
Abstract
Background
An imbalance between inhibitory and excitatory neurometabolites has been implicated in chronic pain. Prior work identified elevated levels of Gamma-aminobutyric acid + macromolecules (“GABA+”) using magnetic resonance spectroscopy (MRS) in people with migraine. What is not understood is whether this increase in GABA+ is a cause, or consequence of living with, chronic migraine. Therefore, to further elucidate the nature of the elevated GABA+ levels reported in migraine, this study aimed to observe how GABA+ levels change in response to changes in the clinical characteristics of migraine over time.
Methods
We observed people with chronic migraine (ICHD-3) over 3-months as their treatment was escalated in line with the Australian Pharmaceutical Benefits Scheme (PBS). Participants underwent an MRS scan and completed questionnaires regarding migraine frequency, intensity (HIT-6) and disability (WHODAS) at baseline and following the routine 3 months treatment escalation to provide the potential for some participants to recover. We were therefore able to monitor changes in brain neurochemistry as clinical characteristics potentially changed over time.
Results
The results, from 18 participants who completed both baseline and follow-up measures, demonstrated that improvements in migraine frequency, intensity and disability were associated with an increase in GABA+ levels in the anterior cingulate cortex (ACC); migraine frequency (r = − 0.51, p = 0.03), intensity (r = − 0.51, p = 0.03) and disability (r = − 0.53, p = 0.02). However, this was not seen in the posterior cingulate gyrus (PCG). An incidental observation found those who happened to have their treatment escalated with CGRP-monoclonal antibodies (CGRP-mAbs) (n = 10) had a greater increase in ACC GABA+ levels (mean difference 0.54 IU IQR [0.02 to 1.05], p = 0.05) and reduction in migraine frequency (mean difference 10.3 IQR [2.52 to 18.07], p = 0.01) compared to those who did not (n = 8).
Conclusion
The correlation between an increase in ACC GABA+ levels with improvement in clinical characteristics of migraine, suggest previously reported elevated GABA+ levels may not be a cause of migraine, but a protective mechanism attempting to suppress further migraine attacks.
Similar content being viewed by others


Background
Migraine is the leading neurological cause of disability worldwide [1], with an estimated global prevalence of 14.7% [2]. Chronic migraine is defined by the International Classification of Headache disorders (ICHD-3) as headaches that persist for more than or equal to 15 days a month, with at least 8 of those days having features of migraine and persisting for at least 3-months [3]. Despite chronic migraine only representing 7.7% of the entire migraine population [4], compared to episodic migraine it is associated with higher healthcare utilization, work disability, and reduction in quality of life [5,6,7] . Even though recent treatments are showing better effects, the responsiveness rate remains less than 50%, leaving 50% of people with ongoing symptoms of chronic migraine [8, 9]. Treatment development is hindered by the limited understanding of the pathophysiology of chronic migraine. Given this, there is a global call to understand the mechanism of chronic migraine to enable the development of more effective treatment strategies [10].
Chronic migraine has been attributed to several proposed mechanisms involving both peripheral and central mediators. One proposed mechanism of migraine is an imbalance between the main inhibitory and excitatory neurometabolites, gamma-aminobutyric acid (GABA) and glutamate. Studying these metabolites has previously proved challenging owing to spectral overlap of more abundant neurometabolites at clinical magnetic resonance imaging (MRI) field strength [11]. However, Advanced 1H-Magnetic Resonance Spectroscopy (MRS) techniques such as MEGA-PRESS [12] address these limitations and allow for more reliable quantification of GABA or GABA+ co-edited macromolecules (GABA+) whilst also reporting the composite glutamate-glutamine-glutathione (Glx).
Several GABA/ GABA+ optimized cross-sectional MRS studies have investigated the imbalance of inhibition and excitation as a potential underlying cause of chronic migraine [13,14,15,16]. Our recent meta-analysis pooled results from 5 studies that reported levels of GABA and GABA+ in the anterior cingulate cortex (ACC), insula, occipital lobe and posterior cingulate cortex (PCG) and 6 studies that reported levels of Glx in the ACC, occipital lobe, PCG and thalamus of people with migraine [17]. We found GABA or GABA+ levels were significantly elevated in individuals with migraine compared to controls, yet there was no difference in Glx levels. These results challenge the concept of loss of inhibition leading to cortical hyperexcitability, where reduced levels of GABA compared to controls might be anticipated [18]. We might postulate that directional differences in GABA levels may be dependent on whether GABA is working within inhibitory or facilitatory circuits in the region being studied, which may result in either decreased or increased axonal firing respectively [19]. Nevertheless, this somewhat unexpected increase in GABA suggests a more complex relationship between the inhibitory and excitatory neurometabolites involved in migraine and warrants further investigation.
In investigating the role of neurometabolites in migraine, the region of brain to be examined must be considered. Studies of the PCG have demonstrated both elevated levels of GABA+ [14, 16] and an association between elevated GABA+ levels and central sensitization [20] in people with migraine. Another region, the ACC, has a well-established role in pain processing and modulation [21], and changes in ACC GABA+ levels have been reported in pain conditions such as fibromyalgia [22] and pelvic pain [23].
The elevated baseline levels of GABA+ observed in this cohort [24] and by others [14, 20, 25] have been proposed as a potential cause of migraine, due to being present in people with migraine but not in healthy controls. However, given the cross-sectional nature of the studies, the temporal and directional nature of these findings are unknown. Therefore, to further elucidate the nature of the elevated GABA+ levels in people with migraine, longitudinal studies, that examine the association between change in migraine characteristics (e.g. migraine frequency, pain intensity and disability) and change in GABA+ or Glx levels are required. Examining a cohort before and after treatment that is known to have a reasonable response rate (e.g. Onabotulinumtoxin A or calcitonin gene-related peptide monoclonal antibodies (CGRP-mAbs); response rate ~ 40% [8, 9], allows such an opportunity.
Aims
Our primary aim was to determine whether there is an association between change in GABA+ levels and change in migraine characteristics over time to further elucidate the nature of GABA’s role in migraine. Secondary aims were to determine whether there is an association between baseline neurometabolite levels and change in clinical characteristics and / or change in neurometabolite levels. This would establish whether baseline levels of GABA+ could predict change either clinically or neurochemically.
Methods
Study design
This study was a longitudinal cohort study, observing a group of migraine participants who formed part of a larger cross-sectional multi-group study [16].
Participants
There were 20 participants with chronic migraine with or without aura as diagnosed by the ICHD-3 [3] recruited by a neurologist (KN) working in private practice (4 males, 16 females, mean age 39.7 ± 10 years). To be eligible to receive treatment (Botox® or CGRP- mAbs) under the Australian Pharmaceutical Benefits Scheme (PBS), participants were required to have experienced an average of at least 15 headache days a month, (8 days of which migrainous) for over 6-months and having failed three or more prophylactic migraine medications [26]. In addition, they were required to have at least moderate headache related disability measured as a HIT-6 score [27] exceeding 50 at the time of recruitment. All participants were recruited when they were due to start a new treatment regimen based on escalating care in line with the PBS guidelines [26]. Participants were included if they received any peripherally acting evidence-based medication to escalate their care (e.g. Onabotulinumtoxin A, CGRP-monoclonal antibodies (CGRP-mAbs). Treatment could be escalated with either Onabotulinumtoxin A injections 155 mg administered 12 weekly according to the PREEMPT protocol [8] or CGRP-mAbs as erenumab 70 to 140 mg self-administered by injection monthly.
Participants were excluded if they were taking medication known to affect GABA levels at baseline (e.g. diazepam, topiramate or gabapentin), had contraindications to MRI (e.g. claustrophobia, MR-unsafe devices/implants) or conditions that compromised MR spectroscopy (e.g. metal braces). In addition, participants were excluded if they experienced any acute health complaints in the 5 days prior to the scan, were diagnosed with a psychiatric or neurological condition, experienced pain in other regions of the body, or if they were unable to communicate in the English language.
