
Abstract
Introduction
The causative role of new hydroxyethyl starch (HES 130/0.4) in renal dysfunction frequency (a > 50% increase in serum creatinine or need for renal replacement therapy (RRT)) remains debated. Using the database of a multicenter study focusing on patients with severe sepsis and septic shock, the present study aimed at identifying factors associated with the occurrence of renal dysfunction.
Methods
Among the 435 patients in a multicenter study of patients with severe sepsis and septic shock in 15 Southern French ICUs, 388 patients surviving after 24 hour, without a history of renal failure were included. Factors associated with renal dysfunction and RRT were isolated using a multivariate analysis with logistic regression.
Results
Renal dysfunction was reported in 117 (33%) patients. Ninety patients required RRT. Among study participants, 379 (98%) were administered fluids in the first 24 hours of management: HES 130/0.4 only (n = 39), crystalloids only (n = 63), or both HES 130/0.4 and crystalloids (n = 276). RRT was independently associated with the need for vasopressors and the baseline value of serum creatinine in the first 24 hours. Multivariate analysis indicated that male gender, SAPS II score, being a surgical patient, lack of decrease in SOFA score during the first 24 hours, and the interventional period of the study were independently associated with renal dysfunction. Mortality increased in the presence of renal dysfunction (48% versus 24%, P < 0.01).
Conclusions
Despite being used in more than 80% of patients with severe sepsis and/or septic shock, the administration of HES 130/0.4 in the first 24 hours of management was not associated with the occurrence of renal dysfunction.
Similar content being viewed by others


Introduction
In patients with severe sepsis and septic shock, acute renal failure (ARF) is an independent factor for mortality [1, 2]. In the last decade, significant efforts were made to standardize the treatment of septic shock [3, 4]. One of the most important recommendations is volume expansion that could also prevent ARF [5, 6]. However, the type of fluid, especially the use of colloids, for volume expansion in septic shock remains a matter of debate [7–11]. Indeed, despite a larger plasma volume expansion power [12–14], the use of hydroxyethylstarch (HES) is not related to better outcomes when compared to isotonic crystalloids. In addition, use of HES has been associated with the development of an impaired renal function [7, 8, 15]. Thus, some experts suggest avoiding the use of HES in septic shock [7–9].
Because recent HES have a lower molecular weight (HES 130/0.4), some authors advocate their use in septic patients [16, 17]. In fact, controversial results have been reported in the literature [18, 19]. In the field of renal transplant, two studies suggested a better renal tolerance with low molecular weight HES, than with high molecular weight HES or gelatins [20, 21]. In patients with septic shock, a recent study suggested that even the use of low molecular weight HES was associated with renal dysfunction. In this study, HES 130/0.4 was used in the first phase of the study when the initial optimization of cardiac preload could be suspected as suboptimal when compared with the final phase using crystalloids [22].
In 2006, a regional program of quality improvement in patients with severe sepsis and septic shock was performed in 15 Southern French ICUs in the Languedoc Roussillon region. After an observational period (six months), an educational program was implemented to optimize the management of patients with severe sepsis and/or septic shock (Sepsi d'Oc study) [23]. As in other studies, the implementation of ten recommendations based on the Surviving Sepsis Campaign [3] and French recommendations were associated with an absolute reduction (13%) of 28-day mortality rates [23].
During this study, information on the type and the volume of fluid was collected in the first 24 hours of patient management. We hypothesized that, in severe sepsis or septic shock patients, the use of HES 130/0.4 may be associated with the development of renal dysfunction. The study was aimed at finding the variables in the first 24 hours that were associated with the occurrence of renal dysfunction in our cohort of patient. The secondary aims were to determine the volume of each type of fluid used in these patients, the relationship between the need for renal replacement therapy (RRT) and the type of fluid, and the outcome and the type of fluid.
Materials and methods
The present study was a part of Sepsi d'Oc (grants from the University Hospital of Nîmes), a quality improvement program for the management of severe sepsis in 15 ICUs in southern France (Languedoc Roussillon, population: 2,402,000 habitants) [23]. Therefore, the Institutional Review Board at the Nîmes University Hospital approved this study and stated that informed consent was waived. The patients or next of kin were informed of the study and could decline participation in the study.
