORX increased PFK activity (p < 0.05, Fig. 6B) and decreased HK activity (p < 0.01, Fig. 6A) in the plantaris muscle and LDH activity in the soleus muscle (p < 0.01, Fig. 6F). These observations suggest that ORX can change the glycolytic capacity of skeletal muscles.

Glycolytic enzyme activities. Hexokinase (HK) (A), phosphofructokinase (PFK) (B), and lactate dehydrogenase (LDH) (C) activities in the plantaris muscle. HK (D), PFK (E), and LDH (F) activities in the soleus muscle. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. **p < 0.01: main effect of training. ††p < 0.01, †p < 0.05: main effect of ORX
Transcription factors involved in glycolytic metabolism
To explore the potential mechanisms by which glycolytic enzyme activity is altered, we determined the protein levels of HIF-1α, a transcription factor that regulates glycolytic metabolism. Endurance training significantly reduced HIF-1α protein levels in the plantaris muscle (p < 0.05, Fig. 7A). In soleus muscle, HIF-1α protein content was decreased by ORX (p < 0.05, Fig. 7B). These observations suggest that HIF-1α protein levels do not always correlate with changes in glycolytic enzyme activity.

Hypoxia-inducible factor 1-α (HIF-1α) protein levels. HIF-1α protein levels in the plantaris (A) and soleus (B) muscles. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. *p < 0.05: main effect of training. †p < 0.05: main effect of ORX
Mitochondrial enzyme activity
Next, we assessed the enzyme activities of the mitochondria, which are the key components for energy production. Endurance training enhanced CS and COX activity in the plantaris (p < 0.01, Fig. 8A, B) and soleus (p < 0.01, Fig. 8E; p < 0.05, Fig. 8F) muscles, as well as β-HAD (p < 0.01, Fig. 8C) and total CPT activity (p < 0.05, Fig. 8D) in the plantaris muscle. ORX significantly reduced CS activity in the plantaris (p < 0.01, Fig. 8A) and soleus (p < 0.01, Fig. 8E) muscles and β-HAD activity in the soleus muscle (p < 0.01, Fig. 8G). There was no significant difference in the total CPT activity of the soleus muscle (Fig. 8H). Thus, the mitochondrial enzyme activity is likely to decline after ORX.

Mitochondrial enzyme activities. Citrate synthase (CS) (A), cytochrome c oxidase (COX) (B), β-hydroxyacyl-CoA dehydrogenase (β-HAD) (C), and total carnitine palmitoyltransferase (CPT) (D) activities in the plantaris muscle. CS (E), COX (F), β-HAD (G), and total CPT (H) activities in the soleus muscle. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. **p < 0.01, *p < 0.05: main effect of training. ††p < 0.01: main effect of ORX
Mitochondria-associated proteins
To better understand ORX-induced mitochondrial adaptation, we evaluated the protein levels of PGC-1α, a master regulator of mitochondrial biogenesis, and mitochondrial electron transport components. In the plantaris muscle, endurance training increased the protein levels of PGC-1α, NDUFB8, SDHB, UQCRC2, MTCO1, COXIV, and ATP5A (p < 0.01, Fig. 9A–G). ORX significantly decreased the protein levels of NDUFB8 (p < 0.01, Fig. 9B), UQCRC2 (p < 0.05, Fig. 9D), and COXIV (p < 0.01, Fig. 9G) in the plantaris muscle, providing additional support for the decrease in mitochondrial content. We also observed that ORX decreased PGC-1α protein levels in the plantaris muscle (p = 0.09, Fig. 9A). In the soleus muscle, endurance training significantly increased NDUFB8, MTCO1, and COXIV protein levels (p < 0.01, Fig. 10B, E and F) and tended to increase PGC-1α protein level (p = 0.06, Fig. 10A). ORX decreased the protein levels of NDUFB8 (p = 0.10, Fig. 10B) and COXIV (p = 0.10, Fig. 10F) in the soleus muscle. The protein levels of SDHB, UQCRC2, and ATP5A did not differ significantly (Fig. 10C, D and G). PGC-1α protein levels were positively correlated with CS activity in the plantaris (p < 0.01, r = 0.66; Fig. 11A) and soleus (p < 0.01, r = 0.51; Fig. 11B) muscles. Taken together, these results suggest that ORX reduces the mitochondrial content in skeletal muscle, and that changes in mitochondrial content can be attributed to changes in mitochondrial biogenesis.

Mitochondria-associated protein levels in the plantaris muscle. Protein levels of peroxisome proliferator-activated receptor γ coactivator 1-α (PGC-1α) (A), NADH:ubiquinone oxidoreductase subunit B8 (NDUFB8) (B), succinate dehydrogenase complex iron sulfur subunit B (SDHB) (C), ubiquinol–cytochrome c reductase core protein 2 (UQCRC2) (D), mitochondrially encoded cytochrome c oxidase 1 (MTCO1) (E), cytochrome c oxidase subunit 4I1 (COX4I1/COXIV) (F), and ATP synthase F1 subunit alpha (ATP5F1A/ATP5A) (G) in the plantaris muscle. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. **p < 0.01, *p < 0.05: main effect of training. ††p < 0.01, (†)p ≤ 0.10: main effect of ORX

Mitochondria-associated protein levels in the soleus muscle. Protein levels of PGC-1α (A), NDUFB8 (B), SDHB (C), UQCRC2 (D), MTCO1 (E), COXIV (F), and ATP5A (G) in the soleus muscle. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. **p < 0.01, (*)p ≤ 0.10: main effect of training. (†)p ≤ 0.10: main effect of ORX

Correlations between CS activity and PGC-1α protein level. Correlation between CS activity and PGC-1α protein level in the plantaris (A) and soleus (B) muscles. Correlations between the two variables were studied using least-squares linear regression followed by Pearson’s correlation coefficient test
Metabolite transport proteins
Given that energy metabolism is facilitated by metabolite transport, we assessed the protein levels of key metabolite transporters. Endurance training significantly enhanced the protein levels of GLUT4 (p < 0.01, Fig. 12B) and MCT1 (p < 0.01, Fig. 12C) in the plantaris muscle. MCT4 protein level in the plantaris muscle was significantly decreased by ORX (p < 0.01, Fig. 12D). ORX tended to decrease GLUT4 protein level (p = 0.08, Fig. 12B) and increase FAT/CD36 protein level (p = 0.06, Fig. 12E) in the plantaris muscle. There was no significant difference in GLUT1 protein level in the plantaris muscle (Fig. 12A). In the soleus muscle, ORX significantly increased MCT1 protein level (p < 0.05, Fig. 13C). MCT4 protein level tended to increase after endurance training (p = 0.08, Fig. 13D). GLUT1, GLUT4, and FAT/CD36 protein levels did not differ in the soleus muscle (Fig. 13A, B and E). These results suggest that ORX induces muscle-specific changes in some metabolite transport proteins.