To test the reliability of collecting longitudinal MRS, 5 healthy participants (2 males, 3 females, mean age 44.8 ± 10.0 years) were recruited for the study through advertisements placed on university and hospital noticeboards. These participants had no history of chronic pain, headache or health conditions and had no contraindications of MRI.
Procedure
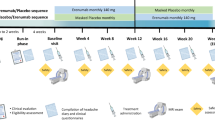
Potential participants were identified by the treating neurologist, who provided study information, and gained consent to be contacted by the research team. The research team screened potential participants for eligibility by telephone, further explained the study and gained written informed consent. Participants immediately started an online pain diary, completed initial questionnaires of headache severity (Headache Impact Test- HIT-6), disability (World Health Organization Disability Assessment Schedule-WHODAS 2.0–12), pain sensitivity (Central Sensitisation Inventory-CSI) and psychological wellbeing (Depression Anxiety and Stress Scale- DASS-21). Questionnaires were completed using the online platform, REsearch Data Capture® (REDcap) [28]. Participants were scanned in their interictal phase and asked to refrain from taking pain medication, caffeine, nicotine or alcohol on the day of the MRI/MRS scan. Following the initial scan participants started their new treatment regimen. At 3-month follow-up participants repeated headache pain and disability questionnaires and attended for a follow-up MRI/MRS scan under the same conditions as their first scan.
Clinical outcome measures
Validated patient reported outcome measures were chosen to evaluate change in headache severity and disability over time. The HIT-6 was chosen due to being specifically designed and validated as a measure of adverse headache impact in both clinical practice and research [27, 29]. Scores range from 36 to 78 with higher scores corresponding to higher levels of disability. The WHODAS 2.0–12 was chosen as a global measure of disability due to its reliability and sensitivity to detecting change in disability over time [30]. Scores range from 12 to 60, with 60 indicating the highest level of disability.
Headache frequency was measured through an online weekly pain diary. Participants recorded the number of days they experienced migraine each week and rated the migraine severity using the Numerical Rating Scale (NRS) where 0 was no pain, and 100 the worst imaginable pain.
Neurometabolites of interest
The primary aim of the study was to understand the role of GABA. We therefore focused on GABA+ levels, as this currently reflects the most reliable method to report GABA when using a repeat measure design. The Glx composite signal was a secondary target, representing glutamate with additional contributions from glutamine (Gln) and glutathione (GSH). The composite signal is reported since Glu, Gln and GSH are heavily overlapped at 3 T field strength and therefore difficult to resolve from each other reliably [31].
MRI/MRS data acquisition
All participants were scanned on a Siemens 3 T Magnetom Prisma (Erlangen, Germany) with 64-channel head coil. High resolution 3D T1-weighted structural images (repetition time (TR) = 2400 ms; echo time (TE) = 2.21 ms; inversion time (TI) = 1150 ms; voxel size = 1.0 × 1.0 × 1.0 mm3; FOV = 256 mm; matrix = 256 × 256; acquisition time = 4 min 35 s) were acquired to inform voxel placement (previously described [24]) and for use in tissue segmentation. A 2D T2-weighted series (TR = 7490 ms; TE = 99 ms; voxel size = 0.6 × 0.3 mm3; FOV = 220 mm; matrix = 384 × 288; acquisition time = 2 min 24 s) was also acquired and sent to a consultant radiologist to review and report any incidental finding. MRS data were acquired using the MEGA-PRESS sequence from two regions shown in Fig. 1, the posterior cingulate gyrus (PCG, voxel size 25 (AP) × 40 (RL) × 25 (CC) mm 3) and the anterior cingulate cortex (ACC, 40 (AP) × 25 (RL) × 25 (CC) mm3). Common parameters for both voxels were: TR = 2000 ms; TE = 68 ms; 192 averages (96 ON, 96 OFF); 2048 data points; spectral width = 2000 Hz; editing pulse frequencies set to 1.9 ppm and 7.5 ppm for editing of GABA+; editing pulse bandwidth = 70 Hz. Water-unsuppressed MEGA-PRESS data (with water suppression RF pulses deactivated) were also acquired from each voxel to perform eddy-current correction and water-scaled quantification.

Exemplary voxel placement and an overlay of all spectra from A) PCG and B) ACC at baseline and 3-month follow-up
MRS data processing
MRS data were processed using the open-source MATLAB-based analysis toolbox Gannet 3.1 [32], including data loading, coil combination, frequency-and-phase-correction of individual transients using the Spectral Registration algorithm [33], and averaging. The 3-ppm GABA+ and 3.75-ppm Glx signals in the difference spectrum were modelled with a single Gaussian and a dual-Lorentzian peak, respectively, including terms for the baseline slope between the two signals. The water signal in the water reference spectrum was modelled with a single Voigtian peak. The voxels were co-registered to the T1-weighted structural acquisition, which was segmented using built-in SPM12 functions. GABA+ and Glx levels were quantified relative to the internal tissue water signal, accounting for tissue composition of the voxel, as well as different water content and relaxation times for grey matter, white matter, and cerebrospinal fluid. Alpha-corrected GABA concentration estimates were reported, accounting for the fact that GABA+ and Glx concentrations differ between grey and white matter at a ratio of ~ 2:1 [34].
Spectroscopy quality
Spectra were visually examined for artefacts by two investigators with eight and ten years’ experience of spectral editing (GO, NP). Spectra were excluded if they demonstrated significant motion artefact or insufficient water suppression (n = 1, healthy participant, ACC voxel). All remaining spectra achieved a fit error below the recommended quality threshold of 10% [32]. The mean fit error was 4.61 ± 0.95% in the PCG and 4.57 ± 0.67% in the ACC.
MRS test-retest reliability
The test-retest reliability of the MEGA-PRESS acquisition over the same 3-month time period was determined in the 5 healthy control participants. One ACC acquisition was excluded from the analysis due to substantial motion artefact. Results demonstrated a test-retest coefficient of variance (CV) of 10% in PCG, and 12.6% in the ACC. This is in agreement with previous MEGA-PRESS studies of GABA+ [35,36,37] and provides evidence of the reliability of the MRS collection in this longitudinal investigation.
Statistical analysis
The power calculation was based on our previous work [14]. A sample size of n = 17 was required to detect a 0.2 IU change in GABA+ level with 80% power and therefore, 20 participants were recruited to allow for a 15% dropout rate.
Participants’ baseline characteristics were reported using descriptive statistics, mean and standard deviation for normally distributed data, and median interquartile range for non-normally distributed data.
The outcomes of GABA+ levels, Glx levels, migraine days per month, HIT-6 scores and WHODAS scores were included in the statistical analysis. Normality for each variable was assessed using Kolmogorov-Smirnov and Shapiro-Wilk tests. Paired sample t-tests were used to examine change in clinical characteristics (migraine days, HIT-6, WHODAS) and change in neurometabolite levels (GABA+, Glx) from baseline to 3-month follow-up.
In addressing our primary aim to determine the degree of correlation between change in characteristics of migraine and change in neurometabolite levels, and to determine the correlation between baseline and change in neurometabolite levels, Pearson’s (r) correlation was used- due to the normal distribution of data. Correlations r > 0.07 were considered strong, 0.4 to 0.69 moderate, 0.1–0.39 weak, < 0.1 negligible [38, 39].
Neurometabolite levels and clinical outcome measures were plotted as raincloud plots, which provide a transparent method of data visualisation [40]. Raincloud plots consist of a half-violin plot to visualize the distribution, a box plot to highlight the median and 95% confidence intervals, and scatter plots with lines connecting each individual participants score at baseline and 3-month follow-up.
