
Abstract
Background
The primary aim of this cross-sectional population-based study was to evaluate the 1-year prevalence of common headache disorders by a face-to-face interview.
Methods
The fourth wave of Nord-Trøndelag Health Survey (HUNT4) started in September 2017. The study was undertaken as part of a project mainly focusing on sleep disorders, where a total of 232 (19.3%) out of 1200 invited HUNT4 participants underwent a face-to-face headache interview.
Results
The mean age of the 232 participants was 58.4 years (range 22–89). There were 71.6% (95% CI 65.7–77.4) who reported headache during the last year, and 18.5% (95% CI 13.5–23.6) had suffered from headache in the same period. The 1-year prevalence of tension-type headache (TTH) was 43.1% (95% CI 36.7–49.5), of idiopathic stabbing headache 34.1% (27.9–40.2), and of definite migraine 18.1% (95% CI 13.1–23.1). A total of 7.6% (95% CI 4.0–10.7%) had migraine with coexisting TTH. Lifetime prevalence of migraine was 32.8% (95% CI 26.7–38.8). Headache yesterday was reported by 12.1% (95% CI 7.9–16.3), and 5.6% (95% CI 2.6–8.6) had headache during the interview.
Conclusion
In this population-based cross-sectional headache study performed by a face-to-face interview, the 1-year prevalence of TTH was 43.1% and of idiopathic stabbing headache 34.1%. A total of 18.1% had active migraine (18.1%), whereas the lifetime prevalence of migraine was 32.8%.
Similar content being viewed by others

Background
A careful history taken by a headache specialist is the gold-standard for making a valid headache diagnosis. This is, however, time-consuming and costly, therefore relatively few large population-based studies have used a face-to-face interview approach [1,2,3,4,5,6,7,8,9]. Most large-scale population-based studies have used telephone interview by lay interviewers, a self-administrated questionnaire, or a combination of a screening questionnaire and an interview by a physician [10, 11].
A face-to-face headache interview performed by headache specialist allow distinction between probable and definite headache diagnoses according to the most recent criteria of the International Classification of Headache Disorders (ICHD). Most studies focus on presence of an active headache disorder to reduce the influence of recall bias, usually defined as occurrence of headache during the last year [11].
Previously, we have done two face-to-face headache interviews in the general population to validate questionnaire-based diagnosis with diagnosis made by a headache specialist [6, 12]. This is also the overall goal by performing face-to-face interviews, but access to questionnaire-data will first be available during 2019.
The aim of the present study was to estimate the 1-year prevalence of common headache types by using a face-to-face interview in a random sample of participants in a large-scale population-based study.
Methods
Study design
This study was undertaken as a part of a large cross-sectional population-based study evaluating the 1-year prevalence of headache disorders by a face-to-face interview.
The fourth Nord-Trøndelag health survey (HUNT4)
All inhabitants aged 20 years or more in Nord-Trøndelag county of Norway have been or will be invited to participate in the adult version of HUNT4 in the period between September 2017 and March 2019, whereas adolescents aged 13–19 will be invited to Young-HUNT4. Individuals living in the town Stjørdal were consecutively invited to participate in HUNT4 in the period between September 4th, 2017 and February 22th 2018. Individuals living in other study areas will be invited in other periods before March 2019.
HUNT4 sleep and pain study
The present study is a part of a subproject of HUNT4 mainly focusing on sleep disorders including an invitation to ambulatory polysomnography (PSG) and neurophysiological measurements. A random sample of adults living in Stjørdal who had participated in HUNT4 and answered both the first and the second questionnaire received a written invitation. The invitation letter informed about an initial interview focusing on sleep and pain and to have ambulatory PSG and measurements of pain thresholds performed later. Participants who confirmed to participate received a sleep diary to fill in at home 5–7 days before the interview. Headache was not mentioned in the invitation letter.