Metabolite transport protein levels in the plantaris muscle. Protein levels of glucose transporter (GLUT)-1 (A), GLUT4 (B), monocarboxylate transporter (MCT)-1 (C), MCT4 (D), and fatty acid translocase/cluster of differentiation 36 (FAT/CD36) (E) in the plantaris muscle. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. **p < 0.01: main effect of training. ††p < 0.01, (†)p ≤ 0.10: main effect of ORX

Metabolite transport protein levels in the soleus muscle. Protein levels of GLUT1 (A), GLUT4 (B), MCT1 (C), MCT4 (D), and FAT/CD36 (E) in the soleus muscle. Data are expressed as the mean ± SEM (n = 8–11). Two-way ANOVA was performed to determine the interactions and main effects of training and ORX. (*)p ≤ 0.10: main effect of training. †p < 0.05: main effect of ORX
Discussion
Main findings and perspectives
The major finding of this study was that ORX-sedentary animals showed impaired exercise performance. We also observed that the blood lactate concentration after exercise was higher in the ORX-sedentary group than in the other three groups. Although blood lactate level can be determined by several factors (glycolysis, oxidation, circulation, etc.) [25], the present observation may suggest greater reliance on glycolytic metabolism. In addition, ORX decreased the glycogen content in the gastrocnemius muscle at rest. Enhanced glycolytic rate and small glycogen storage lead to rapid depletion of glycogen, which is a major factor responsible for fatigue [24, 26, 27]. Therefore, it is likely that the exercise intolerance observed in ORX-sedentary mice results from glycogen depletion due to greater reliance on glycogenolysis and low basal glycogen levels.
Effects of ORX on glycolytic metabolism
The current observation of increased PFK activity in the plantaris muscle after ORX may underpin the notion that castrated animals rely heavily on glycogenolytic metabolism during exercise. In contrast to PFK activity, HK activity was decreased in the plantaris muscle of orchiectomized mice. PFK and HK are the rate-limiting enzymes in glycolysis [28]. PFK yields fructose-1,6-bisphosphate from fructose-6-phosphate derived from both glycogen and glucose, whereas HK catalyzes glucose phosphorylation. The maximal activity of PFK is reported to be much higher than that of HK [29]. These data indicate that PFK determines the overall glycolytic flux, especially glycogen breakdown rate, while HK is primarily involved in glucose metabolism. The partial knockout of HKII, a predominant isoform of HK, impairs exercise-stimulated muscle glucose uptake [30]. Exercise endurance capacity improves along with an increase in HKII protein content, which is related to muscle glucose uptake during exercise [31]. Furthermore, GLUT4 null mice exhibit exercise intolerance, reduced muscle glucose uptake, and increased muscle glycogen breakdown during exercise [32]. We observed that ORX significantly decreased HK activity and tended to decrease GLUT4 protein content in the plantaris muscle. Although measuring specific enzyme activity and protein levels is not always indicative of substrate flux in vivo, the present observations of the decrease in HK activity and GLUT4 protein content in the castrated animals may have resulted in diminished muscle glucose uptake, thereby reducing the glucose availability in the working muscle, leading to accelerated glycogen breakdown to maintain the overall glycolytic flux.
In the present study, the activity of LDH, which is involved in the conversion of pyruvate to lactate, was decreased by ORX in the plantaris muscle. This result seems to contradict the observation that blood lactate levels after exercise were elevated in the ORX sedentary group. LDH is highly abundant, and the catalysis of this enzyme is a near-equilibrium reaction [29, 33], suggesting that a decline in LDH activity does not affect the glycolytic capacity and lactate production. In addition to glycolytic enzyme activity, lactate transport activity across the plasmalemma via MCT1 and MCT4 influences the glycolytic capacity, as lactate efflux from the cells prevents end-product inhibition of glycolysis [34]. MCT1 is a high-affinity lactate transporter (Km = 3.5–8.3 mM) found greater quantity in oxidative fibers, whereas MCT4 is a low-affinity lactate transporter (Km = 25–32 mM) presented abundantly in glycolytic fibers [35]. On the basis of affinity for lactate and tissue-specific abundance, it is considered that MCT1 mainly facilitates lactate uptake, and that MCT4 primarily regulates lactate efflux [36]. In the current study, ORX decreased MCT4 protein level in the plantaris muscle. Since the post-exercise blood lactate level in the ORX-sedentary group (4.2 ± 1.1 mM) was much lower than the affinity of MCT4, we assumed that the muscle lactate level did not reach the value required for lactate release from skeletal muscle via MCT4. MCT1 was presumably sufficient to export lactate out of the skeletal muscle, as MCT can bidirectionally transport lactate across the sarcolemma depending on the concentration gradient [37].
HIF-1α is a transcription factor that regulates the expression levels of glycolytic enzymes and proteins [38], including HK, PFK, LDH, GLUT1, and MCT4. In the current study, the activities of HK and PFK, but not LDH, and protein levels of GLUT1 and MCT4 did not change concomitantly with HIF-1α protein levels. Besides HIF-1α, c-Myc also regulates glycolytic metabolism [39]. c-Myc mRNA expression is enhanced in castrated rat ventral prostate gland [40]. Moreover, nuclear receptor interacting protein 1 (NRIP1/RIP140) is another possible regulator of glycolysis [41]. In prostate cancer cells, RIP140 mRNA expression increases after androgen treatment [42]. Furthermore, a direct DNA binding site of the androgen receptor (AR) that promotes the transcription of glycolytic genes has been identified using chromatin immunoprecipitation with massively parallel DNA sequencing analyses [43]. Taken together, the coordinated transcriptional activity of several factors may explain the altered glycolytic enzyme activity and protein content observed in castrated animals.
