
Abstract
Peptidylarginine deiminases (PADs) convert arginine within a peptide (peptidylarginine) into peptidylcitrulline. Citrullination by human PADs is important in normal physiology and inflammation. Porphyromonas gingivalis, a major pathogen in periodontitis, is the only prokaryote described to possess PAD. P. gingivalis infection may generate citrullinated peptides, which trigger anti-citrullinated peptide antibodies. In susceptible individuals, host protein citrullination by human PADs in the joint probably perpetuates antibody formation, paving the way for the development of chronic arthritis. Blockades of bacterial and human PADs may act as powerful novel therapies by inhibiting the generation of the antigens that trigger and sustain autoimmunity in rheumatoid arthritis.
Similar content being viewed by others


Introduction
Arginine is a positively charged, hydrophilic amino acid that is often found on the surface of proteins, where it participates in ionic interactions with other amino acid side chains and forms stabilizing hydrogen bonds with both the peptide backbone and amino acid side chains. These characteristics make it a key amino acid in the three-dimensional organization of proteins and in the interaction with other biological molecules. Hence, post-translational modification of arginine can alter the three-dimensional protein structure and function and potentially expose previously hidden epitopes to the immune system. Deimination (citrullination) of arginine side chains (peptidylarginine) to form peptidylcitrulline is one of many recognized post-translational modifications of this amino acid. This post-translational conversion is catalyzed by the family of peptidylarginine deiminase (PAD) enzymes. The process of protein citrullination plays a vital role in normal physiology, in which it is involved in the formation of rigid structures such as hair, skin, and myelin sheaths [1]. Aberrant citrullination has been observed in diseases of the skin and nervous system and in inflammatory arthritides, of which rheumatoid arthritis (RA) is one example [1]. Despite the ubiquity of citrullinated proteins, the autoantibody response to citrullinated proteins is largely restricted to RA [2]. The switch that leads to the generation of antibodies to citrullinated peptides and thus loss of immune tolerance to citrullinated proteins is likely to involve a complex interplay of individual genetic and environmental factors.
Citrullination by human and bacterial peptidylarginine deiminases
In humans, a family of five PAD enzymes (PAD1 to 4 and PAD6), encoded by five genes clustered on chromosome 1p35-36, has been described [3]. Apart from PAD4, which can translocate to the nucleus, PAD enzymes are typically found in the cytoplasm of various cell types and show a characteristic tissue distribution. The localization and functions of each of the human PAD enzymes are summarized in Table 1. Homologous amino acid sequences for some or all of these PADs exist in other eukaryotic species, such as the mouse, chicken, frog, and bony fish. Among prokaryotic species, PAD activity has, to date, been described in Porphyromonas gingivalis only [4]. P. gingivalis is a major pathogen in periodontitis, a disease that (akin to RA) is a chronic inflammatory disorder characterized by pro-inflammatory cytokine production and erosion of bone.
As protein citrullination in the joint is not specific to RA [5] and auto antibodies to citrullinated proteins precede the clinical signs of RA [6], it has been proposed that oral citrullination of human and bacterial proteins by P. gingivalis PAD (PPAD) in an infectious context prior to the onset of RA could break tolerance and trigger a latent antibody response against citrullinated protein [7]. Once tolerance is breached, citrullination of host proteins by human PADs perpetuates the immune response through epitope spreading and cross-reactivity, resulting in chronic inflammatory disease (Figure 1). Citrullination by both human and bacterial PAD enzymes may thus provide a target for inhibiting the immune response at an early stage in the inflammatory pathway of RA.

Simplified model illustrating the hypothesis that Porphyromonas gingivalis -mediated citrullination triggers anti-citrulline autoimmunity in rheumatoid arthritis. Citrullination by P. gingivalis peptidylarginine deiminase (PAD) in the inflammatory context of periodontitis produces bacterial and host-derived citrullinated peptides to which the immune system mounts a humoral immune response with the production of peptidylcitrulline antibodies. Inflammation-induced citrullination by human PAD enzymes in the gingiva is also possible (dashed arrow). Tissue injury and inflammation in the joint lead to activation of human PAD enzymes and citrullination of host proteins, such as a-enolase, vimentin, fibrin(ogen), and collagen type II. Peptidylcitrulline antibodies bind citrullinated host and bacterial peptides, which may show molecular mimicry, and in genetically susceptible individuals (presence of the certain HLA alleles), intra- and intermolecular epitope spreading leads to a sustained immune response with the formation of high-affinity antibodies to host citrullinated proteins.
