
Abstract
Background
Migraine is responsible for significant disability and societal burden. Recently, drugs targeting the calcitonin gene-related peptide (CGRP) pathway raised new hopes. CGRP, a potent vasodilator, plays a key role in the pathogenesis of migraine attacks. The deficiency of CGRP is involved in Raynaud’s phenomenon, which consists of abnormal vasoconstriction of the digits. We aimed to assess the potential association of Raynaud’s phenomenon with CGRP-targeting drugs, analyzing real-world data from the World Health Organization (VigiBase®).
Methods
We queried all reports of Raynaud’s phenomenon involving a CGRP-targeting drug. We sought disproportionate reporting of Raynaud’s phenomenon with these drugs. For this purpose, we relied on the calculation of the Information Component (IC). A positive lower end of the 95% confidence interval (CI) of the IC defines a statistically significant association. As migraine patients are prone to Raynaud’s phenomenon, we also calculated the IC of Raynaud’s phenomenon with CGRP-targeting drugs compared to 5HT1B/D agonists (triptans), and beta-blockers used in the treatment of migraine.
Results
Overall, 99 reports of Raynaud’s phenomenon involving CGRP-targeting drugs have been yielded in VigiBase®. The most reported CGRP-targeting drug was erenumab, with 56 reports (56.6%). The median time to onset was 84 days. No fatality was notified, but one patient suffered from gangrene and extremity necrosis. As a whole, CGRP-targeting drugs were significantly associated with Raynaud’s phenomenon, with an IC of 3.3 (95%CI: 3.0–3.5). There was a disproportionate reporting of Raynaud’s phenomenon with CGRP-targeting drugs compared to triptans (IC 0.4; 95%CI: 0.1–0.6) and to beta-blockers (IC 0.5; 95%CI: 0.2–0.7) as well.
Conclusions
There is a significant disproportionality signal of Raynaud’s phenomenon with CGRP-targeting. This signal stands out when CGRP-targeting drugs are compared to other drugs used in patients with migraine. This study is limited by missing data in pharmacovigilance reports. CGRP-targeting drugs may be subject to Weber effect and reporting bias. Nonetheless, CGRP blockade might be the last straw that disrupts the physiological balance of vascular response in patients at-risk of Raynaud’s phenomenon. Pending further data regarding vascular safety of CGRP-targeting drugs, caution is warranted in these patients.
Similar content being viewed by others

Background
Migraine is a primary headache with complex pathophysiology involving trigeminovascular system activation [1, 2]. Migraine afflicts almost 15% of the population [3] and is responsible for significant disability and substantial societal burden [4]. Treatments for migraine patients can be divided into two categories, abortive treatments that relieve headaches, and prophylactic therapy that reduces the frequency of migraine attacks. Unfortunately, drugs used in migraine prevention had so far a limited success, in terms of efficacy as well as patient adherence, due to their side effects [5].
Recently, a new paradigm-shifting class of drugs targeting the calcitonin gene-related peptide (CGRP) pathway has revolutionized migraine treatment [6, 7]. CGRP is the main neuropeptide released by the trigeminal nerve, whose signaling may be a key mechanism underlying the pathogenesis of migraine attacks, as CGRP is a potent vasodilator [8]. Therapeutic strategies to damper CGRP signaling include monoclonal antibodies directed against CGRP (fremanezumab, galcanezumab, eptinezumab), or the CGRP receptor (erenumab), and gepants which are small molecule antagonists of the CGRP receptor (rimegepant, ubrogepant, atogepant) [2, 9]. CGRP-targeting drugs are considered to be effective and generally safe but there are still uncertainties [2, 10, 11].
Due to their mechanism of action, CGRP-targeting drugs could theoretically induce adverse drug reactions (ADRs) underlain by impaired arterial vasodilation [12]. It is known that patients with migraine are at increased risk of vascular events [13,14,15]. Yet, there is still limited knowledge regarding the vascular outcomes of CGRP-targeting drugs [12, 16]. The fact that patients with cardiovascular risk factors are often excluded from trial participation led the European Medicines Agency (EMA) to mention such an “important potential risk” in the Risk Management Plan of CGRP-targeting drugs, pending further pharmacovigilance data [17,18,19].
