
Abstract
Background
Migraine is a neurological disorder resulting in large socioeconomic burden. This network meta-analysis (NMA) is designed to compare the relative efficacy and tolerability of non-steroidal anti-inflammatory agents (NSAIDs) and triptans.
Methods
We conducted systematic searches in database PubMed and Embase. Treatment effectiveness was compared by synthesizing direct and indirect evidences using NMA. The surface under curve ranking area (SUCRA) was created to rank those interventions.
Results
Eletriptan and rizatriptan are superior to sumatriptan, zolmitriptan, almotriptan, ibuprofen and aspirin with respect to pain-relief. When analyzing 2 h-nausea-absence, rizatriptan has a better efficacy than sumatriptan, while other treatments indicate no distinctive difference compared with placebo. Furthermore, sumatriptan demonstrates a higher incidence of all-adverse-event compared with diclofenac-potassium, ibuprofen and almotriptan.
Conclusion
This study suggests that eletriptan may be the most suitable therapy for migraine from a comprehensive point of view. In the meantime ibuprofen may also be a good choice for its excellent tolerability. Multi-component medication also attracts attention and may be a promising avenue for the next generation of migraine treatment.
Similar content being viewed by others

Background
Migraine is a neurological disorder resulting in large socioeconomic burden affecting approximately 18% of females and 6% of males in the United States [1]. The prevalence of migraine varies with age, females between 35 and 45 years old exhibits the highest prevalence [2]. Apart from the factor of age, the prevalence of migraine in the U.S. also varied with household income and race, and such findings are consistent with studies carried out in other countries [3, 4]. Headache is the primary symptom of migraine and patients may also be afflicted by other symptoms including pulsatile pain, light sensitivity, sound sensitivity, nausea, unilateral pain, blurred vision and emesis. Although a large number of treatments have been developed for migraine over the past decades, several disputes have been encountered by clinicians such as misclassification of migraine, inappropriate selection of treatment and medication overuse. Among them, medication overuse has become a major issue in chronic migraine patients who may eventually develop a disabling condition called medication-overuse headache [5]. Therefore, awareness and understanding of migraine should be improved and corresponding treatments or medications should be further explored to overcome these issues.
Two types of migraine therapies have been developed: preventive therapies which are used to reduce attack frequency or severity and acute therapies which are used for the sake of aborting attacks. Compared to preventive therapies, acute therapies are able to provide patients with rapid and complete relief with minimal or no adverse events and hence they are recommended for promptly alleviating the symptoms of patients [6]. The selection of acute treatments has been differentiated into two pathways: non-specific medications which include analgesics and non-steroidal anti-inflammatory drugs (NSAIDs); and specific medications which include ergot derivatives and triptans [5]. As suggested by the European Federation of Neurological Societies (EFNS), both oral NSAIDs and triptans are recommended for treating migraine attacks [7]. Moreover, evidence from the American Headache Society (AHS) concluded that the following treatments are deemed to be effective acute therapies for migraine: triptans, NSAIDs, ergotamine derivatives, opioids and other combinational medications [8]. Stratified care is a primary strategy often used in selecting medications for migraine patients and this strategy takes several aspects into account: attack severity, the presence of associated symptoms and the degree of disability resulting from migraine [9]. However, other factors such as dosage may also have significant influence on the overall effectiveness of medications that are used to abort migraine attacks.
Among the common acute treatments that are used for aborting migraine, different levels of evidence have been provided by a wide range of studies. Although the efficacy of some medications have been established, this does not imply that such medications should be considered as the first line treatments for migraine patients since it may cause adverse events that are specifically associated with these medications. Despite the growing popularity of triptans, NSAIDs remain one of the most recommended acute migraine treatments and they are often used as an initial strategy for aborting migraine attacks [9]. On the other hand, triptans are often used as a rescue medication if an initial treatment fails to abort migraine attacks and evidence suggests that about 60% of non-responders to NSAIDs can be treated by triptans [10]. One distinctive advantage of triptans for migraine patients is that they can be effective at any time during a migraine attack and such an advantage may reduce the impact of dosage timing on the overall efficacy. Moreover, some evidence suggests that earlier intervention by using triptans is associated with an enhanced efficacy [11, 12], while some randomized trials do not support such an improved efficacy when patients experienced allodynia in the course of a migraine attack [13, 14].
Despite the fact that both NSAIDs and triptans have been recommended by the EFNS and AHS as acute treatments for migraine, comparing NSAIDs with triptans is a challenging task. Conventional meta-analysis has several limitations due to the lack of evidence as well as lack of indirect evidence.. For this reason, we designed this network meta-analysis (NMA) to compares the relative efficacy and tolerability between NSAIDs and triptans. We hope that the approach of NMA can provide comprehensive evidence with respect to the efficacy and tolerability of these two popular medications.
Methods
Search strategy
We employed search strategies to explore the medical literature for relevant studies in PubMed and EMBASE systematically, and 2,967 records were identified using the following terms: “migraine disorders”, “tryptans”, “non-steroidal anti-inflammatory agents”, “ergot alkaloids”, “opioid analgesics”, “sumatriptan”, “zolmitriptan”, “almotriptan”, “rizatriptan”, “naratriptan”, “ibuprofen”, “eletriptan”, “diclofenac-potassium” and “aspirin” in PubMed. Reviewers also provided 3 additional references.
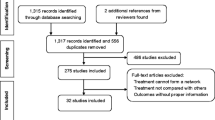
As flow chart Fig. 1 illustrates, among the total 2,970 records, 1,263 were identified as duplicates and hence removed after assessment. 1,408 more studies were excluded from the remaining 1,707 records according to the exclusion criteria, leaving 299 remnant studies. Full-text articles were viewed and included if they met the inclusion criteria, or excluded if not. Eventually 88 studies were included in this research [12, 15–101].

Study flow diagram
Inclusion criteria
Articles were included if they: (1) were randomized clinical trials (RCTs); (2) were categorized as double blind; (3) included relevant clinical outcomes and treatments; (4) contained comparisons between different treatments.
