
Abstract
Introduction
We conducted the present study to determine whether a combination of the mechanical ventilation weaning predictors proposed by the collective Task Force of the American College of Chest Physicians (TF) and weaning endurance indices enhance prediction of weaning success.
Method
Conducted in a tertiary paediatric intensive care unit at a university hospital, this prospective study included 54 children receiving mechanical ventilation (≥6 hours) who underwent 57 episodes of weaning. We calculated the indices proposed by the TF (spontaneous respiratory rate, paediatric rapid shallow breathing, rapid shallow breathing occlusion pressure [ROP] and maximal inspiratory pressure during an occlusion test [Pimax]) and weaning endurance indices (pressure-time index, tension-time index obtained from P0.1 [TTI1] and from airway pressure [TTI2]) during spontaneous breathing. Performances of each TF index and combinations of them were calculated, and the best single index and combination were identified. Weaning endurance parameters (TTI1 and TTI2) were calculated and the best index was determined using a logistic regression model. Regression coefficients were estimated using the maximum likelihood ratio (LR) method. Hosmer–Lemeshow test was used to estimate goodness-of-fit of the model. An equation was constructed to predict weaning success. Finally, we calculated the performances of combinations of best TF indices and best endurance index.
Results
The best single TF index was ROP, the best TF combination was represented by the expression (0.66 × ROP) + (0.34 × Pimax), and the best endurance index was the TTI2, although their performance was poor. The best model resulting from the combination of these indices was defined by the following expression: (0.6 × ROP) – (0.1 × Pimax) + (0.5 × TTI2). This integrated index was a good weaning predictor (P < 0.01), with a LR+ of 6.4 and LR+/LR- ratio of 12.5. However, at a threshold value <1.3 it was only predictive of weaning success (LR- = 0.5).
Conclusion
The proposed combined index, incorporating endurance, was of modest value in predicting weaning outcome. This is the first report of the value of endurance parameters in predicting weaning success in children. Currently, clinical judgement associated with spontaneous breathing trials apparently remain superior.
Similar content being viewed by others

Introduction
Weaning (or discontinuation) from mechanical ventilation is definitive cessation of mechanical ventilation and differs from extubation, which is removal of the endotracheal tube [1, 2]. Determining the optimal time at which to discontinue mechanical ventilation must not be based simply on clinical impression because weaning depends on multiple factors [2, 3]: central drive and peripheral nerves; mechanical respiratory loads, ventilatory muscle properties and gas exchange properties; and cardiac tolerance and peripheral oxygen demands. Premature weaning places the patient at risk for reintubation and airway trauma, whereas delayed weaning exposes them to risk for nosocomial infection and increases hospitalization costs. Indeed, 'the complexity of the decision to extubate provides a strong rationale for developing accurate predictors of extubation outcome' [3].
Extensive efforts have been made to identify predictors of successful weaning in adults [4, 5] as well as in children [6–25]. The following indices were proposed by the Collective Task Force of the American College of Chest Physicians (TF) as the most promising weaning predictors [5]: spontaneous respiratory rate, paediatric rapid shallow breathing (RSB) [13], RSB occlusion pressure (ROP) [26] and maximal inspiratory pressure during an occlusion test (Pimax) [23, 27]. Although none of these predictors appears to be sufficiently sensitive or specific in predicting weaning success, paediatric studies have used integrated indices, including respiratory drive, respiratory load, muscle strength and quality of gas exchange.
Fatigue (for example, diminution of endurance) of the inspiratory muscles is defined as reduction in capacity to develop force and/or velocity of a muscle, which results from muscle activity under load and is reversible with rest [2, 28–30]. The two reference techniques for assessing endurance (for example, detecting fatigue) are analysis of the change in the electromyographic power spectrum and in the force response of muscles to electrical stimulation [2]. Another approach uses the tension-time index (TTI) of the diaphragm, calculated from the mean transdiaphragmatic pressure, which correlates well with reference techniques. However, because determination of transdiaphragmatic pressure is invasive, noninvasive TTI estimated from the measurement of mouth occlusion pressure (P0.1) and from the integral of the airway pressure curve over time during spontaneous ventilation were used as predictors of weaning success [2]. Finally, Jabour and coworkers evaluated ventilatory endurance using a modified TTI, namely the pressure-time index (PTI), which was calculated from peak airway pressure during mechanical ventilation [28].
Respiratory muscle endurance, which has been reported to have particular significance in predicting weaning success in adults [28–30], has never been investigated in children. Thus, the aims of the present prospective study were as follows: to evaluate the ability of indices proposed by the TF [5] and endurance indices to predict weaning outcome; and to determine whether a combined index, including the most accurate TF and endurance indices, could enhance the ability to predict weaning success.
