
Abstract
Introduction
This randomized, controlled study on patients with polymyositis or dermatomyositis was based on three hypotheses: patients display impaired endurance due to reduced aerobic capacity and muscle weakness, endurance training improves their exercise performance by increasing the aerobic capacity, and endurance training has general beneficial effects on their health status.
Methods
In the first part of this study, we compared 23 patients with polymyositis or dermatomyositis with 12 age- and gender-matched healthy controls. A subgroup of patients were randomized to perform a 12-week endurance training program (exercise group, n = 9) or to a non-exercising control group (n = 6). We measured maximal oxygen uptake (VO2 max) and the associated power output during a progressive cycling test. Endurance was assessed as the cycling time to exhaustion at 65% of VO2 max. Lactate levels in the vastus lateralis muscle were measured with microdialysis. Mitochondrial function was assessed by measuring citrate synthase (CS) and β-hydroxyacyl-CoA dehydrogenase (β-HAD) activities in muscle biopsies. Clinical improvement was assessed according to the International Myositis Assessment and Clinical Studies Group (IMACS) improvement criteria. All assessors were blinded to the type of intervention (that is, training or control).
Results
Exercise performance and aerobic capacity were lower in patients than in healthy controls, whereas lactate levels at exhaustion were similar. Patients in the exercise group increased their cycling time, aerobic capacity and CS and β-HAD activities, whereas lactate levels at exhaustion decreased. Six of nine patients in the exercise group met the IMACS improvement criteria. Patients in the control group did not show any consistent changes during the 12-week study.
Conclusions
Polymyositis and dermatomyositis patients have impaired endurance, which could be improved by 12 weeks of endurance training. The clinical improvement corresponds to increases in aerobic capacity and muscle mitochondrial enzyme activities. The results emphasize the importance of endurance exercise in addition to immunosuppressive treatment of patients with polymyositis or dermatomyositis.
Trial registration
ClinicalTrials.gov: NCT01184625
Similar content being viewed by others


Introduction
The idiopathic inflammatory myopathies, including polymyositis (PM) and dermatomyositis (DM), are characterized by muscle weakness and poor muscle endurance, especially in proximal muscles [1, 2]. The mechanisms that lead to muscle weakness are not fully clarified but both immune-mediated and non-immune-mediated mechanisms are thought to be involved in the disease process and the latter mechanisms include endoplasmic reticulum (ER) stress, hypoxia, autophagy and mitochondrial pathology [3–5]. Despite recommended treatment with high doses of glucocorticoids and immunosuppressive agents, few patients can regain their former muscle performance and the reason for this is not fully understood [6, 7].
Abnormalities in energy metabolism has been observed in inflammatory myopathies, including PM and DM [8]. Patients with established PM/DM display fewer oxidative slow-twitch type I muscle fibers and lower aerobic capacity compared to healthy controls [9–11]. Thickened endothelial cells, reduced capillary blood supply and low total number of capillaries may impair oxygen transport to the muscle fibers in inflammatory myopathies [12, 13]. Accordingly, up-regulation of hypoxia-related proteins, such as vascular endothelial growth factor (VEGF) and hypoxia-inducible factor-1 (HIF-1), has been observed in muscle of patients with inflammatory myopathies [13, 14].
Traditionally, physical exercise has not been recommended to patients with PM/DM [6]. However, recent exercise studies in patients with established PM/DM revealed benefits and safety [6, 15], with a potential to prevent muscle loss due to muscle inflammation, physical inactivity and systemic glucocorticoid treatment [16, 17]. For instance, a resistance exercise program resulted in modulations of gene expression transcripts associated with inflammation (down-regulation), fibrosis (down-regulation) and aerobic metabolism (up-regulation) [18]. However, available studies have limitations and it is not possible to recommend one exercise program over another, indicating a need for randomized controlled trials [6, 15].
The major objective of this randomized, controlled, multicenter study was to determine whether endurance exercise can improve muscle function in patients with PM/DM in a chronically stable disease phase. We tested the following hypotheses:
-
1.
Compared to age- and gender-matched healthy controls, PM/DM patients display impaired performance during endurance exercise due to reduced aerobic capacity and muscle weakness (that is, an inability to fully activate the contractile machinery). To test this hypothesis, patients and healthy controls performed endurance exercise and we assessed performance, aerobic capacity, heart rate, muscular lactate concentration and self-reported exertion level.
-
2.
Endurance training improves exercise performance in PM/DM patients by increasing muscle aerobic capacity. To test this hypothesis, patients were randomized into an exercise group (EG), performing a 12-week endurance training program, and a non-exercising control group (CG). Endurance exercise performance, muscular lactate concentration, aerobic capacity and mitochondrial capacity in muscle biopsies were assessed before and after the intervention period.
-
3.
Endurance training has a general beneficial effect on the health status of PM/DM patients. The disease activity was assessed before and after the training period according to the International Myositis Assessment and Clinical Studies Group (IMACS) improvement criteria.