The deficiency of CGRP is believed to play a role in Raynaud’s phenomenon [20, 21]. Raynaud’s phenomenon is underpinned by a local defect in vascular response. It consists of abnormal vasoconstriction in response to various conditions, like cold temperatures or emotional stress. The consequence is sharply demarcated color changes of the skin of the digits. Raynaud’s phenomenon often accompanies migraine [22, 23]. Cases of Raynaud’s phenomenon induced or aggravated by CGRP-targeting drugs have recently been reported [24,25,26].
We aimed to assess the potential association of Raynaud’s phenomenon with CGRP-targeting drugs, relying on real-world data issued from the pharmacovigilance database of the World Health Organization (WHO).
Methods
Data source
The WHO Safety Database (VigiBase®) is managed by the Uppsala Monitoring Center (UMC) [27]. Since 1967, VigiBase® gathers Individual Case Safety Reports issued from the national pharmacovigilance networks of more than 172 countries. These post-marketing reports originate from healthcare professionals, patients, as well as pharmaceutical companies. The anonymity of both patients and reporters is preserved. Each report contains administrative information (country, reporter qualification), characteristics of the patients (sex, age), drugs (indication, start and end dates, dose, concomitant drugs), and ADRs (effects, seriousness, onset, outcome).
Query
All CGRP-targeting drugs belong to the N02CD class in the Anatomical Therapeutic Chemical (ATC) classification system: atogepant, eptinezumab, erenumab, fremanezumab, galcanezumab, olcegepant, rimegepant, telcagepant, ubrogepant, vazegepant. VigiBase® was queried for all reports containing the Preferred Term (PT) “Raynaud’s phenomenon” registered until January 31, 2022, and involving a CGRP-targeting drug (N02CD). In the Medical Dictionary for Regulatory Activities (MedDRA, version 24.1 [28]), the PT is defined as the distinct descriptor for a single medical concept [29]. To take into account coding heterogeneity, VigiBase® was also queried for all reports belonging to the High Level Term (HLT) “Peripheral Vasoconstriction, necrosis and vascular insufficiency” (which includes the PT “Raynaud’s phenomenon” inter alia) with a CGRP-targeting drug. Quantitative variables were described in terms of medians with interquartile ranges (IQR) and/or minimum-maximum ranges (min-max). Qualitative variables were described as numbers and proportions.
Disproportionality analysis
Disproportionality is a case/non-case analysis used to detect pharmacovigilance signals [30, 31]. If the proportion of reports with a specific ADR and a given drug (cases) is greater than the proportion of reports with the same ADR and other drugs (non-cases), an association between this drug and the ADR is suggested. Disproportionality can be assessed by the Information Component (IC), derived from a Bayesian confidence propagation neural network [32]. The IC is a tool validated by UMC. It compares observed and expected numbers of reports with an ADR-drug combination. This tool allows earlier and more specific detection of potential pharmacovigilance signals compared to the other measures, such as the reporting odds ratio. A positive lower end of the 95% confidence interval (CI) of the IC is the common threshold used in statistical signal detection at UMC.
In this study, we used disproportionality to detect whether Raynaud’s phenomenon was reported differentially with CGRP-targeting drugs, as compared to all other combinations of ADRs and active ingredients in VigiBase®. Specifically, we calculated the IC for the combination of each CGRP-targeting drug with Raynaud’s phenomenon. As a sensitivity analysis, the same analysis was performed with the HLT “Peripheral Vasoconstriction, necrosis and vascular insufficiency”.
Comparative disproportionality
As migraine patients are prone to Raynaud’s phenomenon, we sought whether CGRP-targeting drugs were still disproportionately involved in Raynaud’s phenomenon, when compared to 5HT1B/D agonists and to beta-blockers (atenolol, metoprolol, nadolol, propranolol, timolol) used in the treatment of migraine. Indeed, 5HT1B/D agonists (also known as triptans) and beta-blockers are widely used in patients suffering from migraine. Furthermore, both classes are known to induce Raynaud’s phenomenon per se [33,34,35,36]. This comparative disproportionality was calculated by the IC [37, 38]. This additional disproportionality analysis aimed to mitigate the impact of potential confounding factors in patients with migraine and to increase the specificity of any possible findings regarding CGRP-targeting drugs.