Effects of ORX on oxidative metabolism
Among the several parameters used as biomarkers of mitochondrial content, muscle CS activity is strongly correlated with mitochondrial content, as assessed by transmission electron microscopy [44]. In the present study, we found that ORX decreased CS activity in the plantaris and soleus muscles, suggesting that ORX decreases mitochondrial content in skeletal muscles. The current observations that ORX reduced the mitochondrial protein content in the plantaris muscle and β-HAD activity in the soleus muscle may provide additional support for this view. Under conditions of attenuated mitochondrial energy supply, glycolytic metabolism is activated to meet the energy requirement. It is, therefore, likely that the decline in mitochondrial content could be another factor contributing to the elevated blood lactate levels in ORX-sedentary animals.
The mitochondrial content depends on the balance between biogenesis and degradation (mitophagy) [45]. Androgen action via ARs regulates mitochondrial biogenesis. Activated AR complexes bind to the nuclear and mitochondrial gene response elements [46,47,48]. Another proposed pathway of androgen action is through the direct interaction of AR complexes with the androgen response elements of mitochondrial genes. Additional mechanisms may involve indirect interactions with the androgen response element in the nucleus to activate the transcription of genes encoding transcription factors, including PGC-1α, a master regulator of mitochondrial biogenesis [49]. According to a previous report, ORX-induced reduction in mitochondrial content is primarily attributed to altered biogenesis rather than mitophagy [50], as the authors observed concomitant changes in the mitochondrial protein content and mRNA and/or protein levels of PGC-1α. In support of this, we observed significant positive correlations between CS activity and PGC-1α protein levels in the plantaris and soleus muscles. Other researchers have reported that testosterone treatment increases PGC-1α protein levels and mitochondrial protein content in mouse skeletal muscles [51]. Collectively, it appears that androgens, particularly testosterone, alter the mitochondrial content in skeletal muscle by modulating mitochondrial biogenesis.
Ovariectomy-induced estrogen deficiency impairs the mitochondrial respiratory function in rodent skeletal muscle [52, 53], which implies that sex hormones affect mitochondrial respiratory functions. To the best of our knowledge, the role of androgens in mitochondrial respiratory function has yet to be clarified. Future studies are required to examine the ability of androgens to alter the mitochondrial respiratory function.
We and others have repeatedly shown that MCT1 protein level positively correlates with lactate uptake rate, proportion of slow-twitch oxidative fibers, and CS activity in skeletal muscle [54,55,56,57]. In addition, we previously reported concomitant changes in MCT1 protein level and CS activity in equine skeletal muscle during training and detraining [58]. Based on these observations, it is considered that MCT1 facilitates the transport of lactate into skeletal muscle for oxidation in mitochondria and that lactate uptake capacity changes together with muscle oxidative capacity. However, we observed here that ORX increased MCT1 protein level in the soleus muscle despite the decreased CS activity, suggesting a dissociation between lactate uptake and muscle oxidative capacity. We also observed elevated blood lactate concentrations in the ORX-sedentary group after exercise. Our data suggest the relative importance of muscle oxidative capacity compared with lactate uptake capacity in relation to blood lactate levels during endurance exercise. We previously demonstrated that PGC-1α overexpression enhances MCT1 protein level in rodent skeletal muscles [59, 60]. In the present study, PGC-1α protein level in the soleus muscle was unaltered by ORX, suggesting a PGC-1α independent increase in MCT1 protein levels. Further studies are required to clarify the factors and mechanisms that regulate MCT1 protein levels.
ORX and hormonal regulation of substrate metabolism during exercise
Hormones, such as insulin, glucagon, and catecholamines (adrenaline and noradrenaline), exert strong influences on substrate metabolism [61]. During exercise, circulating insulin levels progressively decrease with time owing to adrenergic inhibition of pancreatic β-cells [62]. Previous studies showed a strong relationship between glucagon/insulin ratio and hepatic glucose output [63,64,65]. Although whether ORX changes glucagon/insulin ratio during exercise remains unclear, a previous study reported that ORX decreased basal glycogen concentration in the liver [66]. Hepatic glycogen was reported to be a key regulator of endurance capacity, because it is the primary storage for the maintenance of blood glucose level [67]. It is, therefore, possible that ORX diminishes glucose supply from the liver during prolonged exercise due to decreased basal levels of liver glycogen, which potentially impairs endurance performance. In addition to adrenergic stimulation, the decline in insulin level is also important for increasing adipose tissue lipolysis [68, 69], which leads to increased plasma fatty acid levels and skeletal muscle fat oxidation during exercise [70, 71]. Whether ORX changes hormonal secretions and responses, as well as substrate metabolism in other tissues during exercise requires further investigation.
Muscle phenotype differences in adaptations to ORX
Given the current observation that ORX decreases mitochondrial enzyme activities and protein content in the plantaris and soleus muscles, it is likely that mitochondrial adaptation to ORX is not muscle phenotype-specific. In the present study, changes in glycolytic enzyme activities in the plantaris muscle appeared to be more sensitive to ORX than those in the soleus muscle. This observation may be explained by the greater affinity [8] and/or number [9] of ARs in fast-twitch muscle fibers, because the plantaris muscle comprises more than 90% of fast-twitch fibers, whereas the soleus muscle comprises around 50% of slow-twitch fibers [72]. It should be noted that some human skeletal muscles are composed of more than 50% of slow-twitch fibers [73, 74]. Whether the present findings are also the case for human muscle should be clarified in the future study.
Effects of endurance training
High-intensity interval training (HIIT) is known to enhance the glycolytic capacity owing to increased levels of HK, PFK, LDH, and MCT4 [75,76,77,78,79]. We previously reported that HIIT increased HIF-1α protein level in mouse skeletal muscle [80], suggesting that HIF-1α may be accountable, in part, for HIIT-induced alterations in glycolytic capacity. In the present study, we found that endurance training enhanced HK activity in the plantaris and soleus muscles and PFK activity in the soleus muscle, even though HIF-1α protein levels were decreased in the plantaris muscle and did not change in the soleus muscle. These observations suggest that HIF-1α is not solely responsible for glycolytic adaptation to HIIT and that other transcriptional factors may be involved in endurance training-induced changes in glycolytic enzyme activity and protein levels.
Mitochondria are fundamental cellular components that are related to health and disease [81]. In the current study, although ORX decreased the mitochondrial enzyme activity and protein levels in skeletal muscles, which were enhanced by endurance training. In addition, the PGC-1α protein level after endurance training was increased in the plantaris muscle and tended to increase in the soleus muscle. These observations suggest that the increase in mitochondrial content after endurance training may stem, in part, from PGC-1α protein abundance, and that endurance training would be a viable approach to counteract hypogonadism-induced decline in mitochondrial content and the development of adverse health outcomes. Moreover, the increase in mitochondrial content contributes to endurance performance [82], as it enables the skeletal muscle to spare glycogen during exercise [27]. We found that endurance training restored the exercise performance and normalized post-exercise blood lactate levels in castrated animals. Since endurance training did not decrease HK and PFK activities in the skeletal muscles, the effects of endurance training may be ascribed primarily to the increased mitochondrial content.
