
Abstract
Background
Elevated rates of breast cancer in affluent Marin County, California, were first reported in the early 1990s. These rates have since been related to higher regional prevalence of known breast cancer risk factors, including low parity, education, and income. Close surveillance of Marin County breast cancer trends has nevertheless continued, in part because distinctive breast cancer patterns in well-defined populations may inform understanding of breast cancer etiology.
Methods
Using the most recent incidence and mortality data available from the California Cancer Registry, we examined rates and trends for 1990–1999 for invasive breast cancer among non-Hispanic, white women in Marin County, in other San Francisco Bay Area counties, and in other urban California counties. Rates were age adjusted to the 2000 US standard, and temporal changes were evaluated with weighted linear regression.
Results
Marin County breast cancer incidence rates between 1990 and 1999 increased 3.6% per year (95% confidence interval, 1.8–5.5), six times more rapidly than in comparison areas. The increase was limited to women aged 45–64 years, in whom rates increased at 6.7% per year (95% confidence interval, 3.8–9.6). Mortality rates did not change significantly in Marin County despite 3–5% yearly declines elsewhere.
Conclusion
Patterns of breast cancer incidence and mortality in Marin County are unlike those in other California counties, and they are probably explained by Marin County's unique sociodemographic characteristics. Similar trends may have occurred in other affluent populations for which available data do not permit annual monitoring of cancer occurrence.
Similar content being viewed by others


Introduction
Marin County, located north of San Francisco, California, is distinguished among urban counties in the United States by its relatively small population (250,000 residents), by a median per-capita income of more than 200% that of the nation [1], and by elevated rates of breast cancer that were first reported in the early 1990s [2]. The media has since pronounced Marin County 'the breast cancer capital of the world' [3], and heightened community concern has inspired grassroots and scientific efforts to investigate reasons for the high incidence. Initial studies have suggested that elevated rates in white women living in Marin County and the San Francisco Bay Area (SFBA) are generally explained by the higher prevalence of established breast cancer risk factors, including higher levels of education and income, later age at first birth, and nulliparity [4, 5]. Our previous assessment of breast cancer incidence trends in Marin County isolated the rate elevation to women aged 45–64 years at diagnosis [6]. Community and scientific concern over increasing incidence rates has nevertheless remained high, so detailed surveillance of incidence and mortality rates has continued.
It has been estimated that only 45–55% of breast cancer cases in the United States are explained by established risk factors such as income, reproductive factors, and family history [7]. Distinctive breast cancer incidence and mortality patterns in well-defined populations may therefore inform etiologic understanding. For this reason, and as part of ongoing regional cancer surveillance efforts, we analyzed the most recent breast cancer incidence and mortality data available for Marin County and compared these rates and trends with those from other areas in California.
Materials and methods
Cancer incidence and mortality data
We obtained cancer incidence and mortality data for Marin County and other California counties from the California Cancer Registry and the California Office of Vital Statistics, respectively. Analyses were based on new cases of invasive breast cancer (International Classification of Diseases – Oncology, 2nd edition, site codes 50.0–50.9 excluding histology codes 9590–9989; invasive cases only) and breast cancer deaths (International Classification of Disease, 10th edition, site codes C50–C509) during the period 1 January 1990–31 December 1999. We excluded in situ cancers from this analysis because of ongoing controversy over the diagnosis and malignant potential of these tumors [8]. We additionally limited the analyses to white, non-Hispanic women because of the marked variation in breast cancer incidence by race/ethnicity, and because of the small and unstable numbers of cases and deaths (n <10 each year) among African-American, Hispanic, and Asian/Pacific Islander women in Marin County.
