
Abstract
Introduction
Continuous positive airway pressure ventilation (CPAP) and non-invasive positive pressure ventilation (NPPV) are accepted treatments in acute cardiogenic pulmonary edema (ACPE). However, it remains unclear whether NPPV is better than CPAP in reducing the need for endotracheal intubation (NETI) rates, mortality and other adverse events. Our aim was to review the evidence about the efficacy and safety of these two methods in ACPE management.
Methods
We conducted a systematic review and meta-analysis of randomized controlled trials on the effect of CPAP and/or NIPV in the treatment of ACPE, considering the outcomes NETI, mortality and incidence of acute myocardial infarction (AMI). We searched six electronic databases up to May 2005 without language restrictions, reviewed references of relevant articles, hand searched conference proceedings and contacted experts.
Results
Of 790 articles identified, 17 were included. In a pooled analysis, 10 studies of CPAP compared to standard medical therapy (SMT) showed a significant 22% absolute risk reduction (ARR) in NETI (95% confidence interval (CI), -34% to -10%) and 13% in mortality (95%CI, -22% to -5%). Six studies of NPPV compared to SMT showed an 18% ARR in NETI (95%CI, -32% to -4%) and 7% in mortality (95%CI, -14% to 0%). Seven studies of NPPV compared to CPAP showed a non-significant 3% ARR in NETI (95%CI, -4% to 9%) and 2% in mortality (95%CI, -6% to 10%). None of these methods increased AMI risk. In a subgroup analysis, NPPV did not lead to better outcomes than CPAP in studies including more hypercapnic patients.
Conclusion
Robust evidence now supports the use of CPAP and NPPV in ACPE. Both techniques decrease NETI and mortality compared to SMT and none shows increased AMI risk. CPAP should be considered a first line intervention as NPPV did not show a better efficacy, even in patients with more severe conditions, and CPAP is cheaper and easier to implement in clinical practice.
Similar content being viewed by others


Introduction
The public health burden of heart failure is very high. In the United States, heart failure is the most frequent cause of hospitalization in persons over 65 years of age [1], and in 2004, the estimated direct and indirect costs were 25.8 billion dollars [2]. A 4% hospital mortality due to heart failure was recently reported [3]. This rate increases to 36% in severe cases needing mechanical ventilation [4].
During the past 10 years, continuous positive airway pressure (CPAP) and non-invasive positive pressure ventilation (NPPV) have gained decisive roles in the management of various forms of respiratory failure [5][6]. Non-invasive ventilation achieves physiological improvement and efficacy similar to invasive ventilation [7], and by avoiding endotracheal intubation (ETI) reduces morbidity and complications [6].
Both NPPV and CPAP have been successfully used in patients with acute cardiogenic pulmonary edema (ACPE) [8, 9]. A meta-analysis pooling data from three randomized controlled trials (RCTs) [10], published seven years ago, supported the efficacy of CPAP in avoiding ETI in ACPE patients, but showed no evidence of improved survival. Since that publication, several new RCTs have been published comparing NPPV, CPAP and standard medical therapy (SMT) in ACPE patients [11–25]. However, because most of them were small, several issues remain unresolved. The evidence about the size and significance of a reduction in mortality and about whether one technique is superior to the other remains unclear. Clinically important questions about which technique would lead to better outcomes in more hypercapnic patients [19] and about the best level of pressure support in NPPV [26] have also been raised, and may be preventing the wider use of these technologies.
Concerns have also been raised about safety issues related to non-invasive ventilation. Mehta and colleagues [25] showed, in an interim analysis of an RCT, an increased risk of acute myocardial infarction (AMI) in patients treated with NPPV. Due to the limited number of patients enrolled, however, those results were not conclusive, suggesting the need for a critical analysis of the safety of NPPV and CPAP in the treatment of ACPE.
A very recent meta-analysis unfortunately addressed only some of the questions to which clinicians need answers. Masip and colleagues [27], showed that non-invasive ventilation – jointly considering CPAP and NPPV together as if they were the same technology – was associated with a 43% relative risk reduction in mortality and 56% relative risk reduction in the need for ETI, and found no significant differences in efficacy between those two modalities. An important criticism of this review is that it presents results for non-invasive ventilation (pooling CPAP and NPPV together) and consequently double counting control group patients in three studies (with three arms), inflating the number of patients included and having potential impact on the calculated confidence intervals and conclusions. Moreover, this meta-analysis failed to include two useful studies (one inappropriately excluded and one not found). It also did not analyze evidence about differences in efficacy in the subset of more hypercapnic patients or about differences related to the level of pressure support in NPPV. It commented on but did not present relevant data, or thoroughly analyze, the potentially increased AMI risk associated with non-invasive ventilation, another issue that concerns clinicians. Finally, the results of this meta-analysis were presented using the relative risk scale, which is less easy to translate to practice and more challenging for clinicians to understand.
The aim of our study was to systematically review the evidence in order to answer key clinical questions about the efficacy and safety of CPAP and NPPV in the treatment of patients with ACPE, considering three different outcomes: the need for ETI; in-hospital all cause mortality; and incidence of newly developed AMI. We specifically and separately addressed three different comparisons: CPAP and SMT versus SMT alone; NPPV and SMT versus SMT alone; and NPPV and SMT versus CPAP and SMT. Secondary aims were to analyze the impact of patients' baseline hypercapnia on the efficacy of CPAP and NPPV and to test a common clinical hypothesis about the advantage of NPPV when using higher levels of pressure support ventilation.
Materials and methods
Study design
A systematic review and meta-analysis of RCTs focusing on the effect of CPAP and NPPV in the treatment of ACPE was undertaken. The methodological approach included the development of selection criteria, definition of search strategies, quality assessment of the studies, data abstraction and statistical data analysis [28].
Selection criteria
The study selection criteria were defined before data collection, in order to properly identify high quality studies eligible for the analysis.
The following inclusion criteria were defined. Patient population: adult patients presenting to hospital with ACPE, defined as existence of dyspnea of sudden onset, increased respiratory rate, a compatible physical examination (bilateral crackles on pulmonary auscultation, elevated jugular venous pressure, third heart sound on cardiac auscultation), bilateral pulmonary infiltrates on chest radiograph plus significant hypoxemia. Study design: prospective randomized parallel trials with independent randomization of ACPE patients. Interventions: use of CPAP (delivered using any device) and medical therapy compared with standard medical therapy alone; use of NPPV (with any device) and medical therapy compared with standard medical therapy alone; or use of CPAP and medical therapy compared with NPPV and medical therapy. Outcomes: need for ETI as decided by trialists, all-cause mortality and risk of newly developed AMI after delivery of study interventions.
