
Abstract
Immunocytochemical or molecular assays allow the detection of single disseminated tumor cells (DTCs) in the bone marrow (BM) or the peripheral blood in 10% to 60% of breast cancer patients without signs of metastasis. Results from recently reported studies suggest that circulating tumor cell (CTC) levels may serve as a prognostic marker and be used for early assessment of therapeutic response in patients with metastatic breast cancer. In early stage breast cancer, however, the impact of CTCs is less well established than that of DTCs in BM, where several clinical studies demonstrated that such cells are an independent prognostic factor at primary diagnosis. The characterization of DTCs/CTCs has already shed new light on the complex process underlying early tumor cell dissemination and metastatic progression in cancer patients. Characterization of DTCs should help to identify novel targets for biological therapies aimed to prevent metastatic relapse. In addition, understanding tumor 'dormancy' and identifying metastatic stem cells might result in the development of new therapeutic concepts.
Similar content being viewed by others

Introduction
Early spread of tumor cells usually remains undetected in breast cancer patients even by conventional histopathological analysis and high-resolution imaging technologies. Therefore, sensitive immunocytochemical and molecular assays have been developed that now allow the specific detection of 'occult' metastatic tumor cells at the single-cell stage in the regional lymph nodes, peripheral blood and bone marrow (BM) before the occurrence of incurable overt metastases.
Early detection of disseminated tumor cells (DTCs) might help to identify patients in need of additional systemic therapies after successful surgical resection of the primary tumor. Although all of these therapies are aimed to prevent metastatic relapse, the selection of patients is at present based on their statistical risk of developing tumor recurrence, without knowing whether they actually harbor any DTCs. This uncertainty leads to overtreatment of cancer patients with toxic agents that exert severe side effects. Based on these considerations, it will not be sufficient to simply characterize the primary tumor as a therapeutic target, but it will also be essential to include DTCs in the analysis. This information is important, in particular, for the design of clinical trials using biological therapies directed against specific targets. Sequential screening and monitoring of BM and blood samples could provide early information about the therapeutic efficacy of the tested drug against the DTCs. Clearance of DTCs from BM and/or tumor cells circulating in the blood could serve as an intermediate endpoint in clinical trials with anticancer agents. Further molecular and functional description of these cells will be essential to develop and select more efficient forms of systemic therapy.
Although the detection of DTCs in lymph nodes is also an interesting topic, especially in the context of sentinel lymph node analyses [1–3], this article will focus on the detection, molecular characterization and clinical relevance of hematogeneous tumor cell spread as the most crucial step in breast cancer progression.
Methods for the detection of disseminated tumor cells
Immunocytochemical staining
Several different assays have been developed to detect DTCs in breast cancer and other types of carcinomas. One major approach to identify DTCs is immunocytochemical staining with monoclonal antibodies against epithelial or tumor-associated antigens [4–7]. To date, cytokeratins (CKs) have become the most widely accepted protein markers for the detection of epithelial tumor cells in mesenchymal tissues such as BM, blood or lymph nodes [8–10]; however, different staining techniques can result in specificity variations [11, 12]. Several international organizations have therefore recognized the need for standardization of the immunocytochemical assay and for its evaluation in prospective studies [13–15].
Immunocytochemical analysis is usually used in combination with density gradient centrifugation, immunomagnetic procedures or size filtration methods to enrich tumor cells prior to their detection (Figure 1) [16–19]. One way to improve current detection assays for single tumor cells is to develop better tumor cell enrichment procedures using improved density gradients [20] and antibody-coupled magnetic particles [21–23]. At present it is unclear whether these new enrichment techniques provide more clinically relevant information than the standard density gradient procedure used to isolate the mononuclear cell fraction (Figure 1).

Immunocytochemical detection of disseminated tumor cells (DTCs) in the bone marrow of patients with epithelial tumors. The detection process begins with Ficoll density gradient centrifugation to isolate mononuclear cells (MNC) and uses cytokeratin (CK) antibodies. The detection of the stained DTCs can be performed automatically and suspect cells are displayed in an image gallery.
The use of new automated devices for the microscopic screening of immunostained slides may help to read slides more rapidly and to increase reproducibility of the read-out [21, 24–28] (Figure 1). Among the commercially available automated systems, the CellSearch™ system has gained considerable attention because it allows automated immunomagnetic enrichment and CK staining of blood samples [29].
A recent validation study demonstrated that the recovery rate of spiked samples averaged between 80% and 82%. Circulating tumor cells (CTCs) were detected in approximately 70% of metastatic breast cancer patients. When analyzing identical samples in different centers, inter-instrument accordance was high. Thus, multicenter studies with shipment of samples are possible. However, the system is restricted to the enrichment of epithelial cell adhesion molecule (EpCAM) positive CTCs and EpCAM expression can be lost or downregulated as a consequence of an epithelial to mesenchymal transition [30, 31]. In addition, the number of images that need to be manually checked on the instrument is rather high and increases with the storage time of the sample [32], which limits the throughput of CTC measurements.
PCR approach for the detection of disseminated tumor cells
A widely used alternative to immunocytochemical assays for the detection of DTCs comprises molecular detection procedures. In principle, the nucleic acid in a sample can be amplified by PCR, so that very small numbers of tumor cells can be detected in a heterogeneous population of cells. However, the tumor cells must have changes in DNA or mRNA expression patterns that distinguish them from the surrounding hematopoietic cells. At the DNA level, breast carcinomas are genetically quite heterogeneous, so there is no universally applicable DNA marker available. Therefore, the main approach to develop molecular diagnostic assays for breast carcinomas has focused on RNA markers. A multimarker approach with a panel of tumor-specific mRNA markers may improve the sensitivity for the detection of DTCs over single marker assays [33, 34].
To date, many transcripts have been evaluated as 'tumor-specific' markers, such as CK18, CK19, CK20, Mucin-1 (MUC1), and carcinoembryonic antigen [35]. However, many of these transcripts can also be identified by reverse transcriptase PCR (RT-PCR) in normal BM, blood, and lymph node tissue [36–38]. Pre-analytical depletion of the disturbing normal cell fraction (for example, granulocytes that express CK20) and/or quantitative RT-PCR determinations with well-defined cut-off values might solve this problem. In addition, expression of the mRNA marker might be downregulated, which argues in favor of the use of a multimarker RT-PCR approach [39].
Enzyme-linked immunospot (ELISPOT) technology
A drawback of both immunocytochemistry and RT-PCR is the fact that these technologies are usually unable to distinguish between viable and apoptotic cells. Recently, a new technique that allows this important discrimination was introduced for DTC/CTC analyses [40]. This technique was designated EPISPOT (for epithelial immunospot) and is based on the secretion or active release of specific marker proteins using an adaptation of the enzyme-linked immunospot (ELISPOT) technology. The EPISPOT assay offers the advantages that only viable tumor cells will be detected and that protein secretion can be detected at an individual cell level [41]. For the detection of breast cancer-derived DTCs/CTCs, MUC1 and CK19 were used as marker proteins [42]. MUC1-secreting CTCs were detected in all metastatic breast cancer patients analyzed, whereas such cells were not observed in healthy controls. Moreover, the enumeration of both MUC1-and CK19-secreting cells allowed the detection of viable DTCs in the BM of 90% and 54% of breast cancer patients with and without overt distant metastasis, respectively [42].