Methods
Study design
In the first part of the study we compared patients with PM/DM with age- and gender-matched healthy controls. The controlled part of the study was a hypothesis-driven randomized controlled trial evaluating effects of a supervised 12-week endurance exercise program compared to a non-interventional control group.
Patients and healthy controls
Patients (n = 23) were recruited from 2007 to 2011 from three rheumatology units in Sweden: Karolinska University Hospital, Stockholm; Sahlgrenska University Hospital, Gothenburg; and Uppsala University Hospital, Uppsala, Sweden. Inclusion criteria: a) diagnosis of definite or probable PM or DM [19, 20]; b) age ≥18 years; c) duration since diagnosis more than six months; d) exercising one time or less a week; e) stable medication for at least one month. Exclusion criteria: a) severe heart or lung conditions; b) severe osteoporosis; c) not being able to exercise.
Twelve healthy controls (HC) matched for age, gender and physical activity level were identified among each patient's non-genetic, related family members and friends and health care professionals. Inclusion criteria: a) age ≥18 years; b) exercising one time or less a week. Exclusion criteria: a) chronic musculoskeletal disorder; b) severe osteoarthritis or osteoporosis; c) severe heart or lung conditions. All participants gave informed consent to participate in the study, which was approved by the local ethics committees at Karolinska University Hospital, Sahlgrenska University Hospital and Uppsala University Hospital. The study followed the World Medical Association's 2008 Declaration of Helsinki.
Aerobic capacity
Ergometer cycle maximal oxygen uptake (VO2 max) tests were performed by patients and HC at baseline and by patients after the 12-week intervention (training or control) period. Different cycling protocols were used for patients and HC because a previous study showed approximately 50% lower VO2 max in patients with PM/DM compared to HC [11]. Thus, the patients started at 30 to 40 W and the required power output was increased with 10 W every minute, while the HC started at 50 W and the increase was 15 W every minute. The VO2 max was determined by incremental cycling to exhaustion. Pulmonary minute ventilation and gas exchange (O2 uptake and CO2 output) were measured breath by breath (Sensor Medics, V max 229™, Yorba Linda, CA, USA). The system was calibrated for airflow and gas exchange before each test. VO2 max was defined as the highest O2 uptake rate measured during the test and is expressed as l min-1 and as ml min-1 (kg body weight)-1; the power performed (in W) at the time of VO2 max was recorded. At VO2 max, we also measured the respiratory exchange ratio (RQ) defined as the ratio between the exhaled CO2 and the inhaled O2. Electrocardiography was used to continuously follow the heart rate and the maximum heart rate was recorded. At the end of the test we recorded the self-reported ratings of peripheral exertion (lower extremity) and central exertion on the Borg RPE scale (6 to 20) [21].
Cycling endurance test
Cycling endurance tests were performed by patients and HC at baseline and by patients after the 12-week intervention (training or control) period. Cycling was performed at a power requiring 65% of the VO2 max obtained in the baseline aerobic capacity test (see above) and was continued until exhaustion. The tests were supervised by the same physical therapist throughout the study. At exhaustion, self-reported peripheral and central exertions were recorded and the heart rate was measured.
Lactate measurements
The extracellular concentration of lactate was measured in vivo with microdialysis. Two thin catheters with a 3 cm long membrane with a diameter of 0.5 mm (CMA 63) were inserted in the vastus lateralis, 2 cm apart, under local anesthesia [22]. A reference catheter was inserted in subcutaneous abdominal fat tissue. The microdialysis experiments were performed in patients and HC at baseline and in patients also after 12 weeks intervention (training or control) by the same two physicians, nurse and physical therapist throughout the study. The microdialysis probes were perfused with a physiological solution at a flow rate of 1 μl min-1. Water soluble substances in the interstitial fluid diffuse across the semipermeable dialysis membrane and enter the perfusate, which was collected in small vials. The cycling endurance test (see above) started after an 80-minute equilibration at rest, during which one vial of perfusate per catheter was collected every 20 minutes. After the endurance test, subjects rested for 60 minutes while vials with perfusate were collected every 20 minutes. Analysis of lactate concentration was made directly in a Clinical Microdialysis Analyzer (ICSUS, CMA, Solna, Sweden). Vials collected from the vastus lateralis muscle during the 20 minutes directly after cycling to exhaustion showed the highest lactate concentrations and the mean lactate concentration in vials obtained from the two catheters at this time interval was used in subsequent assessments.
Muscle biopsies and measurements of mitochondrial enzyme activities
Muscle biopsies were taken from the vastus lateralis muscle under local anesthesia using a semi-open technique [23]. Biopsies were taken from the patients before and after the 12-week +/- endurance training. Due to technical reasons, biopsies were only taken from patients who were recruited at the Karolinska University Hospital and at the Uppsala University Hospital. We measured the activities of two mitochondrial enzymes, citrate synthase (CS) and β-hydroxyacyl-CoA dehydrogenase (β-HAD), which reflect the mitochondrial volume to cell volume ratio and the capacity for fatty acid β-oxidation, respectively [24, 25]. Muscle biopsies were freeze dried, dissected free of non-muscle constituents and weighed. Tissue was then homogenized with ground glass homogenizers in ice-cold buffer (HxB) consisting of 50 mM KH2PO4; 1 mM EDTA, 0.05% (vol/vol) Triton X-100, pH 7.5. The homogenate was centrifuged at 1,400 × g for one minute (4°C). Aliquots of the supernatant were analyzed for CS and β-HAD with standard spectrophotometric techniques [26, 27]. Enzyme activities were assayed at room temperature (approximately 22°C) under conditions that yielded linearity with respect to extract volume and time (data not shown). Protein content was measured in the supernatant with the Bradford assay (Bio-Rad Laboratories AB, Sundbyberg, Sweden and activities were adjusted for protein content.