Outcome measures and data extraction
The following data were extracted from eligible studies and shown in Table 1: gender, sample size and diagnostic criteria. Two investigators reviewed the manuscripts of all included studies and extracted data into a database independently. A Jadad scale was generated and is presented in Additional file 1: Table S1. The width of the lines in Fig. 2 is proportional to the number of trials comparing each pair of treatments and the area of circles represents the cumulative number of patients for each intervention.

Network of randomized controlled trials comparing different medications agents of migraine treatments. The width of the lines is proportional to the number of trials comparing each pair of treatments; the area of circles represents the cumulative number of patients for each intervention
Statistical analysis
We initially carried out a conventional pair-wise meta-analysis which directly compares each pair of treatments. The corresponding odds ratios (ORs) and 95% confidence intervals (CIs) for each study were pooled in order to obtain the overall effect size. Furthermore, a NMA was performed for each endpoint with a Bayesian framework using R 3.2.3 software. Treatment efficacy was compared through direct and indirect evidence using the ORs and 95% credible intervals (CrIs). Then the surface under curve ranking area (SUCRA) was created to rank those interventions. The ranking probabilities were defined as cumulative probabilities with each intervention being ranked. For each endpoint, an intervention is more desirable than others with a larger SUCRA value.
Results
Trial eligibility
We included double-blind RCTs to investigate the treatment effects of triptans and NASIDs for adults according to the International Classification of Headache Disorders (ICHD), ICHD-II or the International Headache Society (IHS) criteria.
Characteristic of included studies
All studies included were double-blind RCTs involving 1 four-arm trials with 287 participants and 17 three-arm trials with 9,085 participants in all. The remaining 70 studies were two-arm trials that involve 13 comparisons and a total of 34,850 participants. A detailed list of included studies, patients and diagnostic criteria characteristics is provided in Table 1. All included studies were published between 1993 and 2016.
Pairwise comparisons
We completed pairwise meta-analysis for the 25 comparisons and the weighted ORs for each comparison were calculated. The results of the pair-wise comparisons are shown in Table 2 which illustrates the results of comparison of all 25 direct two-arm trials.
There were a total of 39,004 participants in the placebo controlled trials Direct placebo comparison results suggest all treatments are more effective than placebo with statistical significance in regards to 2 h-pain-free and 2 h-pain-relief (OR > 1, 95% CI excludes 1). All except diclofenac-potassium and almotriptan perform use of rescue medication and most drugs examined show efficacy in 1 h-pain-free and 1 h-pain-relief. Sumatriptan, zolmitriptan, rizatriptan, naratriptan and aspirin also show an increase in all-adverse events indicating some side effects.
From pairwise meta-analysis between different medications, rizatriptan is more efficacious than naratriptan concerning 1 h-pain-free, 2 h-pain-free and 2 h-pain-relief (OR < 1, 95% CI excludes 1). However, naratriptan manifests a lower recurrence than rizatriptan. Sumatriptan has a worse performance than sumatriptan-naproxen and eletriptan with respect to 2 h-pain-free and use of rescue medication. We can derive that rizatriptan and eletriptan tend to show effective performance with respect to outcomes including 1 h-pain-relief and rescue medication. However, a pairwise meta-analysis provides limited information and does not enable us to synthesize indirect evidence. Therefore we subsequently carried a NMA for further information so that all treatments could be compared and ranked.
Network meta-analysis
As suggested in Table 3 and Fig. 3, a large number of comparisons were generated by the NMA. As for 1 h-pain-free, all medication except almotriptan and naratriptan show statistical difference over placebo (Additional file 2: Figure S1). Furthermore, zolmitriptan appears to be less effective than rizatriptan and eletriptan, while other comparisons show no significant statistical difference. Likewise, results from NMA with respect to 1 h-pain-relief, only sumatriptan, zolmitriptan, rizatriptan and eletriptan show efficacy when compared with placebo but there were no statistical differences between any two of them.

Odds ratios (95% credential intervals) for network comparison of migraine treatments
For 2 h-pain-free, eletriptan shows efficacy over sumatriptan, zolmitriptan, almotriptan, ibuprofen and aspirin, while rizatriptan is more effective than sumatriptan, zolmitriptan, almotriptan, ibuprofen and aspirin but again there is no statistical evidence to determine the efficacy contrast between rizatriptan and eletriptan (Additional file 3: Figure S2).
Diclofenac-potassium appears to be more effective than any other intervention regarding 2 h-pain-relief. Apart from that, eletriptan also shows promising results compared with sumatriptan, rizatriptan, ibuprofen and aspirin. On the other hand, aspirin is less effective than rizatriptan, naratriptan, sumatriptan-naproxen, eletriptan and diclofenac-potassium. As a traditional treatment, aspirin is regarded as low performance in respect to 2 h-pain-relief, while diclofenac-potassium and eletriptan are outstanding treatments concerning this clinical outcome, and would be promising candidates in acute therapies.
When analyzing 2 h-nausea-absence, rizatriptan has better efficacy than sumatriptan while other treatments except Sumatriptan-Naproxen indicate no distinctive difference even compared with placebo.
Sumatriptan, diclofenac-potassium and rizatriptan present a much higher rate of recurrence figure compared with naratriptan and sumatriptan-naproxen. Furthermore, solid proof was obtained from the comparison between mono-sumatriptan and sumatriptan-naproxen that naproxen significantly reduces the migraine recurrence rate of sumatriptan while the efficacy of sumatriptan is barely influenced, and further experiments could be designed to investigate this mechanism and to combine treatments with a view to improve their preventive abilities.
Rescue medication data demonstrated that diclofenac-potassium performs the worst compared with rizatriptan, ibuprofen, sumatriptan-naproxen and eletriptan, thus diclofenac-potassium has the most likelihood of all treatments to require a rescue medication. Considering that naproxen has a notable promotion on the tolerability of sumatriptan and that diclofenac-potassium has outstanding behaviors with respect to efficacy, it is desirable to design further experiments to enhance the tolerability of diclofenac-potassium (Additional file 4: Figure S3).