These data demonstrate the high specificity and sensitivity of the new EPISPOT technology, which reveals a unique fingerprint of single viable tumor cells and opens, therefore, a new avenue in the understanding of the biology of early metastatic spread.
Molecular and functional characterization of disseminated tumor cells
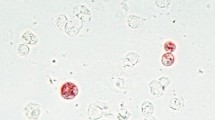
In the past years major efforts have been undertaken to characterize DTCs by phenotyping and genotyping to identify biological features that might favor early dissemination. Using immunological double staining techniques [43] (Figure 2), different DTC phenotypes were discovered. The presence or absence of the HER2 proto-oncogene appears to characterize an aggressive subpopulation with regard to invasive capabilities as well as impaired prognosis [44, 45] and has recently become the focus of potential additional systemic therapy [46, 47]. Furthermore, most DTCs and CTCs do not express the proliferation antigen Ki-67 and may, therefore, be resistant to chemotherapy [48, 49].

Phenotyping and genotyping of disseminated tumor cells. (a) Three cytokeratin-positive and HER2-positive disseminated tumor cells (double staining: green (FITC), cytokeratin; red (TexasRed), HER2). (b) Genotyping of a disseminated tumor cell with DNA probes for chromosome 17 (green) and HER2 (red); HER2 is amplified.
Immunocytochemical assessment of phenotype, however, has been only one aspect of DTC research. Detailed molecular descriptions of breast cancer DTCs found in BM at the genome level revealed a high degree of genetic heterogeneity [50]. With current techniques, it is possible to perform genomic analysis even of single cells (Figure 2). Specifically, genomic aberrations seen in selected areas of the primary tumors were not seen with the DTCs [51]. Conceivably, the DTCs may have originated from small subclones within the primary tumor that were not sampled or they may have undergone significant genetic changes after disseminating into the BM.
By applying gene expression analysis to primary breast tumors in relation to the presence or absence of DTCs in BM, specific gene signatures in primary tumors of patients with DTCs in BM were observed [52]. These findings challenge the traditional concept that tumor cells acquire their metastatic genotype and phenotype late during tumor development, but rather support the alternative concept that tumor cells acquire the genetic changes relevant to their metastatic capacity early in tumorigenesis [53], so that the metastatic potential of human tumors is encoded in the bulk of a primary tumor [53, 54]. This concept could also explain the presence of DTCs in BM at early stages of breast cancer.
BM is a homing organ not only for breast cancer DTCs but also for various epithelial tumors, such as prostate, lung and colon cancer [16, 55, 56]. The exact molecular biological mechanisms, including adhesion molecules and hypoxia, that allow primary tumor cells to disseminate into BM are under investigation [52, 57–59]. Interestingly, disseminated tumor cells express the CXC-chemokine receptor CXCR4 and it has been shown that metastatic cells may use this chemokine-mediated mechanism to find their way into the BM as their preferred reservoir as well as different specific distant sites, such as lung and liver. After homing, phenotypic changes must occur to allow DTCs to evolve into solid metastases. These events require genomic changes such as cytogenic aberrations as well as phenotypic changes involving growth factor receptors, proteases, adhesion molecules and major histocompatibility (MHC) antigens [55].
Half of DTC-positive breast cancer patients will relapse over a ten year period, while the other half will remain free of disease [8] (Table 1). Data from animal models suggest that an important fraction of DTCs might remain in a 'dormant' state and never develop into overt metastases. However, the persistence of DTCs after primary treatment continues to increase the risk for late metastatic relapse even years after primary treatment [60]. What exactly characterizes tumor cell dormancy? Does it describe an entirely non-proliferative state or does it merely reflect a delicate balance between competing mechanisms such as proliferation and apoptosis? Our current knowledge about tumor dormancy as a steady state of cell metabolism remains limited. Both changes in tumor cells themselves (for example, additional mutations) as well as in the surrounding microenvironment (decreased immuno-surveillance or increased angiogenic potential) could be involved in the transformation of the quiescent phase into the dynamic phase of metastasis formation [61–65].
Since we know that the overexpression of the tyrosine kinase receptor HER2 on DTCs is linked to metastatic relapse [45, 66–68], HER2-mediated signaling could be important during the transformation from dormant state to an active growth stage. Other than HER2 related mechanisms, an increase in p53 mutations [69, 70], the accumulation of genomic imbalances [70, 71], and the response to, and secretion of, stem cell growth factors (epidermal growth factor, fibroblast growth factor) [42, 72, 73] could be involved in the 'awakening' of dormant DTCs.
Recent discoveries of new stem cell markers and an increased interest in the role of so-called breast cancer stem cells have opened up new avenues of research on DTCs as well, since it is generally believed that breast cancer stem cells especially have the potential to disseminate from the primary tumor to distant sites [42, 74–76].
The significant correlation between the presence of DTCs in BM and metastatic relapse [76] suggests that the 'stem cells' of overt metastases might be among those DTCs as metastatic stem cells. Various findings provide interesting clues: most DTCs/CTCs are non-proliferating (that is, Ki-67 negative) and resistant to chemotherapy [49, 77, 78], and similar characteristics have been postulated for cancer stem cells. More specifically, Balic and colleagues [79] showed that micrometastases isolated from the BM of early-stage breast cancer contain considerable numbers of CD44+CD24-/low cells, raising the possibility that many, if not the majority, of early disseminated cancer cells in BM have a putative breast cancer stem cell phenotype. Furthermore, it appears that these cells display distinct characteristics, such as increased angiogenic capacity and the expression of CXCR4 receptors [79, 80], which would facilitate their spread to distant sites.
In summary, the direct analysis of DTCs/CTCs and their surrounding microenvironment continues to provide new insights into the complex cascade of breast cancer metastasis. New methods such as whole genome amplification or expression profiling of single tumor cells will provide more information on the molecular characteristics of early disseminating tumor cells in breast cancer patients.
Clinical relevance of DTCs and CTCs for predicting outcome and monitoring therapy
Disseminated tumor cells as a prognostic factor in primary breast cancer
DTCs in the BM of breast cancer patients are an independent significant predictor for poor prognosis (Table 2). Conclusive data on the prognostic relevance of such findings are derived from recently published studies [4, 6, 10, 22, 73, 81–83], as well as a pooled analysis involving 4,703 patients with stage I, II or III breast cancer. In this study, DTCs were found in 31% of the patients [8]. A positive BM finding was a significant prognostic factor with respect to poor overall survival and breast-cancer–specific survival with more than twofold increased hazard ratios. In the multivariate analysis, BM status was the strongest independent factor for disease-free and overall survival.
Based on current published recommendations [14], therapeutic interventions, risk stratifications and deviations from internationally accepted adjuvant treatment strategies based on the presence of DTCs in the BM of patients with newly diagnosed operable (that is stage I to III) breast cancer should still be limited to prospective clinical trials until the clinical value of DTCs for optimization of treatment decisions has been confirmed in such studies.