Rate calculation and statistical considerations
Using population estimates obtained from the California Department of Finance [9], we calculated incidence and mortality rates for the individual years 1990–1999 as well as for the 5-year period 1995–1999 for three geographic areas: Marin County, the rest of the SFBA (Alameda, Contra Costa, San Francisco, San Mateo, and Santa Clara counties), and other urban counties in California. The urban counties, which were defined as US Census Bureau-designated urban areas or as containing at least one city of at least 50,000 residents, included Butte, El Dorado, Fresno, Kern, Los Angeles, Madera, Merced, Monterey, Napa, Orange, Placer, Riverside, Sacramento, San Bernardino, San Diego, San Joaquin, San Luis Obispo, Santa Barbara, Santa Cruz, Shasta, Solano, Sonoma, Stanislaus, Sutter, Tulare, Ventura, Yolo, and Yuba counties. We excluded rural counties from the comparison because of the consistent association between urban residence and breast cancer [10]. SEER*Stat software [11] was used to compute the rates, to age adjust them to the year 2000 US standard population, to produce the 95% confidence interval (CI), and to conduct weighted linear regression to estimate average annual percentage changes, which were evaluated for statistical significance with a two-sided P value of 0.05. The American Joint Commission on Cancer, 3rd edition staging was used to calculate stage-specific rates.
Results
Incidence trends
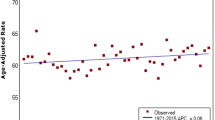
Incidence rates of invasive breast cancer among white women in Marin County show a distinctly increasing trend over the past decade (Fig. 1). Linear regression showed that breast cancer rates increased 37% in Marin County between 1990 and 1999, but increased only 3% in the rest of the SFBA and other urban counties in California. The annual rate of increase (3.6; 95% CI, 1.8–5.5) was, on average, six times higher in Marin County than in comparison areas (Table 1). In addition, there was a significant 20% increase in incidence in Marin County during the 1-year period between 1998 (191 cases per 100,000; 95% CI, 167–219) and 1999 (230 cases per 100,000; 95% CI, 203–261).

Breast cancer incidence and mortality trends among white, non-Hispanic women in Marin County, other San Francisco Bay Area (SFBA) counties, and other urban California counties, 1990–1999.
Our previous study of Marin County incidence trends showed that, between 1991 and 1997, rates increased at a faster pace among women aged 45–64 years than among women of other ages [6]. The present analyses confirm and update these observations, and show that the large rate increase between 1990 and 1999 was limited almost entirely to women aged 45–64 years, who represented about one-half of the breast cancer cases diagnosed in the county. Breast cancer incidence increased 79% between 1990 and 1999 among Marin County women aged 45–64 years, an average annual increase of 6.7% (Table 1). Trends were stable in women of similar age in other regions as well as in women aged <45 and ≥ 65 years regardless of region (Fig. 2). By 1996, breast cancer rates in Marin County women aged 45–64 years approached the magnitude of those aged ≥ 65 years in other counties (Fig. 2).
Breast cancer incidence trends by age at diagnosis among white, non-Hispanic women in Marin County, other San Francisco Bay Area (SFBA) counties, and other urban California counties, 1990–1999.
Comparison of average annual incidence rates
By the end of the decade, breast cancer rates continued to be substantially higher in Marin County than in other parts of California, including other parts of the SFBA. Annual, age-adjusted breast cancer incidence rates for Marin County averaged over the five most recent years for which we have data (1995–1999) exceeded, by at least 20%, those from any single other urban county in California, and they were 28% higher than rates for other SFBA counties and were 38% higher than rates for other urban counties combined (Table 2). Among women aged 45–64 years, average incidence rates were 58% higher in Marin County than in the rest of the SFBA and were 72% higher than in other urban California counties.
Nearly all of the excess in overall rates was for early-stage (stage I/stage II) disease, for which Marin County rates (175 cases per 100,000; 95% CI, 165–187) were 31% higher than those for the rest of the SFBA (134 cases per 100,000; 95% CI, 131–136) and were 48% higher than those for other urban California counties (119 cases per 100,000; 95% CI, 117–120). Rates of later-stage (stage III/stage IV) disease were not significantly different in Marin County (15 cases per 100,000; 95% CI, 12–19) as compared with those in other areas (SFBA: 13 cases per 100,000; 95% CI, 12–14; other urban California counties: 14 cases per 100,000; 95% CI, 13–14).