Post-hoc testing was carried out to explore if change in GABA+ or Glx level was different in those who were escalated with CGRP-mAbs treatment compared to Onabotulinumtoxin A. Due to the normal distribution of data an independent sample t-test was used to determine any between-group differences. A point biserial correlation (Pearson’s (r) correlation using one dichotomous variable and one continuous variable) was then used to determine correlations between group (CGRP-mAbs Yes/No) with headache frequency, intensity and disability.
An alpha level of 0.05 was used for all statistical tests. Statistical testing was carried out using SPSS version 26 [41] and data visualisation was performed in R version 4.0.2 [42].
Results
Of the 20 participants recruited, 18 were included in the final analysis. One was excluded following MRS because they had taken diazepam prior to being scanned, thus not meeting the study’s inclusion criteria, and one did not complete their follow-up scan. Of the final 18 participants, 8 had been escalated to Onabotulinumtoxin A, and 10 with CGRP-mAbs. All participants had received two doses of medication between baseline and 3-month follow-up.
Participants
Baseline characteristics of study population
The mean ± SD duration of migraine was 21 ± 11.0 years in the participants included in the final analysis (n = 18). Participants experienced on average 16.7 ± 5.1 headache days in the month preceding the baseline scan, had an average pain intensity of 66.1% ± 22.9 in the week preceding the scan (Table 1). Participants were scanned in the interictal phase, however due to the chronic nature of the symptoms some still had residual head pain as reflected in the time since migraine (Table 1). Overall, the group’s baseline psychological status indicated that on average, participants were mildly depressed and had moderate anxiety and stress levels [43].
Clinical changes from baseline to 3-month follow-up
In order to address our primary aim, we first report observed changes in migraine characteristics and brain neurometabolite levels from baseline to 3-month follow-up.
Change in migraine characteristics from baseline to 3-month follow-up
Overall the group experienced an improvement in clinical characteristics of migraine from baseline to 3-month follow-up. The mean ± SD headache frequency was 16.7 ± 5.1 days per month at baseline and 12.4 ± 10.0 days at 3-month follow-up (mean difference − 4.22 days, 95% CI [− 8.78 to 0.33] days, t (17) = − 1.96, p = 0.07). Headache intensity (HIT-6) decreased significantly from 65.7 ± 6.6 at baseline to 59.0 ± 8.4 at 3-months (mean difference − 6.72, 95% CI[− 9.15 to − 4.29], t (17) = − 5.84, p = 0.01) and disability (WHODAS) was 24.8 ± 16.1 at baseline and 22.0 ± 23.1 at 3-months (mean difference − 2.78 95% CI[− 12.38 to 6.82], t (17) = − 0.61, p = 0.55) (Fig. 2).

Change in migraine characteristics from baseline to 3-month follow-up. Raincloud plots for change in A) migraine frequency (migraine days per month), B) migraine intensity (HIT-6 score) and C) disability (WHODAS score). Each individual plot represents change in clinical characteristics from baseline to 3-month follow-up in participants with migraine (n = 18). Green data points represent migraine characteristics at baseline and blue at 3-month follow-up. The grey lines represent change in individual participants scores over time
Change in neurometabolite levels from baseline to 3-month follow-up
Overall, mean GABA+ levels in the PCG significantly decreased between baseline and 3-month follow-up from 4.93 ± 0.62 IU to 4.48 ± 0.45 IU (mean difference − 0.45 IU, 95% CI [− 0.79 to − 0.10] IU, t (17) = − 2.72, p = 0.02). At an individual level, a decrease in PCG GABA level was observed in 12 participants, and 6 displayed an increase over the 3-month period. Prior to final analysis, the two outliers (baseline PCG GABA+ 6.5+ and baseline PCG Glx 18+) were reassessed for data quality and modelling and subsequently retained.
In contrast to the PCG, mean GABA+ levels in the ACC did not significantly change from baseline to 3-month follow-up. ACC GABA+ levels in participants with migraine at baseline were 4.51 ± 0.38 IU and 3-month follow up 4.40 ± 0.55 IU (mean difference − 0.12 IU, 95% CI [− 0.41 to 0.18] IU, t (17) = − 0.85, p = 0.41). At an individual level, a decrease in ACC GABA+ levels were observed in 11 participants and an increase in 7. Glx levels were not significantly different between baseline and 3-month follow-up in either the PCG or the ACC (Fig. 3).

Change in neurometabolite levels between timepoints for participants with migraine. GABA+ in A) PCG, B) ACC, and Glx in C) PCG and D) ACC. Each individual plot represents change in neurometabolite levels from baseline to 3-month follow-up in participants with migraine (n = 18). Green data points represent neurometabolite levels at baseline and blue at 3-month follow-up. The grey lines represent change in individual participants neurometabolite levels over time
Primary result
Correlation between change in brain neurometabolite levels and change in migraine characteristics
There were moderate inverse correlations between GABA+ levels in the ACC and all clinical outcomes. Specifically, we found a moderate inverse correlation between increase in GABA+ levels in the ACC and reduction in headache frequency at 3-month follow-up (r = − 0.51, p = 0.03 (Table 2, Fig. 4). Similarly, moderate inverse correlations were found between increase in ACC GABA+ levels and both reduction in headache intensity (r = − 0.51, p = 0.03) and reduction in disability (r = − 0.53, p = 0.03). In contrast to the findings in the ACC, correlations between change in PCG GABA+ levels and changes in migraine frequency, intensity or disability were negligible and not significant (Table 2). In the case of Glx, there were only negligible correlations between change in Glx and change in clinical characteristics of migraine in both the PCG and the ACC (Table 2, Supplementary materials I).

Correlation between change in ACC GABA+ and change in clinical characteristics. Dots represent participants with migraine, the grey ribbon represents the 95% confidence interval, and the blue regression line represents the Pearson’s correlation coefficient (r)
Secondary results
Correlation between baseline brain neurometabolite levels and change in migraine characteristics
The baseline levels of both GABA+ and Glx in the ACC and PCG demonstrated a negligible correlation with change in migraine frequency, intensity and disability (Supplementary materials I).
Correlation between baseline brain neurometabolite levels and change in brain neurometabolite levels
In determining whether baseline neurometabolite levels predict the extent of change in neurometabolite level we found a moderate inverse correlation between baseline levels of GABA+ and change in GABA+ in the ACC (r = − 0.54, p = 0.01) and strong inverse correlation in the PCG (r = − 0.72, p = 0.01) respectively. This reflects that those with higher levels of GABA+ at baseline experienced greater reductions in GABA+ over time.
The baseline level of Glx and change in Glx level demonstrated a strong inverse correlation in the PCG (r = − 0.92, p = 0.01), which was not present in the ACC (r = − 0.34, p = 0.16).
Post-hoc analysis
Change in GABA+ levels and clinical characteristics in those receiving CGRP-mAbs
Post-hoc analysis demonstrated that those who received CGRP-mAbs (n = 10/18) had a significantly greater increase in ACC GABA+ levels and significantly greater improvement in migraine symptoms than those who did not (Supplementary materials II). There was also a moderate positive correlation between receiving CGRP-mAbs (No/Yes) and an increase in ACC GABA+ levels [rpb (18) = 0.47, p = 0.05] which was not seen in the PCG. Furthermore, there was also a moderate inverse correlation between receiving CGRP-mAbs (No/Yes) and a reduction in migraine frequency [rpb (18) = − 0.58, p = 0.01] and migraine intensity [rpb (18) = − 0.49, p = 0.04].