The design of the Sepsi d'Oc study
The design of the Sepsis d'Oc study has been described elsewhere [23]. Briefly, the Sepsi d'Oc study compared patients with severe sepsis and/or septic shock who were seen during two periods. During the first six months of 2006 (1 January to 30 June), an observational study was performed while an intervention was proposed in the second half of the year (1 July to 31 December). The intervention was based on the Surviving Sepsis Campaign (Table 1) [3].
Patients
All patients with severe sepsis and septic shock according to international criteria [3], were eligible for the study. Exclusion criteria were moribund patients, immunosuppression, and evolving severe sepsis or septic shock sepsis for more than 24 hours.
Measurements
Age, sex, body mass index (BMI), simplified acute physiology II (SAPS II) [24] and sequential organ dysfunction (SOFA) [25] scores, the type (crystalloids or colloids or both) and volume of fluid administered during the first 24 hours of severe sepsis and septic shock were studied. The type of colloids was also collected. The type of fluids used for volume expansion during the first six hours and during the remaining 18 hours was also collected. Patient outcomes were used to determine the 28-day mortality rate and the occurrence of organ failure until day 28 (defined by organ dysfunction and/or infection (ODIN) score [26]).
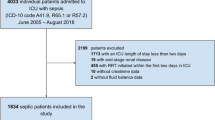
The present study (Figure 1)

Flow chart of the study. RRT, renal replacement therapy.
From the Sepsi d'Oc study data base (institutional free access with anonymized data), we analysed the factors associated with the occurrence of renal dysfunction defined by at least a 50% increase in plasma creatinine concentrations (corresponding to acute kidney injury network (AKIN) stage 1) [27] and/or the need of RRT.
Inclusion criteria
Patients included in the Sepsi d'Oc study, without end stage renal disease, who were alive after the first 24 hours of severe and/or septic shock, participated in the present analysis.
Exclusion criteria
Patients with end stage renal disease and those who died during the first 24 hours of severe and/or septic shock were excluded.
Measured parameters
In addition to variables measured in the Sepsi d'Oc study, the occurrence of renal dysfunction as previously defined was recorded. Information was collected on fluid volumes and the need for vasoactive drugs (vasopressors or inotropes) during the first 24 hours. Moreover, the duration of different organ dysfunctions (ODIN score) until day 28 was also recorded.
Statistical analysis
Quantitative variables are expressed as means (standard deviation (SD)) or medians (first quartile (Q1), third quartile (Q3)) according to variable distributions. The qualitative variables are expressed as frequencies (percentage).
A univariate analysis was first performed using chi-square tests or Fisher exact tests for qualitative factors and using analysis of variance or Mann-Whitney tests for quantitative factors.
For model building, we applied backward introduction of selected variables from univariate analysis (P-entry = 0.20). Data fitting was assessed by the Hosmer Lemeshow test. All analyses were performed using SAS version 9.1 (SAS Institute Inc., Cary, NC) using a 2-sided type 1 error rate of 0.05 as the threshold for statistical significance.
Results
Patient population during the study period
In 2006, 6,902 patients were admitted to the 15 ICUs. Five hundred and thirty-eight patients were initially screened for eligibility. Two patients under 18 years of age, 24 patients lacking
one criterion for severe sepsis (infection or Systemic Inflammatory Response Syndrome or organ failure) and 67 patients presenting a non-inclusion criterion were not included. Therefore, the Sepsi d'Oc study involved 445 patients.
Hemodynamic management
Among the 445 patients included in the Sepsi d'Oc study, 41 patients had prior end-stage renal disease. Sixteen patients died within the first 24 hours of management. Therefore, 388 patients were included in the present study (202 in the initial observational period, 186 in the second interventional period) (Figure 1). The patient characteristics are shown in Table 2. During the first 24 hours of severe sepsis or septic shock, 379 (98%) out of 388 patients received a fluid administration consisting of exclusively HES 130/0.4 (n = 39 (10%)) or crystalloids (n = 63 (17%)), or both HES 130/0.4 and crystalloids (n = 276 (73%)) (Figure 2). The mean total amount of fluid given during the first 24 hours was 3,780 ± 2,487 ml (Table 3). During the first 24 hours, red blood cell transfusion was required in 90 (24%) patients and vasopressors and inotropes were given to 307 (79%) and 71 (18%) patients, respectively. The 28-day mortality rate was 32%.

