
Abstract
Introduction
Mammographic density is a strong risk factor for breast cancer overall, but few studies have examined the association between mammographic density and specific subtypes of breast cancer, especially aggressive basal-like breast cancers. Because basal-like breast cancers are less frequently screen-detected, it is important to understand how mammographic density relates to risk of basal-like breast cancer.
Methods
We estimated associations between mammographic density and breast cancer risk according to breast cancer subtype. Cases and controls were participants in the Carolina Breast Cancer Study (CBCS) who also had mammograms recorded in the Carolina Mammography Registry (CMR). A total of 491 cases had mammograms within five years prior to and one year after diagnosis and 528 controls had screening or diagnostic mammograms close to the dates of selection into CBCS. Mammographic density was reported to the CMR using Breast Imaging Reporting and Data System categories. The expression of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 1 and 2 (HER1 and HER2), and cytokeratin 5/6 (CK5/6) were assessed by immunohistochemistry and dichotomized as positive or negative, with ER+ and/or PR+, and HER2- tumors classified as luminal A and ER-, PR-, HER2-, HER1+ and/or CK5/6+ tumors classified as basal-like breast cancer. Triple negative tumors were defined as negative for ER, PR and HER2. Of the 491 cases 175 were missing information on subtypes; the remaining cases included 181 luminal A, 17 luminal B, 48 basal-like, 29 ER-/PR-/HER2+, and 41 unclassified subtypes. Odds ratios comparing each subtype to all controls and case-case odds ratios comparing mammographic density distributions in basal-like to luminal A breast cancers were estimated using logistic regression.
Results
Mammographic density was associated with increased risk of both luminal A and basal-like breast cancers, although estimates were imprecise. The magnitude of the odds ratio associated with mammographic density was not substantially different between basal-like and luminal A cancers in case–control analyses and case-case analyses (case-case OR = 1.08 (95% confidence interval: 0.30, 3.84)).
Conclusions
These results suggest that risk estimates associated with mammographic density are not distinct for separate breast cancer subtypes (basal-like/triple negative vs. luminal A breast cancers). Studies with a larger number of basal-like breast cancers are needed to confirm our findings.
Similar content being viewed by others

Introduction
Studies of the molecular profiles of breast cancers have indicated that breast tumors can be classified into five etiologically and prognostically relevant subtypes on the basis of gene expression patterns [1]. Since then luminal A (estrogen receptor (ER)-positive, progesterone receptor (PR)-positive, and human epidermal growth factor receptor (HER)-2/neu-negative) and basal-like (ER-negative, PR-negative, HER-2/neu-negative, and cytokeratin 5/6-positive and/or HER-1 positive) breast cancers have been widely studied clinically and epidemiologically [2–14], with luminal A cancers being of interest because they represent the largest percentage (45%) of cancers, and basal-like cancers, whereas rarer (5 to 15% of cases), having the poorest survival outcomes [4, 15, 16]. Basal-like breast cancers are more prevalent among younger African American women with breast cancer and show unique risk factor patterns, often having risk factor-specific associations in the opposite direction of those for breast cancer overall and luminal A tumors [4, 7–14]. For example, the protective effects of parity are observed with breast cancers overall and with luminal breast cancers, but appear to be reversed with basal-like breast cancer [4]. It is important to understand how distinct molecular subtypes are related to established or suspected breast cancer risk factors.
Among breast cancer risk factors, mammographic density is one of the strongest and most consistent risk factors, with studies estimating that women with the highest mammographic density may be at a 4- to 6-fold increased risk of developing breast cancer compared to women with the lowest mammographic density [17–24]. However, there are conflicting results on the association between mammographic density and risk of breast cancer subtypes defined by hormone receptor status (reviewed in Boyd et al. [25]). Of the eight case–control and cohort studies examining the association between mammographic density and breast cancer risk by tumor hormonal status, six [26–31] observed increased risk of both ER- positive (ER+) and ER-negative (ER-) tumors among those with the most dense breast tissue, and two [32, 33] observed increased risks for ER+ tumors only. Of the thirteen studies with cases only, all but two [34, 35] concluded that there were no significant differences in mammographic density by hormone receptor status [36–46]. A recent meta-analysis on the topic also concluded that mammographic density is similarly strongly associated with both ER+ and ER- tumors [47].
Despite these largely negative results, some uncertainty remains. Notably, recent results suggest that basal-like breast cancers are associated with decreased involution of terminal duct lobular units (TDLUs), the structures from which most breast cancer precursors and cancers develop [48]. Because elevated mammographic density is also associated with decreased TDLU involution [49], it may be expected that basal-like breast cancers would therefore be associated with higher mammographic density. However, data relating mammographic density to specific intrinsic subtypes are limited [35]. More detailed subtyping that distinguishes HER2+ tumors from basal-like tumors and from tumors with poor immunohistochemical (IHC) reaction due to fixing artifacts is needed. A few studies have evaluated the association between mammographic density and three IHC markers (ER, PR, HER-2/neu), but further resolution of these triple-negative tumors into those that are truly basal-like would improve these analyses [26, 30, 31, 40].
We hypothesized that the association between mammographic density and breast cancer risk would be different for basal-like versus luminal A breast cancers. We therefore examined the association between mammographic density and basal-like and luminal A subtypes of breast cancer using a panel of five IHC markers. Participants in the Carolina Breast Cancer Study (CBCS) were matched to participants in the Carolina Mammography Registry (CMR) to allow estimation of the association between mammographic density and risk of these specific breast cancer subtypes.
Methods
Study setting and population
Subjects in this study were participants in the CBCS who also had mammograms recorded in the CMR. CBCS is a population-based, case–control study conducted in 24 counties in North Carolina, designed to identify genetic and environmental factors for breast cancer risk in African Americans and Caucasians. Briefly, CBCS participants were women aged 20 to 74 years; cases were identified from the North Carolina Central Cancer Registry and controls were identified using drivers’ license and Medicare beneficiary lists. Controls were age and race frequency-matched to cases. The CMR, funded by the Department of Defense in 1994 and supported as part of the Breast Cancer Surveillance Consortium by the National Cancer institute since 1995, is a mammography registry that prospectively collects data from women and radiologists in mammography facilities in community practice. Both CBCS and CMR are described in detail in Razzaghi et al.[50].