Mortality trends
Despite the excess in early-stage tumors, breast cancer mortality rates have been decreasing more slowly in Marin County than they have been in other parts of the state. Whereas breast cancer mortality declined significantly at 2–3% per year in other parts of California between 1990 and 1999, Marin County rates decreased less than 1% per year; this change was not statistically significantly different from zero (Table 1). Five-year average (1995–1999) breast cancer death rates in Marin County women were 25% higher than those rates observed for other parts of the SFBA and urban California counties (Table 2). Among women age 45–64 years, mortality rates increased 1.9% per year in Marin County while decreasing 3–4.5% per year in other SFBA and urban California counties.
Discussion
Patterns of breast cancer incidence and mortality in Marin County, California, have deviated markedly from those observed in other parts of the state over the past decade. These findings demonstrate the public health burden of breast cancer in this community, but also have the potential to serve as a source of hypothesis generation as regards the association between higher socioeconomic status and breast cancer. Cancer incidence patterns in Marin County have been informative in the past; the soaring incidence of endometrial cancer there in the 1970s [12] was ultimately linked to the utilization of estrogen therapy by postmenopausal women.
The higher breast cancer incidence in Marin County has been attributed to its unique and uniform sociodemographic characteristics [4], which correspond to a higher prevalence of women with known breast cancer risk factors. With a relatively small population for an urban county, Marin County was one of the wealthiest counties in the United States in 2000, with a median per-capita income of almost US$58,000, about 200% higher than the state and national medians [1]. Marin County consistently ranks among counties in the nation with the most highly educated populations, with at least 44% of adults having a bachelor's degree, which is 220% higher than the national rate in 1990 [13]. It also has a higher percentage of white, non-Hispanic residents (80%) than surrounding counties [9].
In accordance with its high socioeconomic status, Marin County has higher proportions of women with other established breast cancer risk factors, including lower parity [4] and later age at childbearing. In 1994, 71% of the live births to white women were to mothers aged 30 years and over in Marin County, as compared with 46% in California [14]. In addition, 69% of all women aged 55–64 years and 47% of all women aged 45 and over reported using hormone replacement therapy as part of a community health survey conducted in Marin County in 2001 (RRE, unpublished data, 2002) although comparable figures are not available for the state. Prehn and West, using 1990 census data, calculated breast cancer incidence rates for aggregations of census block groups matched to Marin County on characteristics associated with higher breast cancer risk (percentage white population, urban status, average parity, median household income, percentage of persons with a college degree, percentage of persons with a working-class occupation, and percentage of households living below the poverty line), and found rates in the matched areas to be comparable with those in Marin County [4]. In another study using interview-based information, higher breast cancer incidence rates among white women in the SFBA were also fully explained by the distribution of parity, age at first birth, months of breast-feeding, age at menarche, and age at menopause [5]. Other previous analyses of nationwide variation in breast cancer incidence and mortality found most of it attributable to the distribution of known breast cancer risk factors [15, 16]. It thus seems likely that a substantial part of the excess incidence observed in Marin County is explained by a higher concentration of women with a higher breast cancer risk profile.
The increasing incidence of breast cancer might be explained by changes in the composition of the Marin County population over the past decade. Data from the US Census Bureau show that Marin County had relatively high levels of outmigration and had low levels of immigration during 1990–1998 compared with other parts of California [17]. Examination of the age-specific population denominators used in this analysis [9] shows that the proportion of women aged 45–64 years, which includes the leading edge of the 'baby boomer' cohort, changed very little over the decade in Marin County, whereas this proportion increased substantially in comparison areas. This deviant pattern could be explained by the outmigration from Marin County of women aged 45–64 years and by the immigration of younger women. As realty data show that the median single family home price surged to $530,000 by the year 2000, making Marin County one of the least affordable counties in the nation [18], we speculate that women in the age group 45–64 years who may have had more children at younger ages left the county over the decade, while younger, perhaps professional, women who did not have children or who delayed child-bearing immigrated to or stayed in the county. Some support for this phenomenon is provided by the widening difference between Marin County and California in the proportion of live births to white mothers aged 30 years and older as compared with those aged younger than 30 years (ratio: 1.54 in 1994, and 1.60 in 2000) [14]. The numbers of women in Marin County with a high breast cancer risk profile may thus have increased further over the decade.