Discussion
This study sought to measure any changes in GABA+ levels in a group of participants with chronic migraine as their care was escalated. We found that as GABA+ levels increase in the ACC, there was a corresponding moderate correlation with a decrease in migraine frequency, intensity and disability. A chance finding illustrated a greater increase in ACC GABA+ level in those taking CGRP-mAbs. These same correlations were not found in the PCG, despite group mean PCG GABA+ levels changing from baseline to 3-month follow-up. Results from this study suggest that GABA is a key neurometabolite of migraine. Proposed reasons for the differences observed between brain regions are discussed.
A major finding of this study was that an increase in ACC GABA+ levels were associated with an improvement in all three migraine outcomes; namely migraine frequency, intensity, and disability. Furthermore, the associations between change in neurometabolite levels and migraine characteristics were only seen for inhibitory GABA+ but not for excitatory Glx. Together this supports the hypothesis that the balance in cortical excitability in migraine is primarily mediated through inhibitory GABA, rather than excitatory Glx.
To date, correlations between GABA levels and clinical characteristics of migraine have only been measured in cross-sectional studies. Results from these studies have been mixed, with some showing an association with higher GABA/GABA+ levels and higher pain levels [15, 20] and others showing either the opposite [44] or negligible associations [45]. Whilst this discrepancy may be related to methodological differences, the variance in these prior results questions the extent to which GABA+ is related to the clinical characteristics of migraine. A single longitudinal study reported a group mean reduction in PCG GABA+ level in 14 people with migraine following treatment with levetiracetam [46]. Although on average the group in that study improved in terms of both migraine frequency and intensity, the relationship between GABA and clinical characteristics was not explored. Our study examined these associations longitudinally and demonstrated that change in clinical characteristics were associated with change in ACC GABA+ levels. This consequently provides plausible evidence that ACC GABA+ levels are related to pain-related measures of migraine.
An observed correlation between the change in GABA+ levels and change in clinical characteristics of migraine in the ACC but not the PCG is consistent with our understanding of how different brain regions process pain. The role of the ACC in pain processing has been well documented in both pre-clinical and human studies. These studies have demonstrated decreased affective pain behaviour, such as reduced escape behaviour following ACC damage [47], and analgesic responses to direct ACC stimulation [48]. Furthermore, human studies have demonstrated ACC activity during both observing and receiving a painful stimulus [49]. These findings combined with altered ACC GABA+ levels in other pain conditions [22, 23], mean the observed correlation between change in ACC GABA+ and change in clinical characteristics of pain are consistent with the role of the ACC in pain processing.
In contrast, the role of the PCG in pain is less clear. As part of the default mode network, deactivation of the PCG has been associated with higher levels of catastrophising in people with migraine [50] and attention to pain in people without a pain condition [51, 52]. Several cross-sectional studies have also demonstrated higher levels of GABA+ in the PCG/visual cortex of people with migraine compared to controls [13,14,15,16]. Taken together with the findings of this study, we can posit that GABA+ levels in the PCG might not directly reflect a measure of pain, rather they reflect another aspect of the migraine experience not captured within this study. Consequently, it could be proposed that the ACC provides a more relevant region to explore when investigating the association between GABA+ levels and pain in people with chronic migraine.
Our findings raise the possibility that GABA+ has a pain suppressing role in migraine. Whilst previous cross-sectional reports have identified elevated baseline GABA+ levels in people with migraine compared to pain-free controls, it was not clear if this difference reflected the underlying cause of migraine or an adaptive response to having migraine. Our data support the latter hypothesis suggesting the role of GABA+ is suppressive given that ACC GABA+ further increased as all three clinical measures of migraine reduced. i.e. where ACC GABA+ increased over time, migraine symptoms improved. Further, the reduction in migraine frequency may suggest that GABA+ has a role in suppressing cortical sensitivity in migraine, thus increasing the threshold required to trigger a migraine, rather than just modulating the migraine’s severity. This hypothesis suggesting a suppressive role of GABA does not support the proposal that future treatments are required to reduce the elevated GABA+ levels to that observed in healthy participants to better treat migraine [14, 17].
The hypothesised suppressive mechanism of GABA+ in the ACC is further supported by our post-hoc analysis. Although this study is not a drug trial and was not designed to evaluate drug interventions, the use of CGRP-mAbs in 10/18 participants provides a subgroup of people with migraine who experienced greater recovery, e.g. decreased migraine frequency (CGRP-mAbs mean ± SD − 8.8 ± 7.4 days versus Onabotulinumtoxin A 1.5 ± 8.2 days, mean difference 10.3 days, 95% CI [2.52 to 18.07], p = 0.01). Accompanying the greater improvement in the CGRP-mAbs group there was also a greater mean increase in ACC GABA+ levels (Supplementary materials II, III). Further, an increase in ACC GABA+ level was observed in 60% (n = 6/10) of the CGRP-mAbs group compared to just 12.5% (n = 1/8) of the Onabotulinumtoxin A group. This supports the hypothesis that those who improve are more likely to experience an increase in ACC GABA+ levels, providing further evidence that ACC GABA+ levels have a pertinent role in the recovery of people with chronic migraine.
Since both CGRP-mAbs and Onabotulinumtoxin A medications are thought to have a peripheral mode of action and do not cross the blood-brain barrier [53, 54], it is likely that they do not directly influence brain GABA levels. We might speculate that CGRP-mAbs or Onabotulinumtoxin A block the activation of trigeminal afferents by blocking peripheral receptors or inhibiting neuropeptide release [54, 55]. Consequently, tonic or phasic trigeminal afferent drive is inhibited, reducing the activity of neurons in the spinal trigeminal nucleus, thalamus and cingulate cortex pathway [56]. This reduction in afferent drive may ultimately underpin the alteration in excitatory and inhibitory balance observed here in the ACC. In addition, altered descending drive from the cingulate cortex to brainstem pain modulatory circuits, [57, 58] may suppress the ability of trigeminal inputs to evoke a migraine attack. Therefore, it is likely that the correlation between change in ACC GABA+ levels and change in pain levels, reflects the central effects of altered trigeminal afferent drive rather than a direct effect of the medication itself.
Future directions
This longitudinal study provides the next stage of exploratory research aimed at understanding the role of the neurometabolites GABA and glutamate in migraine. This study reported the composite measures, GABA+ (GABA + macromolecules) and Glx (glutamate-glutamine-glutathione) as they currently represent the most reliable method when using a repeated-measures design [11, 34, 59]. Therefore, some attention should be paid to the macromolecule content of the signal. As technology advances and the specificity and reliability of GABA and glutamate acquisition improve, future studies may wish to use methods that attempt to separate GABA from macromolecules and report glutamate specifically rather than the composite Glx. Further Glx was obtained from the difference spectra. The reliability of this method has been discussed in several studies which suggest although Glx and glutamate can be measured using MEGA-PRESS the measurement of Glx and glutamate may be more reliable if measured using a PRESS sequence [31, 60, 61]. Therefore, our results for Glx would benefit from further investigation using an experiment specifically optimised for Glx.
Further investigation of the temporal nature of GABA+ levels in chronic migraine would aid our understanding. It is hypothesised that the change in GABA+ levels reported in this study might reflect a chronic shift in GABA levels. However, fluctuation of GABA levels in a person with migraine in the short term or throughout the migraine cycle remains unknown. A study of time-resolved measurements, yet to be conducted in a migraine population, may further elucidate the nature of GABA+ changes reported in this study.
The exploratory nature of the study inevitably meant that we were not adequately powered to fully investigate (beyond exploratory testing) subgroups of participants in terms of treatments received or responsiveness. Future research aimed at investigating neurometabolite profiles of people who respond to particular treatments would significantly benefit the migraine community, providing the next step in delivering targeted treatment for migraine. Treatment strategies based on those most likely to respond would not only reduce the unnecessary prescription of medication, but improve patient outcomes, reduce the risk of side-effects, and reduce unnecessary health care costs.