Vascular adaptations to ORX and endurance training
Skeletal muscle capillarity is also an important factor contributing to endurance performance [83]. In the present study, although we were unable to assess capillarity, the protein content of HIF-1α, which is a transcription factor inducing angiogenesis [84], was declined by ORX. A previous report demonstrated that ORX decreased in vivo angiogenesis, resulting in the reduced capillary density and blood vessel diameter in mouse hindlimbs [85]. Another study reported that the critical power, measured in units of power rather than speed, was positively related to skeletal muscle capillarity in endurance-trained humans [86]. We, therefore, assume that ORX-induced decline in vascularity decreased the critical speed of castrated animals, resulting in impaired performance.
Together with mitochondrial biogenesis, endurance training induces angiogenesis in skeletal muscle [87, 88]. In the present report, however, HIF-1α protein content after endurance training was not restored in the soleus muscle and decreased in the plantaris muscle. Other investigators reported that accumulation of HIF-1α by knocking down prolyl hydroxylase domain protein (PHD) 2, which hydroxylates HIF-1α for ubiquitination and degradation, increased capillaries in mouse skeletal muscle without exercise training [89]. They also showed that endurance training increased capillary density to the same extent in the PHD2 knockdown and wild-type animals [89]. These data may suggest that HIF-1α can increase capillaries in the skeletal muscle, but exercise training-induced angiogenesis is not predominantly mediated through HIF-1α. Another pathway involved in angiogenesis is PGC-1α [90, 91]. It has previously been demonstrated that PGC-1α transgenic mice display the increased capillary density and capillary-to-fiber ratio in skeletal muscle together with fatigue resistance to tetanic muscle contraction [92], although PGC-1α overexpression also increases mitochondrial content in the skeletal muscle [93]. In the current investigation, PGC-1α protein content after endurance training significantly increased in the plantaris muscle, and tended to increase in the soleus muscle. These observations may suggest that endurance training enhances skeletal muscle vascularity through the PGC-1α-dependent pathway, leading to less fatiguability. Finally, cross-sectional data showed that high-intensity training was more effective for increasing the capillary-to-fiber ratio, compared to lower intensities of exercise training [94]. It is, therefore, worth comparing endurance training with high-intensity training to develop effective training strategies for patients with androgen insufficiency or deficiency.
Conclusions
This study demonstrated that endurance training restores ORX-induced impaired physical performance. This effect seems to be attributable to enhanced mitochondrial content, as endurance training did not normalize the ORX-induced changes in glycolytic enzyme activity. We conclude that endurance training may be a potential alternative to androgen replacement therapy for alleviating the negative metabolic consequences of hypoandrogenism.
Availability of data and materials
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- β-HAD:
-
β-Hydroxyacyl-CoA dehydrogenase
- ANOVA:
-
Analysis of variance
- AR:
-
Androgen receptor
- ATP5F1A/ATP5A:
-
ATP synthase F1 subunit alpha
- COX:
-
Cytochrome c oxidase
- CPT:
-
Carnitine palmitoyltransferase
- CS:
-
Citrate synthase
- GLUT1:
-
Glucose transporter 1
- HIF-1α:
-
Hypoxia-inducible factor 1-α
- HIIT:
-
High-intensity interval training
- HK:
-
Hexokinase
- LDH:
-
Lactate dehydrogenase
- MCT1:
-
Monocarboxylate transporter 1
- MTCO1:
-
Mitochondrially encoded cytochrome c oxidase 1
- NDUFB8:
-
NADH: ubiquinone oxidoreductase subunit B8
- NRIP1/RIP140:
-
Nuclear receptor interacting protein 1
- ORX:
-
Orchiectomy
- PFK:
-
Phosphofructokinase
- PGC-1α:
-
Peroxisome proliferator-activated receptor γ coactivator 1-α
- PHD:
-
Prolyl hydroxylase domain protein
- RER:
-
Respiratory exchange ratio
- SDHB:
-
Succinate dehydrogenase complex iron sulfur subunit B
- TG:
-
Triglyceride
- UQCRC2:
-
Ubiquinol-cytochrome c reductase core protein 2
- VCO2 :
-
Carbon dioxide production
- VO2 :
-
Oxygen consumption
References
Long Z, He LY, Tang YX, Jiang XZ, Wang JW, Chen WH, Tang J, Zhang YC, Yang C (2015) Causes of orchiectomy: an analysis of 291 cases. Zhonghua Nan Ke Xue 21:615–618
Traish AM, Abdallah B, Yu G (2011) Androgen deficiency and mitochondrial dysfunction: implications for fatigue, muscle dysfunction, insulin resistance, diabetes, and cardiovascular disease. Horm Mol Biol Clin Investig 8:431–444. https://doi.org/10.1515/hmbci.2011.132
Pitteloud N, Mootha VK, Dwyer AA, Hardin M, Lee H, Eriksson KF, Tripathy D, Yialamas M, Groop L, Elahi D, Hayes FJ (2005) Relationship between testosterone levels, insulin sensitivity, and mitochondrial function in men. Diabetes Care 28:1636–1642. https://doi.org/10.2337/diacare.28.7.1636
Basaria S, Coviello AD, Travison TG, Storer TW, Farwell WR, Jette AM, Eder R, Tennstedt S, Ulloor J, Zhang A, Choong K, Lakshman KM, Mazer NA, Miciek R, Krasnoff J, Elmi A, Knapp PE, Brooks B, Appleman E, Aggarwal S, Bhasin G, Hede-Brierley L, Bhatia A, Collins L, LeBrasseur N, Fiore LD, Bhasin S (2010) Adverse events associated with testosterone administration. N Engl J Med 363:109–122. https://doi.org/10.1056/NEJMoa1000485