Results
Characteristics of the reports
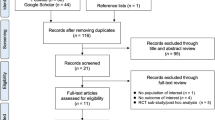
As of January 31, 2022, 172 reports involving CGRP-targeting drugs in VigiBase® belonged to the HLT “Peripheral Vasoconstriction, necrosis and vascular insufficiency”, including 99 reports under the PT “Raynaud’s phenomenon” and 58 reports under the PT “Peripheral coldness”.
Regarding reports of Raynaud’s phenomenon, most patients were female (86, 92.5%), with a median age of 45 years (IQR: 35–57; min-max: 20–70). The United States issued most reports and physicians were the most frequent reporters (Table 1).
Reports were mainly related to CGRP monoclonal antibodies. The most reported CGRP-targeting drugs were erenumab with 56 reports (56.6%), galcanezumab with 28 reports (28.3), and fremanezumab with 13 reports (13.1%). Ubrogepant and rimegepant accounted for one report each (1.0%). There was no report with eptinezumab, atogepant, or CGRP blockade with a concomitant monoclonal antibody and small molecule CGRP receptor antagonist.
Characteristics of reactions
The median time to onset was 84 days (IQR: 18–383). Median dose was 70 mg/month for erenumab (min-max: 70–140), 225 mg/month for fremanezumab (min-max: 225–225), and 120 mg/month for galcanezumab (min-max: 120–240). The ADR was deemed serious in 15 reports (15.2%), including 6 disabling and incapacitating cases. No fatality was notified, but one patient suffered from gangrene and extremity necrosis. The most frequently co-reported MedDRA terms were arthralgia (7 reports, 7.1%), alopecia (5 reports, 5.1%), condition aggravated (5 reports, 5.1%), constipation (4 reports, 4.0%), fatigue (4 reports, 4.0%), skin discoloration (4 reports, 4.0%), and weight increased (4 reports, 4.0%). Suspect co-reported active ingredients include propranolol in 3 reports (3.0%), rizatriptan and nadolol in 2 reports each (2.0%). CGRP antagonist was withdrawn in 23 reports (33.8%). Among 47 reports with available outcomes, Raynaud’s phenomenon did not recover in 31 reports (65.9%), was recovering in 3 reports (6.4%) and recovered in 13 reports (27.7%).
Disproportionality analysis
As a whole, CGRP-targeting drugs were significantly associated with Raynaud’s phenomenon, with an IC of 3.3 (95%CI: 3.0–3.5). Specifically, Raynaud’s phenomenon was disproportionately reported with erenumab (IC IC 3.2; 95%CI: 2.8–3.5), galcanezumab (IC 3.2; 95%CI: 2.6–3.7) and fremanezumab (IC 3.2; 95%CI: 2.3–3.8). The IC025 of ubrogepant and rimegepant did not reach statistical significance.
The whole HLT “Peripheral Vasoconstriction, necrosis and vascular insufficiency” yielded an IC of 0.3 (95%CI: 0.1–0.5). The PT “peripheral coldness” did not reach statistical significance (IC 0.37; 95%CI: 0.0–0.72).
Comparison with triptans and beta-blockers
As of January 31, 2022, 43 reports of Raynaud’s phenomenon were registered in VigiBase® with 5HT1 agonists. Given that 47,417 and 55,506 other ADRs were reported with 5HT1B/D agonists and CGRP antagonists, respectively, the comparative IC of Raynaud’s phenomenon with CGRP antagonists was 0.4 (95%CI: 0.1–0.6).
Likewise, 142 reports of Raynaud’s phenomenon were registered with the beta-blockers atenolol, metoprolol, nadolol, propranolol and timolol. Given that 129,222 other ADRs were reported with those beta-blockers, the comparative IC of Raynaud’s phenomenon with CGRP antagonists was 0.5 (95%CI: 0.2–0.7).