Sample size calculation
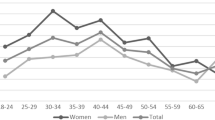
We have previously performed a similar still unpublished PSG study as a part of HUNT3. In this study, participants living in Stjørdal were invited to have a PSG in Trondheim. To perform at least 200 PSGs, it was necessary to invite 1200 persons. Thus, based on a participation rate of 17% in this HUNT3 sub-project, we decided to send 1200 postal written invitations randomly to HUNT4 participants. No stratification by sex or age was performed. However, based on previous experience with HUNT2 [12], we knew that the participation would be higher among women than men, highest in the age group 60–69, and lowest in the age group 20–29.
Headache interview
A semi-structured interview was performed by five medical doctors (three neurologist) with special interest and competence in headache. Initially, all subjects were asked the questions “Have you ever had migraine?”. Those who answered “yes” were asked for age of onset. Later in the interview, we repeated the question regarding age of onset for each type of headache. In the interview, we focused on those who answered “yes” to the question “Have you had a headache during the last 12 months?”.To clarify the burden, we also asked the question “Have you suffered from headache during the last 12 months?” Individuals who reported headache during the past year were asked about frequency (average number of days per month during the last year), time span since last headache, intensity, location, aura symptoms, other migraine and cluster headache features, and use of medication. All diagnoses were based on ICHD-3 version [13]. Up to three different headache types were diagnosed in those with active headache. Subjects with medication overuse headache (MOH) were also categorized according to their primary headache diagnosis.
The participants were also asked the question “Have you during the last year for at least 3 months had pain in muscles and joints?”. Individuals who answered “yes” were defined as having chronic musculoskeletal pain.
The participants also participated in a separate semi-structured interview about sleep disorders with focus on insomnia and restless legs. Individuals were evaluated for insomnia according to DSM-V (Diagnostic and Statistical Manual of Mental Disorders, 5th ed.).
Ethics
The study was included as a part of the HUNT4 project that was approved by the Regional Committee for Ethics in Medical Research and the Norwegian Data Inspectorate.
Statistics
1-year prevalence was estimated with 95% confidence interval (CI). The difference between proportions was analysed by chi-square tests, and p < 0.05 was considered statistically significant.
Results
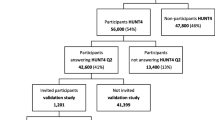
Among the 1200 invited participants, 239 (19.9%) agreed to participate. Among these, seven wanted to participate, but were unable to attend to the interview because they were out of town, had sick husband, were busy at work, or they had forgotten the invitation. Thus, among 1200 invited, 232 persons (19.3%) participated in the headache interview, more women (n = 152) than men (n = 80). The mean age was 58.4 years (range 22–89), and as demonstrated by Table 1, the majority (70%) of participants were in the age group 50–79 years. A total of 33.2% fulfilled the DSM-V diagnosis of insomnia, and 54.3% suffered from chronic musculoskeletal pain during the last year. The mean number of days between answering the two questionnaires in HUNT4 and the interview was 59 days (range 14–110 days).
Lifetime prevalence of migraine
Lifetime prevalence of migraine was 32.8% (26.7–38.8), 38.8% (95% CI 31.0–46.7) among women and 21.3% (95% CI 12.1–30.4) among men. Mean age of the first migraine attack was 24.3 years (95% CI 21.0–27.5), 24.7 years (95% CI 20.9–28.5) among women and 22.9 years (95% CI 15.8–30.0) among men.
1-year prevalence of headache
The 1-year prevalence of different headache disorders by gender among the 232 participants is shown in Table 2. As demonstrated, 71.6% (95% CI 65.7–77.4) reported that they had had headache during the past year, whereas 18.5% (13.5–23.6) stated that they had suffered from headache. The 1-year prevalence of tension-type headache was 43.1% (95% CI 36.7–49.5), 40.1% (336.7–49.5) had episodic TTH and 3.0% (05% CI 0.8–5.2) chronic TTH. The 1-year prevalence of idiopathic stabbing headache was 34.1% (27.9–40.2), whereof 4.7% (95% CI 2.0–7.5) reported attacks with idiopathic stabbing headache at least on a weekly basis. The prevalence of active migraine was 18.1% (95% CI 13.1–23.1), and 7.6% (95% CI 4.0–10.7%) had migraine with coexisting TTH (Table 2). Cervicogenic headache was the most common secondary headache (3.9%, 95% CI 1.4–6.4). Medication overuse headache was present in 0.9%.