Clinical outcome measures
Assessment of disease activity was performed using the proposed preliminary consensus core measures developed for PM/DM patients by IMACS [7, 28]. The core measures include: patients and physicians global disease activity assessments recorded on a Visual Analogue Scale (VAS, 0 to 100); Manual Muscle Testing-8 (MMT (muscle strength), 0 to 10 in eight muscle groups); Health Assessment Questionnaire (HAQ (limitation in daily activities), 0 to 3); measurement of the blood serum activity of the muscle enzyme creatine phosphokinase (s-CPK, μcat l-1); and assessment of the degree of disease activity in six organ systems other than skeletal muscle using the myositis intention to treat activity index (MITAX, 0 to 1). We used the proposed core measures and the assessment of disease activity in the skeletal muscle system rated on VAS (0 to 100). [28–30]
Damage was measured by Myositis disease Damage Index (MDI) proposed by IMACS, which involves clinical assessment of the degree of disease damage in 11 organ systems and the physician global damage tool on a VAS (0 to 100) [28, 29, 31].
The clinical assessment of each patient was performed by the same experienced physician before and after the 12-week intervention period and the assessor was blinded to the type of intervention, (that is, training or control).
Endurance exercise training
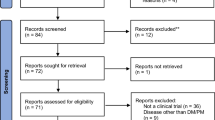
A subgroup of the PM/DM patients was randomized, using a randomization list, either to an exercise group (EG) or a control group (CG) (Figure 1). An independent nurse who was responsible for the randomization then contacted the exercise coach at each center to inform about group allocation. The EG performed an approximately one-hour exercise program three times a week for 12 weeks. The exercise program consisted of five-minute warm-up cycling at 50% of VO2 max, which was followed by up to 30 minutes of more intense cycling where the intensity was gradually increased during the training period aiming at 70% of VO2 max. This was followed by 20 minutes of muscular endurance exercise engaging both the upper and lower limbs at 30 to 40% of one voluntary repetition maximum. The program ended with a cool-down and stretch. At each participating center, the EG was supervised by the same physical therapist. The patients in the CG were instructed not to change their physical activity level during the 12-week intervention period, but they were invited to perform the same endurance exercise program after the intervention period.

Flow diagram for patients according to the CONSORT randomized, controlled trials of non-pharmacologic treatment.
All patients used exercise diaries to register their physical activities during the 12-week intervention period. All nine patients randomized into the EG participated in the training program as scheduled according to their exercise diary. Seven patients were randomized to the CG; however, one started on her own initiative another endurance training program; thus six patients were analyzed in the CG.
Statistical analyses
Data are presented individually, as mean (± SD) or as median (range). Student's unpaired t-test was used to detect differences between patients and HC. For evaluation of the effect of endurance training, measurements performed before and after the intervention period were compared using Student's paired sample t-test. The significance level was set to P <0.05. A power test was performed assuming changes in physiological measurements after endurance training being 30 ± 20% of the control value. With a power of 0.80 and an alpha of 0.05, this gives a sample size of six. Based on this, we aimed for nine patients in the EG, but some analyses were performed with n = 7 (VO2 max measurements) or n = 3 (mitochondrial enzyme activities).
We used the proposed definition by IMACS to define improvement in disease activity during the intervention period [32]. To be a responder, a patient should improve ≥20% in ≥50% of IMACS core measures with no more than two worse by ≥25%, which could not include measures of muscle function (MMT). Improvement in muscle function and exercise performance to the 12-week endurance exercise was evaluated and presented for the individual patients. A responder was defined as improvement by ≥20% in MMT and/or cycling time at 12-week follow-up compared to baseline [33].
Statistical analyses were made using Statistica 10.0 (StatSoft, Inc., Tulsa, Ok, USA) or SigmaStat 3.1 (Systat Software, Inc., Point Richmond, CA, USA).
Results
Patients versus healthy controls
Twenty-three PM or DM patients and 12 HC participated in the initial assessments and their respective demographics are presented in Table 1. The patients were in a stable disease phase with unchanged medication for at least one month before inclusion in the study and had a low disease activity.
We used a progressive ergometer cycle test to measure VO2 max and the corresponding power output. PM/DM patients had an approximately 25% lower VO2 max (P <0.01) and an approximately 35% lower power output (P <0.001) than HC (Figure 2A and Table 2). On the other hand, the RQ at VO2 max, the maximum heart rate, and Borg ratings of peripheral and central exertion were similar in patients and HC (Table 2).