Disseminated tumor cell determination during follow-up
In addition to their use as a prognostic factor in breast cancer, monitoring of BM post-surgery (that is, during and after systemic adjuvant therapy) might be able to provide unique information for the clinical management of individual cancer patients (Table 2). Several studies have indicated that the presence of DTCs in BM after adjuvant therapy is a predictor of poor prognosis [44, 60, 84]. Patients with high-risk breast cancer (more than three involved axillary lymph nodes or extensive invasion of cutaneous lymph vessels) receiving standard taxane or anthracycline containing chemotherapy were monitored by BM analysis before and after adjuvant chemotherapy [84]. The presence of tumor cells after therapy was associated with an extremely poor prognosis and pointed to a heterogeneous response to treatment. A recent European pooled analysis involving 696 patients from three large European academic breast cancer centers confirmed these findings [85]; 16% of breast cancer patients had tumor cell persistence in BM. Moreover, in the multivariate analysis, allowing for BM status, tumor size, nodal status and histopathological grading, DTCs were an independent prognostic factor for subsequent reduced breast cancer survival followed by nodal status at the time of primary diagnosis.
The identification of patients at increased risk for recurrence after completion of adjuvant chemotherapy is an application of high clinical relevance, since these patients might benefit from an additional 'second-line' treatment, for example, bisphosphonates or targeted therapies like anti-HER2 approaches. Encouraging results have already been reported for bisphosphonates.
Bisphosphonates are potent inhibitors of osteoclast-mediated bone resorption. They are successfully used in conditions of increased bone turnover such as osteoporosis or bone metastases. Bisphosphonates inhibit osteoclast precursor cells, modulate migratory and adhesive characteristics, induce apoptosis of osteoclasts and influence the microenvironment [86]. Small trials have been initiated to study the influence of bisphosphonates on DTCs (for example, MRD-ZOL-001). DTC-positive primary breast cancer patients are randomized to zoledronate or observation only after cytotoxic treatment; results have not been reported yet. A similar study was performed by Rack and colleagues [87]. All patients (n = 14) receiving bisphosphonates were DTC negative after treatment. In contrast, 4 of 14 patients without bisphosphonate treatment showed DTC persistence.
HER2-targeted therapy may also be of value for primary breast cancer patients with HER2-positive DTCs. A humanized anti-HER2 monoclonal antibody (trastuzumab) was recently approved by the Food and Drug Administration [46, 47]. Currently, all patients are stratified to this targeted therapy by primary tumor analysis only. However, recent reports have shown that HER2-positive DTCs and CTCs can also be detected in patients with HER2-negative primary tumors [31, 45, 88]. These findings are consistent with previous data on the high frequency and prognostic relevance of HER2 expression on DTCs in BM [67] and they suggest that additional patients could benefit from HER2-directed therapies [88]. Ongoing clinical studies will reveal whether the HER2 status of DTCs may predict response to trastuzumab or other HER2-directed therapies.
However, despite these interesting results, therapeutic interventions based on the presence of DTCs in BM of patients with no evidence of disease should still be limited to prospective clinical trials [87].
Circulating tumor cells as a prognostic factor in primary breast cancer
The clinical relevance of CTCs in primary breast cancer is still under investigation (Table 2). Depending on the detection technique used, CTCs were revealed in 10% to 60% of primary breast cancer patients with no clinical signs of overt metastases [21, 26]. Several studies have used RT-PCR based methods and showed a prognostic impact [89–91]. Nevertheless, the prognostic relevance of CTCs in the blood of patients with early-stage disease needs to still be demonstrated in prospective multicenter studies [92].
Circulating tumor cells for monitoring adjuvant therapy in primary breast cancer
Sequential peripheral blood analyses should be more acceptable than BM aspirations for therapy monitoring. Therefore, many research groups are currently assessing the clinical value of CTCs for therapy monitoring (Table 2). In the German neoadjuvant trial 'GeparQuattro' [93], CTC determinations have been performed before and after primary systemic chemotherapy. The positivity rate defined as the detection of one or more CTCs was 22% before treatment and decreased to 14% after chemotherapy. The correlation with therapy response has not been reported yet [94].
The aim of the SUCCESS trial [95] is to evaluate the clinical value of CTCs in an adjuvant setting [96]. So far, CTCs have been evaluated in 1,767 patients before adjuvant treatment. The positivity rate defined as the detection of more than one CTC was 10%. A positive blood count was only correlated to nodal status. After completion of cytotxic therapy, 7% of patients showed CTC persistence. Further CTC analyses are planned after two and five years. At the beginning of 2009, the first results for the prognostic relevance of CTCs are expected.
Circulating tumor cells as a prognostic and predictive factor in metastatic breast cancer
The prognostic and predictive value of CTCs in metastatic breast cancer has been proven by large studies [29, 97] (Table 2). Cristofanilli and colleagues [29] demonstrated in 177 metastatic breast cancer patients that the presence of five or more tumor cells is associated with worse prognosis. Interestingly, the CTC count after the first cycle of chemotherapy indicates poor clinical outcome and the prognostic impact of increased CTC numbers is also maintained when repeated examinations during follow-up are performed [97]. In addition, CTC determinations seem to be superior over conventional imaging methods for response evaluation [98]. The clinical utility of these findings are now being prospectively addressed in a randomized trial, SWOG S0500, led by the Southwest Oncology group [99].
In this trial only metastatic patients with more than four CTCs are eligible. The aim of this trial is to determine whether women with metastatic breast cancer and CTC levels of 5 or more cells per 7.5 ml of blood after 3 weeks of first-line chemotherapy show an improved overall survival and progression-free survival when changing to an alternative chemotherapy regimen at the next course rather than waiting for clinical evidence of progressive disease.
Circulating tumor cells for 'real time biopsy' at the time of metastatic disease
The development of metastatic disease is assumed to be a highly selective process. Only a small portion of tumor cells of the primary tumor probably have the ability to initiate metastatic growth in different organ sites. Therefore, the phenotype of the primary tumor may not necessarily reflect the phenotype of metastatic disease. There could, therefore, be a striking potential in reevaluating therapeutic targets on CTCs, which might enable more individualized and optimized anti-metastatic therapy in cancer patients. Several small studies have been reported using CTCs for reevaluation of HER2 status. Uhr and colleagues [68] reassessed the HER2 status in 31 metastatic patients with CTCs. Of 24 patients with initially HER2-negative tumors, 9 (38%) had HER2-positive cells. Four of these nine patients were treated with Herceptin. Three of these patients showed partial or complete remission. In the study of Fehm and colleagues [100], HER2 status was reassessed at the time of metastatic disease in 21 metastatic breast cancer patients by CTCs. HER2 was overexpressed in 8 of these 21 initially HER2-negative patients (38%).
Based on these results, it will be important to design clinical trials to correlate clinical responses to HER2-targeted therapy by HER2-positive CTCs in metastatic cancer. Another important question will be whether hormone receptor status also changes during disease progression and, therefore, influences response to palliative endocrine treatment.
Can DTC determination be replaced by CTC analysis?
To date, it is not clear if CTC measurements could replace the examination of BM. Previously, two immunocytochemical studies demonstrated statistically significant correlations between DTC detection in BM and blood but BM was more frequently positive than blood [49, 73]. One possible explanation is that BM is a homing organ for DTCs, whereas blood analyses allow only a 'snap shot' of tumor cell dissemination. Recently, it was also reported that detection of DTCs in BM had superior prognostic significance in comparison with CTC measurements in blood when analyzing patients with metastatic and non-metastatic breast cancer by a quantitative RT-PCR assay for CK19 and mammaglobin mRNAs [101]. In line with this, another report using immunocytochemistry showed that only BM but not blood analyses provided prognostic information [102]. Currently, these findings do not support changing from analyzing DTCs in BM to CTCs from blood, but future studies with improved detection technologies may help to clarify this issue.