Conclusion
In conclusion, we found that an increase in ACC GABA+ levels over time was associated with a decrease in migraine frequency, intensity and disability. Suggesting previously reported elevated GABA+ levels may not be a cause of migraine, but a protective mechanism attempting to suppress further migraine attacks. The findings of this study support that ACC GABA may have a pertinent role in the recovery of people with chronic migraine.
Availability of data and materials
The open-source software code of Gannet 3.1.3 that was used to process and analyze the MRS data is available from https://github.com/richardedden/Gannet3.1/releases/tag/v3.1.3. The scripts for the batch analysis and the R code for the visualization is available through the OSF repository https://osf.io/y8gps/?view_only=0a35454b80dc456f93e84a99b86fbfb4. Datasets generated during the current study are available from the corresponding authors upon reasonable request.
Abbreviations
- GABA:
-
Gamma-aminobutyric acid
- GABA+:
-
GABA + macromolecules
- MRS:
-
Magnetic resonance spectroscopy
- ICHD:
-
International classification of headache disorders
- PBS:
-
Pharmaceutical benefits scheme
- HIT-6:
-
Headache intensity scale
- WHODAS:
-
World health organization disability assessment schedule
- ACC:
-
Anterior cingulate cortex
- PCG:
-
Posterior cingulate gyrus
- MRI:
-
Magnetic resonance imaging
- Glx:
-
Glutamate-gluatmaine-glutathione
- CGRP-mAbs:
-
Calcitonin gene-related peptide monoclonal antibodies
References
Kassebaum NJ, Arora M, Barber RM, Bhutta ZA, Brown J, Carter A, Casey DC, Charlson FJ, Coates MM, Coggeshall M, Cornaby L, Dandona L, Dicker DJ, Erskine HE, Ferrari AJ, Fitzmaurice C, Foreman K, Forouzanfar MH, Fullman N, Gething PW, Goldberg EM, Graetz N, Haagsma JA, Hay SI, Johnson CO, Kemmer L, Khalil IA, Kinfu Y, Kutz MJ, Kyu HH, Leung J, Liang X, Lim SS, Lozano R, Mensah GA, Mikesell J, Mokdad AH, Mooney MD, Naghavi M, Nguyen G, Nsoesie E, Pigott DM, Pinho C, Rankin Z, Reinig N, Salomon JA, Sandar L, Smith A, Sorensen RJD, Stanaway J, Steiner C, Teeple S, Troeger C, Truelsen T, VanderZanden A, Wagner JA, Wanga V, Whiteford HA, Zhou M, Zoeckler L, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, Abraham B, Abubakar I, Abu-Raddad LJ, Abu-Rmeileh NME, Achoki T, Ackerman IN, Adebiyi AO, Adedeji IA, Adsuar JC, Afanvi KA, Afshin A, Agardh EE, Agarwal A, Agarwal SK, Ahmed MB, Kiadaliri AA, Ahmadieh H, Akseer N, al-Aly Z, Alam K, Alam NKM, Aldhahri SF, Alegretti MA, Aleman AV, Alemu ZA, Alexander LT, Ali R, Alkerwi A', Alla F, Allebeck P, Allen C, Alsharif U, Altirkawi KA, Martin EA, Alvis-Guzman N, Amare AT, Amberbir A, Amegah AK, Amini H, Ammar W, Amrock SM, Anderson GM, Anderson BO, Antonio CAT, Anwari P, Ärnlöv J, Arsenijevic VSA, Artaman A, Asayesh H, Asghar RJ, Avokpaho EFGA, Awasthi A, Quintanilla BPA, Azzopardi P, Bacha U, Badawi A, Balakrishnan K, Banerjee A, Barac A, Barker-Collo SL, Bärnighausen T, Barregard L, Barrero LH, Basu S, Bayou TA, Beardsley J, Bedi N, Beghi E, Bell B, Bell ML, Benjet C, Bennett DA, Bensenor IM, Berhane A, Bernabé E, Betsu BD, Beyene AS, Bhala N, Bhansali A, Bhatt S, Biadgilign S, Bienhoff K, Bikbov B, Abdulhak AAB, Biryukov S, Bisanzio D, Bjertness E, Blore JD, Borschmann R, Boufous S, Bourne RRA, Brainin M, Brazinova A, Breitborde NJK, Brugha TS, Buchbinder R, Buckle GC, Butt ZA, Calabria B, Campos-Nonato IR, Campuzano JC, Carabin H, Carapetis JR, Cárdenas R, Carrero JJ, Castañeda-Orjuela CA, Rivas JC, Catalá-López F, Cavalleri F, Chang JC, Chiang PPC, Chibalabala M, Chibueze CE, Chisumpa VH, Choi JYJ, Choudhury L, Christensen H, Ciobanu LG, Colistro V, Colomar M, Colquhoun SM, Cortinovis M, Crump JA, Damasceno A, Dandona R, Dargan PI, das Neves J, Davey G, Davis AC, Leo DD, Degenhardt L, Gobbo LCD, Derrett S, Jarlais DCD, deVeber GA, Dharmaratne SD, Dhillon PK, Ding EL, Doyle KE, Driscoll TR, Duan L, Dubey M, Duncan BB, Ebrahimi H, Ellenbogen RG, Elyazar I, Endries AY, Ermakov SP, Eshrati B, Esteghamati A, Estep K, Fahimi S, Farid TA, Farinha CSS, Faro A, Farvid MS, Farzadfar F, Feigin VL, Fereshtehnejad SM, Fernandes JG, Fernandes JC, Fischer F, Fitchett JRA, Foigt N, Fowkes FGR, Franklin RC, Friedman J, Frostad J, Fürst T, Futran ND, Gabbe B, Gankpé FG, Garcia-Basteiro AL, Gebrehiwot TT, Gebremedhin AT, Geleijnse JM, Gibney KB, Gillum RF, Ginawi IAM, Giref AZ, Giroud M, Gishu MD, Giussani G, Godwin WW, Gomez-Dantes H, Gona P, Goodridge A, Gopalani SV, Gotay CC, Goto A, Gouda HN, Gugnani H, Guo Y, Gupta R, Gupta R, Gupta V, Gutiérrez RA, Hafezi-Nejad N, Haile D, Hailu AD, Hailu GB, Halasa YA, Hamadeh RR, Hamidi S, Hammami M, Handal AJ, Hankey GJ, Harb HL, Harikrishnan S, Haro JM, Hassanvand MS, Hassen TA, Havmoeller R, Hay RJ, Hedayati MT, Heredia-Pi IB, Heydarpour P, Hoek HW, Hoffman DJ, Horino M, Horita N, Hosgood HD, Hoy DG, Hsairi M, Huang H, Huang JJ, Iburg KM, Idrisov BT, Innos K, Inoue M, Jacobsen KH, Jauregui A, Jayatilleke AU, Jeemon P, Jha V, Jiang G, Jiang Y, Jibat T, Jimenez-Corona A, Jin Y, Jonas JB, Kabir Z, Kajungu DK, Kalkonde Y, Kamal R, Kan H, Kandel A, Karch A, Karema CK, Karimkhani C, Kasaeian A, Katibeh M, Kaul A, Kawakami N, Kazi DS, Keiyoro PN, Kemp AH, Kengne AP, Keren A, Kesavachandran CN, Khader YS, Khan AR, Khan EA, Khang YH, Khoja TAM, Khubchandani J, Kieling C, Kim CI, Kim D, Kim YJ, Kissoon N, Kivipelto M, Knibbs LD, Knudsen AK, Kokubo Y, Kolte D, Kopec JA, Koul PA, Koyanagi A, Defo BK, Kuchenbecker RS, Bicer BK, Kuipers EJ, Kumar GA, Kwan GF, Lalloo R, Lallukka T, Larsson A, Latif AA, Lavados PM, Lawrynowicz AEB, Leasher JL, Leigh J, Leung R, Li Y, Li Y, Lipshultz SE, Liu PY, Liu Y, Lloyd BK, Logroscino G, Looker KJ, Lotufo PA, Lucas RM, Lunevicius R, Lyons RA, Razek HMAE, Mahdavi M, Majdan M, Majeed A, Malekzadeh R, Malta DC, Marcenes W, Martinez-Raga J, Masiye F, Mason-Jones AJ, Matzopoulos R, Mayosi BM, McGrath JJ, McKee M, Meaney PA, Mehari A, Melaku YA, Memiah P, Memish ZA, Mendoza W, Meretoja A, Meretoja TJ, Mesfin YM, Mhimbira FA, Millear A, Miller TR, Mills EJ, Mirarefin M, Mirrakhimov EM, Mitchell PB, Mock CN, Mohammad