Polymyositis and dermatomyositis patients have lower aerobic capacity and endurance exercise performance than healthy controls. A. VO2 max vs. the corresponding power output obtained in the progressive bicycle test. B.Concentration of lactate in vastus lateralis muscle dialysate after cycling vs. cycling time in the endurance test performed at the same relative work load in all individuals. Individual data from 23 patients (open circles) and 12 healthy controls (open triangles). Mean data (± SD) from patients (filled circle) and healthy controls (filled triangle) are also shown.
An endurance cycling test was performed with a constant power, which in each individual was set to that requiring 65% of VO2 max; that is, the mean power during this test was markedly lower in patients than in HC. The lactate concentration in the vastus lateralis muscles was measured with microdialysis after this endurance test. The cycling time to exhaustion was approximately 45% shorter in the patients than in HC (P <0.001), despite the fact that patients cycled at a lower power (Figure 2 and Table 2). On the other hand, the lactate concentration, the percentage of max heart rate and Borg ratings of peripheral and central exertion were similar in patients and HC at the end of the endurance test (Table 2).
Effects of a 12-week endurance exercise program
A subgroup of the patients (n = 15) with reliable metabolic marker data was included in the analysis of the effect of a 12-week intervention period. All patients tolerated the exercise program well and no adverse events were noted.
All patients in the EG increased their time to exhaustion in the cycling endurance test by ≥20% and mean data show an approximately doubled cycling time (P <0.01; Figure 3A and Table 3). Moreover, lactate measured after the endurance test was about 35% lower after than before the training period (P <0.01). Conversely, the heart rate at the end of the cycling test and Borg ratings of peripheral and central exertion were similar before and after the training period (Table 3). The patients in the CG, who kept a stable physical activity level, showed no consistent changes in either cycling performance or lactate concentration during the 12 weeks of the study (Figure 3Band Table 3). Their heart rate and Borg ratings at exhaustion were also similar before and after the 12 weeks.

Exercise and aerobic capacity are increased in myositis patients after 12 weeks endurance training. A. Individual data of the concentration of lactate in muscle dialysate after cycling vs. cycling time (at the same absolute work load for each subject) obtained in nine patients before (open circles) and after (filled circles) endurance training. Mean data (± SD) before (open triangle) and after (filled triangle) training are also shown. B. Same as in A but for six patients in the control group (no training). Mean data (± SD) of VO2 max (C) and the corresponding power (D) before (white bars) and after (black bars) the 12-week intervention period in the exercise group (EG, n = 7) and the control group (CG, n = 5). E and F show mean data (± SD) of the change in VO2 max and power after vs. before the intervention period in individual subjects.
Reliable VO2 max tests were performed in seven patients in the EG and in five patients in the CG (Figure 3C-F). VO2 max and power output at VO2 max were higher in all patients in the EG after the endurance exercise period and mean values increased by approximately 20% (P <0.01; Table 3). Conversely, VO2 max was slightly decreased in the CG after the 12 weeks, whereas the power output did not change (Table 3).
The improved cycling performance and VO2 max after training might be due to increased muscular mitochondrial respiration. To test this possibility, we measured the activities of two mitochondrial enzymes, CS and β-HAD, in muscle biopsies. All three EG patients tested had a major improvement in cycling performance (Figure 4A), CS activity (Figure 4B) and β-HAD activity (Figure 4C). Thus, mean data show significant increases in cycling performance (Figure 4D, P <0.05), CS activity (Figure 4E, P <0.001), and β-HAD activity (Figure 4F, P <0.05; Table 3). On the other hand, there were no significant changes in cycling time, CS activity or β-HAD activity in the CG (Figure 4D-F and Table 3).

Increased mitochondrial enzyme activities in muscles of myositis patients after 12 weeks of endurance training. Individual data from three patients obtained before and after 12 weeks of endurance training for cycling time at the same absolute work load for each subject (A) and the activity of two mitochondrial enzymes, CS (B) and β-HAD (C), in muscle biopsies from vastus lateralis muscle. D-F. Mean data of the difference after vs. before training (n = 3); data for five patients in the control group (no training) are also shown.
Six out of nine patients in the EG were responders to the endurance exercise intervention according to the IMACS criteria (Table 4). Note that there was a slight discrepancy between IMACS responders (six out of nine) and responders in relation to muscle endurance (nine out of nine; see Figure 3A, Table 4). Conversely, only one out of six patients in the CG was improved according to the IMACS criteria (Table 4). This patient showed improvement in activity limitation (HAQ), physician's global disease activity and patient's global disease activity, whereas no improvement was observed in muscle endurance (cycling time) or muscle strength (MMT).
Discussion
In this study we report a substantially lower endurance exercise capacity in patients with PM/DM in a stable disease phase compared to healthy controls matched for age, gender and level of physical activity. We also show that 12 weeks of endurance training markedly improved endurance exercise performance in the patients and this improvement was accompanied by increased aerobic capacity. The training period also resulted in a general clinical improvement in the majority of patients.