Materials and methods
This prospective study was approved by the local hospital institutional review board, and parents provided informed consent before the study began. All children admitted to the paediatric intensive care unit at our university-affiliated hospital from March 1999 to July 2001, and who required mechanical ventilation for more than 6 hours were eligible for inclusion in the study. Children with chronic neuromuscular disease, who had undergone tracheostomy, or who were aged under 30 days were excluded. The primary physician was responsible for the weaning decision and process, and was blinded to the results of the measurements performed during the short period of spontaneous breathing (see below). All ventilatory variables were collected by the same investigator, and the weaning procedures were not delayed in his absence (for example nights and weekends); those patients who did undergo weaning procedures in his absence were excluded from the study.
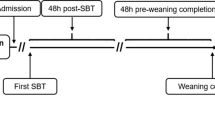
Patients were enrolled in the study if they met all the following criteria, as defined for adults by the French Society of Critical Care Consensus Conference [31]: improvement or resolution of the underlying cause of acute respiratory failure; core temperature <38.5°C; satisfactory renal function; no signs of infection; neuropsychological state compatible with autonomous breathing; correction of electrolyte disorders; a haemoglobin level above 9 g/dl; absence of left ventricular dysfunction or cardiac arrhythmia; no sedation or mild sedation (for example, midazolam <0.5 μg/kg per minute, morphine sulphate <1 mg/kg per day, or fentanyl citrate <0.25 μg/kg per hour); efficient cough; and adequate gas exchange. Moreover, all of the patients were weaned using pressure support ventilation (PSV) on Servo 300 or Servo 900C ventilators (Siemens-Elema, Solna, Sweden), with a pressure support below 15 cmH2O, a positive end-expiratory pressure below 5 cmH2O and fractional inspired oxygen (FiO2) below 40% [31]. After the patient's primary physician made the decision to wean, the patient's respiratory variables were recorded by the investigator, first during mechanical ventilation and then during a short period of spontaneous breathing. Then, the children underwent a spontaneous breathing trial (SBT) through a T-piece circuit or Canopy device for 30 minutes [32]. Then, children were extubated, depending on their clinical status and blood gas determination [31]. Patients who failed SBT were excluded. Weaning failure was defined as reinstitution of invasive or noninvasive mechanical ventilation within 48 hours of extubation, for a reason than upper airway obstruction.
Measurements
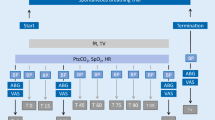
Demographic data collected included age, weight, sex, admission diagnosis, Paediatric Risk of Mortality (PRISM) score calculated during a 24-hour period of observation, tube internal diameter and duration of ventilation. Ventilator settings, recorded when the child was under PSV, included ventilator rate (for example, respiratory rate [RR]PSV), peak inspiratory pressure, positive end-expiratory pressure, mean airway pressure, tidal volume (VT) and FiO2. Then, during a short period of spontaneous breathing, respiratory parameters were measured using a calibrated Fleish no. 0 pneumotachograph (MSR, Paris, France) connected to a ± 2 cmH2O differential pressure transducer (Validyne, Northridge, CA, USA) over 15–30 consecutive breaths. Measured parameters included spontaneous respiratory rate (RRs), spontaneous VT (for example, VTs), inspiratory time (Ti) and total respiratory cycle time (Ttot). Pimax was measured by occluding the airway for a least 20 s using a unidirectional valve system (LSA, Paris, France) that allowed expiration but not inspiration, and a ± 50 cmH2O differential pressure transducer (Validyne). Initial inspiratory pressure was measured as the negative pressure deflection produced by the first inspiration attempt, whereas Pimax was taken as the most negative deflection produced by any inspiration attempt during airway occlusion [9, 23, 27]. Negative pressure 0.1 s after airway occlusion (P0.1) was measured by occluding the airways at the end-expiratory level, with a vibration- and noise-free pneumatic valve (Hans-Rudolph, Kansas City, KS, USA) [8, 33].
Measurements were performed by the same investigator and were repeated three times; mean values were used for data analysis. Between each occlusion trial, sufficient time was allowed to ensure that the patient's arterial oxygen saturation and heart rate had returned to their previous baseline values. VTs and VTPSV were corrected for body weight.
Respiratory parameters calculated included duration of mechanical ventilation, arterial oxygen tension/FiO2 ratio [34, 35], paediatric RSB [13], PTI [28, 36], ROP [26], TTI obtained from P0.1 (TTI1) [37, 38] and TTI obtained from mean airway pressure (TTI2) [39]. Formulae are summarized in Table 1. Age-adjusted RR was calculated using a Z score [14, 19, 20, 40] and used for paediatric RSB and ROP calculations. Adjustment to age was done for P0.1 and age-adjusted values were used for TTI and ROP calculations [41].
