
Abstract
Introduction
In critically ill patients sudden changes in glomerular filtration rate (GFR) are not instantly followed by parallel changes in serum creatinine. The aim of the present study was to analyze the utility of serum cystatin C as a marker of renal function in these patients.
Methods
Serum creatinine, serum cystatin C and 24-hour creatinine clearance (CCr) were determined in 50 critically ill patients (age 21–86 years; mean Acute Physiology and Chronic Health Evaluation II score 20 ± 9). They did not have chronic renal failure but were at risk for developing renal dysfunction. Serum cystatin C was measured using particle enhanced immunonephelometry. Twenty-four-hour body surface adjusted CCr was used as a control because it is the 'gold standard' for determining GFR.
Results
Serum creatinine, serum cystatin C and CCr (mean ± standard deviation [range]) were 1.00 ± 0.85 mg/dl (0.40–5.61 mg/dl), 1.19 ± 0.79 mg/l (0.49–4.70 mg/l), and 92.74 ± 52.74 ml/min per 1.73 m2 (8.17–233.21 ml/min per 1.73 m2), respectively. Our data showed that serum cystatin C correlated better with GFR than did creatinine (1/cystatin C versus CCr: r = 0.832, P < 0.001; 1/creatinine versus CCr: r = 0.426, P = 0.002). Cystatin C was diagnostically superior to creatinine (area under the curve [AUC] for cystatin C 0.927, 95% confidence interval 86.1–99.4; AUC for creatinine 0.694, 95% confidence interval 54.1–84.6). Half of the patients had acute renal dysfunction. Only five (20%) of these 25 patients had elevated serum creatinine, whereas 76% had elevated serum cystatin C levels (P = 0.032).
Conclusion
Cystatin C is an accurate marker of subtle changes in GFR, and it may be superior to creatinine when assessing this parameter in clinical practice in critically ill patients.
Similar content being viewed by others


Introduction
Glomerular filtration rate (GFR) is considered the best marker of renal function, and serum creatinine is the most commonly used biochemical parameter to estimate GFR in routine practice. However, there are some shortcomings to the use of this parameter. Factors such as muscle mass and protein intake can influence serum creatinine, leading to an inaccurate estimation of GFR. Normal serum creatinine may be observed in individuals with significantly impaired GFR [1, 2]. Moreover, in unstable, critically ill patients, acute changes in renal function can make real-time evaluation of GFR using serum creatinine difficult.
Cystatin C is a nonglycosylated protein that belongs to the cysteine protease inhibitors, cystatin superfamily [3]. These proteins play an important role in the regulation of proteolytic damage to the cysteine proteases. Cystatin C is produced at a constant rate by nucleated cells [4]. It is found in relatively high concentrations in many body fluids, especially in the seminal fluid, cerebrospinal fluid and synovial fluid [5]. Its low molecular weight (13.3 kDa) and positive charge at physiological pH levels facilitate its glomerular filtration. Subsequently, it is reabsorbed and almost completely catabolized in the proximal renal tubule [6, 7]. Therefore, because of its constant rate of production, its serum concentration is determined by glomerular filtration [8–11]. Moreover, its concentration is not influenced by infections, liver diseases, or inflammatory diseases. Use of serum cystatin C as a marker of GFR is well documented, and some authors have suggested that it may be more accurate than serum creatinine for this purpose [12–19].
The difficulties associated with monitoring and evaluating GFR in critically ill individuals are well known. Thus far no studies evaluating serum cystatin C as a marker of GFR in these patients have been reported. The aim of the present study were to determine the accuracy of serum cystatin C concentration as a marker of GFR in critically ill individuals.
Methods
Fifty patients, aged 21–86 years (mean 54 years), who were admitted to the intensive care unit at the Hospital Universitario La Paz in Madrid, Spain between January and September 2001, were included in the study. All patients were at risk for developing renal failure (haemodynamically unstable patients, septic patients, individuals receiving nephrotoxic drugs and others). Patients receiving corticoid therapy or with thyroid diseases were excluded. The patients' demographic characteristics and clinical conditions are summarized in Table 1.