Similarly, sumatriptan demonstrates a high all-adverse-event behavior compared with diclofenac-potassium, ibuprofen and almotriptan. Likewise naratriptan also has a poor all-adverse-event perform when compared with ibuprofen and diclofenac-potassium. In other words, diclofenac-potassium and ibuprofen are milder when compared with naratriptan and sumatriptan, which may indicate that NASIDs offer treatments with less adverse reactions. Aside from this, the combination of sumatriptan and naproxen appears to provide patients with much better tolerance in comparison to sumatriptan alone.
With respect to nausea, zolmitriptan and sumatriptan were significantly inferior to ibuprofen, sumatriptan-naproxen, eletriptan and diclofenac-potassium. Interestingly, eletriptan performs better than several other triptans (Additional file 5: Figure S4).
Finally, Fig. 4 provides the ranking diagrams showing probability of each strategy ranked (1–11) for outcomes and Table 4 provides SUCRA results for further comparison. In general, NASIDs show a more prominent tolerability while some triptans such as rizatriptan and eletriptan exhibit more promising efficacy results. On the other hand, almotriptan has the least effectiveness with respect to 1 h-pain-free and 2 h-pain-free. Similar rankings are displayed in Table 3, which reveals that diclofenac-potassium and eletriptan has the best efficacy whereas naratriptan and almotriptan are the least efficacious medications.

Probability of each medication with specific rank (1–11) for outcomes. Ranking indicates the probability to be the best treatment, the second best and so on. Rank 1st is best and Rank 11th is worst
Discussion
In this NMA, 10 medications were included and the result reveals that eletriptan offers the best efficacy and acceptable tolerability. Besides, our research indicates that ibuprofen exhibited the most desirable tolerability. Furthermore, diclofenac-potassium and sumatriptan-naproxen also showed favorable properties concerning efficacy and tolerability.
Triptans were a group of 5-HT1B/1D agonists [102], three main mechanisms of them were all conduced to anti-migraine function. Firstly, triptans attenuated the release of vasoactive peptides trigeminal system, as well as reduced the migraine vascular inflammation. Moreover, triptans were shown to potentially inhibit the nociceptive pathway of central sensitization, thus helped to relieve the pain from migraine [103, 104].
Considering the primary efficacy end-point, triptans perform equally well compared to NSAIDs though eletriptan has the best efficacy, which lends credence to the findings of Chris Cameron et al.’s 2015 study in principle [105]. However, this study did not take adverse events into account. Therefore, we apply 4 adverse-events to characterize this ability in all 10 medications. Additionally we also included a double-component therapy. Here we report this NMA, revealing both the efficacy and the tolerability of present medication against migraine.
At first, we focused on the differences apparent in the primary efficacy end-point between different types of medications. Rizatriptan provides relatively good freedom from pain and nausea though with poor pain relief, the reason for that might be the different criteria for efficacy in each study. When it comes to tolerability, NASIDs seem to be more attractive solutions. Also, it is of significance that this study found naproxen is capable of significantly improving the tolerability of sumatriptan and has no influence on its efficacy.
As suggested by the rank probability of SUCRA, eletriptan exhibited the most considerable efficacy. From the SUCRA data, it is obvious that eletriptan can reduce pain with a better result than any other medication. In the meantime it also performs better than most of others in 1 h pain-free and 2 h pain-free. Eletriptan is a new 5-HT1B/1D/1F-selective receptor agonist with a higher affinity to the receptors when compared with other triptans [106]. Besides, more rapid and consistent absorption has been achieved through structural design, and this has made it possible for the drug to pass through the blood-brain barrier [107]. As a result of its enhanced hydrophobility, higher bioavailability and longer plasma half-life have also been reported [108]. When compared with sumatriptan and other triptans, the difference in efficacy may be explained by the overcoming of the blood-brain barrier, which leads to a faster and more consistent absorption [107].
When we turn attention to the NSAIDs, ibuprofen attracted us by its superior tolerability amongst all observed medications. Though ibuprofen has been available as a non-prescription medication for more than 40 years, the mechanism of how the drug works is still not completely understood. According to a widely accepted theory, it may be related to prostaglandin synthetase inhibition, therefore allowing better tolerability. From the SUCRA data we can observe that ibuprofen ranked top three in all the adverse-event indications.
The results of SUCRA also showed that the diclopenac potassium performs with high efficacy and tolerability, in fact it stood the best option among NSAIDs from a comprehensive point of view. At the mechanism level, NSAIDs inhibit the activity of cyclooxygenase (COX), which is recognized as being composed of two isoforms (COX-1& COX-2). COX acts as a catalyst during the production for prostaglandins, a substance responsible for pain and inflammation. Diclofenac inhibit both COX isoforms, though with a lower activity for COX-2 [109, 110].
Meanwhile we recognized that sumatriptan-naproxen also offered a high-level tolerability, ranking first in rescue medication and recurrence and fourth in the other two indications among the ten medications. The addition of naproxen significantly improved the tolerability of sumatriptan. To understand the reason for this we referred to the mechanism of both the medicines and the migraine.
The pathophysiology mechanism of migraine is quite complex, involving multiple neural pathways that appear to be pivotal during the process [111]. In the early stage of a migraine, vasoactive and substances including calcitonin gene-related peptide and kinins are released by trigeminal nerve endings under the stimulation of cortical spreading depression. At the same time, the central pathways’ activation depends on the signals of pain from the periphery. However, in the later stage, central sensitization has no relationship with peripheral neural input [112].
Considering the multiple pathogenic mechanisms, multi-mechanism-targeted therapy may have better effect than monotherapy. Triptans not only decrease transmission of the pain impulses to the trigeminal nucleus caudalis but also release inflammatory mediators from trigeminal nerves, therefore reduce calcitonin gene-related peptide-mediated vasodilation [113]. As for naproxen, it suppressed sensitization of central trigeminovascular neurons in the spinal trigeminal nucleus [20]. In our study, the combination of sumatriptan and naproxen effectively altered peripheral activation of central pathways during early period and development of central sensitization during later periods. As a result, a high-level tolerability was observed, and this possibility was supported by several clinical studies [114–116].
What attracted our attention most is the potentiality to combine different medications together and make use of the advantages of each considering the relevant stage. Applying different medications to intervene at every key point of the multiple pathogenic mechanisms may bring us closer to a better outcome. For instance, we may combine naproxen with eletriptan to attain treatments with both optimal efficacy and tolerability.