Discussion
Our analysis of the international pharmacovigilance database highlights a significant disproportionality signal of Raynaud’s phenomenon with CGRP-targeting drugs. This signal stands out even when CGRP-targeting drugs are compared to triptans. Yet, triptans are acute treatments of migraine, used in a similar population, and are known to induce Raynaud’s phenomenon [33, 34]. CGRP-targeting drugs are also more likely to be reported for Raynaud’s phenomenon than beta-blockers used as preventive treatments.
Women were represented in the overwhelming majority of reports, probably owing to the epidemiology of both migraine and Raynaud’s phenomenon [4, 39,40,41,42]. Furthermore, a hormonal influence on capsaicin-induced CGRP-mediated vasodilation of the skin has been described [43]. In our study, three CGRP monoclonal antibodies accounted for all but two reports. Erenumab, the front-runner of its class was the most frequently represented. Indeed, the oral small molecule CGRP antagonists were associated to Raynaud’s phenomenon in two reports only. This probably reflects the fact that ubrogepant and rimegepant are more recent, and less extensively used thus far. Moreover, ubrogepant and rimegepant are acute migraine treatments, so patients might be exposed to their potential ADRs for a shorter period, possibly decreasing the frequency of Raynaud’s phenomenon [44].
The involvement of the deficiency of CGRP in the pathogenesis of Raynaud’s phenomenon has been described as far back as the 1990s [20, 21]. These findings led to consider CGRP as a possible candidate to treat Raynaud’s phenomenon and systemic sclerosis [45,46,47]. In fact, CGRP receptor activation results in vasorelaxation and dilation of blood vessels [8, 48]. This mechanism likely underpins the involvement of CGRP-targeting drugs in Raynaud’s phenomenon. Accordingly, by decreasing CGRP release, triptans may alleviate migraine and in some cases induce Raynaud’s phenomenon [49, 50].
Yet, according to clinical trials, the cardiovascular safety profile of CGRP-targeting drugs is thus far reassuring [51]. The rate of vascular events between CGRP-targeting drugs and placebo-treated patients does not differ [12, 52, 53]. Nonetheless, real-life post-marketing pharmacovigilance data are extracted from a larger, non-selected, population of long-term treated patients. These data are paramount to detect a signal for potential ADRs, that might have escaped initial scrutiny [54].
In fact, in 2019, three cases of Raynaud’s phenomenon induced or exacerbated by CGRP monoclonal antibodies have been reported [24]. In addition, the safety of CGRP-targeting drugs among patients with Raynaud’s phenomenon has recently been assessed [25]. Microvascular complications occurred in 9 of 169 patients (5.3%), ranging from worsening Raynaud’s phenomenon to gangrene, requiring distal digit amputation. Broadly speaking, the long-term effects of CGRP blockade, especially in conditions of acute ischemia, still raise many questions [51, 55, 56].
The present study has several limitations. This signal, highlighted by the statistical analysis of quantitative data, needs further qualitative assessment. Despite the disproportionality analysis and the comparison with Raynaud’s phenomenon reported with triptans and beta-blockers, we cannot rule out the possibility that some reports were wrongly attributed to CGRP-targeting drugs. Available clinical data are too scarce to distinguish with certainty an aggravation of a preexisting Raynaud phenomenon from the new onset of a Raynaud phenomenon. Likewise, heterogeneity in the coding of outcomes prevents from precisely assessing the reversibility of Raynaud’s phenomenon. Indeed, some recoveries may apply to an isolated episode of Raynaud phenomenon, while others may relate to all Raynaud’s crises broadly. Another confounding factor may be that CGRP-targeting drugs are used in patients with severe migraines, possibly at higher risk of Raynaud’s phenomenon (even if no correlation has been described to date). Besides, our signal may be confounded by the Weber effect, whereby recent drugs are subject to a rise in ADR reporting during their first years of marketing [57, 58]. Healthcare professionals might also have been influenced by the notoriety bias due to increased awareness towards vascular safety of CGRP blockade [59]. Beta-blockers are not a perfect control group, as they are not exclusively used in patients with migraine. Head-to-head comparisons between drugs classes should not be extrapolated on. Pharmacovigilance studies cannot draw definite conclusions regarding the causal relationship between CGRP antagonists and Raynaud’s phenomenon. Nonetheless, the underlying mechanism appears plausible.