Number of patients receiving each type of fluid regimen during the initial 24-hour management period. HES, hydroxyethyl starch.
Patients with RRT and renal dysfunction
RRT was required in 90 (23%) out of 388 patients. In the patients who did not undergo RRT, an increase in plasma creatinine of at least 50% was found in 27 (7%) patients. An increase in plasma creatinine of less than 50% was identified in 237 (61%) patients. Of note, the course of the plasma creatinine during the first 24 hours could not be determined in 34 (8.8%) patients (missing data). A renal dysfunction was then confirmed in 117 of 364 patients (32%).
Factors associated with renal dysfunction
After univariate and multivariate analyses, male gender, an increase in SAPS II scores, surgical patients, no decrease in SOFA scores during the first 24 hours and the interventional period of the study were independently associated with renal dysfunction (Table 4). The mortality rate was higher in patients with renal dysfunction than in those without renal dysfunction (48% versus 24%, P < 0.01).
Factors associated with RRT
After multivariate analysis, the need for vasopressors and the baseline value of plasma creatinine were independently associated with the need for RRT (Table 4). The mortality rates were 52% in patients requiring RRT and 26% in those not requiring RRT (P < 0.01).
Discussion
The present study focuses on the factors associated with the occurrence of renal dysfunction in patients with severe sepsis and septic shock. In our cohort, 73% of patients were given a combination of HES and crystalloids. With respect to renal dysfunction [27], male gender, a high SAPS II score, no decrease in SOFA scores, the case-mix (surgery), and the interventional period of the Sepsi d'Oc study were identified as risk factors for renal dysfunction. The factors associated with the need for RRT were the baseline value of plasma creatinine and the need for vasopressors. The administration of HES 130/0.4 in the first 24 hours of resuscitation was not associated with a risk of renal dysfunction.
The Sepsi d'Oc study [23] was aimed at improving the initial management (during the first 24 hours) of patients with recent severe sepsis and/or septic shock (< 24 hours). Based on the Surviving Sepsis Campaign [3], ten recommendations were implemented in 15 ICUs of the Southern French 'Languedoc Roussillon' region. This before-after study resulted in a 28 day-mortality reduction. This finding was concordant with those of recent, large studies [28–32].
In the first 24 hours of management, more than 80% of the patients received HES. The volume of colloids was 830 ± 731 ml with a third quartile at 1,800 ml. The use of comparable volumes of HES in patients with severe sepsis or septic shock has already been reported elsewhere [19, 33]. In the present study, the volume of infused HES was in the range of recommended doses, as only 2% of patients received more than 50 ml/Kg of HES. Our findings are globally consistent with the available literature, suggesting that our population is well-representative of severe sepsis and septic shock patients. Of note, the total volume during the initial period of severe sepsis and or septic shock was lower than that reported by other groups [29, 34]. The occurrence of renal dysfunction and the need for RRT are associated with poorer outcomes, as previously reported [1, 2, 35].
In the Sepsi d'Oc study, the interventional period was associated with a larger occurrence of renal dysfunction but a higher 28-day survival rate. This finding suggests that an optimization of the initial management of patients with severe sepsis and septic shock may decrease the impact of renal dysfunction on the outcomes, as recently suggested by Badin et al.[36]. Moreover, the decrease in the 28-day mortality rate could expose more patients to the risk of renal dysfunction.