As with all analyses, we still cannot avoid several limitations. First, age and gender was not under consideration. Further research is needed in assessing the efficacy for different groups of people. Second, long-term assessment is also important. As we all know, people who suffer from migraine may undergo a long-period treatment and therefore the efficacy and safety of medications are vital. Third, the dosage of medications was not considered and that may cause some deviations.
Conclusions
In conclusion, through this NMA we came to the interpretation that eletriptan may be the most suitable therapy for migraine from a comprehensive point of view. In the meantime ibuprofen may also be a good choice for its excellent tolerability. Multi-component medication also attracted our attention and it may be a promising orientation for the next generation of medication for migraine.
Article highlights
-
1.
Uses NMA to analysis the efficacy and tolerability of NSAIDs and triptans in migraine.
-
2.
Eletriptan may be the most preferable treatment for migraine from a comprehensive point of view.
-
3.
Ibuprofen has the best tolerability among all the medications.
-
4.
Multi-component medication may be a good choice for the migraine medication in the future.
References
Stewart WF, Lipton RB, Celentano DD, Reed ML (1992) Prevalence of migraine headache in the United States. Relation to age, income, race, and other sociodemographic factors. JAMA 267(1):64–69
Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M (2001) Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 41(7):646–657
Gobel H, Petersen-Braun M, Soyka D (1994) The epidemiology of headache in Germany: a nationwide survey of a representative sample on the basis of the headache classification of the International Headache Society. Cephalalgia 14(2):97–106
Henry P, Michel P, Brochet B, Dartigues JF, Tison S, Salamon R (1992) A nationwide survey of migraine in France: prevalence and clinical features in adults. GRIM. Cephalalgia 12(4):229–237, discussion 186
Antonaci F, Ghiotto N, Wu S, Pucci E, Costa A (2016) Recent advances in migraine therapy. Springerplus 5:637
Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E (2012) Evidence-based guideline update: pharmacologic treatment for episodic migraine prevention in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 78(17):1337–1345
Evers S, Afra J, Frese A, Goadsby PJ, Linde M, May A et al (2009) EFNS guideline on the drug treatment of migraine--revised report of an EFNS task force. Eur J Neurol 16(9):968–981
Marmura MJ, Silberstein SD, Schwedt TJ (2015) The acute treatment of migraine in adults: the american headache society evidence assessment of migraine pharmacotherapies. Headache 55(1):3–20
Pringsheim T, Davenport WJ, Marmura MJ, Schwedt TJ, Silberstein S (2016) How to apply the AHS evidence assessment of the acute treatment of migraine in adults to your patient with migraine. Headache 56(7):1194–1200
Diamond ML, Hettiarachchi J, Hilliard B, Sands G, Nett R (2004) Effectiveness of eletriptan in acute migraine: primary care for Excedrin nonresponders. Headache 44(3):209–216
Pascual J, Cabarrocas X (2002) Within-patient early versus delayed treatment of migraine attacks with almotriptan: the sooner the better. Headache 42(1):28–31
Dowson AJ, Massiou H, Lainez JM, Cabarrocas X (2004) Almotriptan improves response rates when treatment is within 1 hour of migraine onset. Headache 44(4):318–322
Burstein R, Collins B, Jakubowski M (2004) Defeating migraine pain with triptans: a race against the development of cutaneous allodynia. Ann Neurol 55(1):19–26
Linde M, Mellberg A, Dahlof C (2006) Subcutaneous sumatriptan provides symptomatic relief at any pain intensity or time during the migraine attack. Cephalalgia 26(2):113–121
(1999) Acute treatment of migraine attacks: efficacy and safety of a nonsteroidal anti-inflammatory drug, diclofenac-potassium, in comparison to oral sumatriptan and placebo. The Diclofenac-K/Sumatriptan Migraine Study Group. Cephalalgia 19(4):232–240
Ahrens SP, Farmer MV, Williams DL, Willoughby E, Jiang K, Block GA et al (1999) Efficacy and safety of rizatriptan wafer for the acute treatment of migraine. Cephalalgia 19(5):525–530
Barbanti P, Carpay JA, Kwong WJ, Ahmad F, Boswell D (2004) Effects of a fast disintegrating/rapid release oral formulation of sumatriptan on functional ability in patients with migraine. Curr Med Res Opin 20(12):2021–2029
Bomhof M, Paz J, Legg N, Allen C, Vandormael K, Patel K (1999) Comparison of rizatriptan 10 mg vs. naratriptan 2.5 mg in migraine. Eur Neurol 42(3):173–179
Bousser MG, D’Allens H, Richard A (1993) Efficacy of subcutaneous sumatriptan in the acute treatment of early-morning migraine: a placebo-controlled trial. Early-Morning Migraine Sumatriptan Study Group. J Intern Med 234(2):211–216
Brandes JL, Kudrow D, Stark SR, O’Carroll CP, Adelman JU, O’Donnell FJ et al (2007) Sumatriptan-naproxen for acute treatment of migraine: a randomized trial. JAMA 297(13):1443–1454
Bussone G, Manzoni GC, Cortelli P, Roncolato M, Fabbri L, Benassuti C (2000) Efficacy and tolerability of sumatriptan in the treatment of multiple migraine attacks. Neurol Sci 21(5):272–278
Cady RC, Ryan R, Jhingran P, O’Quinn S, Pait DG (1998) Sumatriptan injection reduces productivity loss during a migraine attack: results of a double-blind, placebo-controlled trial. Arch Intern Med 158(9):1013–1018