Conclusions and perspectives
Besides the prognostic information derived from the detection of DTCs in BM and from CTCs, the presence of these cells may also provide a tool for prediction or monitoring the efficacy of systemic therapy. The study on CTCs with the greatest level of evidence performed to date has been in patients with metastatic disease. However, CTC measurements might also have particular clinical relevance in the context of adjuvant systemic therapy.
Prospective clinical studies are now ongoing to evaluate whether eradication of CTCs in the blood (and also DTCs in BM) is correlated with a longer disease-free period and overall survival in the adjuvant setting and if therapy guided by CTC testing is able to improve the outcome of metastatic patients. An additional important goal is the possibility of identifying metastatic tumor specific targets in order to improve therapy regimens.
The molecular characterization of these cells should allow further insights into the biology of metastatic dissemination and, therefore, help to improve treatment strategies.
Abbreviations
- BM:
-
bone marrow
- CK:
-
cytokeratin
- CTC:
-
circulating tumor cell
- DTC:
-
disseminated tumor cell
- EPISPOT:
-
epithelial immunospot
- MUC1:
-
Mucin-1
- RT-PCR:
-
reverse transcriptase PCR.
References
Herbert GS, Sohn VY, Brown TA: The impact of nodal isolated tumor cells on survival of breast cancer patients. Am J Surg. 2007, 193: 571-573. 10.1016/j.amjsurg.2007.01.007. discussion 573–574.
Imoto S, Ochiai A, Okumura C, Wada N, Hasebe T: Impact of isolated tumor cells in sentinel lymph nodes detected by immunohistochemical staining. Eur J Surg Oncol. 2006, 32: 1175-1179. 10.1016/j.ejso.2006.08.006.
Kahn HJ, Hanna WM, Chapman JA, Trudeau ME, Lickley HL, Mobbs BG, Murray D, Pritchard KI, Sawka CA, McCready DR, Marks A: Biological significance of occult micrometastases in histologically negative axillary lymph nodes in breast cancer patients using the recent American Joint Committee on Cancer breast cancer staging system. Breast J. 2006, 12: 294-301. 10.1111/j.1075-122X.2006.00267.x.
Gebauer G, Fehm T, Merkle E, Beck EP, Lang N, Jager W: Epithelial cells in bone marrow of breast cancer patients at time of primary surgery: clinical outcome during long-term follow-up. J Clin Oncol. 2001, 19: 3669-3674.
Landys K, Persson S, Kovarik J, Hultborn R, Holmberg E: Prognostic value of bone marrow biopsy in operable breast cancer patients at the time of initial diagnosis: results of a 20-year median follow-up. Breast Cancer Res Treat. 1998, 49: 27-33. 10.1023/A:1005980919916.
Gerber B, Krause A, Muller H, Richter D, Reimer T, Makovitzky J, Herrnring C, Jeschke U, Kundt G, Friese K: Simultaneous immunohistochemical detection of tumor cells in lymph nodes and bone marrow aspirates in breast cancer and its correlation with other prognostic factors. J Clin Oncol. 2001, 19: 960-971.
Pierga JY, Bonneton C, Magdelenat H, Vincent-Salomon A, Nos C, Boudou E, Pouillart P, Thiery JP, de Cremoux P: Real-time quantitative PCR determination of urokinase-type plasminogen activator receptor (uPAR) expression of isolated micrometastatic cells from bone marrow of breast cancer patients. Int J Cancer. 2005, 114: 291-298. 10.1002/ijc.20698.
Braun S, Vogl FD, Naume B, Janni W, Osborne M, Coombes RC, Schlimok G, Diel I, Gerber B, Gebauer G, Pierga J-Y, Marth C, Oruzio D, Wiedswang G, Solomayer E-F, Kundt G, Strobl B, Fehm T, Wong GYC, Bliss J, Vincent-Salomon A, Pantel K: International pooled analysis of prognostic significance of bone marrow micrometastasis in patients with stage I, II, or III breast cancer. N Engl J Med. 2005, 353: 793-802. 10.1056/NEJMoa050434.
Pantel K, Schlimok G, Angstwurm M, Weckermann D, Schmaus W, Gath H, Passlick B, Izbicki JR, Riethmuller G: Methodological analysis of immunocytochemical screening for disseminated epithelial tumor cells in bone marrow. J Hematother. 1994, 3: 165-173.
Braun S, Pantel K, Muller P, Janni W, Hepp F, Kentenich CR, Gastroph S, Wischnik A, Dimpfl T, Kindermann G, Riethmüller G, Schlimok G: Cytokeratin-positive cells in the bone marrow and survival of patients with stage I, II, or III breast cancer. N Engl J Med. 2000, 342: 525-533. 10.1056/NEJM200002243420801.
Borgen E, Beiske K, Trachsel S, Nesland JM, Kvalheim G, Herstad TK, Schlichting E, Qvist H, Naume B: Immunocytochemical detection of isolated epithelial cells in bone marrow: non-specific staining and contribution by plasma cells directly reactive to alkaline phosphatase. J Pathol. 1998, 185: 427-434. 10.1002/(SICI)1096-9896(199808)185:4<427::AID-PATH127>3.0.CO;2-7.
Braun S, Pantel K: Micrometastatic bone marrow involvement: detection and prognostic significance. Med Oncol. 1999, 16: 154-165.
Borgen E, Naume B, Nesland JM, Kvalheim G, Beiske K, Fodstad O, Diel I, Solomayer E, Theocharous P, Coombes RC, Smith B, Wunder E, Marolleau J-P, Garcia J, Pantel K: Standardization of the immunocytochemical detection of cancer cells in BM and blood: I. establishment of objecive criteria for the evaluation of immunostained cells. Cytometry. 1999, 1: 377-388.
Fehm T, Braun S, Müller V, Janni W, Marth C, Pantel K, Schindlbeck C, Solomayer E: A concept for the standardized detection of disseminated tumor cells in bone marrow of patients with primary breast cancer and its clinical implementation. Cancer. 2006, 107: 885-892. 10.1002/cncr.22076.
Dismal Project. [http://www.dismal-project.eu/]
Zach O, Lutz D: Tumor cell detection in peripheral blood and bone marrow. Curr Opin Oncol. 2006, 18: 48-56. 10.1097/01.cco.0000198973.51615.fa.
Paterlini-Brechot P, Benali NL: Circulating tumor cells (CTC) detection: clinical impact and future directions. Cancer Lett. 2007, 253: 180-204. 10.1016/j.canlet.2006.12.014.
Pinzani P, Salvadori B, Simi L, Bianchi S, Distante V, Cataliotti L, Pazzagli M, Orlando C: Isolation by size of epithelial tumor cells in peripheral blood of patients with breast cancer: correlation with real-time reverse transcriptase-polymerase chain reaction results and feasibility of molecular analysis by laser microdissection. Hum Pathol. 2006, 37: 711-718. 10.1016/j.humpath.2006.01.026.