The present study failed to show that a low molecular weight HES is associated with poor renal outcomes. Initially, the potential deleterious effect of HES was demonstrated in the renal graft setting with previous non-low molecular weight types of HES [37, 38]. The suggested mechanism was an osmotic nephrosis. In ICU patients with septic shock, Schortgen et al.[39] also reported that more renal dysfunction was predominant in patients receiving HES, but this did not result in an increase in mortality or the need for RRT. In the VISEP study [15], a higher rate of renal dysfunction was reported but this did not impact the 90-day mortality rate. These previous studies used high molecular weight HES that were sometimes given in extremely large doses.
Some studies have shown that HES 130/0.4 is not associated with the development of impaired renal function [18, 19]. In the renal graft setting, two studies have shown that HES 130/0.4 is less deleterious in terms of renal function than the old generations of HES and gelatins [20, 21]. Elsewhere, in ICU patients, three studies reported that HES 130/0.4 administration was associated with poor renal outcome [8, 22, 40]. In the study reported by Bayer et al.[22], the baseline Central Venous Pressure (CVP) value was lower and more albumin and platelets and fresh frozen plasma were administrated in the HES group than in the gelatin and crystalloids groups. Moreover, patients in the HES group were more exposed to nephrotoxic product. These differences could explain why more renal dysfunctions were observed in this group without an increase in the need for RRT. In the study reported by Shortgen et al.[40], patients requiring HES administration previously received larger amounts of fluids. Moreover, they required more mechanical ventilation suggesting that they were more seriously ill whereas the SAPS II score was similar. In contrast, other groups reported similar findings to those of the present study [18, 19]. In the SOAP study [41], the infusion of HES was more frequent in the most seriously ill patients (higher baseline SAPS II and SOFA scores, more mechanically ventilated patients, more patients requiring blood products, more patients with severe sepsis and more patients with shock during their ICU stay) [18]. However, the multivariate analysis did not find that HES were associated with an increased risk of renal dysfunction. The study reported by Boussekey et al.[19] also failed to find a deleterious effect of HES in patients with severe sepsis and/or septic shock. Moreover, volumes of infused HES were similar to those reported in the present study (763 ± 595 ml on day 2, 1,031 ± 800 ml on day 7, 1,361 ± 1,393 ml on day 21). Our study suggests that in a real life situation, the physicians tend to respect the recommended doses of HES. This could probably partly explain the different results with previous studies in which HES was widely given. The present study clearly shows that the use of adequate dosages of HES is not associated with the occurrence of renal dysfunction.
The present study has several limitations. First, it focused on the use of different therapies in the first 24 hours of initial management of patients with severe sepsis and/or septic shock. We cannot report the real volume of fluid after 24 hours. However, Boussekey et al.[19] showed that the main dosage of HES is administrated in the first two days. Second, the present study was a cohort study and several biases could interfere with the findings. The physicians were not blinded, and a pre-selection of patients may have played a role in our results. However, this is a study reporting real-life practice, giving a partial response to an unresolved issue. One should note that more than 70% of our patients received both colloids and crystalloids, while randomized clinical trials often favor the use of a single type of fluid [15, 39]. Even if a multivariate analysis was performed, further randomized clinical trials will probably provide a definitive answer.
Conclusions
In the present study, renal dysfunction was independently associated with male gender, SAPS II score, a surgical patient, no decrease in SOFA score in the first 24 hours, and the interventional period of the Sepsi d'Oc study whereas RRT was independently associated with the need for vasopressors and the baseline value of serum creatinine. HES was widely used in patients with severe sepsis and septic shock in the initial 24-hour period but was not associated with deleterious impacts on renal function.
Key messages
-
During the first 24 hours of severe sepsis or septic shock, 379 (98%) of 388 patients received fluid administration consisting exclusively of HES 130/0.4 (n = 39 (10%)) or crystalloids (n = 63 (17%)), or both HES 130/0.4 and crystalloids (n = 276 (73%)). The mean total amount of fluid given during the first 24 hours was 3,780 ± 2,487 ml. The overall mortality rate was 32%.
-
RRT was required in 90 (23%) of 388 patients. The need for vasopressors and the baseline value of plasma creatinine were independently associated with the need for RRT. The mortality rates were 52% in patients requiring RRT and 26% in those not requiring RRT (P < 0.01).