A serum sample was drawn from each patient in the morning (between 07:00 and 10:00) to determine serum creatinine and serum cystatin C. A 24-hour urine sample was obtained just before the serum sample to calculate the creatinine clearance (CCr) using the following formula: CCr (ml/min) = (urine volume × urine creatinine)/(serum creatinine × 1440).
Serum creatinine values were obtained according to standard laboratory methods. CCr was adjusted to body surface (ml/min per 1.73 m2). Cystatin C values were obtained using particle enhanced immunonephelometry [10]. Normal serum creatinine values range from 0.6 to 1.3 mg/dl, and normal serum cystatin C values range from 0.6 to 1 mg/l. Renal dysfunction was defined as CCr below 80 ml/min per 1.73 m2.
Statistical analysis
The data are expressed in mean ± standard deviation (range). Correlations between quantitative data were determined using Pearson's test. P < 0.05 was considered statistically significant. The diagnostic value of serum cystatin C and serum creatinine for identifying renal dysfunction was evaluated using receiver operating characteristic curve analysis, and the data are expressed as area under the curve (AUC; 95% confidence interval). For statistical analysis, the SPSS R 9.0 (SPSS Inc., Chicago, IL, USA) program was used.
Results
The mean serum creatinine concentration was 1.00 ± 0.85 mg/dl (0.40–5.61 mg/dl) and the mean serum cystatin C concentration was 1.19 ± 0.79 mg/l (0.49–4.70 mg/l). The mean CCr adjusted for the body surface was 92.74 ± 52.74 ml/min per 1.73 m2 (8.17–233.21 ml/min per 1.73 m2).
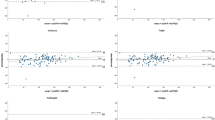
A decline in CCr was followed by an increase in levels of serum creatinine and serum cystatin C (Fig. 1). The inverse of the serum cystatin C and serum creatinine levels were plotted against CCr to determine the relationships of those parameters to this marker of renal function (Fig. 2a,b). There were significant correlations between CCr and 1/serum creatinine (r = 0.426, P = 0.002) and between CCr and 1/serum cystatin C (r = 0.832, P < 0.001).

Relationships of (a) serum creatinine and (b) serum cystatin C to creatinine clearance (CCr).

The (a) inverse of serum creatinine (1/creatinine) and the (b) inverse of cystatin C (1/cystatin c) were plotted against creatinine clearance (CCr) for each of patient (P = 0.002 versus P < 0.001).
Twenty-five out of the 50 patients enrolled in the study had renal dysfunction (CCr <80 ml/min per 1.73 m2). Five (20%) of these 25 patients with renal dysfunction had elevated serum creatinine concentrations, whereas 19 (76%) of them had elevated serum cystatin C levels at the time of renal dysfunction (P = 0.032). On the other hand, serum creatinine levels were within normal ranges in all patients with normal CCr (>80 ml/min per 1.73 m2) whereas 23 (92%) of them had normal concentrations of serum cystatin C.
Nonparametric receiver operating characteristic plots of sensitivity and specificity of serum creatinine and cystatin C for detecting renal dysfunction are shown in Fig. 3. The AUC for serum creatinine was 0.694 (95% confidence interval 54.1–84.6) and the AUC for serum cystatin C was 0.927 (95% confidence interval 86.1–99.4).

Nonparametric receiver operating characteristic plots of sensitivity and specificity of serum creatinine and cystatin C. Area under the curve (95% confidence interval): creatinine 0.694 (54.1–84.6) and cystatin C 0.927 (86.1–99.4).