We consider it doubtful that the observed trends are strongly biased by inaccurate cancer registry or population data. The trends observed in the rates were also observed in the case counts alone. Although some of the observed rate increases could be attributable to inaccuracy of the intercensal population estimates, particularly in the 45–64 age group, systematic population undercounts would presumably have produced similar increases in the incidence of other cancers, which we did not observe. Furthermore, the California Department of Finance population estimate for Marin County for the year 1999 (244,900) was less than 1% lower than the actual count performed by the US Census in 2000 (247,289). Regardless of this, incidence trends will be reassessed when revised population estimates benchmarked to the 2000 census become available.
Breast cancer incidence has been positively associated with socioeconomic status across race/ethnicity, geography, and time [19–23]. Recent data from California show that rates for white women in the highest socioeconomic quintile were 27% higher than the lowest quintile and were 13% higher than the overall rate [23]. However, understanding of the biologic factors mediating this association remains incomplete. In a large, national, interview-based study conducted in the 1970s, adjustment for reproductive patterns, menopausal characteristics, hormone use, alcohol consumption, body mass index, height, and family history did not entirely account for the relations of income and education to breast cancer risk [24]. To achieve a more contemporary understanding of the contributions of established breast cancer risk factors, it would be helpful to reassess the roles of factors whose prevalence has increased substantially over time, including delayed childbearing [25] and use of hormone replacement therapy [26]. In addition, there are ongoing efforts in Marin County to identify novel risk factors relevant to this socioeconomic group. These efforts include a case–control study of adolescent exposures and experiences for which data collection was recently completed, and projects to identify environmental exposures unique to this group or to the county.
It is uncertain to what extent the socioeconomic gradient in breast cancer, and the patterns we have observed in Marin County, might be explained by better awareness of breast cancer, by access to health care, or by utilization of screening programs. Screening mammography has been linked previously to breast cancer incidence increases in the United States, most notably the 4% annual increase after its widespread adoption in the 1980s [27]. In the state of Hawaii, mammography utilization accounted for 23% of the geographic variation in overall breast cancer incidence in 1992–1993 and for 36% of the variation among women aged 50–64 years [28].
At first glance, our observations of incidence excesses limited to early-stage cancers would suggest some relation to regional differences in screening. However, these patterns do not demonstrate other hallmarks of differential 'lead time bias'. There was no evidence of a Marin County deficit in later-stage cancers, mortality rates remained stable despite distinct mortality declines observed in comparison regions, and disparate age-specific incidence trends were observed within the larger age group (aged 40+ years) targeted by screening programs [6]. In addition, mammography utilization data do not suggest substantially elevated rates of screening among Marin County women. A community health survey conducted in Marin County in 2001 found that 68% of women aged 40+ years received a mammogram in the past year; this proportion is comparable with or only slightly higher than those for other areas with lower breast cancer rates (RRE, unpublished data, 2002). There are no data available to explore other aspects of mammographic screening in this population, such as increased frequency or better sensitivity due to higher volume [29]. The possibility of a real increase in small tumors is, however, underscored by reports of significant increases in small breast cancers among unscreened women in Australia [30].
United States cancer registries do not routinely collect information about patient income and education, making assessment of cancer trends by socioeconomic status very difficult [31]. Our findings of rapidly increasing rates of breast cancer in Marin County over the past decade, however, along with evidence that high rates there are explained by the sociodemography of the county [4], cause us to speculate whether breast cancer rates are increasing similarly in other groups of highly educated and affluent women nationwide. While we can monitor incidence rates in Marin County because it is a county, we cannot conduct ongoing annual cancer surveillance in sociodemographically similar populations living in sub-county regions because of a lack of appropriate population estimates. When detailed 2000 Census data are released for subcounty areas, we will re-examine the relations between sociodemographic characteristics and geographic variation in breast cancer incidence. If our speculations are supported by these data, then Marin County statistics indeed serve as a 'canary in the gold mine' as regards breast cancer incidence in educated or affluent women, and they may also be prescient as regards breast cancer mortality. These observations should motivate us to intensify our efforts to learn more about the relationship between socioeconomic status and breast cancer.