Carleton SC, Shesser RF, Pietrzak MP, Chudnofsky CR, Starkman S, Morris DL et al (1998) Double-blind, multicenter trial to compare the efficacy of intramuscular dihydroergotamine plus hydroxyzine versus intramuscular meperidine plus hydroxyzine for the emergency department treatment of acute migraine headache. Ann Emerg Med 32(2):129–138
Charlesworth BR, Dowson AJ, Purdy A, Becker WJ, Boes-Hansen S, Farkkila M (2003) Speed of onset and efficacy of zolmitriptan nasal spray in the acute treatment of migraine: a randomised, double-blind, placebo-controlled, dose-ranging study versus zolmitriptan tablet. CNS Drugs 17(9):653–667
Codispoti JR, Prior MJ, Fu M, Harte CM, Nelson EB (2001) Efficacy of nonprescription doses of ibuprofen for treating migraine headache. A randomized controlled trial. Headache 41(7):665–679
Dahlof C, Diener HC, Goadsby PJ, Massiou H, Olesen J, Schoenen J et al (1998) Zolmitriptan, a 5-HT1B/1D receptor agonist for the acute oral treatment of migraine: a multicentre, dose-range finding study. Eur J Neurol 5(6):535–543
Dahlof C, Hogenhuis L, Olesen J, Petit H, Ribbat J, Schoenen J et al (1998) Early clinical experience with subcutaneous naratriptan in the acute treatment of migraine: a dose-ranging study. Eur J Neurol 5(5):469–477
Diamond S, Elkind A, Jackson RT, Ryan R, DeBussey S, Asgharnejad M (1998) Multiple-attack efficacy and tolerability of sumatriptan nasal spray in the treatment of migraine. Arch Fam Med 7(3):234–240
Diener HC (1999) Efficacy and safety of intravenous acetylsalicylic acid lysinate compared to subcutaneous sumatriptan and parenteral placebo in the acute treatment of migraine. A double-blind, double-dummy, randomized, multicenter, parallel group study. The ASASUMAMIG Study Group. Cephalalgia 19(6):581–588, discussion 542
Diener HC, Bussone G, De Liano H, Eikermann A, Englert R, Floeter T et al (2004) Placebo-controlled comparison of effervescent acetylsalicylic acid, sumatriptan and ibuprofen in the treatment of migraine attacks. Cephalalgia 24(11):947–954
Diener HC, Eikermann A, Gessner U, Gobel H, Haag G, Lange R et al (2004) Efficacy of 1,000 mg effervescent acetylsalicylic acid and sumatriptan in treating associated migraine symptoms. Eur Neurol 52(1):50–56
Diener HC, Gendolla A, Gebert I, Beneke M (2005) Almotriptan in migraine patients who respond poorly to oral sumatriptan: a double-blind, randomized trial. Eur Neurol 53(Suppl 1):41–48
Diener HC, Jansen JP, Reches A, Pascual J, Pitei D, Steiner TJ (2002) Efficacy, tolerability and safety of oral eletriptan and ergotamine plus caffeine (Cafergot) in the acute treatment of migraine: a multicentre, randomised, double-blind, placebo-controlled comparison. Eur Neurol 47(2):99–107
Diener HC, Montagna P, Gács G, Lyczak P, Schumann G, Zöller B et al (2006) Efficacy and tolerability of diclofenac potassium sachets in migraine: a randomized, double-blind, cross-over study in comparison with diclofenac potassium tablets and placebo. Cephalalgia 26(5):537–547
Djupesland PG, Docekal P (2010) Intranasal sumatriptan powder delivered by a novel breath-actuated bi-directional device for the acute treatment of migraine: a randomised, placebo-controlled study. Cephalalgia 30(8):933–942
Dodick D, Brandes J, Elkind A, Mathew N, Rodichok L (2005) Speed of onset, efficacy and tolerability of zolmitriptan nasal spray in the acute treatment of migraine: a randomised, double-blind, placebo-controlled study. CNS Drugs 19(2):125–136
Dodick DW (2002) Almotriptan increases sustained pain-free outcomes in acute migraine: results from three controlled clinical trials. Headache 42(1):21–27
Dowson A, Ball K, Haworth D (2000) Comparison of a fixed combination of domperidone and paracetamol (Domperamol) with sumatriptan 50 mg in moderate to severe migraine: a randomised UK primary care study. Curr Med Res Opin 16(3):190–197
Dowson AJ, MacGregor EA, Purdy RA, Becker WJ, Green J, Levy SL (2002) Zolmitriptan orally disintegrating tablet is effective in the acute treatment of migraine. Cephalalgia 22(2):101–106
Dowson AJ, Massiou H, Lainez JM, Cabarrocas X (2002) Almotriptan is an effective and well-tolerated treatment for migraine pain: results of a randomized, double-blind, placebo-controlled clinical trial. Cephalalgia 22(6):453–461
Freitag F, Diamond M, Diamond S, Janssen I, Rodgers A, Skobieranda F (2008) Efficacy and tolerability of coadministration of rizatriptan and acetaminophen vs rizatriptan or acetaminophen alone for acute migraine treatment. Headache 48(6):921–930
Gallagher RM, Dennish G, Spierings EL, Chitra R (2000) A comparative trial of zolmitriptan and sumatriptan for the acute oral treatment of migraine. Headache 40(2):119–128
Gawel M, Aschoff J, May A, Charlesworth BR (2005) Zolmitriptan 5 mg nasal spray: efficacy and onset of action in the acute treatment of migraine--results from phase 1 of the REALIZE Study. Headache 45(1):7–16
Geraud G, Compagnon A, Rossi A (2002) Zolmitriptan versus a combination of acetylsalicylic acid and metoclopramide in the acute oral treatment of migraine: a double-blind, randomised, three-attack study. Eur Neurol 47(2):88–98
Geraud G, Olesen J, Pfaffenrath V, Tfelt-Hansen P, Zupping R, Diener HC et al (2000) Comparison of the efficacy of zolmitriptan and sumatriptan: issues in migraine trial design. Cephalalgia 20(1):30–38
Goadsby PJ, Massiou H, Pascual J, Diener HC, Dahlof CG, Mateos V et al (2007) Almotriptan and zolmitriptan in the acute treatment of migraine. Acta Neurol Scand 115(1):34–40
