
Abstract
Background
Cystitis glandularis a rare benign proliferative disease of the urinary bladder mucosa is usually a microscopic finding and manifests rarely as a large visible macroscopic lesion of urinary bladder. Only few cases of cystitis glandularis presenting as urinary bladder mass in female patients have been reported in the literature. We are reporting a case of cystitis glandularis presenting as a urinary bladder mass in a very young female patient.
Case presentation.
Our patient, a young female 25 years of age presented in the Urology OPD with complaints of irritative lower urinary tract symptoms for two years and intermittent hematuria for one year. On evaluation, she was found to have a urinary bladder mass. Transurethral resection of her urinary bladder mass was done and on histopathological examination, it came out to be cystitis glandularis.
Conclusion
Clinical presentation of cystitis glandularis is variable. It may remain asymptomatic or could present as irritative lower urinary tract symptoms, hematuria, or mucus in the urine. It is normally a microscopic finding but could also present as an overt urinary bladder mass however this has been reported rarely in the literature.
Similar content being viewed by others


1 Background
Cystitis glandularis is a very rare benign proliferative disease of the urinary bladder mucosa. The commonly affected age group is fifth and sixth decades of life. It is usually a microscopic finding and manifests rarely as a large visible macroscopic lesion of urinary bladder. However, cases of cystitis glandularis presenting as urinary bladder mass have been reported in the literature, very few such cases have been reported in female patients [1, 2].
Semins MJ reported a case of 32 yrs old female patient who was being evaluated for miscarriage. During her workup, a urinary bladder mass was found on pelvic ultrasound. Its histopathological analysis was suggestive of cystitis glandularis [3].
Shigehara et al. have reported a case of cystitis glandularis forming a tumorous lesion with blueberry spots in a 49 yrs old female patient [4].
Harrison S et al. also reported a case of 49 yrs old female patient who presented with nocturia, dysuria, intermittent hematuria and sensation of residual urine. On evaluation, she was found to have urinary bladder mass and on pathological examination it came out to be cystitis glandularis [2].
We present a case of young female of 25 yrs in age, who presented with complaints of irritative lower urinary tract symptoms and intermittent hematuria. Her USG abdomen, CT Urography, and cystoscopic examination revealed a urinary bladder mass. A complete transurethral resection was done. Findings of histopathological analysis were consistent for cystitis glandularis. Our case report will add in the literature a young female patient with cystitis glandularis forming a urinary bladder mass.
2 Case presentation
We present a case of young married female, 25 years of age who presented in the Urology OPD with complaints of irritative lower urinary tract symptoms for two years and intermittent hematuria for one year. Her lower urinary tract symptoms included increased urinary frequency, urgency, and nocturia. Her hematuria was gross, intermittent, total, and sometimes associated with passage of clots. There was no history of fever and burning micturition. There was no history of obstructive lower urinary tract symptoms and acute urinary retention, any chronic illness like hypertension, diabetes mellitus, tuberculosis, coronary artery disease, etc., any other major complaints, any urological intervention or surgery in the past, and any kind of addiction. Her general and systemic examination were apparently normal and could not add any positive finding in her clinical case. Her haemogram, kidney function test, liver function test, and coagulation profile were within normal range except for slightly decreased hemoglobin. Her urine microscopic examination was positive for hematuria, however, her urine culture was sterile and urine cytology was negative for any malignant cells. Her USG whole abdomen was suggestive of a well-circumscribed soft tissue lesion in the urinary bladder near left vesicoureteric junction. Her CT urography was suggestive of a polypoid mass of size approximately 3.2 × 2.9 cm arising from inferoposterior and left lateral surface of urinary bladder and extending into bladder lumen (Fig. 1). Her cystoscopic examination revealed a single polypoid mass of size approximately 3 × 3 cm arising from inferoposterior and left lateral wall (Fig. 2). A complete transurethral resection of the mass was performed. Histopathological examination revealed gland-like lumens with columnar cells lining and surrounding chronic inflammatory cells infiltrate in the lamina propria (Fig. 3). These histopathological findings were suggestive of cystitis glandularis. There was no evidence of von Brunn nests, significant atypia, stromal reaction, muscular invasion, or any other evidence of malignancy on histopathological examination. The patient is in follow-up since her surgery almost one year back.