Rogers MA, Evans WJ (1993) Changes in skeletal muscle with aging: effects of exercise training. Exerc Sport Sci Rev 21:65–102
Wolfe RR (2006) The underappreciated role of muscle in health and disease. Am J Clin Nutr 84:475–482. https://doi.org/10.1093/ajcn/84.3.475
Antonio J, Wilson JD, George FW (1999) Effects of castration and androgen treatment on androgen-receptor levels in rat skeletal muscles. J Appl Physiol (Bethesda, Md: 1985) 87:2016–2019. https://doi.org/10.1152/jappl.1999.87.6.2016
Bricout VA, Serrurier BD, Bigard AX, Guezennec CY (1999) Effects of hindlimb suspension and androgen treatment on testosterone receptors in rat skeletal muscles. Eur J Appl Physiol 79:443–448. https://doi.org/10.1007/s004210050535
Monks DA, Kopachik W, Breedlove SM, Jordan CL (2006) Anabolic responsiveness of skeletal muscles correlates with androgen receptor protein but not mRNA. Can J Physiol Pharmacol 84:273–277. https://doi.org/10.1139/y05-157
Poole DC, Burnley M, Vanhatalo A, Rossiter HB, Jones AM (2016) Critical power: an important fatigue threshold in exercise physiology. Med Sci Sports Exerc 48:2320–2334. https://doi.org/10.1249/mss.0000000000000939
Billat VL, Mouisel E, Roblot N, Melki J (2005) Inter- and intrastrain variation in mouse critical running speed. J Appl Physiol (1985) 98:1258–1263. https://doi.org/10.1152/japplphysiol.00991.2004
Takahashi K, Kitaoka Y, Yamamoto K, Matsunaga Y, Hatta H (2020) Oral lactate administration additively enhances endurance training-induced increase in cytochrome C oxidase activity in mouse soleus muscle. Nutrients. https://doi.org/10.3390/nu12030770
Takahashi K, Kitaoka Y, Matsunaga Y, Hatta H (2020) Effect of post-exercise lactate administration on glycogen repletion and signaling activation in different types of mouse skeletal muscle. Curr Res Physiol 3:34–43. https://doi.org/10.1016/j.crphys.2020.07.002
Shonk CE, Boxer GE (1964) Enzyme patterns in human tissues. I. Methods for the determination of glycolytic enzymes. Cancer Res 24:709–721
Hoshino D, Yoshida Y, Holloway GP, Lally J, Hatta H, Bonen A (2012) Clenbuterol, a β2-adrenergic agonist, reciprocally alters PGC-1 alpha and RIP140 and reduces fatty acid and pyruvate oxidation in rat skeletal muscle. Am J Physiol Regul Integr Comp Physiol 302:R373-384. https://doi.org/10.1152/ajpregu.00183.2011
Srere PA (1969) Citrate synthase. Methods Enzymol 13:3–11. https://doi.org/10.1016/0076-6879(69)13005-0
Spinazzi M, Casarin A, Pertegato V, Salviati L, Angelini C (2012) Assessment of mitochondrial respiratory chain enzymatic activities on tissues and cultured cells. Nat Protoc 7:1235–1246. https://doi.org/10.1038/nprot.2012.058
Bass A, Brdiczka D, Eyer P, Hofer S, Pette D (1969) Metabolic differentiation of distinct muscle types at the level of enzymatic organization. Eur J Biochem 10:198–206. https://doi.org/10.1111/j.1432-1033.1969.tb00674.x
Kaczor JJ, Ziolkowski W, Popinigis J, Tarnopolsky MA (2005) Anaerobic and aerobic enzyme activities in human skeletal muscle from children and adults. Pediatr Res 57:331–335. https://doi.org/10.1203/01.Pdr.0000150799.77094.De
Takahashi K, Kitaoka Y, Matsunaga Y, Hatta H (2019) Effects of lactate administration on mitochondrial enzyme activity and monocarboxylate transporters in mouse skeletal muscle. Physiol Rep 7:e14224. https://doi.org/10.14814/phy2.14224
Enoki T, Yoshida Y, Lally J, Hatta H, Bonen A (2006) Testosterone increases lactate transport, monocarboxylate transporter (MCT) 1 and MCT4 in rat skeletal muscle. J Physiol 577:433–443. https://doi.org/10.1113/jphysiol.2006.115436
Yoshida Y, Hatta H, Kato M, Enoki T, Kato H, Bonen A (2004) Relationship between skeletal muscle MCT1 and accumulated exercise during voluntary wheel running. J Appl Physiol 97:527–534. https://doi.org/10.1152/japplphysiol.01347.2003
Kitaoka Y, Machida M, Takemasa T, Hatta H (2011) Expression of monocarboxylate transporter (MCT) 1 and MCT4 in overloaded mice plantaris muscle. J Physiol Sci 61:467–472. https://doi.org/10.1007/s12576-011-0167-6
Bergström J, Hermansen L, Hultman E, Saltin B (1967) Diet, muscle glycogen and physical performance. Acta Physiol Scand 71:140–150. https://doi.org/10.1111/j.1748-1716.1967.tb03720.x
Poole DC, Rossiter HB, Brooks GA, Gladden LB (2021) The anaerobic threshold: 50+ years of controversy. J Physiol 599:737–767. https://doi.org/10.1113/jp279963
Hearris MA, Hammond KM, Seaborne RA, Stocks B, Shepherd SO, Philp A, Sharples AP, Morton JP (1985) Louis JB (2019) Graded reductions in preexercise muscle glycogen impair exercise capacity but do not augment skeletal muscle cell signaling: implications for CHO periodization. J Appl Physiol 126:1587–1597. https://doi.org/10.1152/japplphysiol.00913.2018
Holloszy JO, Coyle EF (1984) Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J Appl Physiol 56:831–838. https://doi.org/10.1152/jappl.1984.56.4.831
Tanner LB, Goglia AG, Wei MH, Sehgal T, Parsons LR, Park JO, White E, Toettcher JE, Rabinowitz JD (2018) Four key steps control glycolytic flux in mammalian cells. Cell Syst 7:49-62.e48. https://doi.org/10.1016/j.cels.2018.06.003
Spriet LL, Howlett RA, Heigenhauser GJ (2000) An enzymatic approach to lactate production in human skeletal muscle during exercise. Med Sci Sports Exerc 32:756–763