A total of 120 participants were 60 years or older. Comparing to those below 60 years, the 1-year prevalence was lower for migraine (10.0% vs. 26.8%, p < 0.001) and TTH (35.8% vs. 50.9%, p = 0.024). For cervicogenic headache no significant difference was found (5.8% vs. 1.5%, p = 0.17).
Headache yesterday
Headache yesterday was reported by 12.1% (95% CI 7.9–16.3), 15.1% (95% CI 9.4–20.9) among women and 6.3% among men (95% CI 0.8–11.7), and 5.6% (95% CI 2.6–8.6) reported headache during the interview.
Impact of being a headache sufferer
Individuals who answered “yes” to the question “Have you suffered from headache during the last 12 months?” were significantly more likely to have active migraine than those who responded “no” (48.8% versus 11.1%, p < 0.001).
Discussion
In this population-based cross-sectional study evaluating 1-year prevalence of headache disorders by a face-to-face interview, TTH was most common (43.1%), followed by idiopathic stabbing headache (34.1%) and migraine (18.1%).
Comparisons with other studies
Relatively few population-based studies have estimated 1-year prevalence of headache using a face-to-face interview performed by medical doctors with special interest and competence in headache [1,2,3,4,5,6,7,8,9]. We have previously performed interviews of a random sample of 297 participants of HUNT3, reporting higher 1-year prevalence of TTH (51.9%), but almost similar prevalence of idiopathic stabbing headache (35.0%) and migraine (17.2%) [6]. The 1-year prevalence of migraine of 18.1% in the present study was higher than the 11% and 15.5% reported in the two studies from Copenhagen (1, 4), but lower than found in Italy [7] (Table 3). Furthermore, the 1-year prevalence of 43.1% in TTH was higher than reported in Italy [8], but much lower than reported in the two Copenhagen studies [1, 4]. Interestingly, our 1-year prevalence of idiopathic stabbing headache of 34.1% was identical to the prevalence in Vågå (35.2%) in Norway [3]. As demonstrated by Table 3, our 1-year prevalence of chronic TTH of 3.0% were nearly identical to the corresponding prevalence’s reported in Denmark [1] in Spain [2], and in Akershus in Norway [5]. In contrast, a much lower prevalence of chronic TTH was reported in Italy [8].
In the present study, with a high proportion of elderly participants, cervicogenic headache was common with a total 1-year prevalence of 3.9%. In accordance with this, the lifetime prevalence of cervicogenic headache was found to be 4.1% among 1838 inhabitants in Vågå in Norway [14]. Furthermore, in the present study the lifetime prevalence of migraine was 32.8%. An even higher lifetime prevalence of 40.3% was reported in Vågå [15, 16].
Recent population-based studies initiated by the Global Campaign against headache have focused on headache yesterday, to minimize the influence of recall bias [17]. In the present study, 12.1% reported headache yesterday. Almost similar prevalence was found in Lithuania and Italy [18]. According to summery data from nine European countries, 15–17% had headache yesterday lasting on average for 6 h [18].
The present study did not estimate the 1-year prevalence of very rare headache diagnoses very precisely. In the present study, none of the 232 participants had chronic migraine. In comparison, only two out of 904 participants (0,2%) in Italy fulfilled the criteria of chronic migraine [8]. Such low prevalence may explain why we did not identify participants with chronic migraine. To make relatively precise estimates of rare headaches with prevalence of 0.5% or less, you probably need at least 1500–2000 participants. Merging data from both HUNT3 (n = 297) [6] and HUNT4 (n = 232), the total sample size of 529 persons is even too small to give precise estimates of rare headaches. Having this in mind, we briefly should mention that we identified one participant with primary exercise headache, indicating a 1-year prevalence of approximately 0.2%. Furthermore, merged data indicated a 1-year prevalence of MOH 1.7%, and a lifetime prevalence of cluster headache of 0.4%. A similar lifetime prevalence of cluster headache was found in Vågå [19].