Discussion
Monitoring renal function is extremely important in the management of critically ill patients. GFR, which can be measured by determining the clearance of various substances, is the 'gold standard' parameter for monitoring renal function. The ideal endogenous marker would be characterized by stable production rate, stable circulating levels (unaffected by pathological changes), lack of protein binding, free glomerular filtration, and lack of reabsorption or secretion; to date, no such marker has yet been identified. Some substances such as creatinine, urea, β2-microglobulin and retinol-binding protein have been used as endogenous markers of GFR, by measuring either their plasma levels or their renal clearance. Among them, the most useful markers for assessing GFR are serum creatinine and renal CCr. This is secondary to their correlations with the renal clearance of some exogenous substances (inulin, creatinine-EDTA, iothalamate) that are considered 'gold standards' for determining GFR.
Creatinine production changes significantly according to the muscle mass of the body and dietetic factors. It is filtered by the glomeruli, but it is also secreted by the renal tubules. This tubular secretion contributes approximately 20% of the total creatinine excretion by the kidney, and it can increase as GFR decreases. All of these factors explain why serum creatinine concentration may not be a good parameter for accurate determination of GFR, especially at lower rates [1].
Cystatin C production in the body is a stable process that is not influenced by renal conditions, increased protein catabolism, or dietetic factors. Moreover, it does not change with age or muscle mass like creatinine does. Its biochemical characteristics allow free filtration in the renal glomerulus, and subsequent metabolism and reabsorption by the proximal tubule. For these reasons, serum cystatin C has been suggested to be an ideal endogenous marker of GFR [12–19].
Most studies conducted to evaluate whether there is a role for serum cystatin C in determining GFR involved measurement of the clearance of exogenous substances such as creatinine-EDTA [14, 20–22], inulin [15, 23], Tc-DTPA [24, 25] and I-iothalamate [16, 26, 27]. Nevertheless, CCr is still the most reliable marker for determining GFR on a routine basis, and multiple studies have used CCr as a control for evaluating the role for serum cystatin C as a measure of GFR [28–30]. It is also a simple and cheap test, and, as mentioned above, its accuracy is sufficient for determining GFR. However, measurement of CCr can yield erroneous findings in many situations, particularly when poor urine collection technique is employed. That the present study was conducted in critically ill individuals, all of whom had a bladder catheter in place, makes such errors less likely.
Previous studies [14–16, 20–22, 25, 27] have found a wide range of correlations between 1/serum creatinine and clearance of exogenous substances (r = 0.50–0.89). In this study we found a correlation coefficient of 0.426 (P = 0.002) between CCr and 1/serum creatinine. This difference in correlation rates among studies may be explained better by the characteristics of the patients than by the methods used. Most of the studies in the literature were performed in individuals who were in a stable clinical condition (healthy individuals, patients with various renal diseases, and oncological patients undergoing chemotherapy). GFR in critically ill individuals can change rapidly because of, for example, renal hypoperfusion secondary to shock or the use of nephrotoxic agents. Despite this, it is not uncommon to see changes in the serum creatinine for up to several days until the stabilization phase is reached. This may also explain the poor diagnostic usefulness of serum creatinine as seen in our study (AUC 0.694) compared with that in other studies [25]. Only five out of 25 (20%) of the individuals enrolled in our study who developed renal dysfunction exhibited high serum creatinine levels at the time when CCr was tested. The delay that usually exists between the decline in GFR and that in serum creatinine makes the latter test poorly reliable for making therapeutic decisions in critically ill patients, such as a decision to change nephrotoxic agents or to increase renal perfusion.
We found a strong correlation between serum cystatin C concentrations and CCr in this study (r = 0.832, P < 0.001). This is similar to findings reported by other investigators (r = 0.73–0.91) [14–16, 20–22, 25, 27]. The diagnostic utility of cystatin C seen in our study (AUC = 0.927) is similar to that previously reported by other investigators [25]. The fact that most of our patients (76%) with acute renal dysfunction had high serum cystatin C levels at the time of CCr evaluation demonstrates that cystatin C is a good marker for application in real time, and suggests that serum cystatin C is a better marker of GFR than is serum creatinine in unstable, critically ill patients (20% of patients with acute renal dysfunction had high serum cystatin C level).