To improve the internal validity of this meta-analysis, we decided to consider separately trials of NPPV and CPAP, because these two methods have different technical, physiological and clinical characteristics. Pooling those two interventions in a single 'non-invasive ventilation' intervention may not be appropriate and could have led to additional heterogeneity and patient overlap in trials with three arms. Also, trials that included both acute respiratory failure and ACPE patients [29–33] were included only if there was independent stratified randomization of therapies for this sub-group.
Search strategy
Our primary method to locate potentially eligible studies was a computerized literature search in the MEDLINE database, from inception to May 2005, without any restriction on language of publication, using the following search keywords and MeSH terms: (artificial respiration or continuous positive airway pressure or non-invasive positive pressure ventilation or non-invasive ventilation or non-invasive ventilation) and (pulmonary edema or pulmonary oedema or congestive heart failure) and (clinical and trial or clinical trials or clinical trial or random* or random allocation or therapeutic use). Literature searches were also undertaken, using the same search keywords, in the following databases: the American College of Physicians (ACP) Journal Club Database; the Cochrane Central Register of Controlled Trials (CCTR); the Cochrane Database of Systematic Reviews (CDSR); the Digital Academic Repositories (DARE) Database; and the MetaRegister of Controlled Trials at Current Controlled Trials webpage.
In defining all search strategies we gave priority to formats with higher sensitivity, in order to increase the probability of identifying all relevant articles.
We also reviewed the references of all relevant articles and review articles, hand searched abstracts and conference proceedings of recent relevant congresses and scientific forums from 2000 to 2005, and contacted authors and experts working in this field.
Study quality assessment and data abstraction
In the first phase of selection, the titles and abstracts of the retrieved studies were screened for relevance by two reviewers. In the second phase, two reviewers (ALF and WJC) independently analyzed the full-papers of articles identified as potentially relevant. Selection criteria were applied, exclusions were decided and disagreements settled by consensus. Data abstraction for quality assessment and pooled analysis was performed independently using a previously specified standardized form. Quality assessment considered two types of study quality criteria, general and specific.
The general quality criteria included methodological and reporting characteristics of RCTs generally accepted as appropriate to evaluate this type of study (Table 1). The specific quality criteria included characteristics specifically relevant to RCTs studying ACPE patients and the effect of non-invasive ventilation (Table 1).
Statistical analysis
For the pooled assessment of treatment effects in the three comparisons (CPAP versus SMT, NPPV versus SMT and CPAP versus NPPV) and the three outcome variables (need for ETI, mortality and AMI risk) in this review, we used the Mantel-Haenszel method for fixed effects estimation and the DerSimonian and Laird method for random effects estimation. One problem that could have arisen in the pooled analysis is that of patient overlap because of the inclusion of studies with three arms (CPAP, NPPV and SMT)[15, 21, 23]. To overcome this problem, among other previously stated reasons, we separately considered the three comparisons CPAP versus SMT, NPPV versus SMT and CPAP versus NPPV.
We used risk difference (absolute risk reduction) as the scale for measuring efficacy and side effects because clinicians find it a more intuitive and interpretable metric as it measures the absolute difference between outcome risks in intervention and control groups, rather than odds ratios or relative risks, which many clinicians and patients find hard to understand [34, 35].
Heterogeneity of treatment effects was assessed by graphical inspection of forest plots and formally using the Q statistic (at a p value ≤ 0.1) and I2 statistic for estimating inconsistency among study results. The random effects model for pooling effects was preferred and always used if heterogeneity of treatment effects was present. Subgroup and sensitivity analysis were performed following a predefined protocol and considering the hypothesis previously presented.
Potential publication bias was assessed by visual analysis of the funnel plots, which allows evaluation of publication bias by presenting the study's risk difference plotted as a function of its standard error, and then formally checked by the rank correlation test of Begg [36].
The data processing and statistical analysis were performed using the Cochrane Collaboration's Review Manager Software version 4.2 [37] and RevMan Analyses software version 1.0 [38].
Results
Search and study selection
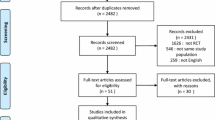
A total of 790 articles were identified using the search strategy and sources listed. After screening titles and abstracts for relevance, 744 articles were excluded (the reasons for exclusion are presented in Figure 1). The remaining 46 articles were retrieved for more detailed full paper evaluation and 22 were excluded [18, 39–51] (Figure 1). Eight other articles reporting randomized controlled trials in ACPE patients were excluded, for the following reasons: two because different interventions were studied [52, 53]; one because it was a randomized cross-over trial focusing on physiological outcome variables [54]; two because of probable patient overlap [55, 56] with the included studies by Crane and colleagues [21] and Lin and colleagues [57]; one because its abstract and full paper were published in Chinese [58]; one (by Sharon and colleagues [59]) because it was performed in a pre-hospital setting and had a different intervention in the control group – SMT plus high dose IV isossorbide-dinitrate – and has been frequently criticized for its methodological problems [60]; and one conference abstract by Liesching and colleagues reporting an RCT comparing NPPV versus CPAP was withdrawn because it was not possible to obtain the minimum information on study design, patients, interventions and outcomes [61].

Flow chart of the study selection process. ACPO, acute cardiogenic pulmonary edema; ARF = acute respiratory failure; CPAP, continuous positive airway pressure ventilation; ETI, endotracheal intubation; NPPV, non-invasive positive pressure ventilation; MT, medical therapy.
Unlike the other meta-analysis previously published [27], we did not excluded the article by Takeda and colleagues [12] because there is no evidence of patient overlap with the other study by the same authors [11]. Patient inclusions in the two articles have different time frames and settings [11, 12].
The final study cohort consisted of 17 studies: seven comparing CPAP with SMT [11, 12, 16, 22, 57, 62, 63], three comparing NPPV with SMT [13, 14, 19], four comparing CPAP directly with NPPV [17, 20, 24, 25] and three studies each with three arms comparing CPAP, NPPV and SMT [15, 21, 23] (Table 2).