Fueger PT, Heikkinen S, Bracy DP, Malabanan CM, Pencek RR, Laakso M, Wasserman DH (2003) Hexokinase II partial knockout impairs exercise-stimulated glucose uptake in oxidative muscles of mice. Am J Physiol Endocrinol Metab 285:E958-963. https://doi.org/10.1152/ajpendo.00190.2003
Fueger PT, Shearer J, Krueger TM, Posey KA, Bracy DP, Heikkinen S, Laakso M, Rottman JN, Wasserman DH (2005) Hexokinase II protein content is a determinant of exercise endurance capacity in the mouse. J Physiol 566:533–541. https://doi.org/10.1113/jphysiol.2005.085043
Fueger PT, Li CY, Ayala JE, Shearer J, Bracy DP, Charron MJ, Rottman JN, Wasserman DH (2007) Glucose kinetics and exercise tolerance in mice lacking the GLUT4 glucose transporter. J Physiol 582:801–812. https://doi.org/10.1113/jphysiol.2007.132902
Rogatzki MJ, Ferguson BS, Goodwin ML, Gladden LB (2015) Lactate is always the end product of glycolysis. Front Neurosci 9:22. https://doi.org/10.3389/fnins.2015.00022
Benjamin D, Robay D, Hindupur SK, Pohlmann J, Colombi M, El-Shemerly MY, Maira SM, Moroni C, Lane HA, Hall MN (2018) Dual Inhibition of the lactate transporters MCT1 and MCT4 is synthetic lethal with metformin due to NAD+ depletion in cancer cells. Cell Rep 25:3047-3058.e3044. https://doi.org/10.1016/j.celrep.2018.11.043
Benton CR, Campbell SE, Tonouchi M, Hatta H, Bonen A (2004) Monocarboxylate transporters in subsarcolemmal and intermyofibrillar mitochondria. Biochem Biophys Res Commun 323:249–253. https://doi.org/10.1016/j.bbrc.2004.08.084
Dimmer KS, Friedrich B, Lang F, Deitmer JW, Broer S (2000) The low-affinity monocarboxylate transporter MCT4 is adapted to the export of lactate in highly glycolytic cells. Biochem J 350(Pt 1):219–227
Halestrap AP (2013) Monocarboxylic acid transport. Compr Physiol 3:1611–1643. https://doi.org/10.1002/cphy.c130008
Semenza GL (2000) HIF-1: mediator of physiological and pathophysiological responses to hypoxia. J Appl Physiol (Bethesda, Md: 1985) 88:1474–1480. https://doi.org/10.1152/jappl.2000.88.4.1474
Dang CV, Le A, Gao P (2009) MYC-induced cancer cell energy metabolism and therapeutic opportunities. Clin Cancer Res 15:6479–6483. https://doi.org/10.1158/1078-0432.Ccr-09-0889
Quarmby VE, Beckman WC Jr, Wilson EM, French FS (1987) Androgen regulation of c-myc messenger ribonucleic acid levels in rat ventral prostate. Mol Endocrinol 1:865–874. https://doi.org/10.1210/mend-1-12-865
Seth A, Steel JH, Nichol D, Pocock V, Kumaran MK, Fritah A, Mobberley M, Ryder TA, Rowlerson A, Scott J, Poutanen M, White R, Parker M (2007) The transcriptional corepressor RIP140 regulates oxidative metabolism in skeletal muscle. Cell Metab 6:236–245. https://doi.org/10.1016/j.cmet.2007.08.004
Carascossa S, Gobinet J, Georget V, Lucas A, Badia E, Castet A, White R, Nicolas JC, Cavaillès V, Jalaguier S (2006) Receptor-interacting protein 140 is a repressor of the androgen receptor activity. Mol Endocrinol 20:1506–1518. https://doi.org/10.1210/me.2005-0286
Massie CE, Lynch A, Ramos-Montoya A, Boren J, Stark R, Fazli L, Warren A, Scott H, Madhu B, Sharma N, Bon H, Zecchini V, Smith DM, Denicola GM, Mathews N, Osborne M, Hadfield J, Macarthur S, Adryan B, Lyons SK, Brindle KM, Griffiths J, Gleave ME, Rennie PS, Neal DE, Mills IG (2011) The androgen receptor fuels prostate cancer by regulating central metabolism and biosynthesis. EMBO J 30:2719–2733. https://doi.org/10.1038/emboj.2011.158
Larsen S, Nielsen J, Hansen CN, Nielsen LB, Wibrand F, Stride N, Schroder HD, Boushel R, Helge JW, Dela F, Hey-Mogensen M (2012) Biomarkers of mitochondrial content in skeletal muscle of healthy young human subjects. J Physiol 590:3349–3360. https://doi.org/10.1113/jphysiol.2012.230185
Hood DA, Memme JM, Oliveira AN, Triolo M (2019) Maintenance of skeletal muscle mitochondria in health, exercise, and aging. Annu Rev Physiol 81:19–41. https://doi.org/10.1146/annurev-physiol-020518-114310
Scheller K, Sekeris CE (2003) The effects of steroid hormones on the transcription of genes encoding enzymes of oxidative phosphorylation. Exp Physiol 88:129–140. https://doi.org/10.1113/eph8802507
Psarra AM, Sekeris CE (2008) Steroid and thyroid hormone receptors in mitochondria. IUBMB Life 60:210–223. https://doi.org/10.1002/iub.37
Gavrilova-Jordan LP, Price TM (2007) Actions of steroids in mitochondria. Semin Reprod Med 25:154–164. https://doi.org/10.1055/s-2007-973428
Wu Z, Puigserver P, Andersson U, Zhang C, Adelmant G, Mootha V, Troy A, Cinti S, Lowell B, Scarpulla RC, Spiegelman BM (1999) Mechanisms controlling mitochondrial biogenesis and respiration through the thermogenic coactivator PGC-1. Cell 98:115–124. https://doi.org/10.1016/s0092-8674(00)80611-x
Rossetti ML, Gordon BS (2017) The role of androgens in the regulation of muscle oxidative capacity following aerobic exercise training. Appl Physiol Nutr Metab 42:1001–1007. https://doi.org/10.1139/apnm-2017-0230
Usui T, Kajita K, Kajita T, Mori I, Hanamoto T, Ikeda T, Okada H, Taguchi K, Kitada Y, Morita H, Sasaki T, Kitamura T, Sato T, Kojima I, Ishizuka T (2014) Elevated mitochondrial biogenesis in skeletal muscle is associated with testosterone-induced body weight loss in male mice. FEBS Lett 588:1935–1941. https://doi.org/10.1016/j.febslet.2014.03.051