KA, Mohammadi A, Mohammed S, Monasta L, Hernandez JCM, Montico M, Moradi-Lakeh M, Mori R, Mueller UO, Mumford JE, Murdoch ME, Murthy GVS, Nachega JB, Naheed A, Naldi L, Nangia V, Newton JN, Ng M, Ngalesoni FN, Nguyen QL, Nisar MI, Pete PMN, Nolla JM, Norheim OF, Norman RE, Norrving B, Obermeyer CM, Ogbo FA, Oh IH, Oladimeji O, Olivares PR, Olusanya BO, Olusanya JO, Oren E, Ortiz A, Ota E, Oyekale AS, PA M, Park EK, Parsaeian M, Patten SB, Patton GC, Pedro JM, Pereira DM, Perico N, Pesudovs K, Petzold M, Phillips MR, Piel FB, Pillay JD, Pishgar F, Plass D, Polinder S, Popova S, Poulton RG, Pourmalek F, Prasad NM, Qorbani M, Rabiee RHS, Radfar A, Rafay A, Rahimi K, Rahimi-Movaghar V, Rahman M, Rahman MHU, Rahman SU, Rai D, Rai RK, Rajsic S, Raju M, Ram U, Ranganathan K, Refaat AH, Reitsma MB, Remuzzi G, Resnikoff S, Reynolds A, Ribeiro AL, Ricci S, Roba HS, Rojas-Rueda D, Ronfani L, Roshandel G, Roth GA, Roy A, Sackey BB, Sagar R, Sanabria JR, Sanchez-Niño MD, Santos IS, Santos JV, Sarmiento-Suarez R, Sartorius B, Satpathy M, Savic M, Sawhney M, Schmidt MI, Schneider IJC, Schutte AE, Schwebel DC, Seedat S, Sepanlou SG, Servan-Mori EE, Shahraz S, Shaikh MA, Sharma R, She J, Sheikhbahaei S, Shen J, Sheth KN, Shibuya K, Shigematsu M, Shin MJ, Shiri R, Sigfusdottir ID, Silva DAS, Silverberg JI, Simard EP, Singh A, Singh JA, Singh PK, Skirbekk V, Skogen JC, Soljak M, Søreide K, Sorensen RJD, Sreeramareddy CT, Stathopoulou V, Steel N, Stein DJ, Stein MB, Steiner TJ, Stovner LJ, Stranges S, Stroumpoulis K, Sunguya BF, Sur PJ, Swaminathan S, Sykes BL, Szoeke CEI, Tabarés-Seisdedos R, Tandon N, Tanne D, Tavakkoli M, Taye B, Taylor HR, Ao BJT, Tegegne TK, Tekle DY, Terkawi AS, Tessema GA, Thakur JS, Thomson AJ, Thorne-Lyman AL, Thrift AG, Thurston GD, Tobe-Gai R, Tonelli M, Topor-Madry R, Topouzis F, Tran BX, Truelsen T, Dimbuene ZT, Tsilimbaris M, Tura AK, Tuzcu EM, Tyrovolas S, Ukwaja KN, Undurraga EA, Uneke CJ, Uthman OA, van Gool CH, van Os J, Vasankari T, Vasconcelos AMN, Venketasubramanian N, Violante FS, Vlassov VV, Vollset SE, Wagner GR, Wallin MT, Wang L, Weichenthal S, Weiderpass E, Weintraub RG, Werdecker A, Westerman R, Wijeratne T, Wilkinson JD, Williams HC, Wiysonge CS, Woldeyohannes SM, Wolfe CDA, Won S, Xu G, Yadav AK, Yakob B, Yan LL, Yano Y, Yaseri M, Ye P, Yip P, Yonemoto N, Yoon SJ, Younis MZ, Yu C, Zaidi Z, Zaki MES, Zeeb H, Zodpey S, Zonies D, Zuhlke LJ, Vos T, Lopez AD, Murray CJL (2016) Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet 388(10053):1603–1658. https://doi.org/10.1016/S0140-6736(16)31460-X
Steiner TJ, Stovner LJ, Birbeck GL (2013) Migraine: the seventh disabler. Headache 53(2):227–229. https://doi.org/10.1111/head.12034
International Headache Society (2018) Headache classification Committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 38(1):1–211
Moriarty M, Mallick-Searle T (2016) Diagnosis and treatment for chronic migraine. Nurs Pract 41(6):18–32. https://doi.org/10.1097/01.NPR.0000483078.55590.b3
Buse DC, Manack A, Serrano D, Turkel C, Lipton RB (2010) Sociodemographic and comorbidity profiles of chronic migraine and episodic migraine sufferers. J Neurol Neurosurg Psychiatry 81(4):428–432. https://doi.org/10.1136/jnnp.2009.192492
Meletiche DM, Lofland JH, Young WB (2001) Quality-of-life differences between patients with episodic and transformed migraine. Headache. 41(6):573–578. https://doi.org/10.1046/j.1526-4610.2001.041006573.x
Stewart WF, Wood GC, Manack A, Varon SF, Buse DC, Lipton RB (2010) Employment and work impact of chronic migraine and episodic migraine. J Occup Environ Med 52(1):8–14. https://doi.org/10.1097/JOM.0b013e3181c1dc56
Dodick DW, Turkel CC, Degryse RE, Aurora SK, Silberstein SD, Lipton RB et al (2010) Onabotulinumtoxin A for treatment of chronic migraine: pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 50(6):921–936. https://doi.org/10.1111/j.1526-4610.2010.01678.x
Silberstein SD, Dodick DW, Bigal ME, Yeung PP, Goadsby PJ, Blankenbiller T, Grozinski-Wolff M, Yang R, Ma Y, Aycardi E (2017) Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med 377(22):2113–2122. https://doi.org/10.1056/NEJMoa1709038
Stovner L, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher A, Steiner TJ, Zwart JA (2007) The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 27(3):193–210. https://doi.org/10.1111/j.1468-2982.2007.01288.x
Mullins PG, McGonigle DJ, O'Gorman RL, Puts NA, Vidyasagar R, Evans CJ, Cardiff Symposium on MRS of GABA, Edden RA (2014) Current practice in the use of MEGA-PRESS spectroscopy for the detection of GABA. Neuroimage. 86:43–52. https://doi.org/10.1016/j.neuroimage.2012.12.004
Mescher M, Merkle H, Kirsch J, Garwood M, Gruetter R (1998) Simultaneous in vivo spectral editing and water suppression. NMR Biomed 11(6):266–272. https://doi.org/10.1002/(SICI)1099-1492(199810)11:6<266::AID-NBM530>3.0.CO;2-J
Chan YM, Pitchaimuthu K, Wu Q-Z, Carter OL, Egan GF, Badcock DR, McKendrick AM (2019) Relating excitatory and inhibitory neurochemicals to visual perception: a magnetic resonance study of occipital cortex between migraine events. PLoS One 14(7):e0208666. https://doi.org/10.1371/journal.pone.0208666
Aguila ME, Lagopoulos J, Leaver AM, Rebbeck T, Hubscher M, Brennan PC et al (2015) Elevated levels of GABA+ in migraine detected using (1) H-MRS. NMR Biomed 28(7):890–897. https://doi.org/10.1002/nbm.3321
Bell T, Stokoe M, Khaira A, Webb M, Noel M, Amoozegar F et al (2020) Gaba and glutamate changes in pediatric migraine. bioRxiv. https://doi.org/10.1101/2020.04.14.041616:2020.04.14.041616
Peek AL, Leaver AM, Foster S, Oeltzschner G, Puts NA, Galloway G et al (2021) Increased GABA+ in people with migraine, headache and pain conditions- a potential marker of pain. J Pain. https://doi.org/10.1016/j.jpain.2021.06.005
Peek AL, Rebbeck T, Puts NA, Watson J, Aguila ME, Leaver AM (2020) Brain GABA and glutamate levels across pain conditions: a systematic literature review and meta-analysis of 1H-MRS studies using the MRS-Q quality assessment tool. Neuroimage:116532