Data from the CBCS and the CMR were combined to allow for case–control and case-case analyses of mammographic density by breast cancer subtype. Briefly, CMR and CBCS were linked using probabilistic linkage with four variables; first and last name, date of birth, and last four digits of the social security number [51–53]. Breast Imaging Reporting and Data System (BI-RADS) breast density, age, and current use of hormone therapy at the time of the mammogram were collected from the CMR, and all other participant data were taken from the CBCS. The following counties from the CBCS were not represented in this study because there were no matching cases and controls in the CMR: Alamance, Orange, Wake, Johnston, Lee, Harnett, Bertie, Wilson, Edgecombe, Pitt, Pamlico, Beaufort, and Tyrell.
Tumor blocks and immunohistochemistry assays
The details of breast cancer subtyping in CBCS have been published previously [4]. Briefly, all breast cancers underwent pathology review and descriptive data including type of biopsy, tumor size, laterality, and other characteristics were abstracted from pathology reports. Three H&E-stained slides were produced from each of the paraffin blocks when slices were made for molecular and IHC analyses. These slides were reviewed in a standardized fashion by the study pathologist to confirm the diagnosis of breast cancer and to assign histologic classification [54]. The following markers were used to determine breast cancer subtypes: luminal A (ER+ and/or PR+, HER2-), luminal B (ER+ and/or PR+, HER2+), basal-like (ER-, PR-, HER2-, HER1+ and/or cytokeratin (CK)5/6+), HER2+/ER- (ER-, PR-, HER2+), and unclassified (negative for all five markers) [4, 16]. Only luminal A and basal-like cancers are examined in detail in the current analysis due to the small number of HER2+ and luminal B cases.
To determine subtype, tumor blocks were sectioned and stained for a panel of IHC markers at the IHC Core Laboratory, University of North Carolina (UNC). Commercially available antibodies to ER, HER2, HER1, and Cytokeratin 5/6 were used in this study [16, 55, 56]. For invasive cases, ER/PR status was obtained from medical records for 80% of cases and determined using IHC assays performed at UNC for the remaining cases. For 11% of the cases with missing status for ER/PR on medical records, paraffin-embedded tissues were used and ER/PR status was determined at the UNC laboratory using IHC. ER/PR status was missing for the remaining 9% of the cases [16, 54, 57].
Of the 491 cases that were in both the CMR and CBCS, 175 had missing information on subtype; the remaining cases included 181 luminal A, 17 luminal B, 48 basal-like, 29 ER-/PR-/HER2+, and 41 unclassified subtypes.
Mammographic density assessment
Mammographic density was determined by the radiologist at the time of the mammogram and recorded qualitatively in the CMR using the BI-RADS scoring system of the American College of Radiology. BI-RADS density assessment defines four categories of breast tissue composition including: 1) almost entirely fat, 2) scattered fibroglandular densities, 3) heterogeneously dense, and 4) extremely dense [58]. As discussed in Razzaghi et al.[50], for cases density was reported from the screening or diagnostic mammogram performed within five years prior to or one year after breast cancer diagnosis. Mammograms for controls were screening or diagnostic mammograms showing no cancer within five years prior to and three years after the selection date. The rationale for choosing a control group with a broader exposure window has been discussed previously [50]. Briefly, studies have shown that elevated risks of breast cancer associated with mammographic density persist for at least 5 years after a mammogram [19, 23, 59–61]. To assess whether inclusion of diagnostic mammograms for cases where screening mammograms were unavailable affected results, we previously conducted sensitivity analyses. No substantial change in effect estimates for the association between mammographic density and breast cancer risk were observed when cases with only diagnostic mammograms were excluded from analyses [50].
For women with multiple mammograms, the order of preference was (1) the mammogram prior to breast cancer diagnosis or selection date into CBCS with the date closest to diagnosis or selection date and (2) the nearest mammogram after diagnosis/selection. Studies have shown that elevated risks of breast cancer associated with mammographic density persist for at least 5 years, with studies showing lasting effects for 10 years or more for both pre- and postmenopausal women [34, 59–61]. Mammograms more than one year following treatment were excluded based on suggestions in the literature that agents used to treat breast cancer may alter mammographic density as early as 18 months after initiating therapy [62]. Mammographic density measured in the CMR is per woman and not per breast. It is expected that mammographic density measured in this way reflects risk because mammographic density is a general marker of breast cancer risk and is not specific to breast side or location of the eventual cancer [63] and because density has been shown to be highly correlated between breasts within a woman [64].
Statistical analysis
Potential confounders were selected based on prior knowledge and using directed acyclic graphs (DAGs) [65]. We adjusted for age, race, body mass index (BMI), hormone therapy (HT) use, menopausal status, first-degree family history of breast cancer, age at menarche, and parity and age at first full-term pregnancy (with the latter two combined into a single variable). We also adjusted for an offset term used in the CBCS to oversample young African American women [66].
The variable coding schemes were chosen for consistency with previous CBCS publications [4]. As there is substantial biological and epidemiologic heterogeneity between BI-RADS 1 and BI-RADS 2 categories, we did not combine density categories. Rather, we present two models: one uses BI-RADS 1 as the referent group to show the magnitude of effect comparing each category to this lowest risk group, and the other uses BI-RADS 2 as the referent group to increase the stability and/or precision of effect estimates. This sample-coding strategy also facilitates comparisons with our previously published investigation of mammographic density and breast cancer risk [50]. Race was categorized as African American or white based on self-report. Mammographic density was based on the four BI-RADS density categories. Age at diagnosis was used for cases and age at selection into the CBCS for controls and was analyzed as a continuous variable. BMI was calculated as body weight (kg)/height2 (m) and was treated as a continuous variable in the analysis. Age at first full-term pregnancy and parity/nulliparity were combined to create a categorical variable that encapsulated both parity status and age at first birth. HT was categorized as current or not-current as collected by the CMR at the time of the mammogram. Because of the association between age, HT use, and mammographic density, we also examined age and current HT use at the time of the mammogram recorded in the CMR, as explained in detail in our previous study [50]. All categorical variables were coded using indicator variables.