Statistical analysis
The distribution of data was expressed as medians with 25th and 75th percentile ranges (Q1–Q3). Comparison of continuous variables between the two outcome groups (weaning success and weaning failure) was done using Kruskal-Wallis test. A χ2 test or Fisher's exact test, when expected number was less than 3, were used for comparison of categorical variables between two groups. All if the indices, including RR and P0.1, were studied before and after age adjustment.
Sensitivity, specificity, positive predictive values and negative predictive values (NPVs) were calculated using standard formulae. A true positive/negative result was defined as occurring when a test predicted weaning success/failure and weaning actually succeeded/failed. A false-positive result occurred when a test predicted success but weaning failed, and a false-negative result was when a test predicted weaning failure but weaning succeeded [34, 35]. General performance of each index was assessed using positive and negative likelihood ratios (LR+ and LR-, respectively) [2, 42–45], calculated for each index [46] after discretization in dichotomous variables. An index could be predictive (LR+ >2, LR- <0.5, or LR+/LR- ratio >4), well predictive (LR+ >5, LR- <0.2, or LR+/LR- ratio >10), or very well predictive (LR+ >10, LR- <0.1, or LR+/LR- ratio >100) [4, 42, 43].
The performances of each individual TF index and combinations of them were calculated, and the best performers were identified from among the individual TF indices and TF combinations. In the same manner, the performances of reported weaning indices, including endurance parameters (TTI1 and TTI2), were calculated and the best endurance index was identified. All variables significant at the P < 0.20 level in the univariate analysis were included in a stepwise logistic regression model using a P-to-remove at 0.05. Regression coefficients were estimated using the maximum likelihood method. The Hosmer–Lemeshow test was used to estimate goodness-of-fit of the model [47]. A final equation was constructed to predict weaning success. Finally, the performance of combinations of best TF indices and best endurance index was calculated.
Area under the receiver operating characteristic curves (AUC) was calculated using the nonparametric method proposed by Hanley and McNeil [48], and the 95% confidence interval was calculated using the Wilcoxon test. Results could be considered uninformative (AUC = 0.5), poorly accurate (0.5 < AUC = 0.7), moderately accurate (0.7 < AUC = 0.9), highly accurate (0.9 < AUC = 1), or perfect (AUC = 1) [49, 50]. P < 0.05 was considered statistically significant. In summary, the AUC, Hosmer–emeshow goodness-of-fit test, LR test, and well predicted outcome percentages were used to evaluate predictive accuracy.
Results
Of the 220 patients who were eligible for inclusion in the study, 56 patients were enrolled (25%) and underwent 59 episodes of weaning (median age 29 [11–94] months, median weight 13 [9–23] kg). The median duration of ventilation was 4 (2–9) days, and 39 patients received mild sedation during the weaning procedure. Two patients who did not tolerate SBT were excluded. Of the remaining 54 children, 17 patients had neurologic disorders (30%), 28 had respiratory failure (49%), three had both neurologic disorders and respiratory failure (5%) and nine underwent surgery (16%). Of the remaining 57 episodes of weaning (in the 54 children), 45 attempts were successful (80%) and 12 were unsuccessful (20%; Table 2). The causes of reintubation were respiratory failure (n = 6; one child with spinal amyotrophy, one with myopathy and one with mucopolysaccharidosis), pulmonary oedema of cardiac origin (n = 3), bronchial obstruction (n = 2; 1 burned child) and atelectasis (n = 1). Three of the 12 patients who failed weaning needed noninvasive ventilation within 48 hours after extubation (20%) and nine required reintubation and mechanical ventilation for a reason other than upper airway obstruction (80%). Two patients who were successfully extubated required reintubation for severe upper airway obstruction (4%). Age, sex, weight, PRISM score, duration of ventilation and internal tube diameter were not statistically different between the weaning success and weaning failure groups (Table 3). Also, diagnoses were not statistically different between the groups. Finally, ventilator settings and spontaneous breathing parameters at the beginning of the weaning procedure were not significantly different between the two groups (Table 4).
The best single TF index was ROP, the best combination of TF indices was represented by the expression (0.66 × ROP) + (0.34 × Pimax), and the best endurance index was the TTI2. However, their performance was statistically poor (Table 5). The best model resulting from the combination of these indices was defined by the expression: (0.6 × ROP) – (0.1 × Pimax) + (0.5 × TTI2). This integrated index fitted the data well (P = 0.364, Hosmer–Lemeshow test) and was a good weaning predictor (P < 0.01, Kruskal-Wallis test). The threshold value that best discriminated between two groups was 1.3, with a value <1.3 predicting weaning success (P = 0.007, Fisher test). Although LR+ was 6.4 and the LR+/LR- ratio was greater than 10, LR- remained above 0.2, meaning that this integrated index was only predictive of weaning success.