In accordance with our first hypothesis, we show a decreased performance during endurance exercise in PM/DM patients compared to age- and gender-matched HC. The impaired performance in the patients was accompanied by a lower VO2 max and, hence, decreased aerobic capacity, which is also in agreement with our hypothesis. We also hypothesized that the patients' exercise performance would be limited by weakness and inability to adequately activate the exercising muscles. The results, however, show no difference between patients and HC in extracellular lactate levels, RQ values, experienced exertion level or percentage of maximum heart rate in the fatigued state; all these four measures would be lower if exercise ended prematurely due to improper muscle activation [34]. Nevertheless, the present cycling exercise requires relatively low muscle power output and exercises requiring a larger fraction of the available muscle force may well be limited by muscle weakness. For instance, such exercises like "walking up one flight of stairs" and "getting up from the ground/floor" have been reported as difficult to perform by patients with PM/DM [35, 36]. Thus, in the present study patients with PM/DM show decreased performance during cycling endurance exercise and this impairment can be explained by reduced aerobic capacity, which is in agreement with a previous study [11]. Furthermore, we suggest that an important mechanism contributing to the reduced aerobic capacity and impaired endurance performance in the patients is a low mitochondrial capacity in muscle. Others have observed that a local inflammatory environment is associated with a mitochondrial dysfunction [37]. It is worth noting that the patients in the present study, as well as in previous studies, have been given conventional immunosuppressive treatment for at least six months, which consequently is not sufficient to regain full muscle endurance performance. In addition, long-term glucocorticoid treatment may cause mitochondrial dysfunction [38] and atrophy in skeletal muscle [39] and these deleterious effects may be aggravated when combined with low physical activity [40], which could be one explanation for persistent impaired performance in PM/DM patients after immunosuppressive treatment.
Our results show a marked improvement in endurance exercise performance in the PM/DM patients after 12 weeks endurance training, which is in agreement with our second hypothesis. This improvement could be explained by increased aerobic capacity after the training period as judged from a lower lactate level and an unchanged relative maximum heart rate in the fatigued state despite a longer cycling time; increased VO2 max and power output at VO2 max; and increased activity of the two mitochondrial enzymes CS and β-HAD. These findings of increased mitochondrial capacity by endurance training in patients with PM/DM are in accordance with previous studies showing improved aerobic capacity and up-regulated transcription of genes for proteins involved in aerobic metabolism in PM/DM patients exposed to a period of physical exercise [17, 18, 41]. It is worth noting that all patients exposed to the training program improved their exercise performance, that is, also patients with initially severely decreased muscle function and endurance capacity. Thus, endurance training is effective in PM/DM patients even when they are in a chronic stable disease phase with severe muscle dysfunction. It would be of great value to know if endurance training is beneficial also in an acute disease phase, but this is outside the scope of the present study.
In the present study, we measured extracellular lactate concentration in muscle after an individually determined cycling endurance test; that is, subjects cycled until exhaustion at a power requiring 65% of their VO2 max at baseline. The lactate concentration and, hence, the extent of anaerobic metabolism required, was similar in PM/DM patients and healthy controls at exhaustion, despite the fact that healthy controls cycled for longer times and at higher power outputs (see Figure 2). A markedly different picture would emerge if we instead would have used a fixed endurance test, that is, the same absolute power output and duration in both groups. The power output and duration tolerated by the PM/DM patients would then be rather mild for the healthy controls and markedly higher lactate levels would be expected in patients at the end of the test. In line with these assumptions, a recent case study showed markedly higher lactate levels after a fixed endurance test in a PM patient than in healthy controls [42]. Furthermore, after five weeks of endurance training, the PM patient had a lower lactate concentration at the end of the endurance test [42], which is in good agreement with our present results (see Figure 3).
In accordance with our third hypothesis, a majority (six out of nine) of the patients exposed to the training program improved concerning disease activity according to IMACS improvement criteria. In a previous seven-week resistance exercise study, two out of seven patients improved according to the same criteria [43]. These results indicate that endurance exercise, longer exercise duration, or a combination of both might be more beneficial than resistance exercise for PM/DM patients in a stable chronic disease phase.
One limitation in this study is that the median age of the HC group was seven years lower than the patients, which might exaggerate the differences between the two groups. However, it should be noted that there was no statistical difference in age between the two groups and they had a similar level of physical exercise. Another potential limitation is the relatively low number of patients in the EG and the CG. Since the patients included in this study were in a stable disease phase, no consistent changes during 12 weeks was expected in the CG and this is also what our results show. A power analysis showed that for physiological assessments we needed measurements from at least six subjects before and after the endurance exercise period. Nine patients were included in the EG, but all measurements were not successfully performed both before and after training in each subject. This limitation resulted in measurements of mitochondrial enzyme activities being clearly underpowered with only three patients in the EG. However, all three subjects showed clear increases in both CS and β-HAD activities after the training period (see Figure 4), which from a physiological perspective fits with the concomitant increases in aerobic capacity and cycling performance (see Figure 3). Finally, it would have been of interest to quantify a potential relationship between reduced disease activity and increased exercise performance in the EG after the training period. Unfortunately, the IMACS six-item core set does not consist of one total score and is, therefore, not suitable for quantifying relationships. However, we could demonstrate that all patients in the EG with reduced disease activity also improved in exercise performance (≥20 % increased cycling time).