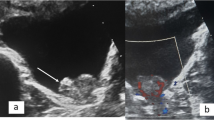
CT urography suggestive of a polypoid mass of size approximately 3.2 × 2.9 cm arising from inferoposterior and left lateral surface of urinary bladder and extending into bladder lumen

Cystoscopic examination revealing a single polypoid mass of size approximately 3 × 3 cm arising from inferoposterior and left lateral wall. This is a close view showing cystoscopic appearance of polypoidal mass

Histopathological examination revealing gland-like lumens with columnar cells lining and surrounding chronic inflammatory cells infiltrate in the lamina propria (H&E, 100X)
3 Discussion
Cystitis glandularis is a rare proliferative disorder of the mucus-producing glands within the mucosa and submucosa of urinary bladder epithelium [5]. It is commonly located on the lateral bladder wall, trigone, and the bladder neck [6]. It was first described by Morgagni in 1761 [7] and since then has been a topic of interest.
Different etiologies regarding its origin exist in the literature however it has been a matter of debate. One hypothesis believes it to be a result of abnormal embryologic development. As per this theory bladder, embryonic rests originate from either urachus or intestinal epithelium and get displaced during separation of the rectum from the urogenital sinus. However embryologic theory of origin was not accepted by all as cystitis glandularis also occurs in ureter and renal pelvis and currently this hypothesis has been abandoned. The second predominant hypothesis believes it to be a metaplastic change in the vesical mucosa due to inflammation and irritation. It leads to formation of Von Brunn nests along with degeneration of central cells and metaplasia of the surrounding cells to a columnar phenotype, which is consistent with cystitis glandularis. Many factors such as bladder exstrophy, pelvic lipohypertrophy, recurrent urinary tract infection, inflammation caused by urolithiasis, outflow obstruction and indwelling urethral or suprapubic catheter are considered to be risk factors for development of cystitis glandularis. Different other suggested etiological factors include avitaminosis, allergy, toxic products of metabolism, hormone imbalance, and specific carcinogens [3, 4, 7,8,9,10].
Clinical presentation of cystitis glandularis is variable. It could remain asymptomatic or could present as irritative lower urinary tract symptoms including dysuria, increased frequency, and urgency. It could also present as hematuria or mucus in the urine. It is normally a microscopic finding and an overt urinary bladder mass is extremely rare in the literature [1, 5, 11]. Its diagnosis is based on histological findings, however nowadays the role of CT and diffusion-weighted MRI is also being explored [12].
Natural history of cystitis glandularis regarding its premalignant potential is also a controversial topic. Shaw et al. in 1958 described a case of cystitis glandularis which gradually converted into adenocarcinoma [13]. Edwards et al. also documented the progression of cystitis glandularis to adenocarcinoma [14]. However, Davies et al. found no clinical evidence to label it a premalignant condition [7]. Similarly, Smith et al. in their study reported that Cystitis glandularis can be identified coincidentally with bladder carcinoma relatively frequently, although the long-term outcomes of their patient population have not supported the role of this condition as preneoplastic [15]. The results of Yi et al. also did not supported the premalignant potential of cystitis glandularis in their study, however, follow-up period in this study ranged from 0.5 years to 17 years [16].