Discussion
In a population of 54 critically ill children, we found that the indices proposed by the TF were insufficient in predicting weaning outcome. Among the combined indices, including endurance in order to enhance prediction of weaning outcome, the best combination was defined by the expression: (0.6 × ROP) – (0.1 × Pimax) + (0.5 × TTI2). However, this index was not a valuable predictor of weaning outcome because it only predicted weaning success.
The best combination of TF indices included ROP and Pimax. Although Pimax was considered by the TF [5] to be one of the most promising weaning predictors in adults (based on LR+ and LR-), no data concerning LRs were available for ROP in the adult or paediatric literature [26]. In the present study ROP alone was only predictive of weaning success, and this finding is in agreement with that obtained in a population of 45 adult patients by Sassoon and Mahutte [26], who found that ROP may be useful and more accurate in predicting weaning outcome when ROP components (P0.1 and RSB) alone were indeterminate [26]. The AUC (0.80 ± 0.9) and LRs (LR+ 2.42, LR- 0.05, and LR+/LR- 48), recalculated from their published data, appear to be better than those in our study. Pimax, which is considered a global index of respiratory muscle strength [35, 38, 51, 52] and was adapted to children by El-Khatib and coworkers [23], was evaluated in five paediatric studies [6, 8–10, 12], but LRs were calculated in only one study designed to predict weaning failure [12]. The LRs were recalculated to predict weaning success, and the results (LR+ 1.09, LR-0.35, and LR+/LR-3.11) appeared similar to those obtained in the present study (Tables 5 and 6) and in five adult studies [5]. AUC values obtained in the five paediatric studies were similar to those in our study and ranged from 0.53 (95% confidence interval 0.47–0.67) [8] to 0.57 (95% confidence interval 0.47–0.67) [12]. However, in a recent adult study that included 52 patients [50], Pimax was a good weaning predictor (LR+ 1.40, LR- 0.12, and LR+/LR- 11.67).
In our study, TTI2 was found to be the best endurance index, although it was not very predictive of weaning success (Table 5). Numerous studies indicate that duration of inspiration relative to the duration of the total respiratory cycle (for example, Ti/Ttot ratio) should be an important determinant of diaphragmatic fatigue [35, 53–55]. Hence, any increase of indices that include Ti/Ttot ratio such as PTI [28, 36], TTI1 [37, 38] and TTI2 [39] could reflect decreased endurance. In adults, Ramonaxto and coworkers [56] reported that TTI2 highly correlated with TTI of the diaphragm, which was proposed by Bellemare and Grassino [54, 55] for quantifying the magnitude and duration of respiratory muscle contraction. However, TTI2 has never been used as a predictor of weaning outcome either in adults or children, whereas TTI1 and PTI appeared to be useful predictors of weaning outcome in adults [28, 56].
Several adult and paediatric studies [7, 9, 13–15] have attempted to define integrated weaning indices that include parameters in relation to respiratory muscle function, such as respiratory drive, respiratory load and muscle strength [35, 53, 57], but none of these integrated indices was found to be predictive of weaning outcome. Respiratory muscle endurance has not been investigated in paediatric patients; however, the diaphragm is less endurant in children than in adults because of anatomic and physiologic differences [58]. Furthermore, in adults respiratory muscle endurance was reported to be of particular significance in predicting weaning outcome [28–30]. Taking respiratory muscle endurance into account should improve prediction of weaning success. In the present study TTI2 was found to contribute strongly to the integrated index, and its association with ROP and Pimax improved LR+, LR- and LR+/LR- ratio.
Comparing the performance of weaning indices is difficult because few studies have calculated LRs, which are considered as the best tests [4]. Indeed, only one paediatric study calculated LRs [12], and most other paediatric studies did not report the number of true-positive and false-positive findings. Furthermore, large discrepancies exist in the literature regarding population characteristics, the definition of weaning and extubation [59], inclusion and exclusion criteria (for example aetiology of respiratory failure and duration of ventilation), the definition of weaning success and weaning failure, and the use (or not) of noninvasive mechanical ventilation after extubation [16, 23].