We used unconditional logistic regression to estimate the odds ratio (OR) and 95% CI for the association between mammographic density and breast cancer risk (SAS version 9.3, SAS Institute, Cary NC, USA). We considered basal-like and luminal A breast cancers primarily, but we also examined risk of triple-negative breast tumors (ER, PR, and HER-2-negative tumors) to facilitate comparison with previous studies on the association between mammographic density and risk of triple-negative breast cancers. Case-case analyses were used to compare the distribution of mammographic density among patients with basal-like tumors to that among patients with luminal A tumors, and to compare mammographic density among triple-negative patients to luminal A patients. Effect measure modification was not assessed, given the small sample size.
As addressed in our previous study, to assess the comparability of the CMR-CBCS merged data and the full CBCS dataset, we compared the characteristics of participants who matched to the CMR (the current dataset) to those in the entire CBCS by estimating ORs for established breast cancer risk factors. The ORs were similar in the CMR-CBCS merged dataset and the CBCS as a whole for all variables assessed [50].
Ethical considerations
Both the CMR and the CBCS were approved by the Institutional Review Board of the UNC and were conducted in compliance with the Helsinki Declaration. Specific patient-informed consent was not required for this study, since all women consented to participate in the CBCS and the program was authorized to collect and use health and clinical information from study participants for evaluation and scientific research.
Results
Characteristics of all breast cancer cases (n = 491) and women with basal-like and luminal A tumors as well as 528 controls are presented in Table 1. Compared with women with luminal A breast cancer, women with the basal-like subtype were younger, had higher BMI and waist-to-height ratio (WHR), were more likely to be African American, premenopausal, younger than 13 years at menarche, parous with first full-term pregnancy at younger than 26 years, not current HT users, users of oral contraceptives, and never having breastfed (Table 1). Thus, associations with standard risk factors showed similar patterns by subtype as reported for the CBCS overall [4].
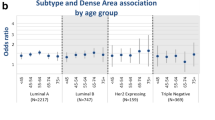
Table 2 presents the ORs and 95% CIs for adjusted models with both BI-RADS 1 (model 1) and 2 (model 2) as the reference groups. Model 1 is included to facilitate comparison with previous studies that have reported risk for the BI-RADS 4 group who had ‘extremely dense’ breast tissue, relative to the BI-RADS 1 group who had ‘entirely fatty’ breast tissue, but model 2 allows for more precise estimates due to a larger referent group. Among all women, those with extremely dense breasts had an increased risk of breast cancer compared to women with entirely fatty breasts and those with scattered fibroglandular densities (OR 2.45, 95% CI 0.99, 6.09, and OR 1.19, 95% CI 0.72, 1.95, respectively) (Table 2). Model 1 resulted in a stronger positive case–control association between mammographic density and breast cancer risk for the basal-like subtype compared to the luminal A subtype (OR 3.6, 95% CI 0.34, 37.97, and OR 1.98, 95% CI 0.54, 7.34, respectively). These associations were of weaker magnitude when using model 2, and associations were of similar magnitude for the basal-like and luminal A subtypes (OR 1.04, 95% CI 0.34, 3.17, and OR 0.98, 95% CI 0.50, 1.92, respectively) (Table 2). These results suggest no heterogeneity of breast cancer risk according to intrinsic subtype; however, the estimates were generally imprecise as evidenced by the wide confidence intervals.
To facilitate comparisons with previous studies of mammographic density by breast cancer subtype [26, 30, 39, 45], we also examined the association between density and breast cancer risk in case–control analyses using the triple-negative definition of breast cancer. Model 1 resulted in a large, imprecise estimate for risk of triple negative breast cancer, and model 2 resulted in a higher odds ratio than previously observed for basal-like or luminal A breast cancers (OR 1.20, 95% CI 0.49, 2.90) (Table 2). To directly compare basal-like/triple-negative to luminal A breast cancers, we used case-case analyses for model 2 (Table 3). As expected based on case–control analyses, there were no statistically significant differences between basal-like and luminal A, or between triple-negative and luminal A breast cancers (OR 1.08, 95% CI 0.30, 3.84, and OR 1.17, 95% CI 0.41, 3.35, respectively) in relation to mammographic density. However, it is important to note that all of these case-case analyses are imprecise due to small case numbers. Thus, based on these findings, there was no suggestion of etiologic heterogeneity with respect to mammographic density and subtype.
Discussion
Recent findings of decreased involution of terminal duct lobular units (TDLU) surrounding basal-like breast cancers [48] have renewed interest in evaluating the association between mammographic density and subtype-specific breast cancer risk. TDLU involution has been inversely associated with mammographic density [49], leading to the hypothesis that density may be higher among basal-like breast cancers. Previous studies evaluating the relation between mammographic density and breast cancer subtype have not supported this hypothesis, but these studies have had significant potential for outcome misclassification, given the lack of positive markers for basal-like breast cancer [67]. ER-negative tumors are clinically heterogeneous, including HER2-positive, basal-like, and unclassified tumors. Therefore, further stratification of these tumors and identification of basal-like tumors as distinct from triple-negative tumors (where all markers failed to show positivity) could help improve estimates of the true associations. However, even using five markers in case–control analyses, we observed no difference in the association between mammographic density and breast cancer for luminal A, basal-like or triple-negative breast cancers.
Furthermore, our estimates from case-case analysis, which can be interpreted as ratios of ORs between the two subtypes of breast cancer (luminal A and basal-like), directly estimated the relative strength of association between the two breast cancer subtypes and showed no significant difference between basal-like and luminal A or triple-negative and luminal A breast cancers, similar to previous results [25, 30, 39]. Considering previous case-only studies, eleven of the thirteen studies that examined mammographic density by hormone receptor status concluded that there were no significant differences [36–46]; only four of these studies (all null) examined the association using breast cancer subtypes including the triple-negative subtype [30, 40, 45, 46]. Our previous findings [50] showed that mammographic density was positively associated with breast cancer risk overall; here, the stratified analyses for both luminal A and basal-like breast cancers show similar effect estimates, such that mammographic density is a risk factor for both subtypes with no evidence of heterogeneity by tumor subtype. Using intrinsic subtypes of breast cancer, our findings were largely consistent with the majority of prior studies evaluating the relation between mammographic density and breast cancer risk by molecular subtypes of breast cancer.
