
Abstract
A technique called in vivo magnetic resonance spectroscopy (MRS) can be performed along with magnetic resonance imaging (MRI) to obtain information about the chemical content of breast lesions. This information can be used for several clinical applications, such as monitoring the response to cancer therapies and improving the accuracy of lesion diagnosis. Initial MRS studies of breast cancer show promising results, and a growing number of research groups are incorporating the technique into their breast MRI protocols. This article introduces 1H-MRS of the breast, reviews the literature, discusses current methods and technical issues, and describes applications for treatment monitoring and lesion diagnosis.
Similar content being viewed by others

Introduction
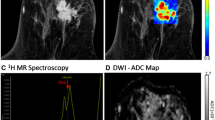
The first in vivo magnetic resonance spectroscopy (MRS) studies of breast measured resonances from phosphorus atoms (31P). These studies showed that measurable variations in phospholipid metabolism could be detected and used for diagnosing cancer and monitoring the response to treatment (reviewed in [1, 2]). More recently, there has been growing interest in breast cancer research using hydrogen (1H)-MRS, because of its higher sensitivity than 31P-MRS. The first breast 1H-MRS reports focused on the diagnostic utility of the water : fat ratio in the breast [3–5], but subsequent studies did not find this ratio to be a useful diagnostic metric [6, 7]. However, several studies performed with 1H-MRS noted that a resonance from choline-containing compounds (tCho) was commonly present in malignant lesions but not in benign or normal tissues [4, 6–11]. Figure 1 shows a representative example of a localized 1H spectrum of an invasive ductal carcinoma, with the tCho resonance indicated.

Example of a localized breast spectrum acquired at 4 T. The image on the left indicates the voxel placement, which covers a rim-enhancing lesion of invasive ductal carcinoma. The water-suppressed spectrum on the right shows the resonances typically observed in malignant breast lesions. Quantifying the spectrum by using water as an internal reference produced a measurement of concentration of total choline-containing compounds of 4.4 ± 0.3 mmol/kg (± SD).
Ex vivo studies have been performed to identify the different choline compounds giving rise to the tCho resonance at a chemical shift of 3.2 ppm. High-resolution 1H spectra acquired from biopsy tissues have shown that the tCho resonance is actually a superposition of several resonances [12–14]. The primary constituents are those with a trimethylamine moiety, R-(CH2)2-N+-(CH3)3, including free choline, phosphocholine, and glycerophosphocholine. Other metabolites possibly contributing include taurine, glucose, phosphoethanolamine, and myo-inositol [14]. The choline head groups associated with semi-mobile lipids may also contribute. These resonances can be separated in ex vivo studies with high-resolution magnetic resonance (MR) spectrometers, but in vivo these peaks are substantially broadened, and at fields as high as 4 T these resonances are generally indistinguishable. Consequently, the simplified approach used in studies in vivo is to treat the 3.2 ppm spectral peak as a single resonance.
Numerous in vivo, ex vivo, and in vitro studies have shown that this tCho peak is elevated in neoplastic tissues. However, the precise mechanisms that produce an elevated tCho concentration ([tCho]) have not yet been fully identified. A working hypothesis is that elevated [tCho] is an indicator of increased cellular proliferation. The largest component contributing to the tCho peak from neoplastic tissue is phosphocholine, a known precursor of membranes. Thus, the increased [tCho] in neoplastic tissues may be a reflection of increased membrane turnover by replicating cells. This is probably an oversimplified view, because [tCho] can be modulated by numerous changes in enzymatic activity and fluxes in biosynthetic and catabolic pathways in which choline compounds serve as both precursors and catabolites. This is an active area of research.
In spite of this seemingly complex situation, several groups have successfully shown that tCho can be used as an indicator of malignancy with clinical 1.5 T scanners. Some groups have also shown that the tCho peak decreases or disappears in response to chemotherapy treatment. The results of these studies are encouraging, and with continued technical development it seems likely that MRS will become a useful tool in detecting and managing breast cancer.