Conclusion
The incidence of invasive breast cancer has increased significantly in the affluent population of Marin County, Cali-fornia, between 1990 and 1999. This large increase has not been observed in other parts of California and appears to be limited to early-stage disease among white women aged 45–64 years at diagnosis. Despite the preponderance of early-stage diagnoses in Marin County, breast cancer mortality rates remain unchanged, declining somewhat overall and increasing slightly among women aged 45–64 years. These findings, coupled with our understanding of the unique sociodemographic characteristics of this region, have the potential to serve as a source of hypothesis generation as regards the association between higher socioeconomic status and breast cancer.
Abbreviations
- CI:
-
= confidence interval
- SFBA:
-
= San Francisco Bay Area.
References
US Department of Commerce: Bureau of Economic Analysis Regional Accounts Data, Local Area Personal Income. [http://www.bea.doc.gov/bea/regional/reis/]
West DW, Davis TE: Breast cancer incidence among women in the San Francisco and Monterey Bay areas. Greater Bay Area Cancer Registry Report. 1991, 3: 1-4.
Shoals M: California's breast cancer blight. BBC News Online. [http://www.news.bbc.co.uk/hi/english/sci/tech/newsid_1791000/1791727.stm]
Prehn AW, West DW: Evaluating local differences in breast cancer incidence rates: a census-based methodology (United States). Cancer Causes Control. 1998, 9: 511-517. 10.1023/A:1008809819218.
Robbins AS, Brescianini S, Kelsey JL: Regional differences in known risk factors and the higher incidence of breast cancer in San Francisco. J Natl Cancer Inst. 1997, 89: 960-965. 10.1093/jnci/89.13.960.
Prehn AW, Clarke CA, Topol B, Glaser SL, West DW: Increase in breast cancer incidence in middle-aged white women during the 1990's. Ann Epidemiol. 2002,
Madigan MP, Ziegler RG, Benichou J, Byrne C, Hoover RN: Proportion of breast cancer cases in the United States explained by well-established risk factors. J Natl Cancer Inst. 1995, 87: 1681-1685. 10.1093/jnci/87.22.1681.
Schwartz GF, Solin LJ, Olivotto IA, Ernster VL, Pressman PI: Consensus Conference on the Treatment of In Situ Ductal Carcinoma of the Breast, April 22–25, 1999. Cancer. 2000, 88: 946-954. 10.1002/(SICI)1097-0142(20000215)88:4<946::AID-CNCR26>3.0.CO;2-5.
California Department of Finance: Race/Ethnic Population Projections with Age and Sex Detail. 1970, [http://www.dof.ca.gov/HTML/DEMOGRAP/Race.htm] –2040
Kelsey JL, Horn-Ross PL: Breast cancer: magnitude of the problem and descriptive epidemiology. Epidemiol Rev. 1993, 15: 7-16.
National Cancer Institute: SEER*Stat 4.0. Silver Spring, Maryland, USA: Information Management Services, Inc;. 2001
Austin DF, Roe KM: Increase in cancer of the corpus uteri in the San Francisco-Oakland standard metropolitan statistical area, 1960–75. J Natl Cancer Inst. 1979, 62: 13-16.
US Census Bureau: Educational Attainment of People 25 Years Old and Older:. 1990, [http://www.census.gov/population/www/socdemo/educ-attn.html] Decennial Census
California Department of Health Services: Vital Statistics Query System. [http://www.applications.dhs.ca.gov/vsq/default.asp]
Sturgeon SR, Schairer C, Gail M, McAdams M, Brinton LA, Hoover RN: Geographic variation in mortality from breast cancer among white women in the United States. J Natl Cancer Inst. 1995, 87: 1846-1853.
Laden F, Spiegelman D, Neas LM, Colditz GA, Hankinson SE, Manson JE, Byrne C, Rosner BA, Speizer FE, Hunter DJ: Geographic variation in breast cancer incidence rates in a cohort of U.S. women. J Natl Cancer Inst. 1997, 89: 1373-1378. 10.1093/jnci/89.18.1373.