Conclusions
In conclusion, PM/DM patients show impaired endurance performance during cycling exercise due to reduced aerobic capacity. After 12 weeks of endurance training, PM/DM patients increased their mitochondrial enzyme activities in muscle, increased aerobic capacity, decreased disease activity and markedly improved exercise performance. These results emphasize that in order to improve muscle performance, PM/DM patients should be prescribed physical endurance exercise in combination with the recommended immunosuppressive treatment.
Abbreviations
- β-HAD:
-
β-hydroxyacyl-CoA dehydrogenase
- CG:
-
control group
- CS:
-
citrate synthase
- DM:
-
dermatomyositis
- EG:
-
exercise group
- ER:
-
endoplasmic reticulum
- HAQ:
-
Health Assessment Questionnaire
- HC:
-
healthy controls
- HIF-1:
-
hypoxia-inducible factor-1
- IMACS:
-
International Myositis Assessment and Clinical Studies Group
- MDI:
-
myositis disease damage index
- MITAX:
-
myositis intention to treat activity index
- MMT:
-
Manual Muscle Testing
- PM:
-
Polymyositis
- s-CPK:
-
the blood serum activity of the muscle enzyme creatine phosphokinase
- VAS:
-
Visual Analogue Scale
- VEGF:
-
vascular endothelial growth factor
- VO2 max:
-
maximal oxygen uptake
References
Hengstman GJ, van den Hoogen FH, van Engelen BG: Treatment of the inflammatory myopathies: update and practical recommendations. Expert Opin Pharmacother. 2009, 10: 1183-1190. 10.1517/14656560902913815.
Harris-Love MO, Shrader JA, Koziol D, Pahlajani N, Jain M, Smith M, Cintas HL, McGarvey CL, James-Newton L, Pokrovnichka A, Moini B, Cabalar I, Lovell DJ, Wesley R, Plotz PH, Miller FW, Hicks JE, Rider LG: Distribution and severity of weakness among patients with polymyositis, dermatomyositis and juvenile dermatomyositis. Rheumatology (Oxford). 2009, 48: 134-139.
Rayavarapu S, Coley W, Nagaraju K: An update on pathogenic mechanisms of inflammatory myopathies. Curr Opin Rheumatol. 2011, 23: 579-584. 10.1097/BOR.0b013e32834b41d2.
Henriques-Pons A, Nagaraju K: Nonimmune mechanisms of muscle damage in myositis: role of the endoplasmic reticulum stress response and autophagy in the disease pathogenesis. Curr Opin Rheumatol. 2009, 21: 581-587. 10.1097/BOR.0b013e3283319265.
Zong M, Lundberg IE: Pathogenesis, classification and treatment of inflammatory myopathies. Nat Rev Rheumatol. 2011, 7: 297-306. 10.1038/nrrheum.2011.39.
Alexanderson H, Lundberg IE: Exercise as a therapeutic modality in patients with idiopathic inflammatory myopathies. Curr Opin Rheumatol. 2012, 24: 201-207. 10.1097/BOR.0b013e32834f19f5.
Miller FW: New approaches to the assessment and treatment of the idiopathic inflammatory myopathies. Ann Rheumatic Dis. 2012, 71 (Suppl 2): i82-85. 10.1136/annrheumdis-2011-200587.
Park JH, Olsen NJ: Utility of magnetic resonance imaging in the evaluation of patients with inflammatory myopathies. Curr Rheumatol Rep. 2001, 3: 334-345. 10.1007/s11926-001-0038-x.
Dastmalchi M, Alexanderson H, Loell I, Stahlberg M, Borg K, Lundberg IE, Esbjornsson M: Effect of physical training on the proportion of slow-twitch type I muscle fibers, a novel nonimmune-mediated mechanism for muscle impairment in polymyositis or dermatomyositis. Arthritis Rheum. 2007, 57: 1303-1310. 10.1002/art.22996.
Loell I, Helmers SB, Dastmalchi M, Alexanderson H, Munters LA, Nennesmo I, Lindroos E, Borg K, Lundberg IE, Esbjörnsson M: Higher proportion of fast-twitch (type II) muscle fibres in idiopathic inflammatory myopathies-evident in chronic but not in untreated newly diagnosed patients. Clin Physiol Funct Imaging. 2011, 31: 18-25. 10.1111/j.1475-097X.2010.00973.x.
Wiesinger GF, Quittan M, Nuhr M, Volc-Platzer B, Ebenbichler G, Zehetgruber M, Graninger W: Aerobic capacity in adult dermatomyositis/polymyositis patients and healthy controls. Arch Phys Med Rehabil. 2000, 81: 1-5. 10.1016/S0003-9993(00)90212-0.