Technical issues
Historically, 1H-MRS research has been focused mainly on the brain, in part because use of this technique on the brain poses fewer technical challenges than on other organ sites. Most of the research and development in the field of MR has been focused on brain applications; as a result, commercial MR systems are generally better optimized for brain rather than breast studies. As a result of increased interest by clinicians and researchers in the application of MR to breast cancer, many technical advances are now taking place that are improving the quality and reliability of breast magnetic resonance imaging (MRI) and MRS. For example, significant improvement in signal : noise ratio can be realized by using multi-channel phased-array coils that are now commercially available.
Single-voxel spectroscopy
Most breast MRS studies so far have used single-voxel spectroscopy (SVS) to localize the chemical signals to a single, cuboid volume (called a voxel) centered on the lesion of interest. Our group uses a specialized pulse sequence called LASER (localization by adiabatic selective refocusing) [15]. This technique has several useful properties; most notably it is insensitive to radiofrequency field inhomogeneity and provides clean localization. Although most breast MRS studies have been done with SVS, other researchers have explored the use of magnetic resonance spectroscopic imaging (MRSI) as an alternative [16]. In MRSI, spectra are acquired in a grid. MRSI has an important advantage: it provides information about the spatial distribution of metabolites, which is useful for studying multiple lesions or evaluating the spatial variation of a metabolite in a heterogeneous lesion. However, MRSI is technically more challenging than SVS, and quantification of metabolite levels is more problematic. For these reasons, and because it is not yet commonly used in the breast, the rest of the discussion here will focus on SVS.
A typical MRS study is performed immediately after acquiring dynamic contrast-enhanced (DCE) MR images. Decisions about the placement of the MRS voxel are usually based on a review of the lesion morphology and the kinetics of contrast agent uptake while the patient is still in the magnet. With SVS, the placement of the voxel is of critical importance. The voxel should be placed so that it contains as much of the lesion as possible while excluding other tissues such as normal fibroglandular or adipose tissue. In studies using MRS to monitor response to treatment, the voxel size and position can be adjusted to cover the same anatomical region of the tumor, decreasing the voxel size as the tumor shrinks.
Lipids
Intense resonances from mobile lipids are a prominent feature of 1H spectra of breast tissues, whereas these signals are essentially absent from brain spectra. The amplitude of the lipid resonance can vary markedly depending on the tissue heterogeneity. The adipose tissue not directly involved in breast carcinoma can pose problems for breast MRS. When trying to place a voxel in a suspect lesion, any adipose tissue inadvertently included in the voxel creates a partial volume effect, reducing the effective volume for spectroscopy. Adipose tissue also limits the ability to optimize (or 'shim') the homogeneity of the magnetic field inside the voxel, which in turn leads to broad resonances and reduced signal : noise ratio. Intense lipid resonances can also produce sideband artefacts that can interfere with MRS measurements. These artefactual resonances can be larger than the tCho resonance. To reduce sideband artefacts, our group uses a method called echo-time averaging, which causes coherent cancellation of sideband artefacts by averaging spectra acquired at several different echo-time values [17]. For all these reasons, it is important to plan voxels carefully to minimize the amount of adipose tissue included.
Quantification
Although several groups have had success in using the detectability of tCho to indicate malignancy, this approach assumes that the MRS measurement sensitivity is roughly constant from one measurement to the next. However, there are several factors that make this assumption questionable in breast MRS, such as variations in voxel size, adipose tissue content, and coil sensitivity. In our experience at 4 T, we have found that these factors produce a large variation in sensitivity [18]. Thus, some form of quantification should be used to correct for sensitivity variations, or at the very least exclude those voxels with unusual sensitivity.
A variety of approaches have been used for quantifying MRS data. We chose to use the intravoxel water resonance as an internal reference, because this method is robust and automatically compensates for variations in many factors [18]. Some groups have proposed using an external standard for referencing [6, 19]. This approach also works but requires additional corrections for voxel size, adipose tissue content, and coil efficiency. Both internal and external referencing methods need correction for differences in relaxation rates, which are difficult to measure in individual subjects.