Methodological quality of included studies
Study quality assessment considered two types of criteria: general and specific. The general quality criteria are presented in Table 2. The studies had generally small sample sizes (median, 40 patients; range, 22 to 130); the total number of patients included was 938. Most of them had adequate randomization concealment and adequate selection criteria. Four out of 17 did not report an intention-to-treat analysis. Only one study blinded physicians, nurses and patients to the intervention by covering the control panel of the ventilator. Almost none of the studies reported or commented on blinding strategies. Most of them reported on strategies for standardization of co-interventions and had complete follow-up details for all participants. Six out of 17 studies had inadequate or unclear outcome definitions.
The specific quality criteria are presented in Table 3. There were several different definitions of ACPE (see Table 3), but most of them included the basic criteria considered in our definition (existence of dyspnea of sudden onset, increased respiratory rate, a compatible physical examination, bilateral crackles on pulmonary auscultation, elevated jugular venous pressure, third heart sound on cardiac auscultation, bilateral pulmonary infiltrates on chest radiograph plus significant hypoxemia). Inclusion and exclusion criteria had some variability (Table 3), with some studies including much selected groups of patients. Baseline co-morbidities differed between studies and in some studies the presence of chronic obstructive pulmonary disease (COPD) or AMI was considered as exclusion criteria (Table 3). The frequency of AMI at baseline, for each study, is presented in Table 3. Major differences were found among studies regarding the methods of implementation and technical characteristics of the ventilation devices (Table 3) and regarding the definition and adequacy of criteria for ETI (Table 3).
The analysis of safety issues will mainly focus on comparisons of AMI risk among interventions. Some other adverse events of non-invasive ventilation were reported sporadically by authors (facial erythema, nasal skin necrosis, vomiting, gastric distension, pulmonary aspiration, barotrauma and asphyxia), but were always described as rare events.
Continuous positive airway pressure ventilation versus standard medical therapy
Results of studies comparing CPAP therapy with SMT are presented in Figure 2. In the random effects pooled analysis, CPAP therapy showed a statistically significant 22% risk reduction in need for ETI (95% confidence interval (CI), -34% to -10%; p = 0.0004) and a 13% risk reduction for mortality (95%CI, -22% to -5%; p = 0.0003). Significant heterogeneity was found in the pooled analysis of need for ETI and borderline significant heterogeneity was found for mortality (Cochran's Q chi-square test, p = 0.0004; I2 = 70.1% for intubation and Cochran's Q chi-square test, p = 0.060; I2 = 44.1% for mortality). Nevertheless, all studies but one found a reduction of risk in the CPAP group. Heterogeneity is in part related to the extreme findings of 55% risk reduction for both ETI and mortality in the study by Takeda and colleagues [12].

Results and pooled analysis of absolute risk differences (RDs) for the outcomes (a) need for endotracheal intubation, (b) mortality and (c) acute myocardial infarction in trials comparing continuous positive airway pressure ventilation (CPAP) versus medical therapy in acute cardiogenic pulmonary edema patients.
Only three studies included data on myocardial infarction and the random effects pooled analysis showed no difference in AMI risk between the CPAP and SMT groups (Risk Difference – RD, -1%; 95%CI, -13% to 11%; p = 0.910) and non-significant heterogeneity (Cochran's Q chi-square test, p = 0.22; I2 = 33.2%).
Non-invasive positive pressure ventilation versus standard medical therapy
Results of the studies comparing NPPV with SMT are presented in Figure 3. The random effects pooled analysis showed a statistically significant 18% risk reduction in need for ETI (95%CI, -32% to -4%; p = 0.010) and a non-significant 7% risk reduction for mortality (95%CI, -14% to 0%; p = 0.060) favoring the NPPV group. Significant heterogeneity was found in the pooled analysis of need for ETI (Cochran's Q chi-square test, p = 0.02; I2 = 62.9%), but again, all studies but one showed risk reduction for the NPPV group.

Results and pooled analysis of absolute risk differences (RDs) for the outcomes (a) need for endotracheal intubation, (b) mortality and (c) acute myocardial infarction in trials comparing non-invasive positive pressure ventilation (NPPV) versus medical therapy in acute cardiogenic pulmonary edema patients.
Random effects pooled analysis of risk differences for AMI showed a small but non-significant risk increase for the NPPV group (RD, 1%; 95%CI, -4% to 5%; p = 0.720).
To test the clinical hypothesis about an advantage of NPPV over SMT when using higher levels of pressure support ventilation [26], we performed a predefined subgroup analysis (Forest plots not presented but available on request) with stratification based on the level of pressure support ventilation (Pressure Support Ventilation – PSV ≥ 10.0 cmH2O versus PSV < 10.0 cmH2O; Table 3). In the subgroup of studies with higher levels of pressure support ventilation [13, 21], a random effects pooled analysis showed a statistically non-significant risk reduction in need for ETI (RD, -13%; 95%CI -44% to 19%; p = 0.430; Cochran's Q chi-square test for heterogeneity, p = 0.020) and mortality (RD, -9%; 95%CI -24% to 5%; p = 0.190; Cochran's Q chi-square test for heterogeneity, p = 0.670) favoring the NPPV group. In the subgroup of studies with lower levels of pressure support ventilation [14, 15, 19, 23], the random effects pooled analysis showed a statistically significant risk reduction in need for ETI (RD, -22%; 95%CI -40% to -3%; p = 0.020; Cochran's Q chi-square test for heterogeneity, p = 0.060) and a non-significant risk reduction for mortality (RD, -6%; 95%CI -14% to 2%; p = 0.160; Cochran's Q chi-square test for heterogeneity, p = 0.690) favoring the NPPV group.
Continuous positive airway pressure ventilation versus non-invasive positive pressure ventilation
Results from studies directly comparing CPAP with NPPV are presented in Figure 4. The random effects pooled analysis showed a statistically non-significant need for ETI risk reduction (RD, 3%; 95%CI -4% to 9%; p = 0.041) and mortality reduction (RD, 2%; 95%CI -6% to 10%; p = 0.640) in the NPPV group. No evidence of significant heterogeneity in need for ETI was found (Cochran's Q chi-square test, p = 0.340; I2 = 11.5%). Heterogeneity with borderline significance was found for mortality (Cochran's Q chi-square test, p = 0.100; I2 = 44.4%). A fixed effects pooled analysis, which could be considered appropriate in this case due to the absence of heterogeneity, obtained similar non-significant results (RD, 4%; 95%CI -2% to 10% and RD, 2%; 95%CI -5% to 8% for ETI and mortality, respectively).