Jackson KC, Wohlers LM, Lovering RM, Schuh RA, Maher AC, Bonen A, Koves TR, Ilkayeva O, Thomson DM, Muoio DM, Spangenburg EE (2013) Ectopic lipid deposition and the metabolic profile of skeletal muscle in ovariectomized mice. Am J Physiol Regul Integr Comp Physiol 304:R206-217. https://doi.org/10.1152/ajpregu.00428.2012
Cavalcanti-de-Albuquerque JP, Salvador IC, Martins EL, Jardim-Messeder D, Werneck-de-Castro JP, Galina A, Carvalho DP (2014) Role of estrogen on skeletal muscle mitochondrial function in ovariectomized rats: a time course study in different fiber types. J Appl Physiol (Bethesda, Md: 1985) 116:779–789. https://doi.org/10.1152/japplphysiol.00121.2013
Dubouchaud H, Butterfield GE, Wolfel EE, Bergman BC, Brooks GA (2000) Endurance training, expression, and physiology of LDH, MCT1, and MCT4 in human skeletal muscle. Am J Physiol Endocrinol Metab 278:E571–E579
McCullagh KJ, Poole RC, Halestrap AP, O’Brien M, Bonen A (1996) Role of the lactate transporter (MCT1) in skeletal muscles. Am J Physiol 271:E143-150. https://doi.org/10.1152/ajpendo.1996.271.1.E143
Pilegaard H, Terzis G, Halestrap A, Juel C (1999) Distribution of the lactate/H+ transporter isoforms MCT1 and MCT4 in human skeletal muscle. Am J Physiol 276:E843-848. https://doi.org/10.1152/ajpendo.1999.276.5.E843
Wilson MC, Jackson VN, Heddle C, Price NT, Pilegaard H, Juel C, Bonen A, Montgomery I, Hutter OF, Halestrap AP (1998) Lactic acid efflux from white skeletal muscle is catalyzed by the monocarboxylate transporter isoform MCT3. J Biol Chem 273:15920–15926. https://doi.org/10.1074/jbc.273.26.15920
Kitaoka Y, Masuda H, Mukai K, Hiraga A, Takemasa T, Hatta H (2011) Effect of training and detraining on monocarboxylate transporter (MCT) 1 and MCT4 in Thoroughbred horses. Exp Physiol 96:348–355. https://doi.org/10.1113/expphysiol.2010.055483
Benton CR, Yoshida Y, Lally J, Han XX, Hatta H, Bonen A (2008) PGC-1alpha increases skeletal muscle lactate uptake by increasing the expression of MCT1 but not MCT2 or MCT4. Physiol Genomics 35:45–54. https://doi.org/10.1152/physiolgenomics.90217.2008
Benton CR, Nickerson JG, Lally J, Han XX, Holloway GP, Glatz JF, Luiken JJ, Graham TE, Heikkila JJ, Bonen A (2008) Modest PGC-1alpha overexpression in muscle in vivo is sufficient to increase insulin sensitivity and palmitate oxidation in subsarcolemmal, not intermyofibrillar, mitochondria. J Biol Chem 283:4228–4240. https://doi.org/10.1074/jbc.M704332200
Richter EA, Sylow L, Hargreaves M (2021) Interactions between insulin and exercise. Biochem J 478:3827–3846. https://doi.org/10.1042/bcj20210185
Järhult J, Holst J (1979) The role of the adrenergic innervation to the pancreatic islets in the control of insulin release during exercise in man. Pflugers Arch 383:41–45. https://doi.org/10.1007/bf00584473
Wasserman DH, Cherrington AD (1991) Hepatic fuel metabolism during muscular work: role and regulation. Am J Physiol 260:E811-824. https://doi.org/10.1152/ajpendo.1991.260.6.E811
Wolfe RR, Nadel ER, Shaw JH, Stephenson LA, Wolfe MH (1986) Role of changes in insulin and glucagon in glucose homeostasis in exercise. J Clin Invest 77:900–907. https://doi.org/10.1172/jci112388
Zinker BA, Mohr T, Kelly P, Namdaran K, Bracy DP, Wasserman DH (1994) Exercise-induced fall in insulin: mechanism of action at the liver and effects on muscle glucose metabolism. Am J Physiol 266:E683-689. https://doi.org/10.1152/ajpendo.1994.266.5.E683
Dubois V, Laurent MR, Jardi F, Antonio L, Lemaire K, Goyvaerts L, Deldicque L, Carmeliet G, Decallonne B, Vanderschueren D, Claessens F (2016) Androgen deficiency exacerbates high-fat diet-induced metabolic alterations in male mice. Endocrinology 157:648–665. https://doi.org/10.1210/en.2015-1713
López-Soldado I, Guinovart JJ, Duran J (2021) Increased liver glycogen levels enhance exercise capacity in mice. J Biol Chem 297:100976. https://doi.org/10.1016/j.jbc.2021.100976
Boden G, Chen X, Desantis RA, Kendrick Z (1993) Effects of insulin on fatty acid reesterification in healthy subjects. Diabetes 42:1588–1593. https://doi.org/10.2337/diab.42.11.1588
Campbell PJ, Carlson MG, Hill JO, Nurjhan N (1992) Regulation of free fatty acid metabolism by insulin in humans: role of lipolysis and reesterification. Am J Physiol 263:E1063-1069. https://doi.org/10.1152/ajpendo.2006.263.6.E1063
Romijn JA, Coyle EF, Sidossis LS, Zhang XJ, Wolfe RR (1995) Relationship between fatty acid delivery and fatty acid oxidation during strenuous exercise. J Appl Physiol (1985) 79:1939–1945. https://doi.org/10.1152/jappl.1995.79.6.1939
Costill DL, Coyle E, Dalsky G, Evans W, Fink W, Hoopes D (1977) Effects of elevated plasma FFA and insulin on muscle glycogen usage during exercise. J Appl Physiol Respir Environ Exerc Physiol 43:695–699
Augusto V, Padovani CR, Campos GER (2017) Skeletal muscle fiber types in C57BL6J mice. J Morphol Sci 21:0–0
Costill DL, Daniels J, Evans W, Fink W, Krahenbuhl G, Saltin B (1976) Skeletal muscle enzymes and fiber composition in male and female track athletes. J Appl Physiol 40:149–154. https://doi.org/10.1152/jappl.1976.40.2.149
Gollnick PD, Armstrong RB, Saubert CWt, Piehl K, Saltin B (1972) Enzyme activity and fiber composition in skeletal muscle of untrained and trained men. J Appl Physiol 33:312–319. https://doi.org/10.1152/jappl.1972.33.3.312
Roberts AD, Billeter R, Howald H (1982) Anaerobic muscle enzyme changes after interval training. Int J Sports Med 3:18–21. https://doi.org/10.1055/s-2008-1026055