Wong NS, Kahn HJ, Zhang L, Oldfield S, Yang LY, Marks A, Trudeau ME: Prognostic significance of circulating tumour cells enumerated after filtration enrichment in early and metastatic breast cancer patients. Breast Cancer Res Treat. 2006, 99: 63-69. 10.1007/s10549-006-9181-4.
Rosenberg R, Gertler R, Friederichs J, Fuehrer K, Dahm M, Phelps R, Thorban S, Nekarda H, Siewert JR: Comparison of two density gradient centrifugation systems for the enrichment of disseminated tumor cells in blood. Cytometry. 2002, 49: 150-158. 10.1002/cyto.10161.
Witzig TE, Bossy B, Kimlinger T, Roche PC, Ingle JN, Grant C, Donohue J, Suman VJ, Harrington D, Torre-Bueno J, Bauer KD: Detection of circulating cytokeratin-positive cells in the blood of breast cancer patients using immunomagnetic enrichment and digital microscopy. Clin Cancer Res. 2002, 8: 1085-1091.
Wiedswang G, Borgen E, Karesen R, Kvalheim G, Nesland JM, Qvist H, Schlichting E, Sauer T, Janbu J, Harbitz T, Naume B: Detection of isolated tumor cells in bone marrow is an independent prognostic factor in breast cancer. J Clin Oncol. 2003, 21: 3469-3478. 10.1200/JCO.2003.02.009.
Woelfle U, Breit E, Zafrakas K, Otte M, Schubert F, Muller V, Izbicki JR, Loning T, Pantel K: Bi-specific immunomagnetic enrichment of micrometastatic tumour cell clusters from bone marrow of cancer patients. J Immunol Methods. 2005, 300: 136-145. 10.1016/j.jim.2005.03.006.
Kraeft SK, Ladanyi A, Galiger K, Herlitz A, Sher AC, Bergsrud DE, Even G, Brunelle S, Harris L, Salgia R, Dahl T, Kesterson J, Chen LB: Reliable and sensitive identification of occult tumor cells using the improved rare event imaging system. Clin Cancer Res. 2004, 10: 3020-3028. 10.1158/1078-0432.CCR-03-0361.
Borgen E, Naume B, Nesland JM, Nowels KW, Pavlak N, Ravkin I, Goldbard S: Use of automated microscopy for the detection of disseminated tumor cells in bone marrow samples. Cytometry. 2001, 46: 215-221. 10.1002/cyto.1130.
Kraeft SK, Sutherland R, Gravelin L, Hu GH, Ferland LH, Richardson P, Elias A, Chen LB: Detection and analysis of cancer cells in blood and bone marrow using a rare event imaging system. Clin Cancer Res. 2000, 6: 434-442.
Bauer KD, de la Torre-Bueno J, Diel IJ, Hawes D, Decker WJ, Priddy C, Bossy B, Ludmann S, Yamamoto K, Masih AS, Espinoza FP, Harrington DS: Reliable and sensitive analysis of occult bone marrow metastases using automated cellular imaging. Clin Cancer Res. 2000, 6: 3552-3559.
Mehes G, Luegmayr A, Ambros IM, Ladenstein R, Ambros PF: Combined automatic immunological and molecular cytogenetic analysis allows exact identification and quantification of tumor cells in the bone marrow. Clin Cancer Res. 2001, 7: 1969-1975.
Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ, Terstappen LW, Hayes DF: Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med. 2004, 351: 781-791. 10.1056/NEJMoa040766.
Thiery JP, Sleeman JP: Complex networks orchestrate epithelial-mesenchymal transitions. Nat Rev Mol Cell Biol. 2006, 7: 131-142. 10.1038/nrm1835.
Meng S, Tripathy D, Shete S, Ashfaq R, Saboorian H, Haley B, Frenkel E, Euhus D, Leitch M, Osborne C, Clifford E, Perkins S, Beitsch P, Khan A, Morrison L, Herlyn D, Terstappen LW, Lane N, Wang J, Uhr J: uPAR and HER-2 gene status in individual breast cancer cells from blood and tissues. Proc Natl Acad Sci USA. 2006, 103: 17361-17365. 10.1073/pnas.0608113103.
Riethdorf S, Fritsche H, Müller V, Rau T, Schindlbeck C, Rack B, Janni W, Coith C, Beck K, Jänicke F, Jackson S, Gornet T, Cristofanilli M, Pantel K: Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the CellSearch system. Clin Cancer Res. 2007, 13: 920-928. 10.1158/1078-0432.CCR-06-1695.
Symmans WF, Liu J, Knowles DM, Inghirami G: Breast cancer heterogeneity: evaluation of clonality in primary and metastatic lesions. Hum Pathol. 1995, 26: 210-216. 10.1016/0046-8177(95)90039-X.
Braun S, Hepp F, Sommer HL, Pantel K: Tumorantigen heterogeneity of disseminated breast cancer cells: implications for immunotherapy of minimal residual disease. Int J Cancer. 1999, 84: 1-5. 10.1002/(SICI)1097-0215(19990219)84:1<1::AID-IJC1>3.0.CO;2-A.
Datta YH, Adams PT, Drobyski WR, Ethier SP, Terry VH, Roth MS: Sensitive detection of occult breast cancer by the reverse-transcriptase polymerase chain reaction. J Clin Oncol. 1994, 12: 475-482.
Zippelius A, Kufer P, Honold G, Kollermann MW, Oberneder R, Schlimok G, Riethmuller G, Pantel K: Limitations of reverse-transcriptase polymerase chain reaction analyses for detection of micrometastatic epithelial cancer cells in bone marrow. J Clin Oncol. 1997, 15: 2701-2708.
Bostick PJ, Chatterjee S, Chi DD, Huynh KT, Giuliano AE, Cote R, Hoon DS: Limitations of specific reverse-transcriptase polymerase chain reaction markers in the detection of metastases in the lymph nodes and blood of breast cancer patients. J Clin Oncol. 1998, 16: 2632-2640.
Jung R, Kruger W, Hosch S, Holweg M, Kroger N, Gutensohn K, Wagener C, Neumaier M, Zander AR: Specificity of reverse transcriptase polymerase chain reaction assays designed for the detection of circulating cancer cells is influenced by cytokines in vivo and in vitro. Br J Cancer. 1998, 78: 1194-1198.
Lankiewicz S, Rivero BG, Bocher O: Quantitative real-time RT-PCR of disseminated tumor cells in combination with immunomagnetic cell enrichment. Mol Biotechnol. 2006, 34: 15-27. 10.1385/MB:34:1:15.
Pantel K, Alix-Panabieres C: The clinical significance of circulating tumor cells. Nat Clin Pract Oncol. 2007, 4: 62-63. 10.1038/ncponc0737.
Czerkinsky C, Moldoveanu Z, Mestecky J, Nilsson L, Ouchterlony O: A novel two colour ELISPOT assay. I. Simultaneous detection of distinct types of antibody-secreting cells. J Immunol Methods. 1988, 115: 31-37. 10.1016/0022-1759(88)90306-7.
Alix-Panabières C, Vendrell J-P, Pellé O, Riethdorf S, Müller V, Fabbro M, Pantel K: Detection and characterization of putative metastatic precursor cells in cancer patients. Clin Chem. 2007, 53: 537-539. 10.1373/clinchem.2006.079509.