Three factors may explain why integrated indices do not improve upon the accuracy of prediction of weaning outcome of single indices. First, most paediatric studies included small numbers of patients with a relative low rate of weaning failure, and it has been demonstrated that a large sample including more than 1,000 patients with at least 100 extubation (or weaning) failures would be necessary to assess adequately the ability of parameters to predict extubation (or weaning) success in children [60]. Second, weaning indices are often measured too late, when patients meet all of the clinical criteria for weaning, and so threshold values are not very discriminatory [5]. Third, SBT is considered to be the most direct and simplest way to assess patient performance without ventilator support [2], and so a failed SBT is synonymous of weaning failure. Thus, the number of false-negative findings (for example, patients who failed SBT but who could have been weaned) is unknown, and the specificity, NPV and LR- of SBT cannot be determined [2]. Among 105 extubations in adults considered to be false negative because of a pre-extubation respiratory rate above 30 breaths/minute, DeHaven and coworkers [17] observed that 97 were successful. Furthermore, Epstein and coworkers [3] noted that 30–70% of unplanned extubation in adult patients did not result in reintubation.
Weaning is usually delayed by clinicians [3], and a weaning index should be more predictive of weaning failure (for example, it should be more specific, and have a good NPV and a lower LR-). Thus far, all paediatric studies of weaning indices, which determined their sensitivity, specificity, LRs, or AUCs, included a SBT. As long as a SBT is defined as a necessary pre-condition for extubation by the TF [2], comparisons between SBT and weaning indices will be limited because of the underestimation of false-negative findings and NPV.
Our study has two other limitations. First, there was no defined protocol for decreasing mechanical ventilation, although there is no evidence that such a protocol must be used in children [4, 61]. Moreover, we employed no set protocol for decreasing sedation, which is supposed to improve weaning success in children [59]. Second, during the study period 220 patients were eligible according to the inclusion criteria, but only 27% of these were included. Like the study conducted by Thiagarajan and coworkers [14], in which 227 children from among 472 admitted to their paediatric intensive care unit (48%) were included, our study design required the presence onsite of the investigator in charge of data collection in order to decrease variability in measurement of the different parameters and to guarantee that the patient's physician remained blinded to the results.
The weaning failure rate was 20%, which is similar to that reported by others in paediatric patients, ranging from 1.4% [62] to 34% [12]. The median PRISM value, calculated within 24 hours of admission, was close to that reported in most previous paediatric studies [11, 12, 16, 63], although PRISM values were found to be lower in two studies [62, 64].
Conclusion
In our population of 54 critically ill children, indices proposed by the TF were insufficient in predicting weaning outcome. The best combined index, incorporating endurance, was defined by the expression: (0.6 × ROP) – (0.1 × Pimax) + (0.5 × TTI2). This is the first report of the value of endurance parameters in predicting weaning success in children. The index had a LR+ of 6.4 and a LR+/LR- ratio above 10; however, at a threshold value <1.3 it was only predictive of weaning success (LR- >0.2). Although this index cannot be considered sufficient for making decisions regarding weaning, the reason for this is probably that it was measured, like in other studies, when children met all clinical criteria for weaning. At the present time, clinical judgement associated with SBT still seems superior in the weaning process in children.
Key messages
-
Determining the optimal time to discontinue mechanical ventilation is important, because premature weaning places the patient at risk for reintubation and delayed weaning exposes the patient to risk for nosocomial infection.
-
The indices proposed by the TF are not sufficiently sensitive or specific in predicting weaning outcome.
-
Until now, indices that reflect respiratory muscle endurance have not been investigated in children.
-
Our best index, combining ROP, Pimax and TTI2, was only predictive of weaning success.
-
Such indices are unable to assist with decisions regarding weaning probably because they are measured when patients meet all clinical criteria for weaning.
Abbreviations
- AUC:
-
area under the curve
- FiO2:
-
fractional inspired oxygen
- LR:
-
likelihood ratio
- NPV:
-
negative predictive value
- Pimax:
-
maximal inspiratory pressure during an occlusion test
- PRISM:
-
Paediatric Risk of Mortality Score
- PSV:
-
pressure support ventilation
- PTI:
-
pressure-time index
- ROP :
-
RSB occlusion pressure
- RR:
-
respiratory rate
- RSB:
-
rapid shallow breathing
- SBT:
-
spontaneous breathing trial
- TF:
-
Task Force of the American College of Chest Physicians
- Ti:
-
inspiratory time
- TTI:
-
tension-time index
- Ttot:
-
total respiratory cycle time.