Conclusions
CGRP blockade might be the last straw that disrupts the physiological balance of vascular response in patients at-risk of Raynaud’s phenomenon. Although uncommon, Raynaud’s phenomenon triggered or aggravated by CGRP blockade may lead to serious complications. Pending further long-term data regarding vascular safety of CGRP-targeting drugs, caution is warranted when considering the use of those promising drugs in patients at-risk of Raynaud’s phenomenon.
Availability of data and materials
The data that support the findings of this study are available from Uppsala Monitoring Center (UMC) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Access to VigiBase® is available without fees to Dr. Fanny Rocher. Data are however available from the authors upon reasonable request and with permission of UMC.
Abbreviations
- ADR:
-
Adverse Drug Reaction
- ATC:
-
Anatomical Therapeutic Chemical
- CGRP:
-
Calcitonin Gene-Related Peptide
- CI:
-
Confidence Interval
- EMA:
-
European Medicines Agency
- HLT:
-
High Level Term
- IC:
-
Information Component
- IQR:
-
InterQuartile Range
- MedDRA:
-
Medical Dictionary for Regulatory Activities
- Min-max:
-
Minimum-maximum
- PT:
-
Preferred Term
- UMC:
-
Uppsala Monitoring Center
- WHO:
-
World Health Organization
References
Gross EC, Lisicki M, Fischer D et al (2019) The metabolic face of migraine — from pathophysiology to treatment. Nat Rev Neurol 15:627–643. https://doi.org/10.1038/s41582-019-0255-4
de Vries T, Villalón CM, MaassenVanDenBrink A (2020) Pharmacological treatment of migraine: CGRP and 5-HT beyond the triptans. Pharmacol Ther 211:107528. https://doi.org/10.1016/j.pharmthera.2020.107528
Steiner TJ, Stovner LJ, Birbeck GL (2013) Migraine: the seventh disabler. J Headache Pain 14:1. https://doi.org/10.1186/1129-2377-14-1
Vos T, Abajobir AA, Abate KH et al (2017) Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet 390:1211–1259. https://doi.org/10.1016/S0140-6736(17)32154-2
Bigal M, Rapoport A, Aurora S et al (2007) Satisfaction with current migraine therapy: experience from 3 centers in US and Sweden. Headache 47:475–479. https://doi.org/10.1111/j.1526-4610.2007.00752.x
Villalón CM, Olesen J (2009) The role of CGRP in the pathophysiology of migraine and efficacy of CGRP receptor antagonists as acute antimigraine drugs. Pharmacol Ther 124:309–323. https://doi.org/10.1016/j.pharmthera.2009.09.003
Urits I, Jones MR, Gress K et al (2019) CGRP antagonists for the treatment of chronic migraines: a comprehensive review. Curr Pain Headache Rep 23:29. https://doi.org/10.1007/s11916-019-0768-y
Edvinsson L, Haanes KA, Warfvinge K, Krause DN (2018) CGRP as the target of new migraine therapies — successful translation from bench to clinic. Nat Rev Neurol 14:338–350. https://doi.org/10.1038/s41582-018-0003-1
Tao X, Yan Z, Meng J et al (2022) The efficacy and safety of atogepant for the prophylactic treatment of migraine: evidence from randomized controlled trials. J Headache Pain 23:19. https://doi.org/10.1186/s10194-022-01391-2
Al-Hassany L, Goadsby PJ, Danser AHJ, MaassenVanDenBrink A (2022) Calcitonin gene-related peptide-targeting drugs for migraine: how pharmacology might inform treatment decisions. Lancet Neurol 21:284–294. https://doi.org/10.1016/S1474-4422(21)00409-9
Diener HC (2022) CGRP-targeted drugs for migraine: still many uncertainties. Lancet Neurol 21:209–210. https://doi.org/10.1016/S1474-4422(21)00468-3
Kudrow D, Pascual J, Winner PK et al (2020) Vascular safety of erenumab for migraine prevention. Neurology 94:e497–e510. https://doi.org/10.1212/WNL.0000000000008743