Results and pooled analysis of absolute risk differences (RDs) for the outcomes (a) need for endotracheal intubation, (b) mortality and (c) acute myocardial infarction in trials comparing of continuous positive airway pressure ventilation (CPAP) versus non-invasive positive pressure ventilation (NPPV) in acute cardiogenic pulmonary edema patients patients.
Random effects pooled analysis of risk differences for AMI showed a non-significant risk reduction in the CPAP group (RD, -5%; 95%CI, -18% to 8%; p = 0.430).
To explore the hypothesis proposed by some clinicians on the advantage of NPPV over CPAP in hypercapnic patients [19], we analyzed the impact of patients' baseline hypercapnia in the comparison between CPAP and NPPV. A subgroup analysis was performed (Figure 5) with stratification based on mean baseline level of arterial carbon dioxide pressure, (PaCO2 <50 mmHg versus PaCO2 ≥ 50 mmHg). In the group of studies with more hypercapnic patients at baseline, the random effects pooled analysis showed a statistically non-significant risk reduction in need for ETI (RD, 2%; 95%CI -5% to 9%; p = 0.560) and mortality (RD, 2%; 95%CI -9% to 13%; p = 0.690) favoring the NPPV group. In the group of studies with less hypercapnic patients at baseline, the random effects pooled analysis showed a statistically non-significant risk reduction in need for ETI (RD, 13%; 95%CI -20% to 46%; p = 0.430) and a non-significant risk increase for mortality (RD, -1%; 95%CI -12% to 10%; p = 0.820) for the NPPV group.

Results and pooled analysis of absolute risk differences (RDs) for the outcomes (a) need for endotracheal intubation, (b) mortality and (c) acute myocardial infarction in trials comparing of continuous positive airway pressure ventilation (CPAP) versus non-invasive positive pressure ventilation (NPPV) in acute cardiogenic pulmonary edema patients patients. Subgroup analysis with stratification by baseline PaCO2 level.
Publication bias
Funnel plots are presented in Figure 6. Although separate analyses for all outcomes and comparisons were performed, we only present here the analysis of potential publication bias for the need for ETI, because results regarding other outcomes are very similar.

Funnel plots with effect measures (risk difference (RD)) as a function of its standard error (SE) for the outcome endotracheal intubation in trials comparing (a) continuous positive airway pressure ventilation (CPAP) versus medical therapy; (b) non-invasive positive pressure ventilation (NPPV) versus medical therapy and CPAP versus NPPV.
For the comparison of CPAP versus SMT, the funnel plot is approximately symmetrical, but larger studies (more precise measures of effect) tend to have smaller effects and smaller studies (less precise measures of effect) tend to have larger effects. The rank correlation test of Begg gives a non-significant result (p = 0.325), so the absence of publication bias cannot be rejected. For the comparison of NPPV versus SMT the funnel plot is asymmetrical and seems to indicate a lack of small studies with small effects. The rank correlation test of Begg gives a non-significant result (p = 0.251). For the comparison of CPAP versus NPPV the funnel plot is asymmetrical and indicates a lack of small studies with effects favoring CPAP therapy. For this comparison, there seems to be some evidence of a publication bias, favoring the publication of studies with positive results for NPPV therapy. Nonetheless, the rank correlation test of Begg gives, once again, a non-significant result (p = 0.129).
Discussion
ACPE is a rather common condition and may require mechanical ventilation [64], leading to high in-hospital mortality. The use of non-invasive ventilation to treat ACPE was first described by Poulton and colleagues [65] more than 60 years ago, and seven years ago the first meta-analysis appeared, showing the efficacy of CPAP in the treatment of ACPE [10]. Since then, several RCTs comparing the use of CPAP and NPPV with SMT or with each other have been published, and the role of non-invasive ventilation, and specially CPAP, in ACPE patients is becoming more clearly defined.
The present meta-analysis focused on important, unresolved clinical questions about the efficacy and safety of these techniques that could be delaying their uptake in most centers.
First, the meta-analysis shows that, in patients with ACPE, CPAP and NPPV, both significantly decrease need for ETI risk, and CPAP alone significantly reduces mortality when compared to SMT. Both NPPV and CPAP appear to be equivalent in reducing need for ETI and mortality. NPPV does not yet show a significant reduction in mortality, probably due to the low power related to the limited number of patients in the studies analyzed.
To put this evidence of clinical efficacy into context, it is also important to take into account the costs and difficulties involved in implementing non-invasive ventilation in clinical practice and the logistic differences between using the two non-invasive ventilation techniques. It is clear that CPAP is more easily implemented in clinical practice and that it carries smaller associated costs [53]. In fact, the cost-effectiveness of CPAP has already been demonstrated [66].
Second, our analysis of the safety of these methods showed that, although some caution is still advised, there is no evidence of increased risk of AMI with either of these techniques and the other adverse events described with these techniques are very rare. Although one study [25] found a higher incidence of AMI with NPPV, subsequent research has not confirmed this finding [13, 19–21, 23]. In the present meta-analysis, there was no significant difference in the risk of AMI between CPAP and NPPV when compared to SMT. Careful and frequent monitoring of patients with ACPE is mandatory, especially in the presence of AMI, but there is no evidence from these trials to contraindicate the use of NPPV.
Third, in a subgroup analysis of studies including patients with mean baseline PaCO2 levels below and above 50 mmHg, NPPV showed only a small trend towards decreased need for ETI and mortality, so the suggested superiority of NPPV in hypercapnic ACPE patients due to respiratory muscle unloading [19] was not confirmed. Although a number of studies in our meta-analysis included patients with ACPE and coexisting COPD [13, 19–21], who one would expect to benefit the most from NPPV [67], studies including hypercapnic ACPE patients without COPD also showed significant improvement in PaCO2 with CPAP [24].