References
Richard C, Beydon L, Cantagrel S, Cuvelier A, Fauroux B, Garo B, Holzapfel L, Lesieur O, Levraut J, Maury E, et al.: [21st Consensus Conference on Intensive Care and Emergency Medicine: mechanical ventilation weaning]. Réanimation 2001, 10: 699-705. 10.1016/S1624-0693(01)00199-2
McIntyre NR, Cook DJ, Ely EW, Epstein S, Fink JB, Heffner JE, Hess D, Hubmayer RD, Scheinhorn DJ: Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians, the American Association for Respiratory Care, and the American College of Critical Care Medicine. Chest 2001, 375S-395S. 10.1378/chest.120.6_suppl.375S
Epstein SK: Decision to extubate. Intensive Care Med 2002, 28: 535-546. 10.1007/s00134-002-1268-8
Meade MO, Ely EW: Protocols to improve the care of critically ill pediatric and adult patients. JAMA 2002, 288: 2601-2603. 10.1001/jama.288.20.2601
Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, Mancebo J, Esteban A, Epstein S: Predicting success in weaning from mechanical ventilation. Chest 2001, 400S-424S. 10.1378/chest.120.6_suppl.400S
Khan N, Brown A, Venkataraman ST: Predictors of extubation success and failure in mechanically ventilated infants and children. Crit Care Med 1996, 24: 1568-1579. 10.1097/00003246-199609000-00023
Manczur TI, Greenough A, Pryor D, Rafferty GF: Comparison of predictors of extubation from mechanical ventilation in children. Pediatr Crit Care Med 2000, 1: 28-32. 10.1097/00130478-200007000-00005
Manczur TI, Greenough A, Pryor D, Rafferty GF: Assessment of respiratory drive and muscle function in the pediatric intensive care unit and prediction of extubation failure. Pediatr Crit Care Med 2000, 1: 124-126. 10.1097/00130478-200010000-00006
Venkataraman ST, Kahn N, Brown A: Validation of predictors of extubation success and failure in mechanically ventilated infants and children. Crit Care Med 2000, 28: 2991-2996. 10.1097/00003246-200008000-00051
Farias JA, Alia I, Esteban A, Golubicki AN, Olazarri FA: Weaning from mechanical ventilation in pediatric intensive care patients. Intensive Care Med 1998, 24: 1070-1075. 10.1007/s001340050718
Farias JA, Retta A, Alia I, Olazarri F, Esteban A, Golubicki A, Allende D, Maliarchuk O, Peltzer C, Ratto ME, et al.: A comparison of two methods to perform a breathing trial before extubation in pediatric intensive care patients. Intensive Care Med 2001, 27: 1649-1654. 10.1007/s001340101035
Farias JA, Alia I, Retta A, Olazarri F, Fernandez A, Esteban A, Palacios K, Di Nunzio L, Fernandez G, Bordon A, et al.: An evaluation of extubation failure predictors in mechanically ventilated infants and children. Intensive Care Med 2002, 28: 752-757. 10.1007/s00134-002-1306-6
Baumeister BL, El-Khatib M, Smith PG, Blumer JL: Evaluation of predictors of weaning from mechanical ventilation in pediatric patients. Pediatr Pulmonol 1997, 24: 344-352. 10.1002/(SICI)1099-0496(199711)24:5<344::AID-PPUL7>3.0.CO;2-I
Thiagarajan RR, Bratton SL, Martin LD, Brogan TV, Taylor D: Predictors of successful extubation in children. Am J Respir Crit Care Med 1999, 160: 1562-1566.
Hubble CL, Gentile MA, Tripp DS, Craig DM, Meliones JM, Cheifetz IM: Deadspace to tidal volume ratio predicts successful extubation in infants and children. Crit Care Med 2000, 28: 2034-2040. 10.1097/00003246-200006000-00059
Leclerc F, Lecine T, Riou Y, Grandbastien B, Noizet O, Dorkenoo A, Leteurtre S, Neve V, Sadik A, Cremer R: Multi-parameter indices of weaning from mechanical ventilation in children [in French]. Rev Mal Respir 2002, 19: 53-61.
De Haven CB, Kirton OC, Morgan JP, Hart AM, Shatz DV, Civetta JM: Breathing measurement reduces false-negative classification of tachypneic preextubation trial failures. Crit Care Med 1996, 24: 976-980. 10.1097/00003246-199606000-00017
Del Rosario N, Sassoon CS, Chetty KG, Gruer SE, Mahutte CK: Breathing pattern during acute respiratory failure and recovery. Eur Respir J 1997, 10: 2560-2565. 10.1183/09031936.97.10112560
Dibley MJ, Goldsby JB, Staehling NW, Trowbridge FL: Development of normalized curves for the international growth reference: historical and technical considerations. Am J Clin Nutr 1987, 46: 736-748.
Dibley MJ, Staehling N, Nieburg P, Trowbridge FL: Interpretation of Z-score anthropometric indicators derived from the international growth reference. Am J Clin Nutr 1987, 46: 749-762.
Dojat M, Harf A, Touchard D, Laforest M, Lemaire F, Brochard L: Evaluation of a knowledge-based system providing ventilatory management and decision for extubation. Am J Respir Crit Care Med 1996, 153: 997-1004.