US Census Bureau: Demographic Components of Population Change, April 1. 1990, [http://eire.census.gov/popest/archives/county/co_99_4.php] to July 1, 1999: California
California Association of Realtors. [http://www.car.org]
Rimpela AH, Pukkala EI: Cancers of affluence: positive social class gradient and rising incidence trend in some cancer forms. Soc Sci Med. 1987, 24: 601-606. 10.1016/0277-9536(87)90064-5.
Liu L, Deapen D, Bernstein L: Socioeconomic status and cancers of the female breast and reproductive organs: a comparison across racial/ethnic populations in Los Angeles County, California (United States). Cancer Causes Control. 1998, 9: 369-380. 10.1023/A:1008811432436.
Krieger N, Quesenberry C, Peng T, Horn-Ross P, Stewart S, Brown S, Swallen K, Guillermo T, Suh D, Alvarez-Martinez L, Ward F: Social class, race/ethnicity, and incidence of breast, cervix, colon, lung, and prostate cancer among Asian, Black, Hispanic, and White residents of the San Francisco Bay Area, 1988–92 (United States). Cancer Causes Control. 1999, 10: 525-537. 10.1023/A:1008950210967.
Pukkala E, Weiderpass E: Time trends in socio-economic differences in incidence rates of cancers of the breast and female genital organs (Finland, 1971–1995). Int J Cancer. 1999, 81: 56-61. 10.1002/(SICI)1097-0215(19990331)81:1<56::AID-IJC11>3.0.CO;2-4.
Yost K, Perkins C, Cohen R, Morris C, Wright W: Socioeconomic status and breast cancer incidence in California for different race/ethnic groups. Cancer Causes Control. 2001, 12: 703-711. 10.1023/A:1011240019516.
Heck KE, Pamuk ER: Explaining the relation between education and postmenopausal breast cancer. Am J Epidemiol. 1997, 145: 366-372.
Heck KE, Schoendorf KC, Ventura SJ, Kiely JL: Delayed child-bearing by education level in the United States, 1969–1994. Matern Child Health J. 1997, 1: 81-88. 10.1023/A:1026218322723.
Keating NL, Cleary PD, Rossi AS, Zaslavsky AM, Ayanian JZ: Use of hormone replacement therapy by postmenopausal women in the United States. Ann Intern Med. 1999, 130: 545-553.
Wun LM, Feuer EJ, Miller BA: Are increases in mammographic screening still a valid explanation for trends in breast cancer incidence in the United States?. Cancer Causes Control. 1995, 6: 135-144.
Maskarinec G, Wilkens L, Meng L: Mammography screening and the increase in breast cancer incidence in Hawaii. Cancer Epidemiol Biomarkers Prev. 1997, 6: 201-208.
Esserman L, Cowley H, Eberle C, Kirkpatrick A, Chang S, Berbaum K, Gale A: Improving the accuracy of mammography: volume and outcome relationships. J Natl Cancer Inst. 2002, 94: 369-375. 10.1093/jnci/94.5.369.
Harmer C, Staples M, Kavanagh AM: Evaluation of breast cancer incidence: is the increase due entirely to mammo-graphic screening?. Cancer Causes Control. 1999, 10: 333-337. 10.1023/A:1008949819969.
Krieger N: Socioeconomic data in cancer registries. Am J Public Health. 2001, 91: 156-157.
Acknowledgements
Cancer incidence data were collected by the Northern California Cancer Center under contract N01-CN-65107 with the National Cancer Institute, National Institutes of Health, and with support of the California Cancer Registry, a project of the Cancer Surveillance Section, California Department of Health Services, under subcontract 1000891 with the Public Health Institute. The content of this publication does not necessarily reflect the views or policies of the US Department of Health and Human Services or the California Department of Health Services, nor does mention of trade names, commercial products, or organization imply endorsement by the US Government or the state of California.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Clarke, C.A., Glaser, S.L., West, D.W. et al. Breast cancer incidence and mortality trends in an affluent population: Marin County, California, USA, 1990–1999. Breast Cancer Res 4, R13 (2002). https://doi.org/10.1186/bcr458
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/bcr458