Conclusion
In the present study we evaluated and compared serum creatinine and serum cystatin C as markers of GFR in unstable, critically ill patients. Our data indicate that serum cystatin C is a good real-time marker of GFR in such patients. If this finding is subsequently confirmed, then the simplicity of serum cystatin C detection and its reasonable cost suggest that this test may soon replace CCr as the biochemical marker of choice for monitoring GFR in a routine practice.
Key messages
-
In this study, serum cystatin C was found to be a good marker of GFR.
-
Serum cystatin C was better at detecting changes in GFR than was serum creatinine in critically ill patients.
-
Determination of serum cystatin C levels is useful in the management of critically ill patients.
Abbreviations
- AUC:
-
= area under the curve
- CCr:
-
= creatinine clearance
- GFR:
-
= glomerular filtration rate.
References
Levey AS, Perrone RD, Madias NE: Serum creatinine and renal function. Annu Rev Med 1988, 39: 465-490. 10.1146/annurev.me.39.020188.002341
Shemesh O, Golbetz H, Kriss JP, Myers BD: Limitations of creatinine as filtration marker in glomerulopathic patients. Kidney Int 1985, 28: 830-836.
Perrone RD, Madias NE, Levey AS: Serum creatinine as an index of function renal: new insights into old concepts. Clin Chem 1992, 38: 1933-1953.
Abrahamson M, Olafsson I, Palsdottir A, Ulvsback M, Lundwall A, Jensson O, Grubb A: Structure and expression of the human cystatin C gene. Biochem J 1990, 268: 287-294.
Abrahasom M, Barret AJ, Salveson G, Grubb A: Isolation of six cysteine protease inhibitors from human urine. J Biol Chem 1986, 261: 11282-11289.
Grubb A: Diagnostic value of analysis of cystatin C and protein HC in biological fluids. Clin Nephrol 1992, S20-S27.
Tenstad O, Roald AB, Grubb A, Aukland K: Renal handling of radiolabelled human cystatin C in the rat. Scand J Clin Lab Invest 1996, 56: 409-414.
Nilsson-Ehle P, Grubb A: New markers for the determination of GFR: iohexol clearance and cystatin C serum concentration. Kidney Int Suppl 1994, 47: S17-S19.
Kyhse-Andersen J, Schmidt C, Nordin G, Andersson B, Nilsson-Ehle P, Lindstrom V, Grubb A: Serum cystatin C, determined by a rapid, automated particle-enhanced turbidimetric method, is a better marker than serum creatinine for glomerular filtration rate. Clin Chem 1994, 40: 1921-1926.
Finney H, Newman DJ, Gruber W, Merle P, Price CP: Initial evaluation of cystatin C measurement by partcle-enhanced inmunonephelometry on Behring nephelometer system (BNA, BN II). Clin Chem 1997, 43: 1016-1022.
Pergande M, Jung K: Sandwich enzyme inmunoassay of cystatin C in serum with commercially avaible antibodies. Clin Chem 1993, 39: 1885-1890.
Herget-Rosenthal S, Trabold S, Pietruck F, Holtmann M, Philipp T, Kribben A, Cystatin C: Efficacy as screening test for reduced glomerular filtration rate. Am J Nephrol 2000, 20: 97-102. 10.1159/000013564
Jung K, Jung M: Cystatin C: a promising marker of glomerular filtration rate to replace creatinine. Nephron 1995, 70: 370-371.
Newman DJ, Thakkar H, Hedward RG, Wilkie M, White T, Grubb A, Price CP: Serum cystatin C measured by automated inmunoassay: a more sensititive marker of changes in GFR than serum creatinine. Kidney Int 1995, 47: 312-318.
Stickle D, Cole B, Hock K, Hruska KA, Scott MG: Correlation of plasma concentrations of cystatin C and creatinine to inulin clearance in pediatric population. Clin Chem 1998, 44: 1334-1338.