Edmunds S, Weiss I, Harrison R: Extubation failure in a large pediatric ICU population. Chest 2001, 119: 897-900. 10.1378/chest.119.3.897
El-Khatib MF, Baumeister B, Smith PG, Chatburn RL, Blumer JL: Inspiratory pressure/maximal inspiratory pressure: does it predict successful extubation in critically ill infants and children? Intensive Care Med 1996, 22: 264-268. 10.1007/BF01712248
Ely EW, Meade O, Haponik EF, Kollef MH, Cook DJ, Guyatt GH, Stoller JK: Mechanical ventilator weaning protocols driven by nonphysician health-care professionals: evidence-based clinical practice guidelines. Chest 2001, 454S-463S. 10.1378/chest.120.6_suppl.454S
Epstein SK, Nevins ML, Chung J: Effect of unplanned extubation on outcome of mechanical ventilation. Am J Respir Crit Care Med 2000, 161: 1912-1916.
Sassoon CS, Mahutte CK: Airway occlusion pressure and breathing pattern as predictors of weaning outcome. Am Rev Respir Dis 1993, 148: 860-866.
Marini JJ, Smith TC, Lamb V: Estimation of inspiratory muscle strength in mechanically ventilated patients: the measurement of maximal inspiratory pressure. J Crit Care 1986, 1: 32-38.
Jabour ER, Rabil DM, Truwit JD, Rochester DF: Evaluation of a new weaning index based on ventilatory endurance and the efficiency of gas exchange. Am Rev Respir Dis 1991, 144: 531-537.
Gandia F, Blanco J: Evaluation of indexes predicting the outcome of ventilator weaning and value of adding supplemental inspiratory load. Intensive Care Med 1992, 18: 327-333. 10.1007/BF01694360
Roussos CS, Macklem PT: Diaphragmatic fatigue in man. J Appl Physiol 1982, 53: 1190-1206. 10.1063/1.330569
Gibert C, Bourgain JL, Brunet F, Derenne JP, Daoudal P, Manier G: [Weaning from mechanical ventilation in adults]. Rean Urg 1992, 1: 159-167.
Esteban A, Alia I, Gordo F, Fernandez R, Solsona JF, Vallverdu I, Macias S, Allegue JM, Blanco J, Carriedo D, Leon M, et al.: Extubation outcome after spontaneous breathing trial with T-tube or pressure support ventilation. Am J Respir Crit Care Med 1997, 156: 459-465.
Sassoon CS, Te TT, Mahutte CK, Light RW: Airway occlusion pressure: an important indicator for successful weaning in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis 1987, 135: 107-113.
Yang KL, Tobin MJ: A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. NEJM 1991, 324: 1445-1450.
Tobin MJ, Alex CG: Discontinuation of mechanical ventilation. In Principles and Practice of Mechanical Ventilation. Edited by: Tobin MJ. New York: MacGraw-Hill; 1994:1177-1206.
Morganroth ML, Morganroth JL, Nett LM, Petty TL: Criteria for weaning prolonged mechanical ventilation. Arch Intern Med 1984, 144: 112-116. 10.1001/archinte.144.5.1012
Gaultier C: Tension-time index of inspiratory muscles in children. Pediatr Pulmonol 1997, 23: 327-329. 10.1002/(SICI)1099-0496(199705)23:5<327::AID-PPUL3>3.0.CO;2-H
Gaultier C, Boule M, Tournier G, Girard F: Inspiratory force reserve of the respiratory muscles in children with chronic obstructive pulmonary disease. Am Rev Respir Dis 1985, 131: 811-815.
Vassilakopoulos T, Zakynthinos S, Roussos C: The tension-time index and the frequency/tidal volume ratio are the major pathophysiologic determinants of weaning failure and success. Am J Respir Crit Care Med 1998, 158: 378-385.
Iliff A, Lee VA: Pulse rate, respiratory rate, and body temperature of children between two months and eighteen years of age. Child Dev 1952, 23: 237-245.
Gaultier C, Perret L, Boule M, Buvry A, Girard F: Occlusion pressure and breathing pattern in healthy children. Respir Physiol 1981, 46: 71-80. 10.1016/0034-5687(81)90069-4
Jaeschke R, Guyatt GH, Sackett DL, for the Evidence-Based Medicine Working Group: Users' guides to medical literature: how to use an article about a diagnostic test, are the results of the study valid? JAMA 1994, 271: 389-391. 10.1001/jama.271.5.389
Jaeschke R, Guyatt GH, Sackett DL, for the Evidence-Based Medicine Working Group: Users' guides to medical literature: how to use an article about a diagnostic test, what are the results and will help me in caring for my patients? JAMA 1994, 271: 703-708. 10.1001/jama.271.9.703
Sackett DL, Strauss SE, Richardson WS, Rosenberg W, Hayes RB: Asking answerable clinical questions. In Evidence-based Medicine. How to Practice and Teach EBM. 2nd edition. New York: Churchill Livingstone; 2000:13-27.