Fourth, in a subgroup analysis we found no evidence supporting the clinical hypothesis about the advantage of NPPV over SMT when using higher levels of pressure support ventilation [26, 13, 21].
Although our conclusions appear robust and well supported by the evidence, this meta-analysis has some limitations that should be pointed out. We found important clinical differences among the studies included in the analysis. The patients selected may not be completely comparable from study to study. Specifically, we found relevant differences relating to the etiology of ACPE. The mortality rate in the control groups had a wide range (from 0% [15] to 64% [12]), indicating large differences in severity of illness between studies. In addition, the rates of AMI on admission, one of the most important predictors of mortality [4, 64, 68] varied from 0% in Bellone and colleagues [20] to 100% in Takeda and colleagues' study [12].
Some of the studies included had moderate methodological limitations. When analyzing the comparison between NPPV and SMT, some concern may be raised about study recruitment and randomization procedures. In fact, one study had significantly more patients with a history of AMI, COPD and diabetes mellitus and patients with higher baseline PaCO2 levels randomized to the control group [13]. Studies comparing CPAP with NPPV also had problems with baseline differences between groups. For instance, in Park and colleagues' study [15], patients treated with CPAP were more severely ill than those treated with NPPV, and in the study by Crane and colleagues [21], the NPPV group had significantly more co-morbidities, lower PaCO2 and a trend toward higher median peak creatine kinase (CK) levels. These differences could potentially account for the advantage of NPPV in reducing ETI in Park and colleagues' study [15] and for the advantage of CPAP in reducing mortality in Crane and colleagues' study [21].
Important heterogeneity was also found in relation with outcome definitions. The criteria and time frame used in the definition of patients needing ETI was very different from study to study. Moreover, some studies considered the need for intubation as the outcome whereas others considered actual intubation. The creation of consensus guidelines for outcome definitions for this type of study would be very useful to promote further rigorous research and would support future systematic reviewers.
Differences were also found in the technical specifications of the ventilation devices studied. Although face mask was the main interface used, in some studies [11, 12, 14, 25] a nasal mask or a combination of the two were applied. Duration of non-invasive ventilation and the type of ventilator may have also influenced outcomes, and this was not examined in this review. Some different kinds of interfaces and ventilatory modes have produced better patient comfort [69, 70], but they do not seem to have a major impact on survival or other outcomes. The differences relating to ventilators and interfaces among studies included in this meta-analysis do not seem to account for the differences in the results.
Finally, a search for potential publication bias was performed using funnel plots and the rank correlation test of Begg. Using these methods, it is not possible to rule out the hypothesis of publication bias in our meta-analysis. We found some evidence indicating that smaller studies are more likely to be published if they have larger effects and some evidence of a publication bias favoring the publication of studies with positive results for NPPV therapy when compared to CPAP. We should remember, though, that the rank correlation test of Begg has low power. It is also important to emphasize that the asymmetry found in funnel plots could be related to several other sources of bias, and is not necessarily evidence of publication bias.
Conclusion
The evidence for the advantage of non-invasive ventilation techniques, and especially of CPAP, over SMT is now robust, and its use as a first line intervention in ACPE patients is becoming mandatory. Although one recent guideline for the treatment of ACPE suggests CPAP to avoid ETI and mechanical ventilation [71], this technique is still underused in many clinical centers, partly because the clinical questions we address in this meta analysis had not been answered. Although both techniques, CPAP and NPPV, showed similar efficacy in decreasing need for ETI and mortality without increasing the risk of AMI, from a practical point of view CPAP has been shown to be cheaper and easier to use and implement in clinical practice [53], so it could be considered the preferred intervention in ACPE patients.
Finally, we think it is important for researchers in this field to create consensus guidelines over methods for reporting and defining population, interventions and outcome measures. Taking into account the evidence presented here, it does not seem advisable, from an ethical point of view, to pursue further research comparing non-invasive ventilation methods with SMT in ACPE patients. Research in the future should concentrate on the definition of subgroups of patients for whom NPPV could eventually have advantage over CPAP, the optimal levels of pressure when using NPPV and definition of the best time to start non-invasive ventilation.
Key messages
-
CPAP and NPPV have gained decisive roles in the management of various forms of respiratory failure, namely ACPE.
-
In this meta-analysis we show that, in ACPE patients, CPAP and NPPV both significantly decrease the need for ETI, and CPAP significantly reduces mortality when compared to SMT. The evidence is now robust, and the use of these techniques as a first line intervention in ACPE patients is becoming mandatory.
-
Although both techniques, CPAP and NPPV, showed similar efficacy in decreasing need for ETI and mortality, CPAP has been shown to be cheaper and easier to use and implement in clinical practice, so it could be considered the preferred intervention in ACPE patients.
-
Analysis of the safety of these methods showed that, although some caution is still advised, there is no evidence of increased risk of AMI with either of these techniques and other adverse events described are very rare.
-
No evidence supporting the suggested superiority of NPPV in hypercapnic ACPE patients was found and the advantage of higher levels of pressure support ventilation when using NPPV was not confirmed.
Abbreviations
- ACPE:
-
= acute cardiogenic pulmonary edema
- AMI:
-
= acute myocardial infarction
- CI:
-
= confidence interval
- COPD:
-
= chronic obstructive pulmonary disease
- CPAP:
-
= continuous positive airway pressure ventilation
- ETI:
-
= endotracheal intubation
- NPPV:
-
= non-invasive positive pressure ventilation
- RCT:
-
= randomized controlled trial
- SMT:
-
= standard medical therapy.
References
Jessup M, Brozena S: Heart Failure. N Engl J Med 2003, 348: 2007-18. 10.1056/NEJMra021498
American Heart Association: 2004 Heart and Stroke statistical update. Dallas, Texas: American Heart Association; 2004.
Fonarow G, ADHERE scientific advisory committee: The acute decompensated heart failure national registry (ADHERE): opportunities to improve care of patients hospitalized with acute decompensated heart failure. Rev Cardiovasc Med 2003,4(Suppl 7):S21-30.
Fedullo AJ, Swinburne AJ, Wahl GW, Bixby K: Acute cardiogenic pulmonary edema treated with mechanical ventilation. Factors determining in-hospital mortality. Chest 1991, 99: 1220-6.