Fehm T, Sagalowsky A, Clifford E, Beitsch P, Saboorian H, Euhus D, Meng S, Morrison L, Tucker T, Lane N, Ghadimi BM, Heselmeyer-Haddad K, Ried T, Rao C, Uhr J: Cytogenetic evidence that circulating epithelial cells in patients with carcinoma are malignant. Clin Cancer Res. 2002, 8: 2073-2084.
Wiedswang G, Borgen E, Karesen R, Qvist H, Janbu J, Kvalheim G, Nesland JM, Naume B: Isolated tumor cells in bone marrow three years after diagnosis in disease-free breast cancer patients predict unfavorable clinical outcome. Clin Cancer Res. 2004, 10: 5342-5348. 10.1158/1078-0432.CCR-04-0245.
Wülfing P, Borchard J, Buerger H, Heidl S, Zanker KS, Kiesel L, Brandt B: HER2-positive circulating tumor cells indicate poor clinical outcome in stage I to III breast cancer patients. Clin Cancer Res. 2006, 12: 1715-1720. 10.1158/1078-0432.CCR-05-2087.
Piccart-Gebhart MJ, Procter M, Leyland-Jones B, Goldhirsch A, Untch M, Smith I, Gianni L, Baselga J, Bell R, Jackisch C, Cameron D, Dowsett M, Barrios CH, Steger G, Huang CS, Andersson M, Inbar M, Lichinitser M, Láng I, Nitz U, Iwata H, Thomssen C, Lohrisch C, Suter TM, Rüschoff J, Suto T, Greatorex V, Ward C, Straehle C, McFadden E, Dolci MS, Gelber RD, Herceptin Adjuvant (HERA) Trial Study Team: Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005, 353: 1659-1672. 10.1056/NEJMoa052306.
Romond EH, Perez EA, Bryant J, Suman VJ, Geyer CE, Davidson NE, Tan-Chiu E, Martino S, Paik S, Kaufman PA, Swain SM, Pisansky TM, Fehrenbacher L, Kutteh LA, Vogel VG, Visscher DW, Yothers G, Jenkins RB, Brown AM, Dakhil SR, Mamounas EP, Lingle WL, Klein PM, Ingle JN, Wolmark N: Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005, 353: 1673-1684. 10.1056/NEJMoa052122.
Pantel K, Schlimok G, Braun S, Kutter D, Lindemann F, Schaller G, Funke I, Izbicki JR, Riethmuller G: Differential expression of proliferation-associated molecules in individual micrometastatic carcinoma cells. J Natl Cancer Inst. 1993, 85: 1419-1424. 10.1093/jnci/85.17.1419.
Müller V, Stahmann N, Riethdorf S, Rau T, Zabel T, Goetz A, Jänicke F, Pantel K: Circulating tumor cells in breast cancer: correlation to bone marrow micrometastases, heterogeneous response to systemic therapy and low proliferative activity. Clin Cancer Res. 2005, 11: 3678-3685. 10.1158/1078-0432.CCR-04-2469.
Klein CA, Blankenstein TJF, Schmidt-Kittler O, Petronio M, Polzer B, Stoecklein NH, Riethmüller G: Genetic heterogeneity of single disseminated tumour cells in minimal residual cancer. Lancet. 2002, 360: 683-689. 10.1016/S0140-6736(02)09838-0.
Gangnus R, Langer S, Breit E, Pantel K, Speicher MR: Genomic profiling of viable and proliferative micrometastatic cells from early-stage breast cancer patients. Clin Cancer Res. 2004, 10: 3457-3464. 10.1158/1078-0432.CCR-03-0818.
Woelfle U, Cloos J, Sauter G, Riethdorf L, Janicke F, van Diest P, Brakenhoff R, Pantel K: Molecular signature associated with bone marrow micrometastasis in human breast cancer. Cancer Res. 2003, 63: 5679-5684.
Bernards R, Weinberg RA: A progression puzzle. Nature. 2002, 418: 823-10.1038/418823a.
Ramaswamy S, Ross KN, Lander ES, Golub TR: A molecular signature of metastasis in primary solid tumors. Nat Genet. 2003, 33: 49-54. 10.1038/ng1060.
Pantel K, Brakenhoff RH: Dissecting the metastatic cascade. Nat Rev Cancer. 2004, 4: 448-456. 10.1038/nrc1370.
Fehm T, Becker S, Bachmann C, Beck V, Gebauer G, Banys M, Wallwiener D, Solomayer EF: Detection of disseminated tumor cells in patients with gynecological cancers. Gynecol Oncol. 2006, 103: 942-947. 10.1016/j.ygyno.2006.05.049.
Müller A, Homey B, Soto H, Ge N, Catron D, Buchanan ME, McClanahan T, Murphy E, Yuan W, Wagner SN, Barrera JL, Mohar A, Verástegui E, Zlotnik A: Involvement of chemokine receptors in breast cancer metastasis. Nature. 2001, 410: 50-56. 10.1038/35065016.
Kaifi JT, Yekebas EF, Schurr P, Obonyo D, Wachowiak R, Busch P, Heinecke A, Pantel K, Izbicki JR: Tumor-cell homing to lymph nodes and bone marrow and CXCR4 expression in esophageal cancer. J Natl Cancer Inst. 2005, 97: 1840-1847.
Generali D, Berruti A, Brizzi MP, Campo L, Bonardi S, Wigfield S, Bersiga A, Allevi G, Milani M, Aguggini S, Gandolfi V, Dogliotti L, Bottini A, Harris AL, Fox SB: Hypoxia-inducible factor-1alpha expression predicts a poor response to primary chemoendocrine therapy and disease-free survival in primary human breast cancer. Clin Cancer Res. 2006, 12: 4562-4568. 10.1158/1078-0432.CCR-05-2690.
Janni W, Rack B, Schindlbeck C, Strobl B, Rjosk D, Braun S, Sommer H, Pantel K, Gerber B, Friese K: The persistence of isolated tumor cells in bone marrow from patients with breast carcinoma predicts an increased risk for recurrence. Cancer. 2005, 103: 884-891. 10.1002/cncr.20834.
Naumov GN, Bender E, Zurakowski D, Kang SY, Sampson D, Flynn E, Watnick RS, Straume O, Akslen LA, Folkman J, Almog N: A model of human tumor dormancy: an angiogenic switch from the nonangiogenic phenotype. J Natl Cancer Inst. 2006, 98: 316-325.
Meng S, Tripathy D, Frenkel EP, Shete S, Naftalis EZ, Huth JF, Beitsch PD, Leitch M, Hoover S, Euhus D, Haley B, Morrison L, Fleming TP, Herlyn D, Terstappen LW, Fehm T, Tucker TF, Lane N, Wang J, Uhr JW: Circulating tumor cells in patients with breast cancer dormancy. Clin Cancer Res. 2004, 10: 8152-8162. 10.1158/1078-0432.CCR-04-1110.
Marches R, Scheuermann R, Uhr J: Cancer dormancy: from mice to man. Cell Cycle. 2006, 5: 1772-1778.