Halkin A, Reichman M, Schwaber O, Paltiel O, Brezis M: Likelihood ratios: getting diagnostic testing into perspective. QJM 1998, 91: 247-258. 10.1093/qjmed/91.4.247
Pauker SG, Kassirer JP: The thresholds approach to clinical making decision. N Engl J Med 1980, 302: 1109-1117.
Hosmer DW, Lemeshow S: Confidence interval estimates of an index of quality performance based on logistic regression model. Stat Med 1995, 14: 2161-2172.
Hanley JA, McNiel BJ: The meaning and use of the area under a receiver-operating characteristics curve. Radiology 1982, 143: 29-36.
Swets JA: Measuring the accuracy of diagnostic systems. Science 1988, 240: 1285-1293.
Conti G, Montini L, Pennisi MA, Cavaliere F, Arcangeli A, Bocci MG, Proietti R, Antonelli M: A prospective, blinded evaluation of indexes proposed to predict weaning from mechanical ventilation. Intensive Care Med 2004, 30: 830-836. 10.1007/s00134-004-2230-8
Wagener JS, Hibbert ME, Landau LI: respiratory pressures in children. Am Rev Respir Dis 1984, 129: 873-875.
Wilson SH, Cook NT, Edwards RH, Spiro SG: Predicted normal values for maximal respiratory pressures in caucasian adults and children. Thorax 1984, 39: 535-538.
Laghi F, Tobin MJ: Disorders of the respiratory muscles. Am J Respir Crit Care Med 2003, 168: 10-48. 10.1164/rccm.2206020
Bellemare F, Grassino A: Effect of pressure and timing of contraction on human diaphragm fatigue. J Appl Physiol 1982, 53: 1190-1195. 10.1063/1.330569
Bellemare F, Grassino A: Force reserve of the diaphragm in patients with chronic obstructive pulmonary disease. J Appl Physiol 1983, 55: 8-15.
Ramonaxto M, Boulard Ph, Prefaut C: Validation of a non-invasive tension-time index of inspiratory muscles. J Appl Physiol 1995, 78: 646-653.
Manthous CA, Schmidt GA, Hall JB: Liberation from mechanical ventilation: a decade of progress. Chest 1998, 114: 886-901.
Stocks J: Respiratory physiology during early life. Monaldi Arch Chest Dis 1999, 54: 358-364.
Khamiees M, Raj P, DeGirolamo A, Amoateng-Adjepong Y, Manthous Y: Predictors of extubation outcome in patients who ave successfully completed a spontaneous breathing trial. Chest 2001, 120: 1262-1270. 10.1378/chest.120.4.1262
Randolph A: Weaning from mechanical ventilation. New Horizons 1999, 7: 374-85.
Randolph AG, Wypij D, Venkataraman ST, Hanson JH, Gedeit RG, Meert KL, Luckett PM, Forbes P, Lilley M, Thompson J, Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network, et al.: Effect of mechanical ventilator weaning protocols on respiratory outcomes in infants and children: a randomized controlled trial. JAMA 2002, 288: 2561-2568. 10.1001/jama.288.20.2561
Restrepo RD, Fortenberry JD, Spainhour C, Stockwemm J, Goodfellow LT: Protocol-driven ventilator management in children: comparison to nonprotocol care. J Intensive Care Med 2004, 19: 274-284. 10.1177/0885066604267646
Randolph A, Meert KL, O'Neil ME, Hanson JH, Luckett PM, Arnold JH, Gedeit RG, Cox PN, Roberts JS, Venkataraman ST, et al.: The feasability of conducting clinical trials in infants and children with acute respiratory failure. Am J Respir Crit Care Med 2003, 167: 1334-1340. 10.1164/rccm.200210-1175OC
Schultz TR, Lin RJ, Watzman HM, Durning SM, Hales R, Woodson A, Francis B, Tyler L, Napoli L, Godinez RI: Weaning children from mechanical ventilation: a prospective randomized trial of protocol-directed versus physician-directed weaning. Respir Care 2001, 46: 772-782.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
BG performed the statistical analysis and interpretation of the data. ON, FL, BG, YR conceived the study, participated in the design and execution of the study, the analysis of data and writing of the manuscript. BG performed the statistical analysis and interpretation of the data. AS performed respiratory investigations. ON, AD, CF, RC, SL performed clinical data collection. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Noizet, O., Leclerc, F., Sadik, A. et al. Does taking endurance into account improve the prediction of weaning outcome in mechanically ventilated children?. Crit Care 9, R798 (2005). https://doi.org/10.1186/cc3898
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc3898