-
A renal dysfunction was diagnosed in 117 of 364 patients (32%) (34 patients were excluded because of missing information concerning the initial course of plasma creatinine). After multivariate analysis, male gender, an increase in SAPS II scores, surgical patients, no decrease in SOFA scores during the first 24 hours and the interventional period of the Sepsi d'Oc study were independently associated with renal dysfunction. The mortality rate was higher in patients with renal dysfunction than in those without renal dysfunction (48% versus 24%, P < 0.01).
-
The use of HES was not associated with RRT or renal dysfunction.
Abbreviations
- AKIN:
-
acute kidney injury network
- ARF:
-
acute renal failure
- BMI:
-
body mass index
- HES:
-
hydroxyethyl starch
- ODIN:
-
organ dysfunction and/or infection
- RRT:
-
renal replacement therapy
- SAPS II:
-
simplified acute physiology score II
- SOFA:
-
sequential organ dysfunction score
References
Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) investigators: Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA 2005, 294: 813-818. 10.1001/jama.294.7.813
de Mendonca A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, Takala J, Sprung C, Cantraine F: Acute renal failure in the ICU: risk factors and outcome evaluated by the SOFA score. Intensive Care Med 2000, 26: 915-921. 10.1007/s001340051281
Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Intensive Care Med 2004, 30: 536-555. 10.1007/s00134-004-2210-z
Annane D, Bellissant E, Cavaillon JM: Septic shock. Lancet 2005, 365: 63-78. 10.1016/S0140-6736(04)17667-8
Brochard L, Abroug F, Brenner M, Broccard AF, Danner RL, Ferrer M, Laghi F, Magder S, Papazian L, Pelosi P, Polderman KH, ATS/ERS/ESICM/SCCM/SRLF AD HOC Committee on Acute Renal Failure: An Official ATS/ERS/ESICM/SCCM/SRLF Statement: Prevention and Management of Acute Renal Failure in the ICU Patient: an international consensus conference in intensive care medicine. Am J Respir Crit Care Med 2010, 181: 1128-1155. 10.1164/rccm.200711-1664ST
Dennen P, Douglas IS, Anderson R: Acute kidney injury in the intensive care unit: an update and primer for the intensivist. Crit Care Med 2010, 38: 261-275. 10.1097/CCM.0b013e3181bfb0b5
Bayer O, Reinhart K, Sakr Y, Kabisch B, Kohl M, Riedemann NC, Bauer M, Settmacher U, Hekmat K, Hartog CS: Renal effects of synthetic colloids and crystalloids in patients with severe sepsis: A prospective sequential comparison. Crit Care Med 2011, 39: 1335-1342. 10.1097/CCM.0b013e318212096a
Hartog CS, Kohl M, Reinhart K: A systematic review of third-generation hydroxyethyl starch (HES 130/0.4) in resuscitation: safety not adequately addressed. Anesth Analg 2011, 112: 635-645. 10.1213/ANE.0b013e31820ad607
Hartog CS, Bauer M, Reinhart K: The efficacy and safety of colloid resuscitation in the critically ill. Anesth Analg 2011, 112: 156-164. 10.1213/ANE.0b013e3181eaff91
Hartog C, Reinhart K: CONTRA: Hydroxyethyl starch solutions are unsafe in critically ill patients. Intensive Care Med 2009, 35: 1337-1342. 10.1007/s00134-009-1521-5
Perel P, Roberts I: Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database Syst Rev 2007, CD000567.
McIlroy DR, Kharasch ED: Acute intravascular volume expansion with rapidly administered crystalloid or colloid in the setting of moderate hypovolemia. Anesth Analg 2003, 96: 1572-1577.