Henderson LA, Peck CC, Petersen ET, Rae CD, Youssef AM, Reeves JM, Wilcox SL, Akhter R, Murray GM, Gustin SM (2013) Chronic pain: lost inhibition? J Neurosci 33(17):1754–1782. https://doi.org/10.1523/JNEUROSCI.0174-13.2013
Ye H, Kaszuba S (2017) Inhibitory or excitatory? Optogenetic interrogation of the functional roles of GABAergic interneurons in epileptogenesis. J Biomed Sci 24(1):93. https://doi.org/10.1186/s12929-017-0399-8
Aguila M-ER, Rebbeck T, Leaver AM, Lagopoulos J, Brennan PC, Hübscher M, Refshauge KM (2016) The association between clinical characteristics of migraine and brain GABA levels: an exploratory study. J Pain 17(10):1058–1067. https://doi.org/10.1016/j.jpain.2016.06.008
Fuchs PN, Peng YB, Boyette-Davis JA, Uhelski ML (2014) The anterior cingulate cortex and pain processing. Front Integr Neurosci 8:35
Foerster BR, Petrou M, Edden RA, Sundgren PC, Schmidt-Wilcke T, Lowe SE et al (2012) Reduced insular gamma-aminobutyric acid in fibromyalgia. Arthritis Rheum 64(2):579–583. https://doi.org/10.1002/art.33339
Harper DE, Ichesco E, Schrepf A, Halvorson M, Puiu T, Clauw DJ, Harris RE, Harte SE, MAPP Research Network (2018) Relationships between brain metabolite levels, functional connectivity, and negative mood in urologic chronic pelvic pain syndrome patients compared to controls: a MAPP research network study. NeuroImage Clin 17:570–578. https://doi.org/10.1016/j.nicl.2017.11.014
Peek AL, Leaver AM, Foster S, Oeltzschner G, Puts NA, Galloway G, Sterling M, Ng K, Refshauge K, Aguila MER, Rebbeck T (2021) Increased GABA+ in people with migraine, headache, and pain conditions- a potential marker of pain. J Pain. https://doi.org/10.1016/j.jpain.2021.06.005
Bell T, Stokoe M, Khaira A, Webb M, Noel M, Amoozegar F, Harris AD (2021) GABA and glutamate in pediatric migraine. PAIN. 162(1):300–308. https://doi.org/10.1097/j.pain.0000000000002022
Committee PBA (2018) PBAC public summary document: Erenumab Canberra: Australian Government Department of Health
Kosinski M, Bayliss MS, Bjorner JB, Ware JE Jr, Garber WH, Batenhorst A et al (2003) A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res 12(8):963–974. https://doi.org/10.1023/A:1026119331193
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42(2):377–381. https://doi.org/10.1016/j.jbi.2008.08.010
Yang M, Rendas-Baum R, Varon SF, Kosinski M (2011) Validation of the headache impact test (HIT-6™) across episodic and chronic migraine. Cephalalgia 31(3):357–367. https://doi.org/10.1177/0333102410379890
Chwastiak LA, Von Korff M (2003) Disability in depression and back pain: evaluation of the World Health Organization disability assessment schedule (WHO DAS II) in a primary care setting. J Clin Epidemiol 56(6):507–514. https://doi.org/10.1016/S0895-4356(03)00051-9
Bell T, Boudes ES, Loo RS, Barker GJ, Lythgoe DJ, Edden RAE et al (2020) In vivo Glx and Glu measurements from GABA-edited MRS at 3 T. NMR Biomed. https://doi.org/10.1002/nbm.4245
Edden RA, Puts NA, Harris AD, Barker PB, Evans CJ (2014) Gannet: a batch-processing tool for the quantitative analysis of gamma-aminobutyric acid-edited MR spectroscopy spectra. J Magn Reson Imaging 40(6):1445–1452. https://doi.org/10.1002/jmri.24478
Near J, Edden R, Evans CJ, Paquin R, Harris A, Jezzard P (2015) Frequency and phase drift correction of magnetic resonance spectroscopy data by spectral registration in the time domain. Magn Reson Med 73(1):44–50. https://doi.org/10.1002/mrm.25094
Harris AD, Puts NA, Barker PB, Edden RA (2015) Spectral-editing measurements of GABA in the human brain with and without macromolecule suppression. Magn Reson Med 74(6):1523–1529. https://doi.org/10.1002/mrm.25549
Mikkelsen M, Singh KD, Sumner P, Evans CJ (2016) Comparison of the repeatability of GABA-edited magnetic resonance spectroscopy with and without macromolecule suppression. Magn Reson Med 75(3):946–953. https://doi.org/10.1002/mrm.25699
Mikkelsen M, Rimbault DL, Barker PB, Bhattacharyya PK, Brix MK, Buur PF, Cecil KM, Chan KL, Chen DYT, Craven AR, Cuypers K, Dacko M, Duncan NW, Dydak U, Edmondson DA, Ende G, Ersland L, Forbes MA, Gao F, Greenhouse I, Harris AD, He N, Heba S, Hoggard N, Hsu TW, Jansen JFA, Kangarlu A, Lange T, Lebel RM, Li Y, Lin CYE, Liou JK, Lirng JF, Liu F, Long JR, Ma R, Maes C, Moreno-Ortega M, Murray SO, Noah S, Noeske R, Noseworthy MD, Oeltzschner G, Porges EC, Prisciandaro JJ, Puts NAJ, Roberts TPL, Sack M, Sailasuta N, Saleh MG, Schallmo MP, Simard N, Stoffers D, Swinnen SP, Tegenthoff M, Truong P, Wang G, Wilkinson ID, Wittsack HJ, Woods AJ, Xu H, Yan F, Zhang C, Zipunnikov V, Zöllner HJ, Edden RAE (2019) Big GABA II: water-referenced edited MR spectroscopy at 25 research sites. Neuroimage. 191:537–548. https://doi.org/10.1016/j.neuroimage.2019.02.059
Bogner W, Gruber S, Doelken M, Stadlbauer A, Ganslandt O, Boettcher U, Trattnig S, Doerfler A, Stefan H, Hammen T (2010) In vivo quantification of intracerebral GABA by single-voxel (1) H-MRS-how reproducible are the results? Eur J Radiol 73(3):526–531. https://doi.org/10.1016/j.ejrad.2009.01.014
Schober P, Boer C, Schwarte LA (2018) Correlation coefficients: appropriate use and interpretation. Anesth Analg 126(5):1763–1768. https://doi.org/10.1213/ANE.0000000000002864
Overholser BR, Sowinski KM (2008) Biostatistics primer: part 2. Nutr Clin Pract 23(1):76–84. https://doi.org/10.1177/011542650802300176
Allen M, Poggiali D, Whitaker K, Marshall TR, Kievit RA (2019) Raincloud plots: a multi-platform tool for robust data visualization. Wellcome Open Res 4:63. https://doi.org/10.12688/wellcomeopenres.15191.1
Corp IBM (2019) IBM SPSS statistics for windows. IBM Corp, Armonk
R Development Core Team (2010) R: a languauge and environment for statistical computing. 4.0.2 ed. Austria: R Foundation for statistical computing, Vienna
Lovibond PF, Lovibond SH (1995) The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav Res Ther 33(3):335–343. https://doi.org/10.1016/0005-7967(94)00075-U
Bigal M, Friedman B, Grosberg B, Hetherington H, Lipton R, Pan J (2007) Gaba and glutamate levels in migraine suffers and controls - a study using magnetic resonance imaging spectroscopy. Cephalalgia 27(6):599