It is possible that there are genetic and heritable factors that alter mammographic density and breast cancer risk overall, and are therefore responsible for the association of mammographic density and breast cancer regardless of breast cancer subtype [68]. For example, heritable differences in exposure or response to hormones and growth factors may increase proliferative activity and quantities of stromal and epithelial tissue, with effects on both mammographic density and breast cancer risk across all subtypes [68, 69]. Consistent with this, two of fourteen established breast cancer susceptibility loci examined in a recent study contributed to between-woman differences in mammographic density [70]. This finding suggests a model that considers mammographic density as an integrated marker of many different hormonal and non-hormonal influences on breast tissue composition, and is also supported by work examining relationships between mammographic density and non-genetic breast cancer risk factors.
In contrast to mammographic density, many well-established breast cancer risk factors have shown opposite effects on basal-like and luminal A subtypes of breast cancer [4]. For example, Millikan et al. identified risk factors for the basal-like subtype, including younger age at diagnosis, higher parity, younger age at first full-term pregnancy, shorter duration of breastfeeding, fewer number of children breastfed, fewer number of months breastfeeding per child, and increased WHR ratio [4]. Many other studies have confirmed similar heterogeneity by anthropometric and reproductive factors [10, 71–75]. Because many of these variables that have distinct associations with breast cancer subtypes also impact mammographic density, we might have expected to see differences in the association between mammographic density and breast cancer subtype. For example, young age at first full-term pregnancy is associated with lower mammographic density [76] and a reduction in risk for luminal A breast cancers [17]. However, it appears that mammographic density does not have an association with subtypes that is independent of these factors. In our models that controlled for these as potential confounders, there was no evidence of heterogeneity of the association between mammographic density and breast cancer by subtype.
Major strengths of our study were reduced outcome misclassification through use of five markers to identify breast cancer subtypes (ER, PR, HER2, HER1 and CK5/6) and linkage of established datasets to allow for a relatively large study for assessing this association. However, we note that in the years since the subtyping was performed on CBCS Phase I and Phase II, several improvements have been made to further delineate luminal A and luminal B breast cancers. For example, the classification for luminal B tumors has improved by using the Ki67 index (percentage of Ki67-positive cancer nuclei) [76]. Ideally, these newer markers could be added to improve identification of luminal B in CBCS 1 and 2, but we have emphasized luminal A tumors. Results by Bastien et al.[9] show that ER, PR and HER2 staining are relatively homogeneous within luminal A cancers (more than 93% and 94% of luminal A cancers are ER- and PR-positive, respectively, and more than 99% of these tumors are HER2-negative). Therefore, it is unlikely that changes in classification schema would substantially bias the estimates for luminal A reported herein. Moreover, results from Bastien et al. also show that standard clinical marker, such as grade, cannot capture the same qualitative information that IHC for Ki-67 would obtain. Therefore, further delineation of luminal B tumors was not conducted in this study. Because of our stratification of breast cancers into many groups, we share a limitation of most studies by molecular subtype, namely, small sample size within strata resulting in imprecise effect-measure estimates for each subtype. In addition, menopausal status or other hormonal exposures may be important in determining the effects of mammographic density on breast cancer risk, but we were underpowered to study effect-measure modification and did not attempt these analyses. Although our study is limited by small sample size, this study is the first to have used molecular subtypes to identify basal-like breast cancers. A pooled analysis or meta-analysis of the association between mammographic density and breast cancer subtypes would provide a larger sample size; however, this will only be possible if future studies differentiate between basal-like and triple-negative breast cancers.
Many recent studies have emphasized etiologic heterogeneity by intrinsic subtype. It is important to recognize that intrinsic subtype classification was greatly influenced by clinical needs and is based on heterogeneity of tumors long after the etiologically relevant window has passed. Many genomic changes occurring late in tumor progression may not be relevant from an etiologic perspective. While some studies have found that there is etiologic heterogeneity, pathogenesis of each subtype is not well-defined and other markers of heterogeneity may be more relevant for a given exposure. For example, tumor characteristics that reflect proliferation or response to DNA damage may be important if the mechanism of density-associated risk is mitogenesis or mutagenesis (as suggested by Martin et al. [68]). Alternatively, factors such as hormone receptor status may be more important etiologically than intrinsic subtype.
Future studies of breast cancer subtypes and mammographic density by race are desirable, particularly given that basal-like breast cancers are more prevalent in African American women and appear to have distinct etiology. However, based on current data, there is little evidence to support differences in the effect of mammographic density by breast cancer subtype.
Conclusions
Using five markers in case–control analyses, we observed no difference in the association between mammographic density and breast cancer for luminal A, basal-like or triple-negative breast cancers. Furthermore, our estimates from case-case analysis, which directly estimated the relative strength of association between the two breast cancer subtypes, showed no significant difference between basal-like and luminal A, or triple-negative and luminal A breast cancers.
Abbreviations
- BI-RADS:
-
Breast Imaging Reporting and Data System
- BMI:
-
Body mass index
- CBCS:
-
Carolina Breast Cancer Study
- CK5/6:
-
cytokeratin 5/6
- CMR:
-
Carolina Mammography Registry
- DAG:
-
Directed acyclic graph
- ER:
-
Estrogen receptor
- H&E:
-
Hematoxylin and eosin
- HER:
-
Human epidermal growth factor receptor
- HT:
-
Hormone therapy
- IHC:
-
Immunohistochemical
- OR:
-
Odds ratio
- PR:
-
Progesterone receptor
- TDLU:
-
Terminal duct lobular units
- UNC:
-
University of North Carolina
- WHR:
-
Waist-to-height ratio.
References
Perou CM, Sorlie T, Eisen MB, Van de Rijn M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA, Fluge O, Pergamenschikov A, Williams C, Zhu SX, Lonning PE, Borresen-Dale AL, Brown PO, Botstein D: Molecular portraits of human breast tumours. Nature. 2000, 406: 747-752. 10.1038/35021093.
Sorlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, Hastie T, Eisen MB, Van de Rijn M, Jeffrey SS, Thorsen T, Quist H, Matese JC, Brown PO, Botstein D, Lonning PE, Borresen-Dale AL: Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA. 2001, 98: 10869-10874. 10.1073/pnas.191367098.
Sorlie T, Tibshirani R, Parker J, Hastie T, Marron JS, Nobel A, Deng S, Johnsen H, Pesich R, Geisler S, Demeter J, Perou CM, Lonning PE, Brown PO, Borresen-Dale AL, Botstein D: Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci USA. 2003, 100: 8418-8423. 10.1073/pnas.0932692100.
Millikan RC, Newman B, Tse CK, Moorman PG, Conway K, Dressler LG, Smith LV, Labbok MH, Geradts J, Bensen JT, Jackson S, Nyante S, Livasy C, Carey L, Earp HS, Perou CM: Epidemiology of basal-like breast cancer. Breast Cancer Res Treat. 2008, 109: 123-139. 10.1007/s10549-007-9632-6.
Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S, et al: Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006, 295: 2492-2502. 10.1001/jama.295.21.2492.
Sorlie T: Molecular portraits of breast cancer: tumour subtypes as distinct disease entities. Eur J Cancer. 2004, 40: 2667-2675. 10.1016/j.ejca.2004.08.021.
Kwan ML, Kushi LH, Weltzien E, Maring B, Kutner SE, Fulton RS, Lee MM, Ambrosone CB, Caan BJ: Epidemiology of breast cancer subtypes in two prospective cohort studies of breast cancer survivors. Breast Cancer Res. 2009, 11: R31-10.1186/bcr2261.
Phipps AI, Chlebowski RT, Prentice R, McTiernan A, Wactawski-Wende J, Kuller LH, Adams-Campbell LL, Lane D, Stefanick ML, Vitolins M, Kabat GC, Rohan TE, Li CI: Reproductive history and oral contraceptive use in relation to risk of triple-negative breast cancer. J Natl Cancer Inst. 2011, 103: 470-477. 10.1093/jnci/djr030.
Yang XR, Pfeiffer RM, Garcia-Closas M, Rimm DL, Lissowska J, Brinton LA, Peplonska B, Hewitt SM, Cartun RW, Mandich D, Sasano H, Evans DB, Sutter TR, Sherman ME: Hormonal markers in breast cancer: coexpression, relationship with pathologic characteristics, and risk factor associations in a population-based study. Cancer Res. 2007, 67: 10608-10617. 10.1158/0008-5472.CAN-07-2142.
Yang XR, Chang-Claude J, Goode EL, Couch FJ, Nevanlinna H, Milne RL, Gaudet M, Schmidt MK, Broeks A, Cox A, Fasching PA, Hein R, Spurdle AB, Blows F, Driver K, Flesch-Janys D, Heinz J, Sinn P, Vrieling A, Heikkinen T, Aittomaki K, Heikkila P, Blomqvist C, Lissowska J, Peplonska B, Chanock S, Figueroa J, Brinton L, Hall P, Czene K, et al: Associations of breast cancer risk factors with tumor subtypes: a pooled analysis from the Breast Cancer Association Consortium studies. J Natl Cancer Inst. 2011, 103: 250-263. 10.1093/jnci/djq526.
Broeks A, Schmidt MK, Sherman ME, Couch FJ, Hopper JL, Dite GS, Apicella C, Smith LD, Hammet F, Southey MC, Van’t Veer LJ, de Groot R, Smit VT, Fasching PA, Beckmann MW, Jud S, Ekici AB, Hartmann A, Hein A, Schulz-Wendtland R, Burwinkel B, Marme F, Schneeweiss A, Sinn HP, Sohn C, Tchatchou S, Bojesen SE, NOrdestgaard BG, Flyger H, Orsted DD, et al: Low penetrance breast cancer susceptibility loci are associated with specific breast tumor subtypes: findings from the Breast Cancer Association Consortium. Hum Mol Genet. 2011, 20: 3289-3303. 10.1093/hmg/ddr228.
Phipps AI, Chlebowski RT, Prentice R, McTiernan A, Stefanick ML, Wactawski-Wende J, Kuller LH, Adams-Campbell LL, Lane D, Vitolins M, Kabat GC, Rohan TE, Li CI: Body size, physical activity, and risk of triple-negative and estrogen receptor-positive breast cancer. Cancer Epidemiol Biomarkers Prev. 2011, 20: 454-463. 10.1158/1055-9965.EPI-10-0974.
Phipps AI, Buist DS, Malone KE, Barlow WE, Porter PL, Kerlikowske K, Li CI: Reproductive history and risk of three breast cancer subtypes defined by three biomarkers. Cancer Causes Control. 2011, 22: 399-405. 10.1007/s10552-010-9709-0.
Ma H, Wang Y, Sullivan-Halley J, Weiss L, Marchbanks PA, Spirtas R, Ursin G, Burkman RT, Simon MS, Malone KE, Strom BL, McDonald JA, Press MF, Berstein L: Use of four biomarkers to evaluate the risk of breast cancer subtypes in the women's contraceptive and reproductive experiences study. Cancer Res. 2010, 70: 575-587. 10.1158/0008-5472.CAN-09-3460.
Bertucci F, Finetti P, Cervera N, Charafe Jauffret E, Buttarelli M, Jacquemier J, Chaffanet M, Maraninchi D, Viens P, Birnbaum D: How different are luminal A and basal breast cancers?. Int J Cancer. 2009, 124: 1338-1348. 10.1002/ijc.24055.
Reis Filho JS, Tutt ANJ: Triple negative tumours: a critical review. Histopathology. 2008, 52: 108-118.
McCormack VA, dos Santos SI: Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2006, 15: 1159-1169. 10.1158/1055-9965.EPI-06-0034.