Aguirre-Ghiso JA: Models, mechanisms and clinical evidence for cancer dormancy. Nat Rev Cancer. 2007, 7: 834-846. 10.1038/nrc2256.
Vessella RL, Pantel K, Mohla S: Tumor cell dormancy: an NCI workshop report. Cancer Biol Ther. 2007, 6: 1496-1504.
Apostolaki S, Perraki M, Pallis A, Bozionelou V, Agelaki S, Kanellou P, Kotsakis A, Politaki E, Kalbakis K, Kalykaki A, Vamvakas L, Georgoulias V, Mavroudis D: Circulating HER2 mRNA-positive cells in the peripheral blood of patients with stage I and II breast cancer after the administration of adjuvant chemotherapy: evaluation of their clinical relevance. Ann Oncol. 2007, 18: 851-858. 10.1093/annonc/mdl502.
Braun S, Schlimok G, Heumos I, Schaller G, Riethdorf L, Riethmuller G, Pantel K: ErbB2 overexpression on occult metastatic cells in bone marrow predicts poor clinical outcome of stage I–III breast cancer patients. Cancer Res. 2001, 61: 1890-1895.
Meng S, Tripathy D, Shete S, Ashfaq R, Haley B, Perkins S, Beitsch P, Khan A, Euhus D, Osborne C, Frenkel E, Hoover S, Leitch M, Clifford E, Vitetta E, Morrison L, Herlyn D, Terstappen LW, Fleming T, Fehm T, Tucker T, Lane N, Wang J, Uhr J: HER-2 gene amplification can be acquired as breast cancer progresses. Proc Natl Acad Sci USA. 2004, 101: 9393-9398. 10.1073/pnas.0402993101.
Putz E, Witter K, Offner S, Stosiek P, Zippelius A, Johnson J, Zahn R, Riethmuller G, Pantel K: Phenotypic characteristics of cell lines derived from disseminated cancer cells in bone marrow of patients with solid epithelial tumors: establishment of working models for human micrometastases. Cancer Res. 1999, 59: 241-248.
Klein CA, Blankenstein TJ, Schmidt-Kittler O, Petronio M, Polzer B, Stoecklein NH, Riethmuller G: Genetic heterogeneity of single disseminated tumour cells in minimal residual cancer. Lancet. 2002, 360: 683-689. 10.1016/S0140-6736(02)09838-0.
Schmidt-Kittler O, Ragg T, Daskalakis A, Granzow M, Ahr A, Blankenstein TJ, Kaufmann M, Diebold J, Arnholdt H, Muller P, Bischoff J, Harich D, Schlimok G, Riethmüller G, Eils R, Klein CA: From latent disseminated cells to overt metastasis: genetic analysis of systemic breast cancer progression. Proc Natl Acad Sci USA. 2003, 100: 7737-7742. 10.1073/pnas.1331931100.
Solakoglu O, Maierhofer C, Lahr G, Breit E, Scheunemann P, Heumos I, Pichlmeier U, Schlimok G, Oberneder R, Kollermann MW, Kollermann J, Speicher MR, Pantel K: Heterogeneous proliferative potential of occult metastatic cells in bone marrow of patients with solid epithelial tumors. Proc Natl Acad Sci USA. 2002, 99: 2246-2251. 10.1073/pnas.042372199.
Pierga JY, Bonneton C, Vincent-Salomon A, de Cremoux P, Nos C, Blin N, Pouillart P, Thiery JP, Magdelenat H: Clinical significance of immunocytochemical detection of tumor cells using digital microscopy in peripheral blood and bone marrow of breast cancer patients. Clin Cancer Res. 2004, 10: 1392-1400. 10.1158/1078-0432.CCR-0102-03.
Shackleton M, Vaillant F, Simpson KJ, Stingl J, Smyth GK, Asselin-Labat ML, Wu L, Lindeman GJ, Visvader JE: Generation of a functional mammary gland from a single stem cell. Nature. 2006, 439: 84-88. 10.1038/nature04372.
Clarke MF, Fuller M: Stem cells and cancer: two faces of eve. Cell. 2006, 124: 1111-1115. 10.1016/j.cell.2006.03.011.
Liu R, Wang X, Chen GY, Dalerba P, Gurney A, Hoey T, Sherlock G, Lewicki J, Shedden K, Clarke MF: The prognostic role of a gene signature from tumorigenic breast-cancer cells. N Engl J Med. 2007, 356: 217-226. 10.1056/NEJMoa063994.
Becker S, Becker-Pergola G, Wallwiener D, Solomayer EF, Fehm T: Detection of cytokeratin-positive cells in the bone marrow of breast cancer patients undergoing adjuvant therapy. Breast Cancer Res Treat. 2006, 97: 91-96. 10.1007/s10549-005-9095-6.
Becker S, Solomayer E, Becker-Pergola G, Wallwiener D, Fehm T: Primary systemic therapy does not eradicate disseminated tumor cells in breast cancer patients. Breast Cancer Res Treat. 2007, 106: 239-243. 10.1007/s10549-006-9484-5.
Balic M, Lin H, Young L, Hawes D, Giuliano A, McNamara G, Datar RH, Cote RJ: Most early disseminated cancer cells detected in bone marrow of breast cancer patients have a putative breast cancer stem cell phenotype. Clin Cancer Res. 2006, 12: 5615-5621. 10.1158/1078-0432.CCR-06-0169.
Wicha MS: Cancer stem cells and metastasis: lethal seeds. Clin Cancer Res. 2006, 12: 5606-5607. 10.1158/1078-0432.CCR-06-1537.
Cote RJ, Rosen PP, Lesser ML, Old LJ, Osborne MP: Prediction of early relapse in patients with operable breast cancer by detection of occult bone marrow micrometastases. J Clin Oncol. 1991, 9: 1749-1756.
Diel IJ, Kaufmann M, Costa SD, Holle R, von Minckwitz G, Solomayer EF, Kaul S, Bastert G: Micrometastatic breast cancer cells in bone marrow at primary surgery: prognostic value in comparison with nodal status. J Natl Cancer Inst. 1996, 88: 1652-1658. 10.1093/jnci/88.22.1652.
Mansi JL, Gogas H, Bliss JM, Gazet JC, Berger U, Coombes RC: Outcome of primary-breast-cancer patients with micrometastases: a long-term follow-up study. Lancet. 1999, 354: 197-202. 10.1016/S0140-6736(98)10175-7.
Braun S, Kentenich C, Janni W, Hepp F, de Waal J, Willgeroth F, Sommer H, Pantel K: Lack of effect of adjuvant chemotherapy on the elimination of single dormant tumor cells in bone marrow of high-risk breast cancer patients. J Clin Oncol. 2000, 18: 80-86.
Janni W, Wiedswang G, Fehm T, Jueckstock J, Borgen E, Rack B, Braun S, Sommer H, Pantel K, Naume B: Persistence of disseminated tumor cells (DTC) in bone marrow (BM) of breast cancer patients predicts increased risk for relapse – results of pooled European data. J Clin Oncol. 2006, 24 (18S): Abstract 10083-
Santini D, Vespasiani Gentilucci U, Vincenzi B, Picardi A, Vasaturo F, La Cesa A, Onori N, Scarpa S, Tonini G: The antineoplastic role of bisphosphonates: from basic research to clinical evidence. Ann Oncol. 2003, 14: 1468-1476. 10.1093/annonc/mdg401.