Cea G, Bendahan D, Manners D, Hilton-Jones D, Lodi R, Styles P, Taylor DJ: Reduced oxidative phosphorylation and proton efflux suggest reduced capillary blood supply in skeletal muscle of patients with dermatomyositis and polymyositis: a quantitative 31P-magnetic resonance spectroscopy and MRI study. Brain. 2002, 125: 1635-1645. 10.1093/brain/awf163.
Grundtman C, Tham E, Ulfgren AK, Lundberg IE: Vascular endothelial growth factor is highly expressed in muscle tissue of patients with polymyositis and patients with dermatomyositis. Arthritis Rheum. 2008, 58: 3224-3238. 10.1002/art.23884.
Probst-Cousin S, Neundörfer B, Heuss D: Microvasculopathic neuromuscular diseases: lessons from hypoxia-inducible factors. Neuromuscul Disord. 2010, 20: 192-197. 10.1016/j.nmd.2010.01.005.
Habers GE, Takken T: Safety and efficacy of exercise training in patients with an idiopathic inflammatory myopathy - a systematic review. Rheumatology (Oxford). 2011, 50: 2113-2124. 10.1093/rheumatology/ker292.
Nader GA, Lundberg IE: Exercise as an anti-inflammatory intervention to combat inflammatory diseases of muscle. Curr Opin Rheumatol. 2009, 21: 599-603. 10.1097/BOR.0b013e3283319d53.
Wiesinger GF, Quittan M, Aringer M, Seeber A, Volc-Platzer B, Smolen J, Graninger W: Improvement of physical fitness and muscle strength in polymyositis/dermatomyositis patients by a training programme. Br J Rheumatol. 1998, 37: 196-200. 10.1093/rheumatology/37.2.196.
Nader GA, Dastmalchi M, Alexanderson H, Grundtman C, Gernapudi R, Esbjornsson M, Wang Z, Ronnelid J, Hoffman EP, Nagaraju K, Lundberg IE: A longitudinal, integrated, clinical, histological and mRNA profiling study of resistance exercise in myositis. Mol Med. 2010, 16: 455-464.
Bohan A, Peter JB: Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975, 292: 344-347. 10.1056/NEJM197502132920706.
Bohan A, Peter JB: Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975, 292: 403-407. 10.1056/NEJM197502202920807.
Borg GA: Perceived exertion. Exerc Sport Sci Rev. 1974, 2: 131-153.
Lundberg G, Olofsson P, Ungerstedt U, Jansson E, Sundberg CJ: Lactate concentrations in human skeletal muscle biopsy, microdialysate and venous blood during dynamic exercise under blood flow restriction. Pflugers Arch. 2002, 443: 458-465. 10.1007/s004240100706.
Dorph C, Nennesmo I, Lundberg IE: Percutaneous conchotome muscle biopsy. A useful diagnostic and assessment tool. J Rheumatol. 2001, 28: 1591-1599.
Holloszy JO, Coyle EF: Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J Appl Physiol. 1984, 56: 831-838.
Reisch AS, Elpeleg O: Biochemical assays for mitochondrial activity: assays of TCA cycle enzymes and PDHc. Methods Cell Biol. 2007, 80: 199-222.
Alp PR, Newsholme EA, Zammit VA: Activities of citrate synthase and NAD+-linked and NADP+-linked isocitrate dehydrogenase in muscle from vertebrates and invertebrates. Biochem J. 1976, 154: 689-700.
Bass A, Brdiczka D, Eyer P, Hofer S, Pette D: Metabolic differentiation of distinct muscle types at the level of enzymatic organization. Eur J Biochem. 1969, 10: 198-206. 10.1111/j.1432-1033.1969.tb00674.x.
Isenberg DA, Allen E, Farewell V, Ehrenstein MR, Hanna MG, Lundberg IE, Oddis C, Pilkington C, Plotz P, Scott D, Vencovsky J, Cooper R, Rider L, Miller F, International Myositis and Clinical Studies Group (IMACS): International consensus outcome measures for patients with idiopathic inflammatory myopathies. Development and initial validation of myositis activity and damage indices in patients with adult onset disease. Rheumatology (Oxford). 2004, 43: 49-54. 10.1093/rheumatology/keg427.
Miller FW, Rider LG, Chung YL, Cooper R, Danko K, Farewell V, Lundberg I, Morrison C, Oakley L, Oakley I, Pilkington C, Vencovsky J, Vincent K, Scott DL, Isenberg DA, International Myositis Outcome Assessment Collaborative Study Group: Proposed preliminary core set measures for disease outcome assessment in adult and juvenile idiopathic inflammatory myopathies. Rheumatology (Oxford). 2001, 40: 1262-1273. 10.1093/rheumatology/40.11.1262.
Sultan SM, Allen E, Oddis CV, Kiely P, Cooper RG, Lundberg IE, Vencovsky J, Isenberg DA: Reliability and validity of the myositis disease activity assessment tool. Arthritis Rheum. 2008, 58: 3593-3599. 10.1002/art.23963.