Gobel H, Winter P, Boswell D, Crisp A, Becker W, Hauge T et al (2000) Comparison of naratriptan and sumatriptan in recurrence-prone migraine patients. Naratriptan International Recurrence Study Group. Clin Ther 22(8):981–989
Goldstein J, Ryan R, Jiang K, Getson A, Norman B, Block GA et al (1998) Crossover comparison of rizatriptan 5 mg and 10 mg versus sumatriptan 25 mg and 50 mg in migraine. Rizatriptan Protocol 046 Study Group. Headache 38(10):737–747
Goldstein J, Silberstein SD, Saper JR, Elkind AH, Smith TR, Gallagher RM et al (2005) Acetaminophen, aspirin, and caffeine versus sumatriptan succinate in the early treatment of migraine: results from the ASSET trial. Headache 45(8):973–982
Goldstein J, Silberstein SD, Saper JR, Ryan RE Jr, Lipton RB (2006) Acetaminophen, aspirin, and caffeine in combination versus ibuprofen for acute migraine: results from a multicenter, double-blind, randomized, parallel-group, single-dose, placebo-controlled study. Headache 46(3):444–453
Gross ML, Kay J, Turner AM, Hallett K, Cleal AL, Hassani H (1994) Sumatriptan in acute migraine using a novel cartridge system self-injector. United Kingdom Study Group. Headache 34(10):559–563
Gruffyd-Jones K, Kies B, Middleton A, Mulder LJ, Rosjo O, Millson DS (2001) Zolmitriptan versus sumatriptan for the acute oral treatment of migraine: a randomized, double-blind, international study. Eur J Neurol 8(3):237–245
Havanka H, Dahlof C, Pop PH, Diener HC, Winter P, Whitehouse H et al (2000) Efficacy of naratriptan tablets in the acute treatment of migraine: a dose-ranging study. Naratriptan S2WB2004 Study Group. Clin Ther 22(8):970–980
Henry P, d’Allens H (1993) Subcutaneous sumatriptan in the acute treatment of migraine in patients using dihydroergotamine as prophylaxis. French Migraine Network Bordeaux-Lyon-Grenoble. Headache 33(8):432–435
Jelinski SE, Becker WJ, Christie SN, Ahmad FE, Pryse-Phillips W, Simpson SD (2006) Pain free efficacy of sumatriptan in the early treatment of migraine. Can J Neurol Sci 33(1):73–79
Kellstein DE, Lipton RB, Geetha R, Koronkiewicz K, Evans FT, Stewart WF et al (2000) Evaluation of a novel solubilized formulation of ibuprofen in the treatment of migraine headache: a randomized, double-blind, placebo-controlled, dose-ranging study. Cephalalgia 20(4):233–243
Klapper J, Lucas C, Rosjo O, Charlesworth B (2004) Benefits of treating highly disabled migraine patients with zolmitriptan while pain is mild. Cephalalgia 24(11):918–924
Kolodny A, Polis A, Battisti WP, Johnson-Pratt L, Skobieranda F (2004) Comparison of rizatriptan 5 mg and 10 mg tablets and sumatriptan 25 mg and 50 mg tablets. Cephalalgia 24(7):540–546
Lange R, Schwarz JA, Hohn M (2000) Acetylsalicylic acid effervescent 1000 mg (Aspirin) in acute migraine attacks; a multicentre, randomized, double-blind, single-dose, placebo-controlled parallel group study. Cephalalgia 20(7):663–667
Le Jeunne C, Gomez JP, Pradalier A, Titus i Albareda F, Joffroy A, Liano H et al (1999) Comparative efficacy and safety of calcium carbasalate plus metoclopramide versus ergotamine tartrate plus caffeine in the treatment of acute migraine attacks. Eur Neurol 41(1):37–43
Lewis DW, Kellstein D, Dahl G, Burke B, Frank LM, Toor S et al (2002) Children’s ibuprofen suspension for the acute treatment of pediatric migraine. Headache 42(8):780–786
Lipton RB, Baggish JS, Stewart WF, Codispoti JR, Fu M (2000) Efficacy and safety of acetaminophen in the treatment of migraine: results of a randomized, double-blind, placebo-controlled, population-based study. Arch Intern Med 160(22):3486–3492
Lipton RB, Goldstein J, Baggish JS, Yataco AR, Sorrentino JV, Quiring JN (2005) Aspirin is efficacious for the treatment of acute migraine. Headache 45(4):283–292
Lipton RB, Grosberg B, Singer RP, Pearlman SH, Sorrentino JV, Quiring JN et al (2010) Efficacy and tolerability of a new powdered formulation of diclofenac potassium for oral solution for the acute treatment of migraine: results from the International Migraine Pain Assessment Clinical Trial (IMPACT). Cephalalgia 30(11):1336–1345
Lipton RB, Stewart WF, Cady R, Hall C, O’Quinn S, Kuhn T et al (2000) Sumatriptan for the range of headaches in migraine sufferers: results of the spectrum study. Headache 40(10):783–791
Loder E, Freitag FG, Adelman J, Pearlmand S, Abu-Shakra S (2005) Pain-free rates with zolmitriptan 2.5 mg ODT in the acute treatment of migraine: results of a large double-blind placebo- controlled trial. Curr Med Res Opin 21(3):381–389
MacGregor EA, Dowson A, Davies PT (2002) Mouth-dispersible aspirin in the treatment of migraine: a placebo-controlled study. Headache 42(4):249–255
Mannix LK, Loder E, Nett R, Mueller L, Rodgers A, Hustad CM et al (2007) Rizatriptan for the acute treatment of ICHD-II proposed menstrual migraine: two prospective, randomized, placebo-controlled, double-blind studies. Cephalalgia 27(5):414–421
Mannix LK, Martin VT, Cady RK, Diamond ML, Lener SE, White JD et al (2009) Combination treatment for menstrual migraine and dysmenorrhea using sumatriptan-naproxen: two randomized controlled trials. Obstet Gynecol 114(1):106–113
Mathew NT, Finlayson G, Smith TR, Cady RK, Adelman J, Mao L et al (2007) Early intervention with almotriptan: results of the AEGIS trial (AXERT Early Migraine Intervention Study). Headache 47(2):189–198