Kurth T, Rist PM, Ridker PM et al (2020) Association of Migraine with Aura and Other Risk Factors with Incident Cardiovascular Disease in women. JAMA 323:2281–2289. https://doi.org/10.1001/jama.2020.7172
Øie LR, Kurth T, Gulati S, Dodick DW (2020) Migraine and risk of stroke. J Neurol Neurosurg Psychiatry 91:593–604. https://doi.org/10.1136/jnnp-2018-318254
Magalhães JE, Sampaio Rocha-Filho PA (2018) Migraine and cerebrovascular diseases: epidemiology, pathophysiological, and clinical considerations. Headache: the journal of head and face. Pain 58:1277–1286. https://doi.org/10.1111/head.13378
Favoni V, Giani L, Al-Hassany L et al (2019) CGRP and migraine from a cardiovascular point of view: what do we expect from blocking CGRP? J Headache Pain 20:27. https://doi.org/10.1186/s10194-019-0979-y
EMA AIMOVIG (erenumab): Summary of the risk management plan. https://www.ema.europa.eu/en/documents/rmp-summary/aimovig-epar-risk-management-plan-summary_en.pdf. Accessed 1 Feb 2022
EMA EMGALITY (galcanezumab): Summary of the risk management plan. https://www.ema.europa.eu/en/documents/rmp-summary/emgality-epar-risk-management-plan-summary_en.pdf. Accessed 1 Feb 2022
EMA AJOVY (fremanezumab): Summary of the risk management plan. https://www.ema.europa.eu/en/documents/rmp-summary/ajovy-epar-risk-management-plan-summary_en.pdf. Accessed 1 Feb 2022
Bunker CB, Dowd PM, Terenghi G et al (1990) Deficiency of calcitonin gene-related peptide in Raynaud’s phenomenon. Lancet 336:1530–1533. https://doi.org/10.1016/0140-6736(90)93307-B
Bunker CB, Goldsmith PC, Leslie TA et al (1996) Calcitonin gene-related peptide, endothelin-1, the cutaneous microvasculature and Raynaud’s phenomenon. Br J Dermatol 134:399–406
Zahavi I, Chagnac A, Hering R et al (1984) Prevalence of Raynaud’s phenomenon in patients with migraine. Arch Intern Med 144:742–744
Voulgari PV, Alamanos Y, Papazisi D et al (2000) Prevalence of Raynaud’s phenomenon in a healthy Greek population. Ann Rheum Dis 59:206–210. https://doi.org/10.1136/ard.59.3.206
Evans RW (2019) Raynaud’s phenomenon associated with calcitonin gene-related peptide monoclonal antibody antagonists. Headache: the journal of head and face. Pain 59(1360–1364). https://doi.org/10.1111/head.13596
Breen ID, Brumfiel CM, Patel MH et al (2021) Evaluation of the safety of calcitonin gene-related peptide antagonists for migraine treatment among adults with Raynaud phenomenon. JAMA Netw Open 4:e217934. https://doi.org/10.1001/jamanetworkopen.2021.7934
Manickam AH, Buture A, Tomkins E, Ruttledge M (2021) Raynaud’s phenomenon secondary to erenumab in a patient with chronic migraine. Clin Case Rep 9:e04625. https://doi.org/10.1002/ccr3.4625
VigiBase UMC | Analytics in VigiLyze. https://www.who-umc.org/vigibase/vigilyze/analytics-in-vigilyze/. Accessed 3 Sep 2021
Welcome to MedDRA | MedDRA. https://www.meddra.org/. Accessed 14 Nov 2020
MedDRA Hierarchy | MedDRA. https://www.meddra.org/how-to-use/basics/hierarchy. Accessed 3 Sep 2021
Bate A, Evans SJW (2009) Quantitative signal detection using spontaneous ADR reporting: QUANTITATIVE SIGNAL DETECTION. Pharmacoepidem Drug Safe 18:427–436. https://doi.org/10.1002/pds.1742
Salem J-E, Manouchehri A, Moey M et al (2018) Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol 19:1579–1589. https://doi.org/10.1016/S1470-2045(18)30608-9
Bate A, Lindquist M, Edwards IR et al (1998) A Bayesian neural network method for adverse drug reaction signal generation. Eur J Clin Pharmacol 54:315–321. https://doi.org/10.1007/s002280050466
FDA IMITREX (sumatriptan): label. https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/020132s028,020626s025lbl.pdf. Accessed 1 Feb 2022