Trof RJ, Sukul SP, Twisk JW, Girbes AR, Groeneveld AB: Greater cardiac response of colloid than saline fluid loading in septic and non-septic critically ill patients with clinical hypovolaemia. Intensive Care Med 2010, 36: 697-701. 10.1007/s00134-010-1776-x
Verheij J, van Lingen A, Beishuizen A, Christiaans HM, de Jong JR, Girbes AR, Wisselink W, Rauwerda JA, Huybregts MA, Groeneveld AB: Cardiac response is greater for colloid than saline fluid loading after cardiac or vascular surgery. Intensive Care Med 2006, 32: 1030-1038. 10.1007/s00134-006-0195-5
Brunkhorst FM, Engel C, Bloos F, Meier-Hellmann A, Ragaller M, Weiler N, Moerer O, Gruendling M, Oppert M, Grond S, Olthoff D, Jaschinski U, John S, Rossaint R, Welte T, Schaefer M, Kern P, Kuhnt E, Kiehntopf M, Hartog C, Matanson C, Loeffler M, Reinhart K, German Competence Network Sepsis (SepNet): Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 2008, 358: 125-139. 10.1056/NEJMoa070716
Ertmer C, Rehberg S, Van Aken H, Westphal M: Relevance of non-albumin colloids in intensive care medicine. Best Pract Res Clin Anaesthesiol 2009, 23: 193-212. 10.1016/j.bpa.2008.11.001
Westphal M, James MF, Kozek-Langenecker S, Stocker R, Guidet B, Van Aken H: Hydroxyethyl starches: different products--different effects. Anesthesiology 2009, 111: 187-202. 10.1097/ALN.0b013e3181a7ec82
Sakr Y, Payen D, Reinhart K, Sipmann FS, Zavala E, Bewley J, Marx G, Vincent JL: Effects of hydroxyethyl starch administration on renal function in critically ill patients. Br J Anaesth 2007, 98: 216-224. 10.1093/bja/ael333
Boussekey N, Darmon R, Langlois J, Alfandari S, Devos P, Meybeck A, Chiche A, Georges H, Leroy O: Resuscitation with low volume hydroxyethylstarch 130 kDa/0.4 is not associated with acute kidney injury. Crit Care 2010, 14: R40. 10.1186/cc8920
Wu Y, Wu AS, Wang J, Tian M, Jia XY, Rui Y, Yue Y: Effects of the novel 6% hydroxyethyl starch 130/0.4 on renal function of recipients in living-related kidney transplantation. Chin Med J (Engl) 2010, 123: 3079-3083.
Blasco V, Leone M, Antonini F, Geissler A, Albanese J, Martin C: Comparison of the novel hydroxyethylstarch 130/0.4 and hydroxyethylstarch 200/0.6 in brain-dead donor resuscitation on renal function after transplantation. Br J Anaesth 2008, 100: 504-508. 10.1093/bja/aen001
Bayer O, Reinhart K, Sakr Y, Kabisch B, Kohl M, Riedemann NC, Bauer M, Settmacher U, Hekmat K, Hartog CS: Renal effects of synthetic colloids and crystalloids in patients with severe sepsis: A prospective sequential comparison. Crit Care Med 2011, 39: 1335-1342. 10.1097/CCM.0b013e318212096a
Lefrant JY, Muller L, Raillard A, Jung B, Beaudroit L, Favier L, Masson B, Dingemans G, Thevenot F, Selcer D, Jonquet O, Capdevila X, Fabbro-Peray P, Jaber S, Sepsi d'Oc Study Group in the AzuRéa Group: Reduction of the severe sepsis or septic shock associated mortality by reinforcement of the recommendations bundle: a multicenter study. Ann Fr Anesth Reanim 2010, 29: 621-628. 10.1016/j.annfar.2010.04.007
Le Gall JR, Lemeshow S, Saulnier F: A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270: 2957-2963. 10.1001/jama.1993.03510240069035
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, Reinhart CK, Suter PM, Thijs LG: The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996, 22: 707-710. 10.1007/BF01709751
Fagon JY, Chastre J, Novara A, Medioni P, Gibert C: Characterization of intensive care unit patients using a model based on the presence or absence of organ dysfunctions and/or infection: the ODIN model. Intensive Care Med 1993, 19: 137-144. 10.1007/BF01720528
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A: Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 2007, 11: R31. 10.1186/cc5713