Bathel A, Schweizer L, Stude P, Glaubitz B, Wulms N, Delice S, Schmidt-Wilcke T (2018) Increased thalamic glutamate/glutamine levels in migraineurs. J Headache Pain 19(1):55. https://doi.org/10.1186/s10194-018-0885-8
Li Q, Chen C, Gong T (2018) High-field MRS study of GABA+ in patients with migraine: response to levetiracetam treatment. Neuroreport. 29(12):1007–1010. https://doi.org/10.1097/WNR.0000000000001067
Johansen JP, Fields HL, Manning BH (2001) The affective component of pain in rodents: direct evidence for a contribution of the anterior cingulate cortex. Proc Natl Acad Sci U S A 98(14):8077–8082. https://doi.org/10.1073/pnas.141218998
Kang SJ, Kwak C, Lee J, Sim S-E, Shim J, Choi T, Collingridge GL, Zhuo M, Kaang BK (2015) Bidirectional modulation of hyperalgesia via the specific control of excitatory and inhibitory neuronal activity in the ACC. Mol Brain 8(1):81. https://doi.org/10.1186/s13041-015-0170-6
Peyron R, Laurent B, Garcia-Larrea L (2000) Functional imaging of brain responses to pain. A review and meta-analysis (2000). Neurophysiol Clin 30(5):263–288. https://doi.org/10.1016/S0987-7053(00)00227-6
Zhang Y, Chen H, Zeng M, He J, Qi G, Zhang S, Liu R (2020) Abnormal whole brain functional connectivity pattern homogeneity and couplings in migraine without Aura. Front Hum Neurosci 14. https://doi.org/10.3389/fnhum.2020.619839
Mathur VA, Moayedi M, Keaser ML, Khan SA, Hubbard CS, Goyal M et al (2016) High frequency migraine is associated with lower acute pain sensitivity and abnormal insula activity related to migraine pain intensity, attack frequency, and pain catastrophizing. Front Hum Neurosci:10
Kucyi A, Salomons TV, Davis KD (2013) Mind wandering away from pain dynamically engages antinociceptive and default mode brain networks. Proc Natl Acad Sci 110(46):18692–18697. https://doi.org/10.1073/pnas.1312902110
Burstein R, Blumenfeld AM, Silberstein SD, Manack Adams A, Brin MF (2020) Mechanism of action of Onabotulinumtoxin A in chronic migraine: a narrative review. Headache 60(7):1259–1272. https://doi.org/10.1111/head.13849
Tso AR, Goadsby PJ (2017) Anti-CGRP monoclonal antibodies: the next era of migraine prevention? Curr Treat Options Neurol 19(8):27. https://doi.org/10.1007/s11940-017-0463-4
Do TP, Hvedstrup J, Schytz HW (2018) Botulinum toxin: a review of the mode of action in migraine. Acta Neurol Scand 137(5):442–451. https://doi.org/10.1111/ane.12906
Yang J-W, Shih H-C, Shyu B-C (2006) Intracortical circuits in rat anterior cingulate cortex are activated by nociceptive inputs mediated by medial thalamus. J Neurophysiol 96(6):3409–3422. https://doi.org/10.1152/jn.00623.2006
Kong J, P-c T, Zyloney C, T-p S (2010) Intrinsic functional connectivity of the periaqueductal gray, a resting fMRI study. Behav Brain Res 211(2):215–219. https://doi.org/10.1016/j.bbr.2010.03.042
Bingel U, Lorenz J, Schoell E, Weiller C, Büchel C (2006) Mechanisms of placebo analgesia: rACC recruitment of a subcortical antinociceptive network. Pain. 120(1–2):8–15. https://doi.org/10.1016/j.pain.2005.08.027
Mikkelsen M, Barker PB, Bhattacharyya PK, Brix MK, Buur PF, Cecil KM, Chan KL, Chen DYT, Craven AR, Cuypers K, Dacko M, Duncan NW, Dydak U, Edmondson DA, Ende G, Ersland L, Gao F, Greenhouse I, Harris AD, He N, Heba S, Hoggard N, Hsu TW, Jansen JFA, Kangarlu A, Lange T, Lebel RM, Li Y, Lin CYE, Liou JK, Lirng JF, Liu F, Ma R, Maes C, Moreno-Ortega M, Murray SO, Noah S, Noeske R, Noseworthy MD, Oeltzschner G, Prisciandaro JJ, Puts NAJ, Roberts TPL, Sack M, Sailasuta N, Saleh MG, Schallmo MP, Simard N, Swinnen SP, Tegenthoff M, Truong P, Wang G, Wilkinson ID, Wittsack HJ, Xu H, Yan F, Zhang C, Zipunnikov V, Zöllner HJ, Edden RAE (2017) Big GABA: edited MR spectroscopy at 24 research sites. Neuroimage. 159:32–45. https://doi.org/10.1016/j.neuroimage.2017.07.021
van Veenendaal TM, Backes WH, van Bussel FCG, Edden RAE, Puts NAJ, Aldenkamp AP, Jansen JFA (2018) Glutamate quantification by PRESS or MEGA-PRESS: validation, repeatability, and concordance. Magn Reson Imaging 48:107–114. https://doi.org/10.1016/j.mri.2017.12.029
Maddock RJ, Caton MD, Ragland JD (2018) Estimating glutamate and Glx from GABA-optimized MEGA-PRESS: off-resonance but not difference spectra values correspond to PRESS values. Psychiatry Res Neuroimaging 279:22–30. https://doi.org/10.1016/j.pscychresns.2018.07.003
Acknowledgements
We would like to acknowledge the research assistants working on the project Mi Hoang Amanda Dinh and Alexis Curtis, and the team at Westmead Hospital Radiology department, Australia. In addition, Edward J. Auerbach, Ph.D. and Małgorzata Marjańska, Ph.D. (Center for Magnetic Resonance Research and Department of Radiology, University of Minnesota, USA) for the development of the pulse sequences for the Siemens platform which were provided by the University of Minnesota under a C2P agreement.
Funding
This research was funded by the National Health and Medical Research Council (NHMRC) Centre of Research Excellence in recovery following road Traffic Injuries (CRERTI) APP1079022, NHMRC (Career Development Fellowship) APP1161467 and the University of Sydney Research Accelerator (SOAR) Fellowship.
Author information
Authors and Affiliations
Contributions
TR, KR, AL, GG, AP and KN supported the conception and design of the project. SF and AP acquired the data. AP analysed the data, NP, GO, LH, TR contributed to the interpretation of the data. AP, AL, TR, KR produce the first draft. All authors contributed intellectual content to revised manuscripts and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted through Western Sydney Local Health District reference number HREC/17/WMEAD/429. Written informed consent was gained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peek, A.L., Leaver, A.M., Foster, S. et al. Increase in ACC GABA+ levels correlate with decrease in migraine frequency, intensity and disability over time. J Headache Pain 22, 150 (2021). https://doi.org/10.1186/s10194-021-01352-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-021-01352-1