Antonelli M, Pennisi MA, Montini L: Clinical review: Noninvasive ventilation in the clinical setting-experience from the past 10 years. Crit Care 2005, 9: 98-103. 10.1186/cc2933
Girou E, Brun-Buisson C, Taille S, Lemaire F, Brochard L: Secular trends in nosocomial infections and mortality associated with noninvasive ventilation in patients with exacerbation of COPD and pulmonary edema. JAMA 2003, 290: 2985-91. 10.1001/jama.290.22.2985
Antonelli M, Conti G, Rocco M, Bufi M, De Blasi RA, Vivino G, Gasparetto A, Meduri GU: A comparison of noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients with acute respiratory failure. N Engl J Med 1998, 339: 429-35. 10.1056/NEJM199808133390703
Vaisanen IT, Rasanen J: Continuous positive airway pressure and supplemental oxygen in the treatment of cardiogenic pulmonary edema. Chest 1987, 92: 481-5.
Hoffmann B, Welte T: The use of noninvasive pressure support ventilation for severe respiratory insufficiency due to pulmonary oedema. Intensive Care Med 1999, 25: 15-20. 10.1007/s001340050781
Pang D, Keenan SP, Cook DJ, Sibbald WJ: The effect of positive pressure airway support on mortality and the need for intubation in cardiogenic pulmonary edema: a systematic review. Chest 1998, 114: 1185-92.
Takeda S, Takano T, Ogawa R: The effect of nasal continuous positive airway pressure on plasma endothelin-1 concentrations in patients with severe cardiogenic pulmonary edema. Anesth Analg 1997, 84: 1091-6. 10.1097/00000539-199705000-00025
Takeda S, Nejima J, Takano T, Nakanishi K, Takayama M, Sakamoto A, Ogawa R: Effect of nasal continuous positive airway pressure on pulmonary edema complicating acute myocardial infarction. Jpn Circ J 1998, 62: 553-8. 10.1253/jcj.62.553
Masip J, Betbese AJ, Paez J, Vecilla F, Canizares R, Padro J, Paz MA, de Otero J, Ballus J: Non-invasive pressure support ventilation versus conventional oxygen therapy in acute cardiogenic pulmonary oedema: a randomised trial. Lancet 2000, 356: 2126-32. 10.1016/S0140-6736(00)03492-9
Levitt MA: A prospective, randomized trial of BiPAP in severe acute congestive heart failure. J Emerg Med 2001, 21: 363-9. 10.1016/S0736-4679(01)00385-7
Park M, Lorenzi-Filho G, MI Feltrim, PR Viecili, MC Sangean, M Volpe, Leite PF, Mansur AJ: Oxygen therapy, continuous positive airway pressure, or noninvasive bilevel positive pressure ventilation in the treatment of acute cardiogenic pulmonary edema. Arq Bras Cardiol 2001, 76: 221-30. 10.1590/S0066-782X2001000300005
Kelly CA, Newby DE, McDonagh TA, Mackay TW, Barr J, Boon NA, Dargie HJ, Douglas NJ: Randomised controlled trial of continuous positive airway pressure and standard oxygen therapy in acute pulmonary oedema; effects on plasma brain natriuretic peptide concentrations. Eur Heart J 2002, 23: 1379-86. 10.1053/euhj.2001.3156
Martin-Bermudez RJ, Rodriguez-Portal JA, Garcia-Garmendia JL, Garcia-Diaz E, Montano-Diaz M, Soto-Espinosa B, Murillo-Cabezas F, Muniz-Grijalvo O: Non-invasive ventilation in cardiogenic pulmonary edema. Preliminary results of a randomized trial. Intensive Care Med 2002, 28: S68. 10.1007/s00134-001-1157-6
Cross AM, Cameron P, Kierce M, Ragg M, Kelly AM: Non-invasive ventilation in acute respiratory failure: a randomised comparison of continuous positive airway pressure and bi-level positive airway pressure. Emerg Med J 2003, 20: 531-534. 10.1136/emj.20.6.531
Nava S, Carbone G, DiBattista N, Bellone A, Baiardi P, Cosentini R, Marenco M, Giostra F, Borasi G, Groff P: Noninvasive ventilation in cardiogenic pulmonary edema: a multicenter randomized trial. Am J Respir Crit Care Med 2003, 168: 1432-7. 10.1164/rccm.200211-1270OC
Bellone A, Monari A, Cortellaro F, Vettorello M, Arlati S, Coen D: Myocardial infarction rate in acute pulmonary edema: noninvasive pressure support ventilation versus continuous positive airway pressure. Crit Care Med 2004, 32: 1860-5. 10.1097/01.CCM.0000139694.47326.B6
Crane SD, Elliott MW, Gilligan P, Richards K, Gray AJ: Randomised controlled comparison of continuous positive airways pressure, bilevel non-invasive ventilation, and standard treatment in emergency department patients with acute cardiogenic pulmonary oedema. Emerg Med J 2004, 21: 155-61. 10.1136/emj.2003.005413
L'Her E, Duquesne F, Girou E, de Rosiere XD, Le Conte P, Renault S, Allamy JP, Boles JM: Noninvasive continuous positive airway pressure in elderly cardiogenic pulmonary edema patients. Intensive Care Med 2004, 30: 882-8. 10.1007/s00134-004-2183-y
Park M, Sangean MC, Volpe Mde S, Feltrim MI, Nozawa E, Leite PF, Passos Amato MB, Lorenzi-Filho G: Randomized, prospective trial of oxygen, continuous positive airway pressure, and bilevel positive airway pressure by face mask in acute cardiogenic pulmonary edema. Crit Care Med 2004, 32: 2407-15. 10.1097/01.CCM.0000147770.20400.10
Bellone A, Vettorello M, Monari A, Cortellaro F, Coen D: Noninvasive pressure support ventilation vs. continuous positive airway pressure in acute hypercapnic pulmonary edema. Intensive Care Med 2005, 31: 807-11. 10.1007/s00134-005-2649-6
Mehta S, Jay GD, Woolard RH, Hipona RA, Connolly EM, Cimini DM, Drinkwine JH, Hill NS: Randomized, prospective trial of bilevel versus continuous positive airway pressure in acute pulmonary edema. Crit Care Med 1997, 25: 620-8. 10.1097/00003246-199704000-00011
Masip J, Paez J, Betbese AJ, Vecilla F: Noninvasive ventilation for pulmonary edema in the emergency room. Am J Respir Crit Care Med 2004, 169: 1072.