Applications
Diagnosis
The first and most studied application for breast MRS is to distinguish benign from malignant lesions before biopsy. The first published paper on this topic, by Roebuck and colleagues in 1998 [6], proposed the idea that tCho could be used as a marker of malignancy. Several papers that followed, listed in Table 1, continued to use this hypothesis but performed studies with somewhat different techniques. The overall results are quite consistent. Katz-Brull and colleagues published a combined analysis of the first five papers in Table 1 and reported an overall sensitivity of 83% and specificity of 85% [20]. These results are very encouraging, especially considering that the determination of malignancy was done without considering any other diagnostic or historical information that would normally be available clinically.
Other publications describing tCho detection in breast cancers did not report diagnostic specificity and sensitivity [5, 7]. Although the results using a simple detectability hypothesis are encouraging, it seems likely that there are benign pathologies that also produce detectable levels of tCho. Indeed, at 1.5 T, a detectable tCho resonance has been reported in fibroadenomas [8, 9, 16, 21], tubular adenomas [6, 10] and lactating subjects [8, 11].
Two recent studies have sought to evaluate whether MRS can improve the specificity of a diagnostic breast MR exam. Huang and colleagues appended a single-voxel MRS measurement and a single-slice T 2*-weighted perfusion measurement to a conventional DCE-MRI exam [21]. They found that the addition of MRS increased the specificity of the exam from 62.5% to 87.5%, and the further addition of the perfusion measurement raised the specificity to 100%. Our group recently performed a retrospective blinded-observer performance study with four readers and 55 subjects to determine whether quantitative MRS could improve the specificity and sensitivity of a DCE-MRI exam [22]. In this study we reported that adding quantitative MRS results to a DCE-MRI exam produced improvements in the sensitivity, specificity, and accuracy for all readers, and improved the interobserver agreement between the readers.
Monitoring response to treatment
A second and perhaps more promising application is the use of breast MRS for predicting response to cancer treatment. Current clinically available methods such as palpation and imaging rely on changes in tumor size, which take several weeks before any changes are detectable. Breast MRS, in contrast, detects changes in intracellular metabolism that would occur before any gross morphological change. The first report using tCho measurements to detect treatment response in breast cancer was by Jaganathan and colleagues, who observed that the tCho resonance disappeared or became smaller in 89% of subjects undergoing chemotherapy [11].
Expanding on this observation, our group performed a study designed to determine whether changes in [tCho] could provide a biomarker of clinical response as soon as 24 hours after the first dose of doxorubicin-based chemotherapy for locally advanced breast cancer [23]. Of the first 13 patients who successfully completed the protocol without technical problems, the change in [tCho] between baseline and 24 hours after the first dose of chemotherapy showed a significant positive correlation (R = 0.79, P = 0.001) with the change in lesion size measured at the end of four cycles of chemotherapy (median duration 67 days; range 65 to 72 days). The change in [tCho] within 24 hours was significantly different between responders and nonresponders (P = 0.007) classified with RECIST (Response Evaluation Criteria in Solid Tumors). These results suggest that the change in [tCho] within 24 hours after the first dose of the drug can serve as an early indicator for predicting clinical response to treatment for locally advanced breast cancer.
Conclusion
The quality and reliability of MRS data will only improve as further refinements in MR systems and techniques continue to occur. At present, dissemination of MRS methodology optimized for breast studies is occurring, and breast MRS and MRI are rapidly becoming standard capabilities of most state-of-the-art clinical MR systems with magnets 1.5 T or stronger. The promising results from multiple institutions reported so far suggest that MRS, along with MRI, will have an increased role in the clinical assessment of breast cancer in the future. However, large multicenter trials are still needed before the tCho biomarker can be widely used to guide diagnostic decisions and to predict response to therapy.
Note
This article is part of a review series on Imaging in breast cancer, edited by David A Mankoff.
Other articles in the series can be found online at http://breast-cancer-research.com/articles/review-series.asp?series=bcr_imaging
Abbreviations
- DCE:
-
dynamic contrast-enhanced
- MR:
-
magnetic resonance
- MRI:
-
magnetic resonance imaging
- MRS:
-
magnetic resonance spectroscopy
- MRSI:
-
magnetic resonance spectroscopic imaging
- SVS:
-
single-voxel spectroscopy
- tCho:
-
total choline-containing compounds
- [tCho]:
-
concentration of total choline-containing compounds.