Strengths and limitations of the study
The major strength of this study was the population-based design using a face-to-face interview performed by headache experts. The invitation letter did not mention that a detailed headache interview would be performed, hence a selective participation of headache patients is less likely. Several study limitations should also be considered. Since our estimates were based on data from 19.1% of the invited population, one may question to what degree the results can be generalized. The present study mainly focused on sleep disorders, and the very low participation rate could possibly be explained by the supplementary invitation to an ambulatory PSG and neurophysiological measurements. This time-consuming study included traveling to Trondheim two consecutive days, which may not be possible for most full-time workers. Furthermore, most full-time workers could not attend interviews during daytime and we regrettably had no time for afternoon appointments. Thus, the present participants had a high proportion of elderly who could attend, had much more insomnia and slightly more chronic musculoskeletal pain than previously found in HUNT3. In the present study, 33.2% fulfilled the DSM-V diagnosis of insomnia, and 54.3% had chronic musculoskeletal pain. The corresponding figures in HUNT3 were respectively 7.9 and 50.4% [20, 21]. It should be highlighted that a bidirectional association between insomnia and headache has been found, in particular for headache ≥7 days/month [22,23,24]. Thus, we cannot rule out the possibility that the high prevalence of insomnia among participants may have influenced on the prevalence of migraine and other headaches. Because of a very low participation rate and the high prevalence of insomnia among participants, generalization of our results to the entire population must accordingly be done with great caution.
Conclusions
In this cross-sectional study evaluating 1-year prevalence of headache by a face-to-face interview, 43.1% had TTH, and 34.1% idiopathic stabbing headache. A total of 18.1% had active migraine (18.1%), whereas the lifetime prevalence of migraine was 32.8%.
References
Rasmussen BK, Jensen R, Schroll M, Olesen J (1991) Epidemiology of headache in a general population - a prevalence study. J Clin Epideiol 44:1147–1157
Castillo J, Muñoz P, Guitera V, Pascual J (1999) Epidemiology of chronic daily headache in the general population. Headache 39:190–196
Sjaastad O, Pettersen H, Bakketeig LS (2001) The Vågå study, epidemiology of headache. The prevalence of ultrashort paroxysms. Cephalalgia 21:207–215
Lyngberg AC, Rasmussen BK, Jorgensen T, Jensen R (2005) Has the prevalence of migraine and tension-type headache changed over a 12-year period? A Danish population survey. Eur J Epidemiol 20:243–249
Grande RB, Aaseth K, Gulbransen P, Lundquist C, Russell MB (2008) Prevalence of primary chronic headache in a population-based sample of 30- to 44-year-old persons. The Akershus study of chronic headache. Neuroepidemiology 30:76–83
Hagen K, Zwart JA, Aamodt AH, Nilsen KB, Bråthen G, Helde G, Stjern M, Tronvik EA, Stovner LJ (2008) A face-to-face interview of participants in HUNT 3: the impact of the screening question on headache prevalence. J Headache Pain 9:289–294
Ferrante T, Castellini P, Abrignani G, Latte L, Russo M, Camarda C, Veronesi L, Pasquarella C, Manzoni GC, Torelli P (2012) The PACE study: past-year prevalence of migraine in Parma’s adult general population. Cephalalgia 32:358–365
Ferrante T, Manzoni GC, Russo M, Taga A, Camarda C, Veronesi L, Pasquarella C, Sansebastiano G, Torelli P (2015) The PACE study: past-year prevalence of tension-type headache and its subtypes in Parma's adult general population. Neurol Sci 36:35–42
Kandil MR, Hamed SA, Fadel KA, Khalifa HE, Ghanem MK, Mohamed KO (2016) Migraine in Assiut governorate, Egypt: epidemiology, risk factors, comorbid conditions and predictors of change from episodic to chronic migraine. Neurol Res 38:232–241