Masip J, Roque M, Sanchez B, Fernandez R, Subirana M, Exposito JA: Noninvasive Ventilation in Acute Cardiogenic Pulmonary Edema-Systematic Review and Meta-analysis. JAMA 2005, 294: 3124-30. 10.1001/jama.294.24.3124
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF: Improving the quality of reports of meta-analysis of randomised controlled trials: The QUOROM statement. Lancet 1999, 354: 1896-1900. 10.1016/S0140-6736(99)04149-5
Ferrer M, Esquinas A, Leon M, Gonzalez G, Alarcon A, Torres A: Noninvasive ventilation in severe hypoxemic respiratory failure: a randomized trial. Am J Respir Crit Care Med 2003, 168: 1438-44. 10.1164/rccm.200301-072OC
Delclaux C, L'Her E, Alberti C, Mancebo J, Abroug F, Conti G, Guerin C, S F, Lefort Y, Antonelli M, et al.: Treatment of acute hypoxemic nonhypercapnic respiratory insufficiency with continuous airway pressure delivered by a face mask: a randomized controlled trial. JAMA 2000, 284: 2352-60. 10.1001/jama.284.18.2352
Antonelli M, Conti G, Bufi M, Costa MG, Lappa A, Rocco M, Gasparetto A, Meduri GU: Noninvasive ventilation for treatment of acute respiratory failure in patients undergoing solid organ transplantation: a randomized trial. JAMA 2000, 283: 235-41. 10.1001/jama.283.2.235
Wood KA, Lewis L, Von Harz B, Kollef MH: The use of noninvasive positive pressure ventilation in the emergency department: results of a randomized clinical trial. Chest 1998, 113: 1339-46.
Wysocki M, Tric L, Wolff MA, Millet H, Herman B: Noninvasive pressure support ventilation in patients with acute respiratory failure. A randomized comparison with conventional therapy. Chest 1995, 107: 761-8.
Schechtman E: Odds ratio, relative risk, absolute risk reduction, and the number needed to treat – which of these should we use? Value Health 2002, 5: 430-5. 10.1046/j.1524-4733.2002.55150.x
Walter SD: Choice of effect measure for epidemiological data. J Clin Epidemiol 2000, 53: 931-9. 10.1016/S0895-4356(00)00210-9
Begg CB, Mazumdar M: Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50: 1088-101.
Review Manager (RevMan) [Computer program]: Version 4.2 for Windows.Oxford, England: The Cochrane Collaboration; 2002. [http://www.cc-ims.net/RevMan]
RevMan Analyses [Computer program]: Version 1.0 for Windows.Oxford, England: The Cochrane Collaboration; 2002. [http://www.cc-ims.net/RevMan]
Craven RA, Singletary N, Bosken L, Sewell E, Payne M, Lipsey R: Use of bilevel positive airway pressure in out-of-hospital patients. Acad Emerg Med 2000, 7: 1065-8.
Sarullo FM, D'Alfonso G, Brusca I, De Michele P, Taormina A, Di Pasquale P, Castello A: Efficacy and safety of non-invasive positive pressure ventilation therapy in acute pulmonary edema. Monaldi Arch Chest Dis 2004,62(1):7-11.
Giacomini M, Iapichino G, Cigada M, Minuto A, Facchini R, Noto A, Assi E: Short-term noninvasive pressure support ventilation prevents ICU admittance in patients with acute cardiogenic pulmonary edema. Chest 2003, 123: 2057-61. 10.1378/chest.123.6.2057
Valipour A, Cozzarini W, Burghuber OC: Non-invasive pressure support ventilation in patients with respiratory failure due to severe acute cardiogenic pulmonary edema. Respiration 2004, 71: 144-51. 10.1159/000076675
Rusterholtz T, Kempf J, Berton C, Gayol S, Tournoud C, Zaehringer M, Jaeger A, Sauder P: Noninvasive pressure support ventilation (NIPSV) with face mask in patients with acute cardiogenic pulmonary edema (ACPE). Intensive Care Med 1999, 25: 21-8. 10.1007/s001340050782
Wigder HN, Hoffmann P, Mazzolini D, Stone A, Scholly S, Clark J: Pressure support noninvasive positive pressure ventilation treatment of acute cardiogenic pulmonary edema. Am J Emerg Med 2001, 19: 179-81. 10.1053/ajem.2001.21718
Baratz DM, Westbrook PR, Shah PK, Mohsenifar Z: Effect of nasal continuous positive airway pressure on cardiac output and oxygen delivery in patients with congestive heart failure. Chest 1992, 102: 1397-401.
Lenique F, Habis M, Lofaso F, Dubois-Rande JL, Harf A, Brochard L: Ventilatory and hemodynamic effects of continuous positive airway pressure in left heart failure. Am J Respir Crit Care Med 1997, 155: 500-5.
Kallio T, Kuisma M, Alaspaa A, Rosenberg PH: The use of prehospital continuous positive airway pressure treatment in presumed acute severe pulmonary edema. Prehosp Emerg Care 2003, 7: 209-13.
Thys F, Roeseler J, Reynaert M, Liistro G, Rodenstein DO: Noninvasive ventilation for acute respiratory failure: a prospective randomised placebo-controlled trial. Eur Respir J 2002, 20: 545-55. 10.1183/09031936.02.00287402
Yosefy C, Hay E, Ben-Barak A, Derazon H, Magen E, Reisin L, Scharf S: BiPAP ventilation as assistance for patients presenting with respiratory distress in the department of emergency medicine. Am J Respir Med 2003, 2: 343-7.
Mollica C, Brunetti G, Buscajoni M, Cecchini L, Maialetti E, Marazzi M, Principe R, Sabato R, Antonini VE: Non-invasive pressure support ventilation in acute hypoxemic (non hypercapnic) respiratory failure. Observations in Respiratory Intermediate Intensive Care Unit. Minerva Anestesiol 2001, 67: 107-15.
L'Her E, Moriconi M, Texier F, Bouquin V, Kaba L, Renault A, Garo B, Boles JM: Non-invasive continuous positive airway pressure in acute hypoxaemic respiratory failure-experience of an emergency department. Eur J Emerg Med 1998, 5: 313-8.