Vachon CM, Brandt KR, Ghosh K, Scott CG, Maloney SD, Carston MJ, Pankratz VS, Sellers TA: Mammographic breast density as a general marker of breast cancer risk. Cancer Epidemiol Biomarkers Prev. 2007, 16: 43-49. 10.1158/1055-9965.EPI-06-0738.
Boyd NF, Byng JW, Jong RA, Fishell EK, Little LE, Miller AB, Lockwood GA, Tritchler DL, Yaffe MJ: Quantitative classification of mammographic densities and breast cancer risk: results from the Canadian National Breast Screening Study. J Natl Cancer Inst. 1995, 87: 670-675. 10.1093/jnci/87.9.670.
Ziv E, Shepherd J, Smith-Bindman R, Kerlikowske K: Mammographic breast density and family history of breast cancer. J Natl Cancer Inst. 2003, 95: 556-558. 10.1093/jnci/95.7.556.
Boyd NF, Lockwood GA, Martin LJ, Knight JA, Byng JW, Yaffe MJ, Tritchler DL: Mammographic densities and breast cancer risk. Breast Dis. 1998, 10: 113-126.
Ursin G, Ma H, Wu AH, Bernstein L, Salane M, Parisky YR, Astrahan M, Siozon CC, Pike MC: Mammographic density and breast cancer in three ethnic groups. Cancer Epidemiol Biomarkers Prev. 2003, 12: 332-338.
Maskarinec G, Pagano I, Lurie G, Wilkens LR, Kolonel LN: Mammographic density and breast cancer risk: the multiethnic cohort study. Am J Epidemiol. 2005, 162: 743-752. 10.1093/aje/kwi270.
Brisson J, Merletti F, Sadowsky NL, Twaddle JA, Morrison AS, Cole P: Mammographic features of the breast and breast cancer risk. Am J Epidemiol. 1982, 115: 428-437.
Boyd NF, Martin LJ, Yaffe MJ, Minkin S: Mammographic density and breast cancer risk: current understanding and future prospects. Breast Cancer Res. 2011, 13: 223-10.1186/bcr2942.
Ma H, Luo J, Press MF, Wang Y, Bernstein L, Ursin G: Is there a difference in the association between percent mammographic density and subtypes of breast cancer? Luminal A and triple-negative breast cancer. Cancer Epidemiol Biomarkers Prev. 2009, 18: 479-485. 10.1158/1055-9965.EPI-08-0805.
Ziv E, Tice J, Smith-Bindman R, Shepherd J, Cummings S, Kerlikowske K: Mammographic density and estrogen receptor status of breast cancer. Cancer Epidemiol Biomarkers Prev. 2004, 13: 2090-2095.
Olsen AH, Bihrmann K, Jensen MB, Vejborg I, Lynge E: Breast density and outcome of mammography screening: a cohort study. Br J Cancer. 2009, 100: 1205-1208. 10.1038/sj.bjc.6604989.
Yaghjyan L, Colditz GA, Collins LC, Schnitt SJ, Rosner B, Vachon C, Tamimi RM: Mammographic breast density and subsequent risk of breast cancer in postmenopausal women according to tumor characteristics. J Natl Cancer Inst. 2011, 103: 1179-1189. 10.1093/jnci/djr225.
Phipps A, Buist DSM, Malone K, Barlow W, Porter P, Kerlikowske K, O'Meara E, Li C: Breast density, body mass index, and risk of tumor marker-defined subtypes of breast cancer. Ann Epidemiol. 2012, 22: 340-348.
Pollan M, Ascunce N, Ederra M, Murillo A, Erdozain N, Ales Martinez J, Pastor Barriuso R: Mammographic density and risk of breast cancer according to tumor characteristics and mode of detection: a Spanish population-based case–control study. Breast Cancer Res. 2013, 15: R9-10.1186/bcr3380.
Ding J, Warren R, Girling A, Thompson D, Easton D: Mammographic density, estrogen receptor status and other breast cancer tumor characteristics. Breast J. 2010, 16: 279-289. 10.1111/j.1524-4741.2010.00907.x.
Conroy SM, Pagano I, Kolonel LN, Maskarinec G: Mammographic density and hormone receptor expression in breast cancer: the Multiethnic Cohort Study. Cancer Epidemiol. 2011, 35: 448-452. 10.1016/j.canep.2010.11.011.
Hinton CP, Roebuck EJ, Williams MR, Blamey RW, Glaves J, Nicholson RI, Griffiths K: Mammographic parenchymal patterns: value as a predictor of hormone dependency and survival in breast cancer. AJR Am J Roentgenol. 1985, 144: 1103-1107. 10.2214/ajr.144.6.1103.
Heusinger K, Jud SM, Haberle L, Hack CC, Fasching PA, Meier-Meitinger M, Lux MP, Hagenbeck C, Loehberg CR, Wittenberg T, Rauh C, Wagner F, Uder M, Harmann A, Schulz-Wendtland R, Beckmann MW, Wachter DL: Association of mammographic density with the proliferation marker Ki-67 in a cohort of patients with invasive breast cancer. Breast Cancer Res Treat. 2012, 135: 885-892. 10.1007/s10549-012-2221-3.
Morishita M, Ohtsuru A, Hayashi T, Isomoto I, Itoyanagi N, Maeda S, Honda S, Yano H, Uga T, Nagayasu T, Kanematsu T, Yamashita S: Clinical significance of categorisation of mammographic density for breast cancer prognosis. Int J Oncol. 2005, 26: 1307-1312.
Ghosh K, Brandt KR, Sellers TA, Reynolds C, Scott CG, Maloney SD, Carston MJ, Pankratz VS, Vachon CM: Association of mammographic density with the pathology of subsequent breast cancer among postmenopausal women. Cancer Epidemiol Biomarkers Prev. 2008, 17: 872-879. 10.1158/1055-9965.EPI-07-0559.
Chen JH, Hsu FT, Shih HN, Hsu CC, Chang D, Nie K, Nalcioglu O, Su MY: Does breast density show difference in patients with estrogen receptor-positive and estrogen receptor-negative breast cancer measured on MRI?. Ann Oncol. 2009, 20: 1447-1449. 10.1093/annonc/mdp362.