Bouquet E, Lavigne C, Urbanski G, Lainé-Cessac P (2015) Les syndromes de Raynaud d’origine médicamenteuse : analyse des données de la base nationale de pharmacovigilance. La Revue de Médecine Interne 36:A44. https://doi.org/10.1016/j.revmed.2015.03.273
Marshall AJ, Roberts CJ, Barritt DW (1976) Raynaud’s phenomenon as side effect of beta-blockers in hypertension. Br Med J 1:1498–1499. https://doi.org/10.1136/bmj.1.6024.1498
Khouri C, Blaise S, Carpentier P et al (2016) Drug-induced Raynaud’s phenomenon: beyond β-adrenoceptor blockers. Br J Clin Pharmacol 82:6–16. https://doi.org/10.1111/bcp.12912
Renoud L, Khouri C, Revol B et al (2021) Association of Facial Paralysis with mRNA COVID-19 vaccines: a disproportionality analysis using the World Health Organization Pharmacovigilance database. JAMA Intern Med 181:1243–1245. https://doi.org/10.1001/jamainternmed.2021.2219
Norén GN, Hopstadius J, Bate A (2013) Shrinkage observed-to-expected ratios for robust and transparent large-scale pattern discovery. Stat Methods Med Res 22:57–69. https://doi.org/10.1177/0962280211403604
Manzoni GC, Torelli P (2003) Epidemiology of migraine. J Headache Pain 4:s18–s22. https://doi.org/10.1007/s101940300003
Caponnetto V, Deodato M, Robotti M et al (2021) Comorbidities of primary headache disorders: a literature review with meta-analysis. J Headache Pain 22:71. https://doi.org/10.1186/s10194-021-01281-z
Burch RC, Loder S, Loder E, Smitherman TA (2015) The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache: the journal of head and face. Pain 55:21–34. https://doi.org/10.1111/head.12482
Suter LG, Murabito JM, Felson DT, Fraenkel L (2005) The incidence and natural history of Raynaud’s phenomenon in the community. Arthritis Rheum 52:1259–1263. https://doi.org/10.1002/art.20988
Vermeersch S, Frederiks P, Maassen VandenBrink A, de Hoon J (2013) Capsaicin-induced CGRP-mediated vasodilatation of the human skin: influence of gender, female hormones and migraine. J Headache Pain 14:P124. https://doi.org/10.1186/1129-2377-14-S1-P124
Kielbasa W, Helton DL (2019) A new era for migraine: pharmacokinetic and pharmacodynamic insights into monoclonal antibodies with a focus on galcanezumab, an anti-CGRP antibody. Cephalalgia 39:1284–1297. https://doi.org/10.1177/0333102419840780
Bunker CB, Reavley C, Dowd PM, O’Shaughnessy DJ (1993) Calcitonin gene-related peptide in treatment of severe peripheral vascular insufficiency in Raynaud’s phenomenon. Lancet 342:80–83. https://doi.org/10.1016/0140-6736(93)91286-U
Raynaud A, Cohen R, Modigliani E (1994) Calcitonin gene-related peptide (CGRP). Presse Med 23:171–175
Uslu U, Streiff L, Sticherling M (2018) Systemic therapy with calcitonin has positive clinical effects on systemic sclerosis in patients with cutaneous manifestations. Eur J Dermatol 28:364–369. https://doi.org/10.1684/ejd.2018.3300
Russell FA, King R, Smillie S-J et al (2014) Calcitonin gene-related peptide: physiology and pathophysiology. Physiol Rev 94:1099–1142. https://doi.org/10.1152/physrev.00034.2013
Arvieu L, Mauborgne A, Bourgoin S et al (1996) Sumatriptan inhibits the release of CGRP and substance P from the rat spinal cord. Neuroreport 7:1973–1976. https://doi.org/10.1097/00001756-199608120-00023
Kageneck C, Nixdorf-Bergweiler BE, Messlinger K, Fischer MJ (2014) Release of CGRP from mouse brainstem slices indicates central inhibitory effect of triptans and kynurenate. J Headache Pain 15:7. https://doi.org/10.1186/1129-2377-15-7
Messlinger K, MaassenVanDenBrink A (2019) Cardio- and cerebrovascular safety of erenumab, a monoclonal antibody targeting CGRP receptors – important studies on human isolated arteries. Cephalalgia 39:1731–1734. https://doi.org/10.1177/0333102419877169