Ferrer R, Artigas A, Levy MM, Blanco J, Gonzalez-Diaz G, Garnacho-Montero J, Ibanez J, Palencia E, Quintana M, de la Torre-Prados MV: Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA 2008, 299: 2294-2303. 10.1001/jama.299.19.2294
Jones AE, Shapiro NI, Trzeciak S, Arnold RC, Claremont HA, Kline JA: Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA 2010, 303: 739-746. 10.1001/jama.2010.158
Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, Parker M, Gerlach H, Reinhart K, Silva E, Harvey M, Regan S, Angus DC: The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med 2010, 36: 222-231. 10.1007/s00134-009-1738-3
Jansen TC, van Bommel J, Schoonderbeek FJ, Sleeswijk Visser SJ, van der Klooster JM, Lima AP, Willemsen SP, Bakker J: Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med 2010, 182: 752-761. 10.1164/rccm.200912-1918OC
Castellanos-Ortega A, Suberviola B, Garcia-Astudillo LA, Holanda MS, Ortiz F, Llorca J, Delgado-Rodriguez M: Impact of the Surviving Sepsis Campaign protocols on hospital length of stay and mortality in septic shock patients: results of a three-year follow-up quasi-experimental study. Crit Care Med 2010, 38: 1036-1043. 10.1097/CCM.0b013e3181d455b6
Hartog CS, Brunkhorst FM, Bloos F, Bogatsch H, Engel C, Sengebusch K, Reinhart K, Ragaller M: Practice of volume therapy in patients with severe sepsis: results from a nationwide sepsis prevalence study. Intensive Care Med 2010, 36: 553-554. 10.1007/s00134-009-1736-5
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001, 345: 1368-1377. 10.1056/NEJMoa010307
Bagshaw SM, Laupland KB, Doig CJ, Mortis G, Fick GH, Mucenski M, Godinez-Luna T, Svenson LW, Rosenal T: Prognosis for long-term survival and renal recovery in critically ill patients with severe acute renal failure: a population-based study. Crit Care 2005, 9: R700-709. 10.1186/cc3879
Badin J, Boulain T, Ehrmann S, Skarzynski M, Bretagnol A, Buret J, Benzekri-Lefevre D, Mercier E, Runge I, Garot D, Mathonnet A, Dequin PF, Perrotin D: Relation between mean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study. Crit Care 2011, 15: R135. 10.1186/cc10253
Legendre C, Thervet E, Page B, Percheron A, Noel LH, Kreis H: Hydroxyethylstarch and osmotic-nephrosis-like lesions in kidney transplantation. Lancet 1993, 342: 248-249.
Cittanova ML, Leblanc I, Legendre C, Mouquet C, Riou B, Coriat P: Effect of hydroxyethylstarch in brain-dead kidney donors on renal function in kidney-transplant recipients. Lancet 1996, 348: 1620-1622. 10.1016/S0140-6736(96)07588-5
Schortgen F, Lacherade JC, Bruneel F, Cattaneo I, Hemery F, Lemaire F, Brochard L: Effects of hydroxyethylstarch and gelatin on renal function in severe sepsis: a multicentre randomised study. Lancet 2001, 357: 911-916. 10.1016/S0140-6736(00)04211-2
Schortgen F, Girou E, Deye N, Brochard L: The risk associated with hyperoncotic colloids in patients with shock. Intensive Care Med 2008, 34: 2157-2168. 10.1007/s00134-008-1225-2
Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR, Payen D: Sepsis in European intensive care units: results of the SOAP study. Crit Care Med 2006, 34: 344-353. 10.1097/01.CCM.0000194725.48928.3A
Acknowledgements
The authors thank the medical and nursing staffs of each unit participating to the study.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
LM, SJ, NM and JYL designed the study. LM, SJ, SA, NM and JYL participated in the statistical analysis. LM, SJ, NM, ML, CS and JYL wrote the manuscript. ML, BA, JMC helped to review the final version of the manuscript. All authors participated in the enrollment of patients and in the acquisition of data. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Muller, L., Jaber, S., Molinari, N. et al. Fluid management and risk factors for renal dysfunction in patients with severe sepsis and/or septic shock. Crit Care 16, R34 (2012). https://doi.org/10.1186/cc11213
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc11213