Yang WT, Dryden M, Broglio K, Gilcrease M, Dawood S, Dempsey PJ, Valero V, Hortobagyi G, Atchley D, Arun B: Mammographic features of triple receptor-negative primary breast cancers in young premenopausal women. Breast Cancer Res Treat. 2008, 111: 405-410. 10.1007/s10549-007-9810-6.
Arora N, King TA, Jacks LM, Stempel MM, Patil S, Morris E, Morrow M: Impact of breast density on the presenting features of malignancy. Ann Surg Oncol. 2010, 17 (Suppl 3): 211-218.
Cil T, Fishell E, Hanna W, Sun P, Rawlinson E, Narod SA, McCready DR: Mammographic density and the risk of breast cancer recurrence after breast-conserving surgery. Cancer. 2009, 115: 5780-5787. 10.1002/cncr.24638.
Roubidoux MA, Bailey JE, Wray LA, Helvie MA: Invasive cancers detected after breast cancer screening yielded a negative result: relationship of mammographic density to tumor prognostic factors. Radiology. 2004, 230: 42-48. 10.1148/radiol.2301020589.
Aiello EJ, Buist DS, White E, Porter PL: Association between mammographic breast density and breast cancer tumor characteristics. Cancer Epidemiol Biomarkers Prev. 2005, 14: 662-668. 10.1158/1055-9965.EPI-04-0327.
Fasching P, Heusinger K, Loehberg C, Wenkel E, Lux M, Schrauder M, Koscheck T, Bautz W, Schulz-Wendtland R, Beckmann M, Bani M: Influence of mammographic density on the diagnostic accuracy of tumor size assessment and association with breast cancer tumor characteristics. Eur J Radiol. 2006, 60: 398-404. 10.1016/j.ejrad.2006.08.002.
Eriksson L, Hall P, Czene K, Dos Santos Silva I, McCormack V, Bergh J, Bjohle J, Ploner A: Mammographic density and molecular subtypes of breast cancer. Br J Cancer. 2012, 107: 18-23. 10.1038/bjc.2012.234.
Gierach GL, Lissowska J, Garcia-Closas M, Yang XR, Figuero JD, Anzick S, Wesolowska E, Brinton LA, Meltzer PS, Boyd NF, Sherman ME: Relationship of mammographic density with breast cancer subtypes [Abstract]. American Association for Cancer Research. 2010, 2779-
Antoni S, Sasco AJ, dos Santos Silva I, McCormack V: Is mammographic density differentially associated with breast cancer according to receptor status? A meta-analysis. Breast Cancer Res Treat. 2013, 137: 337-347. 10.1007/s10549-012-2362-4.
Yang X, Figueroa J, Falk R, Zhang H, Pfeiffer R, Hewitt S, Lissowska J, Peplonska B, Brinton L, Garcia Closas M, Sherman M: Analysis of terminal duct lobular unit involution in luminal A and basal breast cancers. Breast Cancer Res. 2012, 14: R64-10.1186/bcr3170.
Ghosh K, Hartmann LC, Reynolds C, Visscher DW, Brandt KR, Vierkant RA, Scott CG, Radisky DC, Sellers TA, Pankratz VS, Vachon CM: Association between mammographic density and age-related lobular involution of the breast. J Clin Oncol. 2010, 28: 2207-2212. 10.1200/JCO.2009.23.4120.
Razzaghi H, Troester M, Gierach G, Olshan A, Yankaskas B, Millikan R: Mammographic density and breast cancer risk in White and African American Women. Breast Cancer Res Treat. 2012, 135: 571-580. 10.1007/s10549-012-2185-3.
Gomatam S, Carter R, Ariet M, Mitchell G: An empirical comparison of record linkage procedures. Stat Med. 2002, 21: 1485-1496. 10.1002/sim.1147.
Jaro MA: Probabilistic linkage of large public health data files. Stat Med. 1995, 14: 491-498. 10.1002/sim.4780140510.
Quantin C, Binquet C, Bourquard K, Pattisina R, Gouyon-Cornet B, Ferdynus C, Gouyon J-B, François André A: Which are the best identifiers for record linkage?. Med Informatics Internet Medicine. 2004, 29: 221-227. 10.1080/14639230400005974.
Newman B, Moorman PG, Millikan R, Qaqish BF, Geradts J, Aldrich TE, Liu ET: The Carolina Breast Cancer Study: integrating population-based epidemiology and molecular biology. Breast Cancer Res Treat. 1995, 35: 51-60. 10.1007/BF00694745.
Livasy CA, Perou CM, Karaca G, Cowan DW, Maia D, Jackson S, Tse CK, Nyante S, Millikan RC: Identification of a basal-like subtype of breast ductal carcinoma in situ. Hum Pathol. 2007, 38: 197-204. 10.1016/j.humpath.2006.08.017.
O'Brien KM, Cole SR, Tse CK, Perou CM, Carey LA, Foulkes WD, Dressler LG, Geradts J, Millikan RC: Intrinsic breast tumor subtypes, race, and long-term survival in the Carolina Breast Cancer Study. Clin Cancer Res. 2010, 16: 6100-6110. 10.1158/1078-0432.CCR-10-1533.
Huang WY, Newman B, Millikan RC, Schell MJ, Hulka BS, Moorman PG: Hormone-related factors and risk of breast cancer in relation to estrogen receptor and progesterone receptor status. Am J Epidemiol. 2000, 151: 703-714. 10.1093/oxfordjournals.aje.a010265.
Liberman L, Menell J: Breast imaging reporting and data system (BI-RADS). Radiol Clin North Am. 2002, 40: 409-430. 10.1016/S0033-8389(01)00017-3.
Byrne C, Schairer C, Wolfe J, Parekh N, Salane M, Brinton LA, Hoover R, Haile R: Mammographic features and breast cancer risk: effects with time, age, and menopause status. J Natl Cancer Inst. 1995, 87: 1622-1629. 10.1093/jnci/87.21.1622.
Kato I, Beinart C, Bleich A, Su S, Kim M, Toniolo PG: A nested case–control study of mammographic patterns, breast volume, and breast cancer (New York City, NY, United States). CCC Cancer Causes Control. 1995, 6: 431-438. 10.1007/BF00052183.