Rack B, Janni W, Schoberth A, Heinrigs M, Schindlbeck C, Strobl B, Blankenstein T, Sommer H, Friese K: Secondary adjuvant therapy with zoledronate in patients with early breast cancer: is there an effect on persisting isolated tumor cells (ITC) in the bone marrow (BM)?. Breast Cancer Res Treat. 2004, 88 (Suppl 1): Abstract 6019-
Solomayer EF, Becker S, Pergola-Becker G, Bachmann R, Kramer B, Vogel U, Neubauer H, Wallwiener D, Huober J, Fehm TN: Comparison of HER2 status between primary tumor and disseminated tumor cells in primary breast cancer patients. Breast Cancer Res Treat. 2006, 98: 179-184. 10.1007/s10549-005-9147-y.
Ntoulia M, Stathopoulou A, Ignatiadis M, Malamos N, Mavroudis D, Georgoulias V, Lianidou ES: Detection of Mammaglobin A-mRNA-positive circulating tumor cells in peripheral blood of patients with operable breast cancer with nested RT-PCR. Clin Biochem. 2006, 39: 879-887. 10.1016/j.clinbiochem.2006.06.009.
Xenidis N, Perraki M, Kafousi M, Apostolaki S, Bolonaki I, Stathopoulou A, Kalbakis K, Androulakis N, Kouroussis C, Pallis T, Christophylakis C, Argyraki K, Lianidou ES, Stathopoulos S, Georgoulias V, Mavroudis D: Predictive and prognostic value of peripheral blood cytokeratin-19 mRNA-positive cells detected by real-time polymerase chain reaction in node-negative breast cancer patients. J Clin Oncol. 2006, 24: 3756-3762. 10.1200/JCO.2005.04.5948.
Quintela-Fandino M, Lopez JM, Hitt R, Gamarra S, Jimeno A, Ayala R, Hornedo J, Guzman C, Gilsanz F, Cortes-Funes H: Breast cancer-specific mRNA transcripts presence in peripheral blood after adjuvant chemotherapy predicts poor survival among high-risk breast cancer patients treated with high-dose chemotherapy with peripheral blood stem cell support. J Clin Oncol. 2006, 24: 3611-3618. 10.1200/JCO.2005.04.0576.
Cristofanilli M, Mendelsohn J: Circulating tumor cells in breast cancer: advanced tools for "tailored" therapy?. Proc Natl Acad Sci USA. 2006, 103: 17073-17074. 10.1073/pnas.0608651103.
GeparQuattro. [http://www.germanbreastgroup.de/geparquattro/]
Müller V, Riethdorf S, Loibl S, Komor M, Houber J, Schrader I, Conrad M, Untch M, vMinckwitz G, Pantel K: Prospective monitoring of circulating tumor cells in breast cancer patients treated with primary systemic therapy – a translational project of the German Breast Group study GeparQuattro. J Clin Oncol. 2007, 25 (18S): Abstract 21085-
SUCCESS. [http://www.success-studie.de/]
Rack B, Schindlbeck C, Hofmann S, Schneeweiss A, Rezai M, Beckmann M, Pantel K, Schneider A, Sommer H, Janni W: Circulating tumor cells (CTCs) in peripheral blood of primary breast cancer patients. J Clin Oncol. 2007, 25 (18S): Abstract 10595-
Hayes DF, Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Miller MC, Matera J, Allard WJ, Doyle GV, Terstappen LW: Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin Cancer Res. 2006, 12: 4218-4224. 10.1158/1078-0432.CCR-05-2821.
Budd GT, Cristofanilli M, Ellis MJ, Stopeck A, Borden E, Miller MC, Matera J, Repollet M, Doyle GV, Terstappen LW, Hayes DF: Circulating tumor cells versus imaging – predicting overall survival in metastatic breast cancer. Clin Cancer Res. 2006, 12: 6403-6409. 10.1158/1078-0432.CCR-05-1769.
National Cancer Institute Clinical Trials: SWOG S0500. [http://www.cancer.gov/clinicaltrials/SWOG-S0500]
Fehm T, Becker S, Duerr-Stoerzer S, Sotlar K, Müller V, Wallwiener D, Lane N, Solomayer E, Uhr J: Reassessment of HER2 status in breast cancer patients with initially HER2 negative or HER2 unknown primary tumors at the time of metastatic disease by serum HER2 and HER2 status of circulating tumor cells. Breast Can Res. 2007, 9: R74-10.1186/bcr1783.
Benoy IH, Elst H, Philips M, Wuyts H, Van Dam P, Scharpe S, Van Marck E, Vermeulen PB, Dirix LY: Real-time RT-PCR detection of disseminated tumour cells in bone marrow has superior prognostic significance in comparison with circulating tumour cells in patients with breast cancer. Br J Cancer. 2006, 94: 672-680.
Wiedswang G, Borgen E, Schirmer C, Karesen R, Kvalheim G, Nesland JM, Naume B: Comparison of the clinical significance of occult tumor cells in blood and bone marrow in breast cancer. Int J Cancer. 2006, 118: 2013-2019. 10.1002/ijc.21576.
Schlimok G, Funke I, Holzmann B, Gottlinger G, Schmidt G, Hauser H, Swierkot S, Warnecke HH, Schneider B, Koprowski H: Micrometastatic cancer cells in bone marrow: in vitro detection with anti-cytokeratin and in vivo labeling with anti-17-1A monoclonal antibodies. Proc Natl Acad Sci USA. 1987, 84: 8672-8676. 10.1073/pnas.84.23.8672.
Harbeck N, Untch M, Pache L, Eiermann W: Tumour cell detection in the bone marrow of breast cancer patients at primary therapy: results of a 3-year median follow-up. Br J Cancer. 1994, 69: 566-571.
Molino A, Pelosi G, Turazza M, Sperotto L, Bonetti A, Nortilli R, Fattovich G, Alaimo C, Piubello Q, Pavanel F, Micciolo R, Cetto GL: Bone marrow micrometastases in 109 breast cancer patients: correlations with clinical and pathological features and prognosis. Breast Cancer Res Treat. 1997, 42: 23-30. 10.1023/A:1005747711084.
Acknowledgements
This work was supported by grants from the Ministère de l'Economie des Finances et de l'Industrie (MINEFI); the University Medical Center of Montpellier, France; The Deutsche Forschungsgemeinschaft (PA 341/15-2), Bonn, Germany; and the European Commission (DISMAL-project, contract no. LSHC-CT-2005-018911).
This article is published as part of Breast Cancer Research Volume 10 Supplement 1, 2008: The Scientific Basis of Breast Cancer http://breast-cancer-research.com/content/10/S1.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
KP has received unrestricted research grants from Veridex. The other authors have no potential conflict of interest to declare.
Authors' contributions
All authors contributed to the writing of the manuscript.
Rights and permissions
About this article
Cite this article
Fehm, T., Müller, V., Alix-Panabières, C. et al. Micrometastatic spread in breast cancer: detection, molecular characterization and clinical relevance. Breast Cancer Res 10 (Suppl 1), S1 (2008). https://doi.org/10.1186/bcr1869
Published:
DOI: https://doi.org/10.1186/bcr1869