Apart from management of risk factors of cystitis glandularis (inflammation and obstruction) and complete transurethral resection of the urinary bladder lesion, different other treatment modalities have also been reported in the literature. Yuksel OH et al. have reported the use of oral steroid for the treatment of intractable cystitis glandularis [17]. Takizawa et al. reported the use of celecoxib(a non-steroidal anti-inflammatory COX-2 selective inhibitor) for treatment of refractory cystitis glandularis [18]. Stillwell et al. reported use of whole bladder neodymium:YAG laser therapy for a case of severe cystitis glandularis of the entire bladder [19]. Black et al. reported a case of rapidly recurring cystitis glandularis who developed a low compliance small-capacity bladder and bilateral ureteral obstruction. They performed total cystoprostatectomy with cavernosal nerve-sparing and ileal neobladder construction [20].
Endoscopic resection is usually sufficient for symptomatic relief of patients, however, for severe and recurrent cases, extensive surgical management may be needed. After transurethral resection annual surveillance by cystoscopy with bladder biopsies is recommended, owing to risk of progression from cystitis glandularis to adenocarcinoma. Imaging and urinary cytology is also advocated [2].
Hu J et al. in their study revealed that the urinary infection, long-term indwelling catheter usage, urinary calculus, squamous metaplasia, and atypical hyperplasia were independent risk factors for CG recurrence [21].
4 Conclusions
Cystitis Glandularis is a rare proliferative condition of urinary bladder and usually presents as a microscopic finding. It is very rare to find a large visible macroscopic lesion of urinary bladder due to cystitis glandularis. Many more studies and work are required on this topic to solve different associated controversies and debate.
Availability of data and materials
Not applicable
Abbreviations
- OPD:
-
Out Patient Department
- USG:
-
Ultrasonography
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- COX-2:
-
Cyclooxygenase 2
- YAG:
-
Yttrium aluminium garnet
- H&E:
-
Hematoxylin and Eosin
References
Kaya C, Akpinar IN, Aker F, Turkeri LN (2007) Large Cystitis glandularis: a very rare cause of severe obstructive urinary symptoms in an adult. Int Urol Nephrol 39(2):441–444. https://doi.org/10.1007/s11255-006-9042-4
Harrison S, Lamchahab H, Djamal J, Jabbour Y, Alae T, Karmouni T, El Khader K, Koutani A, Andaloussi AIA (2018) Cystitis glandularis: a rare benign condition presenting as bladder tumor. Open Journal of Urology 8:336–343. https://doi.org/10.4236/oju.2018.812037
Semins MJ, Schoenberg MP (2007) A case of florid cystitis glandularis. Nat Clin Pract Urol 4(6):341–345. https://doi.org/10.1038/ncpuro0814
Shigehara K, Miyagi T, Nakashima T, Shimamura M (2008) Cystitis glandularis forming a tumorous lesion in the urinary bladder: a rare appearance of disease. Indian J Urol: IJU : J Urol Soc India 24(4):558–560. https://doi.org/10.4103/0970-1591.44268
Hochberg DA, Motta J, Brodherson MS (1998) Cystitis glandularis. Urology 51(1):112–113. https://doi.org/10.1016/s0090-4295(97)00502-5
Abasher A, Abdel Raheem A, Aldarrab R, Aldurayhim M, Attallah A, Banihani O (2020) Bladder outlet obstruction secondary to posterior urethral cystitis cystica & glandularis in a 12-year-old boy. A rare case scenario. Urol Case Rep 33:101425. https://doi.org/10.1016/j.eucr.2020.101425
Davies G, Castro JE (1977) Cystitis glandularis. Urology 10(2):128–129. https://doi.org/10.1016/0090-4295(77)90009-7
Liu XG, Chen ZQ, Ye ZQ (2007) Etiological Study on Cystitis Glandularis Caused by Bacterial Infection. J Huazhong Univ Sci Technol [Med Sci] 27:678–680. https://doi.org/10.1007/s11596-007-0615-y