Sultan SM, Allen E, Cooper RG, Agarwal S, Kiely P, Oddis CV, Vencovsky J, Lundberg IE, Dastmalchi M, Hanna MG, Isenberg DA: Interrater reliability and aspects of validity of the myositis damage index. Ann Rheum Dis. 2011, 70: 1272-1276. 10.1136/ard.2010.142117.
Rider LG, Giannini EH, Brunner HI, Ruperto N, James-Newton L, Reed AM, Lachenbruch PA, Miller FW: International consensus on preliminary definitions of improvement in adult and juvenile myositis. Arthritis Rheum. 2004, 50: 2281-2290. 10.1002/art.20349.
Paulus HE, Egger MJ, Ward JR, Williams HJ: Analysis of improvement in individual rheumatoid arthritis patients treated with disease-modifying antirheumatic drugs, based on the findings in patients treated with placebo. The Cooperative Systematic Studies of Rheumatic Diseases Group. Arthritis Rheum. 1990, 33: 477-484. 10.1002/art.1780330403.
McComas AJ, Miller RG, Gandevia SC: Fatigue brought on by malfunction of the central and peripheral nervous systems. Adv Exp Med Biol. 1995, 384: 495-512. 10.1007/978-1-4899-1016-5_38.
Alemo Munters L, van Vollenhoven RF, Alexanderson H: Patient preference assessment reveals disease aspects not covered by recommended outcomes in polymyositis and dermatomyositis. ISRN Rheumatol. 2011, 2011: 463124-
Alexanderson H, Reed AM, Ytterberg SR: The myositis activities profile-initial validation for assessment of polymyositis/dermatomyositis in the USA. J Rheumatol. 2012, 39: 2134-2141. 10.3899/jrheum.120504.
Harty LC, Biniecka M, O'Sullivan J, Fox E, Mulhall K, Veale DJ, Fearon U: Mitochondrial mutagenesis correlates with the local inflammatory environment in arthritis. Ann Rheum Dis. 2012, 71: 582-588. 10.1136/annrheumdis-2011-200245.
Mitsui T, Azuma H, Nagasawa M, Iuchi T, Akaike M, Odomi M, Matsumoto T: Chronic corticosteroid administration causes mitochondrial dysfunction in skeletal muscle. J Neurol. 2002, 249: 1004-1009. 10.1007/s00415-002-0774-5.
Hasselgren PO: Glucocorticoids and muscle catabolism. Curr Opin Clin Nutr Metab Care. 1999, 2: 201-205. 10.1097/00075197-199905000-00002.
Fitts RH, Romatowski JG, Peters JR, Paddon-Jones D, Wolfe RR, Ferrando AA: The deleterious effects of bed rest on human skeletal muscle fibers are exacerbated by hypercortisolemia and ameliorated by dietary supplementation. Am J Physiol Cell Physiol. 2007, 293: C313-320. 10.1152/ajpcell.00573.2006.
Wiesinger GF, Quittan M, Graninger M, Seeber A, Ebenbichler G, Sturm B, Kerschan K, Smolen J, Graninger W: Benefit of 6 months long-term physical training in polymyositis/dermatomyositis patients. Br J Rheumatol. 1998, 37: 1338-1342. 10.1093/rheumatology/37.12.1338.
Dalise S, Bertolucci F, Simonella C, Rossi B, Chisari C: Intensive aerobic training improves motor performances and oxidative metabolism efficiency in chronic polymyositis: a case report. Neuromuscul Disord. 2012, 22: S221-S225.
Alexanderson H, Dastmalchi M, Esbjornsson-Liljedahl M, Opava CH, Lundberg IE: Benefits of intensive resistance training in patients with chronic polymyositis or dermatomyositis. Arthritis Rheum. 2007, 57: 768-777. 10.1002/art.22780.
Acknowledgements
We want to thank Christina Ottosson for participation in the study coordination and the collection of clinical and experimental data; Vivianne Andgren and Christina Emilson for performing the intervention; and Eva Lindroos for participating in collection of experimental data. This study was supported by grants from the Myositis Association, the Swedish Research Council, the Swedish Rheumatism Association, King Gustaf V 80 Year Foundation, Funds at the Karolinska Institutet, Promobilia, the Association Francaise contres les Myopathies and through "The regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet".
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
LAM coordinated the study, participated in the study design, performed intervention and microdialysis experiments, analyzed clinical and experimental data, and drafted the manuscript. MD participated in the study design and recruitment, and collected experimental and clinical data. AB performed and analyzed the mitochondrial enzyme activity experiments and assisted in the analyses of physiological results. ME and IL participated in the study design. BH and ML participated in recruitment and collected clinical data. HW analyzed experimental data and assisted in drafting the manuscript. IEL developed and planned the study design, collected experimental and clinical data, and participated in recruitment. HA developed and planned the study design and participated in analysis of clinical data. All authors participated in discussions and the finalizing of the manuscript and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Alemo Munters, L., Dastmalchi, M., Katz, A. et al. Improved exercise performance and increased aerobic capacity after endurance training of patients with stable polymyositis and dermatomyositis. Arthritis Res Ther 15, R83 (2013). https://doi.org/10.1186/ar4263
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/ar4263