References
Daly PF, Cohen JS: Magnetic resonance spectroscopy of tumors and potential in vivo clinical applications: a review. Cancer Res. 1989, 49: 770-779.
Leach MO, Verrill M, Glaholm J, Smith TAD, Collins DJ, Payne GS, Sharp JC, Ronen SM, McCready VR, Powles TJ, et al: Measurements of human breast cancer using magnetic resonance spectroscopy: a review of clinical measurement and a report of localized 31P measurements of response to treatment. NMR Biomed. 1998, 11: 314-340. 10.1002/(SICI)1099-1492(1998110)11:7<314::AID-NBM522>3.0.CO;2-Z.
Sijens PE, Wijrdeman HK, Moerland MA, Bakker CJG, Vermeulen JWAH, Luyten PR: Human breast cancer in vivo: H-1 and P-31 MR spectroscopy at 1.5 T. Radiology. 1988, 169: 615-620.
Jagannathan NR, Singh M, Govindaraju V, Raghunathan P, Choshic O, Julka PK, Rath GK: Volume localized in vivo proton MR spectroscopy of breast carcinoma: variation of water-fat ratio in patients receiving chemotherapy. NMR Biomed. 1998, 11: 414-422. 10.1002/(SICI)1099-1492(199812)11:8<414::AID-NBM537>3.0.CO;2-W.
Thomas MA, Binesh N, Yue K, DeBruhl N: Volume-localized two-dimensional correlated magnetic resonance spectroscopy of human breast cancer. J Magn Reson Imaging. 2001, 14: 181-186. 10.1002/jmri.1170.
Roebuck JR, Cecil KM, Schnall MD, Lenkinski RE: Human breast lesions: characterization with proton MR spectroscopy. Radiology. 1998, 209: 269-275.
Gribbestad IS, Singstad TE, Nilsen G, Fjosne HE, Engan T, Haugen OA, Rinck PA: In vivo 1H MRS of normal breast and breast tumors using dedicated double breast coil. J Magn Reson Imaging. 1998, 8: 1191-1197.
Kvistad KA, Bakken IJ, Gribbestad IS, Ehrnholm B, Lundgren S, Fjosne HE, Haraldseth O: Characterization of neoplastic and normal human breast tissues with in vivo 1H MR spectroscopy. J Magn Reson Imaging. 1999, 10: 159-164. 10.1002/(SICI)1522-2586(199908)10:2<159::AID-JMRI8>3.0.CO;2-0.
Yeung DK, Cheung HS, Tse GM: Human breast lesions: characterization with contrast-enhanced in vivo proton MR spectroscopy – initial results. Radiology. 2001, 220: 40-46.
Cecil KM, Schnall MD, Siegelman ES, Lenkinski RE: The evaluation of human breast lesions with magnetic resonance imaging and proton magnetic resonance spectroscopy. Breast Cancer Res Treat. 2001, 68: 45-54. 10.1023/A:1017911211090.
Jagannathan NR, Kumar M, Seenu V, Coshic O, Dwivedi SN, Julka PK, Srivastava A, Rath GK: Evaluation of total choline from in vivo volume localized proton MR spectroscopy and its response to neoadjuvant chemotherapy in locally advanced breast cancer. Br J Cancer. 2001, 84: 1016-1022. 10.1054/bjoc.2000.1711.
Mackinnon WB, Barry PA, Malycha PL, Gillett DJ, Russell P, Lean CL, Doran ST, Barraclough BH, Bilous M, Mountford CE: Fine-needle biopsy specimens of benign breast lesions distinguished from invasive cancer ex vivo with proton MR spectroscopy. Radiology. 1997, 204: 661-666.
Cheng LL, Chang W, Smith BL, Gonzalez RG: Evaluating human breast ductal carcinomas with high-resolution magic-angle spinning proton magnetic resonance spectrscopy. J Magn Reson. 1998, 135: 194-202. 10.1006/jmre.1998.1578.