Thomas D, Carter R, Bush W, Ray R, Stanford J, Lehman C, Daling J, Malone K, Davis S: Risk of subsequent breast cancer in relation to characteristics of screening mammograms from women less than 50 years of age. Cancer Epidemiol Biomarkers Prev. 2002, 11: 565-571.
Cuzick J, Warwick J, Pinney E, Warren RML, Duffy S: Tamoxifen and breast density in women at increased risk of breast cancer. J Natl Cancer Inst. 2004, 96: 621-628. 10.1093/jnci/djh106.
Vachon CM, van Gils CH, Sellers TA, Ghosh K, Pruthi S, Brandt KR, Pankratz VS: Mammographic density, breast cancer risk and risk prediction. Breast Cancer Res. 2007, 9: 217-10.1186/bcr1829.
Yaffe MJ, Boyd NF, Byng JW, Jong RA, Fishell E, Lockwood GA, Little LE, Tritchler DL: Breast cancer risk and measured mammographic density. Eur J Cancer Prev. 1998, 7 (Suppl 1): S47-S55.
Greenland S, Pearl J, Robins JM: Causal diagrams for epidemiologic research. Epidemiology. 1999, 10: 37-48. 10.1097/00001648-199901000-00008.
Weinberg CR, Sandler DP: Randomized recruitment in case–control studies. Am J Epidemiol. 1991, 134: 421-432.
Nielsen T, Hsu F, Jensen K, Cheang M, Karaca G, Hu Z, Hernandez Boussard T, Livasy C, Cowan D, Dressler L, Akslen L, Ragaz J, Gown A, Gilks CB, Van de Rijn M, Perou C: Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res. 2004, 10: 5367-5374. 10.1158/1078-0432.CCR-04-0220.
Martin LJ, Boyd NF: Mammographic density. Potential mechanisms of breast cancer risk associated with mammographic density: hypotheses based on epidemiological evidence. Breast Cancer Res. 2008, 10: 201-10.1186/bcr1831.
Boyd NF, Rommens JM, Vogt K, Lee V, Hopper JL, Yaffe MJ, Paterson AD: Mammographic breast density as an intermediate phenotype for breast cancer. Lancet Oncol. 2005, 6: 798-808. 10.1016/S1470-2045(05)70390-9.
Vachon CM, Scott CG, Fasching PA, Hall P, Tamimi RM, Li J, Stone J, Apicella C, Odefrey F, Gierach GL, Jud SM Heusinger K, Beckmann MW, Pollan M, Fernandez-Navarro P, Gonzalez-Neira A, Benitez J, Van Gils CH, Lokate M, Onland-Moret NC, Peeters PH, Brown J, Leyland J, Varghese JS, Easton DF, Thompson DJ, Luben RN, Warren RM, Wareham NJ, Loos RJ, et al: Common breast cancer susceptibility variants in LSP1 and RAD51L1 are associated with mammographic density measures that predict breast cancer risk. Cancer Epidemiol Biomarkers Prev. 2012, 21: 1156-1166. 10.1158/1055-9965.EPI-12-0066.
Palmer J, Boggs D, Wise L, Ambrosone C, Adams Campbell L, Rosenberg L: Parity and lactation in relation to estrogen receptor negative breast cancer in African American women. Cancer Epidemiol Biomarkers Prev. 2011, 20: 1883-1891. 10.1158/1055-9965.EPI-11-0465.
Kwan M, Chen W, Kroenke C, Weltzien E, Beasley J, Nechuta S, Poole E, Lu W, Holmes M, Quesenberry C, Pierce J, Shu X, Caan B: Pre-diagnosis body mass index and survival after breast cancer in the After Breast Cancer Pooling Project. Breast Cancer Res Treat. 2012, 132: 729-739. 10.1007/s10549-011-1914-3.
Turkoz FP, Solak M, Petekkaya I, Keskin O, Kertmen N, Sarici F, Arik Z, Babacan T, Ozisik Y, Altundag K: Association between common risk factors and molecular subtypes in breast cancer patients. Breast. 2013, 22: 344-350. 10.1016/j.breast.2012.08.005.
Tamimi R, Colditz G, Hazra A, Baer H, Hankinson S, Rosner B, Marotti J, Connolly J, Schnitt S, Collins L: Traditional breast cancer risk factors in relation to molecular subtypes of breast cancer. Breast Cancer Res Treat. 2012, 131: 159-167. 10.1007/s10549-011-1702-0.
Devi CRB, Tang TS, Corbex M: Incidence and risk factors for breast cancer subtypes in three distinct South-East Asian ethnic groups: Chinese, Malay and natives of Sarawak, Malaysia. Int J Cancer. 2012, 131: 2869-2877. 10.1002/ijc.27527.
Rauh C, Faschingbauer F, Haeberle L, Jud SM, Heusinger K, Fasching PA, Goecke TW, Rajakaruna N, Voigt F, Bani MR, Lux MP, Renner SP, Loehberg CR, Hartmann A, Schulz-Wendtland R, Beckmann MW, Bayer CM: Factors influencing breast changes after pregnancy. Eur J Cancer Prev. 2012, 3: 259-261.
Acknowledgements
The authors are grateful to Jessica Tse and Robert Christopher Allis for their assistance with data management and data analysis for this manuscript. This research was supported (in part) by the Intramural Research Program of the NIH and the National Cancer Institute. MAT was supported by the National Institute Breast Cancer and the Environment Research Program 5U01ES019472-02 and NCI grant 5R01CA138255. MAT is also supported by a SPORE in Breast Cancer 5P50CA058233.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HR designed the study, carried out the analysis, and drafted the manuscript. MAT participated in study design, analysis, and the manuscript draft. GLG participated in study design and provided expertise in mammographic density. RCM participated in study design and provided expertise in breast cancer subtypes. BCY and AFO participated in study design. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Razzaghi, H., Troester, M.A., Gierach, G.L. et al. Association between mammographic density and basal-like and luminal A breast cancer subtypes. Breast Cancer Res 15, R76 (2013). https://doi.org/10.1186/bcr3470
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/bcr3470