Russell MB, Aaseth K, Grande RB, Gulbrandsen P, Lundqvist C (2007) Which strategy should be applied? Design of a Norwegian epidemiological survey on chronic headache. Acta Neurol Scand 115(suppl. 187):59–63
Stovner LJ, Al Jumah M, Birbeck GL, Gururaj G, Jensen R, Katsarava Z, Queiroz LP, Scher AI, Tekle-Haimanot R, Wang SJ, Steiner TJ (2014) The methodology of population surveys of headache prevalence, burden and cost: principles and recommendations from the global campaign against headache. J Headache Pain 15:5
Hagen K, Zwart JA, Vatten L, Stovner LJ, Bovim G (2000) Head-HUNT: validity and reliability of a headache questionnaire in a large population-based study in Norway. Cephalalgia 20:244–251
Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders (IHS), 3rd edition (2018). 38:1–211. Cephalalgia
Sjaastad O, Bakketeig LS (2008) Prevalence of cervicogenic headache: Vågå study of headache epidemiology. Acta Neurol Scand 117:173–180
Sjaastad O, Bakketeig LS (2008) Migraine without aura: comparison with cervicogenic headache. Vågå study of headache epidemiology. Acta Neurol Scand 117:377–383
Sjaastad O, Bakketeig LS, Petersen HC (2006) Migraine with aura: visual disturbances and interrelationship with the pain phase. Vågå study of headache epidemiology. J Headache Pain 7:127–135
Steiner TJ (2004) Lifting the burden: the global campaign against headache. Lancet Neurol 3:204–205
Andrée C, Steiner TJ, Barré J, Katsarava Z, Lainez JM, Lampl C, Lantéri-Minet M, Rastenyte D, Ruiz de la Torre E, Tassorelli C, Stovner LJ (2014) Headache yesterday in Europe. J Headache Pain 15:33
Sjaastad O, Bakketeig LS (2003) Cluster headache prevalence. Vågå study of headache epidemiology. Cephalalgia 23:528–533
Uhlig BL, Sand T, Odegård SS, Hagen K. Prevalence and associated factors of DSM-V Insomnia in Norway. The HUNT 3 study. Sleep Med 15:708–713
Hagen K, Linde M, Heuch I, Stovner LJ, Zwart JA (2011) Increasing prevalence of chronic musculoskeletal complaints. A large 11-year follow-up in the general population (HUNT 2 and 3). Pain Med 12:1657–1666
Ødegård SS, Sand T, Engstrøm M, Stovner LJ, Zwart JA, Hagen K (2011) The long-term effect of insomnia on primary headaches. A prospective population-based cohort study. Headache 51(4):570–80. doi:https://doi.org/10.1111/j.1526-4610.2011.01859.x
Ødegård SS, Sand T, Engstrøm M, Zwart JA, Hagen K (2013) The impact of headache and chronic musculoskeletal complaints on the risk of insomnia: longitudinal data from the Nord-Trøndelag health study. J Headache Pain 14:24
Uhlig BL, Engstrøm M, Ødegård SS, Hagen K, Sand T (2014) Headache and insomnia in population-based studies. Cephalalgia 34:745–751
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT study) is a collaboration between The HUNT Research Centre, Faculty of Medicine, The Norwegian University of Science and Technology (NTNU); and the Nord-Trøndelag County Council.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Availability of data and materials
Part of the dataset supporting the conclusions of this article is available on request to the corresponding author. Some of the data are the property of HUNT research centre and can only be accessed through direct contact with the research centre.
Author information
Authors and Affiliations
Contributions
KH: Study concept and design, collection of data, analysis and interpretation of data, writing of manuscript. AÅ, BLU, ET and EB: Collection of data, analysis and interpretation of data, critical revision of manuscript. MS, GH and GBG: Organizing the study, critical revision of manuscript. TS: Study concept and design, organizing the study, critical revision of manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests..
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hagen, K., Åsberg, A.N., Uhlig, B.L. et al. The epidemiology of headache disorders: a face-to-face interview of participants in HUNT4. J Headache Pain 19, 25 (2018). https://doi.org/10.1186/s10194-018-0854-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-018-0854-2