Mathew NT, Schoenen J, Winner P, Muirhead N, Sikes CR (2003) Comparative efficacy of eletriptan 40 mg versus sumatriptan 100 mg. Headache 43(3):214–222
Misra UK, Jose M, Kalita J (2004) Rofecoxib versus ibuprofen for acute treatment of migrainne: a randomised placebo controlled trial. Postgrad Med J 80(950):720–723
Misra UK, Kalita J, Yadav RK (2007) Rizatriptan vs. ibuprofen in migraine: a randomised placebo-controlled trial. J Headache Pain 8(3):175–179
Myllyla VV, Havanka H, Herrala L, Kangasniemi P, Rautakorpi I, Turkka J et al (1998) Tolfenamic acid rapid release versus sumatriptan in the acute treatment of migraine: comparable effect in a double-blind, randomized, controlled, parallel-group study. Headache 38(3):201–207
Nappi G, Sicuteri F, Byrne M, Roncolato M, Zerbini O (1994) Oral sumatriptan compared with placebo in the acute treatment of migraine. J Neurol 241(3):138–144
Pascual J, Falk RM, Piessens F, Prusinski A, Docekal P, Robert M et al (2000) Consistent efficacy and tolerability of almotriptan in the acute treatment of multiple migraine attacks: results of a large, randomized, double-blind, placebo-controlled study. Cephalalgia 20(6):588–596
Pascual J, Vega P, Diener HC, Allen C, Vrijens F, Patel K (2000) Comparison of rizatriptan 10 mg vs. zolmitriptan 2.5 mg in the acute treatment of migraine. Rizatriptan-Zolmitriptan Study Group. Cephalalgia 20(5):455–461
Peikert A, Becker WJ, Ashford EA, Dahlof C, Hassani H, Salonen RJ (1999) Sumatriptan nasal spray: a dose-ranging study in the acute treatment of migraine. Eur J Neurol 6(1):43–49
Peroutka SJ, Lyon JA, Swarbrick J, Lipton RB, Kolodner K, Goldstein J (2004) Efficacy of diclofenac sodium softgel 100 mg with or without caffeine 100 mg in migraine without aura: a randomized, double-blind, crossover study. Headache 44(2):136–141
Pfaffenrath V, Cunin G, Sjonell G, Prendergast S (1998) Efficacy and safety of sumatriptan tablets (25 mg, 50 mg, and 100 mg) in the acute treatment of migraine: defining the optimum doses of oral sumatriptan. Headache 38(3):184–190
Rothner AD, Wasiewski W, Winner P, Lewis D, Stankowski J (2006) Zolmitriptan oral tablet in migraine treatment: high placebo responses in adolescents. Headache 46(1):101–109
Ryan RE Jr, Diamond S, Giammarco RAM, Aurora SK, Reed RC, Fletcher PE (2000) Efficacy of Zolmitriptan at early time-points for the acute treatment of migraine and treatment of recurrence: a randomised, placebo-controlled trial. CNS Drugs 13(3):215–226
Sakai F, Iwata M, Tashiro K, Itoyama Y, Tsuji S, Fukuuchi Y et al (2002) Zolmitriptan is effective and well tolerated in Japanese patients with migraine: a dose–response study. Cephalalgia 22(5):376–383
Salonen R, Ashford E, Dahlof C, Dawson R, Gilhus NE, Luben V et al (1994) Intranasal sumatriptan for the acute treatment of migraine. International Intranasal Sumatriptan Study Group. J Neurol 241(8):463–469
Scherl ER, Wilson JF (1995) Comparison of dihydroergotamine with metoclopramide versus meperidine with promethazine in the treatment of acute migraine. Headache 35(5):256–259
Schulman EA, Cady RK, Henry D, Batenhorst AS, Putnam DG, Watson CB et al (2000) Effectiveness of sumatriptan in reducing productivity loss due to migraine: results of a randomized, double-blind, placebo-controlled clinical trial. Mayo Clin Proc 75(8):782–789
Schulman EA, Dermott KF (2003) Sumatriptan plus metoclopramide in triptan-nonresponsive migraineurs. Headache 43(7):729–733
Sheftell FD, Dahlof CG, Brandes JL, Agosti R, Jones MW, Barrett PS (2005) Two replicate randomized, double-blind, placebo-controlled trials of the time to onset of pain relief in the acute treatment of migraine with a fast-disintegrating/rapid-release formulation of sumatriptan tablets. Clin Ther 27(4):407–417
Smith TR, Sunshine A, Stark SR, Littlefield DE, Spruill SE, Alexander WJ (2005) Sumatriptan and naproxen sodium for the acute treatment of migraine. Headache 45(8):983–991
Spierings EL, Gomez-Mancilla B, Grosz DE, Rowland CR, Whaley FS, Jirgens KJ (2001) Oral almotriptan vs. oral sumatriptan in the abortive treatment of migraine: a double-blind, randomized, parallel-group, optimum-dose comparison. Arch Neurol 58(6):944–950
Spierings EL, Rapoport AM, Dodick DW, Charlesworth B (2004) Acute treatment of migraine with zolmitriptan 5 mg orally disintegrating tablet. CNS Drugs 18(15):1133–1141
Steiner TJ, Diener HC, MacGregor EA, Schoenen J, Muirheads N, Sikes CR (2003) Comparative efficacy of eletriptan and zolmitriptan in the acute treatment of migraine. Cephalalgia 23(10):942–952
Teall J, Tuchman M, Cutler N, Gross M, Willoughby E, Smith B et al (1998) Rizatriptan (MAXALT) for the acute treatment of migraine and migraine recurrence. A placebo-controlled, outpatient study. Headache 38(4):281–287
Tepper SJ, Donnan GA, Dowson AJ, Bomhof MA, Elkind A, Meloche J et al (1999) A long-term study to maximise migraine relief with zolmitriptan. Curr Med Res Opin 15(4):254–271
Tfelt-Hansen P, Henry P, Mulder LJ, Scheldewaert RG, Schoenen J, Chazot G (1995) The effectiveness of combined oral lysine acetylsalicylate and metoclopramide compared with oral sumatriptan for migraine. Lancet 346(8980):923–926
Tfelt-Hansen P, Teall J, Rodriguez F, Giacovazzo M, Paz J, Malbecq W et al (1998) Oral rizatriptan versus oral sumatriptan: a direct comparative study in the acute treatment of migraine. Rizatriptan 030 Study Group. Headache 38(10):748–755