Bollaert PE, Sauder P, Girard F, Rusterholtz T, Feissel M, Harlay ML, Zaehringer M, Dusang B: Continuous positive airway pressure (CPAP) vs. Proportional Assist Ventilation (PAV) for noninvasive ventilation in cardiogenic pulmonary edema: a randomized study. Am J Respir Crit Care Med 2002,165(Suppl 8):A387.
Moritz F, Benichou J, Vanheste M, Richard JC, Line S, Hellot MF, Bonmarchand G, Muller JM: Boussignac continuous positive airway pressure device in the emergency care of acute cardiogenic pulmonary oedema: a randomized pilot study. Eur J Emerg Med 2003, 10: 204-8. 10.1097/00063110-200309000-00009
Chadda K, Annane D, Hart N, Gajdos P, Raphael JC, Lofaso F: Cardiac and respiratory effects of continuous positive airway pressure and noninvasive ventilation in acute cardiac pulmonary edema. Crit Care Med 2002, 30: 2457-61. 10.1097/00003246-200211000-00009
M Lin, HT Chiang: The efficacy of early continuous positive airway pressure therapy in patients with acute cardiogenic pulmonary edema. J Formos Med Assoc 1991, 90: 736-43.
Crane SD, Richards K, Gilligan P, Gray A, Elliott MW: Randomised controlled trial of non-invasive ventilation in acute cardiogenic pulmonary oedema (3PO study). Emerg Med J 2004,21(Suppl 38):155-161. 10.1136/emj.2003.005413
Lin M, Yang YF, Chiang HT, Chang MS, Chiang BN, Cheitlin MD: Reappraisal of continuous positive airway pressure therapy in acute cardiogenic pulmonary edema. Short-term results and long-term follow-up. Chest 1995, 107: 1379-86.
Hao CX, Luo XR, Liu YM: Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure by basal face mask. Acta Academiae Medicinae Jiangxi 2002, 42: 48-50.
Sharon A, Shpirer I, Kaluski E, Moshkovitz Y, Milovanov O, Polak R, Blatt A, A Simovitz, Shaham O, Faigenberg Z, et al.: High-dose intravenous isosorbide-dinitrate is safer and better than Bi-PAP ventilation combined with conventional treatment for severe pulmonary edema. J Am Coll Cardiol 2000, 36: 832-7. 10.1016/S0735-1097(00)00785-3
Brochard L: Noninvasive ventilation for Acute Respiratory Failure. JAMA 2002, 288: 932-5. 10.1001/jama.288.8.932
Liesching TN, Cromier K, Nelson D, Short K, Sucov A, Hill NS: Bilevel Noninvasive Ventilation vs Continuous Positive Airway Pressure to treat Acute Pulmonary Edema. Am J Respir Crit Care Med 2003, 167: A864.
Rasanen J, Heikkila J, Downs J, Nikki P, Vaisanen I, Viitanen A: Continuous positive airway pressure by face mask in acute cardiogenic pulmonary edema. Am J Cardiol 1985, 55: 296-300. 10.1016/0002-9149(85)90364-9
Bersten AD, Holt AW, Vedig AE, Skowronski GA, Baggoley CJ: Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face mask. N Engl J Med 1991, 325: 1825-30.
Adnet F, Le Toumelin P, Leberre A, Minadeo J, Lapostolle F, Plaisance P, Cupa M: In-hospital and long-term prognosis of elderly patients requiring endotracheal intubation for life-threatening presentation of cardiogenic pulmonary edema. Crit Care Med 2001, 29: 891-5. 10.1097/00003246-200104000-00042
Poulton PE: Left-sided heart failure with pulmonary edema:its treatment with the"pulmonary plus pressure machine". Lancet 1936, 2: 981-3. 10.1016/S0140-6736(00)47948-1
Holt AW, Bersten AD, Fuller S, Piper RK, Worthley LI, Vedig AE: Intensive care costing methodology: cost benefit analysis of mask continuous positive airway pressure for severe cardiogenic pulmonary oedema. Anaesth Intensive Care 1994, 22: 170-4.
Lightowler JV, Wedzicha JA, Elliott MW, Ram FS: Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ 2003, 326: 185. 10.1136/bmj.326.7382.185
Masip J, Paez J, Merino M, Parejo S, Vecilla F, Riera C, Rios A, Sabater J, Ballus J, Padro J: Risk factors for intubation as a guide for noninvasive ventilation in patients with severe acute cardiogenic pulmonary edema. Intensive Care Med 2003, 29: 1921-8. 10.1007/s00134-003-1922-9
Kwok H, McCormack J, Cece R, Houtchens J, Hill NS: Controlled trial of oronasal versus nasal mask ventilation in the treatment of acute respiratory failure. Crit Care Med 2003, 31: 468-73. 10.1097/01.CCM.0000045563.64187.20
Gay PC, Hess DR, Hill NS: Noninvasive proportional assist ventilation for acute respiratory insufficiency. Comparison with pressure support ventilation. Am J Respir Crit Care Med 2001, 164: 1606-11.
Nieminen MS, Bohm M, Cowie MR, Drexler H, Filippatos GS, Jondeau G, Hasin Y, Lopez-Sendon J, Mebazaa A: Executive summary of the guidelines on the diagnosis and treatment of acute heart failure: the Task Force on Acute Heart Failure of the European Society of Cardiology. Eur Heart J 2005, 26: 384-416. 10.1093/eurheartj/ehi044
Acknowledgements
We thank the precious help of Dr André Moreira in the search for references and the invaluable cooperation of Dr Martin-Bermudez, Dr Anthony Cross, Dr Marcelo Park and Dr Steven Crane for data not shown in their papers.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no conflicting interests.
Authors' contributions
JCW is responsible for initiation and direction of the review. LFA is responsible for study design, methods and statistical analysis. JCW and LFA selected studies and extracted data. JCW, LFA and AC-P interpreted results and wrote the manuscript. JCW and MA critically reviewed the manuscript for important intellectual content.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Winck, J.C., Azevedo, L.F., Costa-Pereira, A. et al. Efficacy and safety of non-invasive ventilation in the treatment of acute cardiogenic pulmonary edema – a systematic review and meta-analysis. Crit Care 10, R69 (2006). https://doi.org/10.1186/cc4905
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc4905