Fournier M, Ricci J, Taylor AW, Ferguson RJ, Montpetit RR, Chaitman BR (1982) Skeletal muscle adaptation in adolescent boys: sprint and endurance training and detraining. Med Sci Sports Exerc 14:453–456. https://doi.org/10.1249/00005768-198206000-00008
MacDougall JD, Hicks AL, MacDonald JR, McKelvie RS, Green HJ, Smith KM (1998) Muscle performance and enzymatic adaptations to sprint interval training. J Appl Physiol (Bethesda, Md: 1985) 84:2138–2142. https://doi.org/10.1152/jappl.1998.84.6.2138
Perry CG, Heigenhauser GJ, Bonen A, Spriet LL (2008) High-intensity aerobic interval training increases fat and carbohydrate metabolic capacities in human skeletal muscle. Appl Physiol Nutr Metab 33:1112–1123. https://doi.org/10.1139/h08-097
Hoshino D, Yoshida Y, Kitaoka Y, Hatta H, Bonen A (2013) High-intensity interval training increases intrinsic rates of mitochondrial fatty acid oxidation in rat red and white skeletal muscle. Appl Physiol Nutr Metab 38:326–333. https://doi.org/10.1139/apnm-2012-0257
Abe T, Kitaoka Y, Kikuchi DM, Takeda K, Numata O, Takemasa T (2015) High-intensity interval training-induced metabolic adaptation coupled with an increase in Hif-1alpha and glycolytic protein expression. J Appl Physiol (Bethesda, Md: 1985) 119:1297–1302. https://doi.org/10.1152/japplphysiol.00499.2015
Russell AP, Foletta VC, Snow RJ, Wadley GD (2014) Skeletal muscle mitochondria: a major player in exercise, health and disease. Biochem Biophys Acta 1840:1276–1284. https://doi.org/10.1016/j.bbagen.2013.11.016
Fitts RH, Booth FW, Winder WW, Holloszy JO (1975) Skeletal muscle respiratory capacity, endurance, and glycogen utilization. Am J Physiol 228:1029–1033. https://doi.org/10.1152/ajplegacy.1975.228.4.1029
Joyner MJ, Coyle EF (2008) Endurance exercise performance: the physiology of champions. J Physiol 586:35–44. https://doi.org/10.1113/jphysiol.2007.143834
Pugh CW, Ratcliffe PJ (2003) Regulation of angiogenesis by hypoxia: role of the HIF system. Nat Med 9:677–684. https://doi.org/10.1038/nm0603-677
Sieveking DP, Lim P, Chow RW, Dunn LL, Bao S, McGrath KC, Heather AK, Handelsman DJ, Celermajer DS, Ng MK (2010) A sex-specific role for androgens in angiogenesis. J Exp Med 207:345–352. https://doi.org/10.1084/jem.20091924
Mitchell EA, Martin NRW, Bailey SJ, Ferguson RA (2018) Critical power is positively related to skeletal muscle capillarity and type I muscle fibers in endurance-trained individuals. J Appl Physiol (1985) 125:737–745. https://doi.org/10.1152/japplphysiol.01126.2017
Hudlická O (1977) Effect of training on macro- and microcirculatory changes in exercise. Exerc Sport Sci Rev 5:181–230
Poole DC, Mathieu-Costello O, West JB (1989) Capillary tortuosity in rat soleus muscle is not affected by endurance training. Am J Physiol 256:H1110-1116. https://doi.org/10.1152/ajpheart.1989.256.4.H1110
Nunomiya A, Shin J, Kitajima Y, Dan T, Miyata T, Nagatomi R (2017) Activation of the hypoxia-inducible factor pathway induced by prolyl hydroxylase domain 2 deficiency enhances the effect of running training in mice. Acta Physiol (Oxf) 220:99–112. https://doi.org/10.1111/apha.12751
Arany Z, Foo SY, Ma Y, Ruas JL, Bommi-Reddy A, Girnun G, Cooper M, Laznik D, Chinsomboon J, Rangwala SM, Baek KH, Rosenzweig A, Spiegelman BM (2008) HIF-independent regulation of VEGF and angiogenesis by the transcriptional coactivator PGC-1alpha. Nature 451:1008–1012. https://doi.org/10.1038/nature06613
Chinsomboon J, Ruas J, Gupta RK, Thom R, Shoag J, Rowe GC, Sawada N, Raghuram S, Arany Z (2009) The transcriptional coactivator PGC-1alpha mediates exercise-induced angiogenesis in skeletal muscle. Proc Natl Acad Sci USA 106:21401–21406. https://doi.org/10.1073/pnas.0909131106
Kano Y, Miura S, Eshima H, Ezaki O (1985) Poole DC (2014) The effects of PGC-1α on control of microvascular P(O2) kinetics following onset of muscle contractions. J Appl Physiol 117:163–170. https://doi.org/10.1152/japplphysiol.00080.2014
Lin J, Wu H, Tarr PT, Zhang C-Y, Wu Z, Boss O, Michael LF, Puigserver P, Isotani E, Olson EN, Lowell BB, Bassel-Duby R, Spiegelman BM (2002) Transcriptional co-activator PGC-1α drives the formation of slow-twitch muscle fibres. Nature 418:797. https://doi.org/10.1038/nature00904
Liu Y, Christensen PM, Hellsten Y, Gliemann L (2022) Effects of exercise training intensity and duration on skeletal muscle capillarization in healthy subjects: a meta-analysis. Med Sci Sports Exerc. https://doi.org/10.1249/mss.0000000000002955
Acknowledgements
Not applicable.
Funding
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (Grant numbers 20H04071 [to Y. K. and H. H.] and 21K21249 [to K. T.]).
Author information
Authors and Affiliations
Contributions
KT designed the study, performed all experiments, interpreted the results, and wrote the first draft of the manuscript. YK and HH designed the experiments, interpreted the results, and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent of participate
All experiments were reviewed and approved by the Animal Experimental Committee of The University of Tokyo (No. 2021-1).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Takahashi, K., Kitaoka, Y. & Hatta, H. Effects of endurance training on metabolic enzyme activity and transporter protein levels in the skeletal muscles of orchiectomized mice. J Physiol Sci 72, 14 (2022). https://doi.org/10.1186/s12576-022-00839-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12576-022-00839-z