Sun H, Dodick DW, Silberstein S et al (2016) Safety and efficacy of AMG 334 for prevention of episodic migraine: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol 15:382–390. https://doi.org/10.1016/S1474-4422(16)00019-3
Goadsby PJ, Reuter U, Hallström Y et al (2017) A controlled trial of Erenumab for episodic migraine. N Engl J Med 377:2123–2132. https://doi.org/10.1056/NEJMoa1705848
Mofid S, Bolislis WR, Kühler TC (2022) Real-world data in the Postapproval setting as applied by the EMA and the US FDA. Clin Ther. https://doi.org/10.1016/j.clinthera.2021.12.010
Sekiguchi N, Kanatsuka H, Sato K et al (1994) Effect of calcitonin gene-related peptide on coronary microvessels and its role in acute myocardial ischemia. Circulation 89:366–374. https://doi.org/10.1161/01.CIR.89.1.366
Rubio-Beltrán E, van den Brink AM (2019) Understanding CGRP and cardiovascular risk. In: Brain SD, Geppetti P (eds) Calcitonin gene-related peptide (CGRP) mechanisms: focus on migraine. Springer International Publishing, Cham, pp 131–140
Wallenstein EJ, Fife D (2001) Temporal patterns of NSAID spontaneous adverse event reports. Drug-Safety 24:233–237. https://doi.org/10.2165/00002018-200124030-00006
Hartnell NR, Wilson JP (2004) Replication of the weber effect using postmarketing adverse event reports voluntarily submitted to the United States Food and Drug Administration. Pharmacotherapy 24:743–749. https://doi.org/10.1592/phco.24.8.743.36068
Pariente A, Gregoire F, Fourrier-Reglat A et al (2007) Impact of safety alerts on measures of disproportionality in spontaneous reporting databases the notoriety Bias. Drug-Safety 30:891–898. https://doi.org/10.2165/00002018-200730100-00007
Acknowledgements
The authors acknowledge the UMC who manages and provided the data used in the present study. Access to VigiBase® is available without fees to Dr. Fanny Rocher. The views expressed in this article are the authors’ personal views and may not be understood or quoted as being made on behalf of or reflect the position of the ANSM, the EMA, the WHO, or one of their committees or working parties.
Funding
The authors do declare there is no source of funding for this study.
Author information
Authors and Affiliations
Contributions
AOG, DM, EKVO, AD, ML-M, MDD wrote the manuscript. AOG, DM, ML-M, MDD designed the research. AOG, DM, FR performed the research. AOG, DM analyzed the data. All authors read and approved the final manuscript.
Authors’ information
Not applicable.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics committee approval was not required for this observational study because the analysis was carried out on an anonymized pharmacovigilance database.
Consent for publication
Not applicable.
Competing interests
ML-M reports personal fee for advisory boards, speaker panels or investigation studies from Allergan, Amgen, Astellas, ATI, BMS, Boehringer, Boston Scientific, CoLucid, Convergence, GlaxoSmithKline, Grunenthal, Lilly, Lundbeck, Medtronic, MSD, Novartis, Pfizer, ReckittBenckiser, Saint-Jude, Sanofi-Aventis, Teva, UCB, UPSA and Zambon.
All other authors do declare no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gérard, A.O., Merino, D., Van Obberghen, E.K. et al. Calcitonin gene-related peptide-targeting drugs and Raynaud’s phenomenon: a real-world potential safety signal from the WHO pharmacovigilance database. J Headache Pain 23, 53 (2022). https://doi.org/10.1186/s10194-022-01424-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-022-01424-w