Gribbestad IS, Sitter B, Lundgren S, Krane J, Axelson D: Metabolite composition in breast tumors examined by proton nuclear magnetic resonance spectroscopy. Anticancer Res. 1999, 19: 1737-1746.
Garwood M, DelaBarre L: The return of the frequency sweep: designing adiabatic pulses for contemporary NMR. J Magn Reson. 2001, 153: 155-177. 10.1006/jmre.2001.2340.
Jacobs MA, Barker PB, Bottomley PA, Bhujwalla Z, Bluemke DA: Proton magnetic resonance spectroscopic imaging of human breast cancer: a preliminary study. J Magn Reson Imaging. 2004, 19: 68-75. 10.1002/jmri.10427.
Bolan PJ, DelaBarre L, Baker EH, Merkle H, Everson LI, Yee D, Garwood M: Eliminating spurious lipid sidebands in 1H MRS of breast lesions. Magn Reson Med. 2002, 48: 215-222. 10.1002/mrm.10224.
Bolan PJ, Meisamy S, Baker EH, Lin J, Emory T, Nelson M, Everson LI, Yee D, Garwood M: In vivo quantification of choline compounds in the breast with 1H MR spectroscopy. Magn Reson Med. 2003, 50: 1134-1143. 10.1002/mrm.10654.
Bakken IJ, Gribbestad IS, Singstad TE, Kvistad KA: External standard method for the in vivo quantification of choline-containing compounds in breast tumors by proton MR spectroscopy at 1.5 Tesla. Magn Reson Med. 2001, 46: 189-192. 10.1002/mrm.1175.
Katz-Brull R, Lavin PT, Lenkinski RE: Clinical utility of proton magnetic resonance spectroscopy in characterizing breast lesions. J Natl Cancer Inst. 2002, 94: 1197-1203.
Huang W, Fisher PR, Dulaimy K, Tudorica LA, O'Hea B, Button TM: Detection of breast malignancy: diagnostic MR protocol for improved specificity. Radiology. 2004, 232: 585-591.
Meisamy S, Bolan PJ, Baker EH, Pollema MG, Le CT, Kelcz F, Lechner MC, Luikens BA, Carlson RA, Brandt KR, et al: The value of adding quantitative 1H MRS for improving diagnostic accuracy of breast MRI: preliminary results from an observer performance study at 4 Tesla. Radiology. 2005,
Meisamy S, Bolan PJ, Baker EH, Bliss RL, Gulbahce E, Everson LI, Nelson MT, Emory TH, Tuttle TM, Yee D, et al: Predicting response to neoadjuvant chemotherapy of locally advanced breast cancer with in vivo 1H MRS: a pilot study at 4 Tesla. Radiology. 2004, 233: 424-431.
Kim J-K, Park S-H, Lee HM, Lee Y-H, Sung N-K, Chung D-S, Kim O-D: In vivo 1H-MRS evaluation of malignant and benign breast disease. Breast. 2003, 12: 179-182. 10.1016/S0960-9776(03)00012-2.
Tse GMK, Cheung HS, Pang L-M, Chu WCW, Law BKB, Kung FYL, Yeung DKW: Characterization of lesions of the breast with proton MR spectroscopy: comparison of carcinomas, benign lesions, and phyllodes tumors. Am J Roentgenol. 2003, 181: 1267-1272.
Acknowledgements
The authors acknowledge support from the NIH (grants CA92004, RR08079, and RR00400), the DOD Breast Cancer Research program (DAMD 17-01-1-0331), the Lillian Quist–Joyce Henline Chair in Biomedical Research, the Tickle Family Land Grant Endowment in Breast Cancer Research, and the MIND Institute.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Bolan, P.J., Nelson, M.T., Yee, D. et al. Imaging in breast cancer: Magnetic resonance spectroscopy. Breast Cancer Res 7, 149 (2005). https://doi.org/10.1186/bcr1202
Published:
DOI: https://doi.org/10.1186/bcr1202