Touchon J, Bertin L, Pilgrim AJ, Ashford E, Bes A (1996) A comparison of subcutaneous sumatriptan and dihydroergotamine nasal spray in the acute treatment of migraine. Neurology 47(2):361–365
Tullo V, Allais G, Ferrari MD, Curone M, Mea E, Omboni S et al (2010) Frovatriptan versus zolmitriptan for the acute treatment of migraine: a double-blind, randomized, multicenter, Italian study. Neurol Sci 31(Suppl 1):S51–S54
Wang SJ, Fuh JL, Wu ZA (2007) Intranasal sumatriptan study with high placebo response in Taiwanese patients with migraine. J Chin Med Assoc 70(2):39–46
Wendt J, Cady R, Singer R, Peters K, Webster C, Kori S et al (2006) A randomized, double-blind, placebo-controlled trial of the efficacy and tolerability of a 4-mg dose of subcutaneous sumatriptan for the treatment of acute migraine attacks in adults. Clin Ther 28(4):517–526
Winner P, Mannix LK, Putnam DG, McNeal S, Kwong J, O’Quinn S et al (2003) Pain-free results with sumatriptan taken at the first sign of migraine pain: 2 randomized, double-blind, placebo-controlled studies. Mayo Clin Proc 78(10):1214–1222
Capi M, Curto M, Lionetto L, de Andres F, Gentile G, Negro A et al (2016) Eletriptan in the management of acute migraine: an update on the evidence for efficacy, safety, and consistent response. Ther Adv Neurol Disord 9(5):414–423
Lionetto L, Casolla B, Mastropietri F, D’Alonzo L, Negro A, Simmaco M et al (2012) Pharmacokinetic evaluation of zolmitriptan for the treatment of migraines. Expert Opin Drug Metab Toxicol 8(8):1043–1050
Napoletano F, Lionetto L, Martelletti P (2014) Sumatriptan in clinical practice: effectiveness in migraine and the problem of psychiatric comorbidity. Expert Opin Pharmacother 15(3):303–305
Cameron C, Kelly S, Hsieh SC, Murphy M, Chen L, Kotb A et al (2015) Triptans in the acute treatment of migraine: a systematic review and network meta-analysis. Headache 55(Suppl 4):221–235
Napier C, Stewart M, Melrose H, Hopkins B, McHarg A, Wallis R (1999) Characterisation of the 5-HT receptor binding profile of eletriptan and kinetics of [3H]eletriptan binding at human 5-HT1B and 5-HT1D receptors. Eur J Pharmacol 368(2–3):259–268
Knyihar-Csillik E, Tajti J, Csillik AE, Chadaide Z, Mihaly A, Vecsei L (2000) Effects of eletriptan on the peptidergic innervation of the cerebral dura mater and trigeminal ganglion, and on the expression of c-fos and c-jun in the trigeminal complex of the rat in an experimental migraine model. Eur J Neurosci 12(11):3991–4002
Johnson DE, Rollema H, Schmidt AW, McHarg AD (2001) Serotonergic effects and extracellular brain levels of eletriptan, zolmitriptan and sumatriptan in rat brain. Eur J Pharmacol 425(3):203–210
Patrono C, Patrignani P, Garcia Rodriguez LA (2001) Cyclooxygenase-selective inhibition of prostanoid formation: transducing biochemical selectivity into clinical read-outs. J Clin Invest 108(1):7–13
Patrono C, Baigent C (2009) Low-dose aspirin, coxibs, and other NSAIDS: a clinical mosaic emerges. Mol Interv 9(1):31–39
Goadsby PJ, Lipton RB, Ferrari MD (2002) Migraine--current understanding and treatment. N Engl J Med 346(4):257–270
Burstein R, Cutrer MF, Yarnitsky D (2000) The development of cutaneous allodynia during a migraine attack clinical evidence for the sequential recruitment of spinal and supraspinal nociceptive neurons in migraine. Brain 123(Pt 8):1703–1709
Burstein R (2001) Deconstructing migraine headache into peripheral and central sensitization. Pain 89(2–3):107–110
Loo CY, Tan HJ, Teh HS, Raymond AA (2007) Randomised, open label, controlled trial of celecoxib in the treatment of acute migraine. Singapore Med J 48(9):834–839
Krymchantowski AV, Bigal ME (2004) Rizatriptan versus rizatriptan plus rofecoxib versus rizatriptan plus tolfenamic acid in the acute treatment of migraine. BMC Neurol 4:10
Krymchantowski AV, Barbosa JS (2002) Rizatriptan combined with rofecoxib vs. rizatriptan for the acute treatment of migraine: an open label pilot study. Cephalalgia 22(4):309–312
Funding
None.
Authors’ contributions
HX and ML were involved in conception and design of the study. WH collected, analyzed, and interpreted the data. The manuscript was drafted by HX and JW. All authors reviewed and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Additional files
Additional file 1: Table S1.
Jadad scale table of 88 included studies (DOCX 20 kb)
Additional file 2: Figure S1.
Node splitting of direct and indirect comparisons according to type of interventions for 1 h clinical outcomes. (EPS 1868 kb)
Additional file 3: Figure S2.
Node splitting of direct and indirect comparisons according to type of interventions for 2 h clinical outcomes. (EPS 2444 kb)
Additional file 4: Figure S3.
Node splitting of direct and indirect comparisons according to type of interventions for rescue medication and recurrence. (EPS 1963 kb)
Additional file 5: Figure S4.
Node splitting of direct and indirect comparisons according to type of interventions for all adverse events. Treatment: A Placebo; B Sumatriptan; C Zolmitriptan; D Almotriptan; E Rizatriptan; F Naratriptan; G Ibuprofen; H Sumatriptan-Naproxen; I Eletriptan; J Diclofenacpotassium; K Aspirin. (EPS 2065 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Xu, H., Han, W., Wang, J. et al. Network meta-analysis of migraine disorder treatment by NSAIDs and triptans. J Headache Pain 17, 113 (2016). https://doi.org/10.1186/s10194-016-0703-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-016-0703-0