Capozza N, Collura G, Nappo S, de Dominicis M, Francalanci P, Caione P (2005) Cystitis glandularis in children. BJU Int 95(3):411–413. https://doi.org/10.1111/j.1464-410X.2005.05311.x
Heyns CF, De Kock ML, Kirsten PH, van Velden DJ (1991) Pelvic lipomatosis associated with cystitis glandularis and adenocarcinoma of the bladder. J Urol 145(2):364–366. https://doi.org/10.1016/s0022-5347(17)38342-8
Agrawal A, Kumar D, Jha AA, Aggarwal P (2020) Incidence of adenocarcinoma bladder in patients with cystitis cystica et glandularis: A retrospective study. Indian J Urol: IJU: J Urol Soc India 36(4):297–302. https://doi.org/10.4103/iju.IJU_261_20
Wang HJ, Pui MH, Guo Y, Guan J, Zhang XL, Liu MJ, Li SR, Lin JH (2016) Preliminary study of diffusion-weighted MRI in the preoperative diagnosis of cystitis glandularis. Clin Radiol 71(9):937.e1-937.e9374. https://doi.org/10.1016/j.crad.2016.05.008
Shaw JL, Gislason GJ, Imbriglia JE (1958) Transition of cystitis glandularis to primary adenocarcinoma of the bladder. J Urol 79(5):815–822. https://doi.org/10.1016/s0022-5347(17)66349-3
Edwards PD, Hurm RA, Jaeschke WH (1972) Conversion of cystitis glandularis to adenocarcinoma. J Urol 108:568–570
Smith AK, Hansel DE, Jones JS (2008) Role of cystitis cystica et glandularis and intestinal metaplasia in development of bladder carcinoma. Urology 71(5):915–918. https://doi.org/10.1016/j.urology.2007.11.079
Yi X, Lu H, Wu Y, Shen Y, Meng Q, Cheng J, Tang Y, Wu F, Ou R, Jiang S, Bai X, Xie K (2014) Cystitis glandularis: A controversial premalignant lesion. Oncol Lett 8(4):1662–1664. https://doi.org/10.3892/ol.2014.2360
Yuksel OH, Urkmez A, Erdogru T, Verit A (2015) The role of steroid treatment in intractable cystitis glandularis: a case report and literature review. Can Urol Assoc J9(5–6):E306–E309. https://doi.org/10.5489/cuaj.2636
Takizawa N, Matsuzaki T, Yamamoto T, Mishima T, Miyasaka C, Tanaka S, Kinoshita H, Uemura Y, Yamada H, Matsuda T (2016) Novel strategy for cystitis glandularis: Oral treatment with cyclooxygenase-2 inhibitor. Int J Urol 23(8):706–708. https://doi.org/10.1111/iju.13121
Stillwell TJ, Patterson DE, Rife CC, Farrow GM (1988) Neodymium:YAG laser treatment of cystitis glandularis. J Urol 139(6):1298–1299. https://doi.org/10.1016/s0022-5347(17)42899-0
Black PC, Lange PH (2005) Cystoprostatectomy and neobladder construction for florid cystitis glandularis. Urology 65(1):174. https://doi.org/10.1016/j.urology.2004.07.026
Hu J, Li C, Guo X, Zhang H, Li H, Qiu D, Gong G, Liu P, Ren W, Chen J, Zu X (2020) Development and validation of a predictive nomogram for the risk of recurrence in patients with cystitis glandularis. Ann Transl Med 8(6):352. https://doi.org/10.21037/atm.2020.02.102
Acknowledgments
We are thankful to radiologists for their important role in the workup of our patient.
Funding
No source of funds.
Author information
Authors and Affiliations
Contributions
A.A. and N.R. made the clinical decision of the case and were having leading role in operative procedure and have helped to draft the manuscript. R.K.T. and M.Z.I. have done the research work related to topic and participated in manuscript writing. B.K. was responsible for histopathological diagnosis, and provision of the pathological microphotographs. Q.K. was involved in describing pathological findings and manuscript writing. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ahmad, A., Imbisat, M.Z., Ranjan, N. et al. Cystitis glandularis- rare cause of urinary bladder mass: case report and literature review. Afr J Urol 28, 11 (2022). https://doi.org/10.1186/s12301-022-00279-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-022-00279-6