Risch L, Blumberg A, Huber AR: Assessment of function renal in renal transplant patiens using cystatin C. A comparison to other renal function markers and estimates. Ren Fail 2001, 23: 439-448. 10.1081/JDI-100104727
Le Bricon T, Thervet E, Benlakehal M, Bousquet B, Legendre C, Erlich D: Changes in plasma cystatin C after renal transplantation and acute rejection in adults. Clin Chem 1999, 45: 2243-2249.
Randers E, Erlandsen EJ: Serum cyistatin C as as endogenous marker of the renal function. Clin Chem Lab Med 1999, 37: 389-395. 10.1515/CCLM.1999.064
Finney H, Newman DJ, Price CP: Adult reference for serum cystatin C, creatinine and predicted creatinine clearance. Ann Clin Biochem 2000, 37: 49-59. 10.1258/0004563001901524
Grubb A, Simonsen O, Sturfelt G, Trudsson L, Thysell H: Serum concentration of cystatin C, factor D and β 2 -microglobulin as a measure of glomerular filtrate rate. Acta Med Scand 1985, 218: 499-503.
Simonsen O, Grubb A, Thysell H: The blood serum concentration of cystatin D (gamma-trace) as a measure of the glomerular filtration rate. Scand J Clin Lab Invest 1985, 45: 97-101.
Bökenkamp A, Domanetzki M, Zinck R, Schumann G, Byrd D, Brodehl J: Cystatin C: a new marker of glomerular filtration rate in children independent of age and height. Pediatrics 1998, 101: 875-881. 10.1542/peds.101.5.875
Fliser D, Ritz E: Serum cystatin C concentration as a marker of renal dysfunction in the elderly. Am J Kidney Dis 2001, 37: 79-83.
Randers E, Erlandsen EJ, Pedersen OL, Hasling C, Danielsen H: Serum cystatin C as an endogenous parameter of the renal function in patients with normal to moderately impaired kidney function. Clin Nephrol 2000, 54: 203-209.
Randers E, Kristensen JH, Erlandsen EJ, Danielsen H: Serum cystatin C as a marker of the renal function. Scand J Clin Lab Invest 1998, 58: 585-592. 10.1080/00365519850186210
Coll E, Botey A, Alvarez L, Poch E, Quintó Ll, Saurina A, Vera M, Piera C, Darnell A: Serum cystanin C as a new marker for noninvasive estimation of glomerular filtration rate and as a marker for early renal impairment. Am J Kidney Dis 2000, 36: 29-34.
Risch L, Blumberg A, Huber A: Rapid and accurate assessment of glomerular filtration rate in patients with renal transplants using serum cystatin C. Nephrol Dial Transplant 1999, 14: 1991-1996. 10.1093/ndt/14.8.1991
Herget-Rosenthal S, Trabold S, Huesing J, Heemann U, Philipp T, Kribben A: Cystatin C: an accurate marker of glomerular filtration rate after renal transplantion? Transpl Int 2000, 13: 285-289. 10.1007/s001470050703
Paskalev E, Lambreva L, Simeonov P, Koicheva N, Beleva B, Genova M, Marcovska R, Nashkov A: Serum cystatin C in renal transplant patients. Clin Chim Acta 2001, 310: 53-56. 10.1016/S0009-8981(01)00522-8
Tian S, Kusano E, Ohara T, Tabei K, Itoh Y, Kawai T, Asano Y: Cystatin C measurement and its practical use in patients with various renal diseases. Clin Nephrol 1997, 48: 104-108.
Acknowledgements
We thank Concepción Madero, MD, from the Statistical Service of Hospital Universitario La Paz for her assistance with the analysis of the data. We thank Cynthia McCoig MD for reviewing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
PV managed patients, recruited them into the study and participated in the drafting of the manuscript. MJ conceived the study and participated in its design and coordination. MCS and JM were subinvestigators of the study; their principal role was to recruit patients. PC analyzed the samples.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Villa, P., Jiménez, M., Soriano, MC. et al. Serum cystatin C concentration as a marker of acute renal dysfunction in critically ill patients. Crit Care 9, R139 (2005). https://doi.org/10.1186/cc3044
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc3044