The best-established autoantigens in RA include α-enolase, fibrinogen, vimentin, and type II collagen (reviewed in [1]) and all are efficiently deiminated by mammalian PADs. In theory, citrullinated peptides from these antigens could also be generated by PPAD, although this has yet to be demonstrated experimentally. Alpha-enolase is of particular interest in this respect because it is highly conserved among eukaryotes and prokaryotes. A sequence of nine amino acids (Asp-Ser-Arg-Gly-Asn-Pro-Thr-Val-Glu) spanning the immunodominant epitope on the peptide known as citrullinated enolase peptide-1 (CEP-1) is 100% identical to the corresponding region in P. gingivalis enolase, and affinity-purified antibodies to CEP-1 react with recombinant enolase citrullinated in vitro from both humans and P. gingivalis [8], providing an attractive target for molecular mimicry between human and bacterial species.
Etiological association between periodontitis and rheumatoid arthritis
The rationale for considering both human and P. gingivalis PADs in the etiology and pathology of RA is also based on epidemiological data suggesting an association between the two diseases (reviewed in [9]). Periodontitis and RA are chronic inflammatory disorders characterized by erosion of bone and production of pro-inflammatory cytokines. The reported prevalence of periodontitis is highly variable; in one large study of the American population, the prevalence was 4.2% [10]. Epidemiological studies have shown that RA is more prevalent among patients with periodontal disease (3.95%) than in the general population (1%) [11]. In addition, patients with RA have a higher frequency of advanced periodontal disease than the general population [12]. P. gingivalis, Treponema denticola, and Tannerella forsythia are some of the major Gram-negative bacteria that exist as part of a complex bacterial biofilm in the gingival crevice and are linked to the development and progression of periodontitis but can also be found in lower numbers in periodontally healthy subjects [13]. Long-term plaque accumulation and an interplay of host and bacterial factors result in chronic inflammation and tissue damage. Destruction of the adjacent bone and periodontal ligament attachment may eventually lead to tooth loss [14]. P. gingivalis antibody levels have been shown to correlate with anti-CCP (anti-cyclic citrullinated peptide) antibody titres [15], making this periodontopathic oral bacterium an attractive candidate environmental trigger in the development of RA.
Several research groups have reported an increased variety and number of oral bacterial DNA and antibodies targeting these bacteria in serum and synovial fluid of patients with RA and other inflammatory joint diseases compared with controls (non-inflammatory arthritides or healthy donors) [15–19]. Oral bacterial DNA could reach the joint as free DNA or intracellularly in immune cells. Owing to the stringent growth requirements of live oral bacteria, their presence in the joint is unlikely, and no viable organisms have been obtained from synovial fluid [19]. However, these observations need to be interpreted with caution since many bacterial antibody assays using whole-bacterium lysates are of questionable specificity, and the same applies to polymerase chain reaction-based detection and DNA-DNA hybridization using a complex nucleic acid mixture containing an excess of human DNA. A number of antibiotics used in the treatment of periodontitis, such as tetracyclines and clarithromycin, are efficacious in the treatment of RA [20–24], although to date there has been no direct evidence that this therapeutic effect is due to their anti-bacterial activity. For example minocycline has anti-inflammatory and anti-apoptotic effects that are separate from its anti-bacterial role and that are mediated by inhibition of nitric oxide synthase [25], matrix metalloproteinases [26], and caspases [27]. As will be discussed below, minocycline and other tetracycline derivatives may also be direct inhibitors of human PAD4 [28] and P. gingivalis arginine-gingipains [29], which are potent proteinases and major virulence factors in periodontal disease.
Human peptidylarginine deiminases in disease
In normal physiology, PAD enzymes are involved in regulatory processes such as epidermal differentiation, maturation of hair follicles, insulation of nerve fibers, and epigenetic regulation. Aberrant citrullination contributes to skin diseases such as psoriasis and neurological disorders such as multiple sclerosis, Alzheimer disease, and prion disease [30–32]. Citrullination of histones and other nuclear proteins by PAD4 is involved in transcriptional regulation and response to cellular stresses and contributes to the innate immune response through the formation of neutrophil extracellular traps [33–36]. Recently, citrullination of various chemokines has been shown to have functional roles in receptor binding and signalling, proteolytic cleavage, and extravasation of neutrophils [37, 38]. Furthermore, citrullination appears to play a role in the coagulation system and associated pathways, and this is supported by the findings that in vitro citrullinated fibrinogen shows impaired thrombin-catalyzed fibrin polymerization [39] and in vitro citrullination of antithrombin with PAD4 abolishes its thrombin-inhibitory activity [40]. Both citrullinated fibrin(ogen) and citrullinated antithrombin were detected in patients with inflammatory arthritis [40, 41].
Citrullination is thus a widespread phenomenon in normal physiology and inflammation, although targeting citrullinated proteins for an autoimmune response is relatively restricted to RA as shown by the high specificity of anti-citrullinated peptide antibodies for RA [2]. Therefore, it is important to consider which of the deiminases are used for generating the antigens that drive this autoimmunity. On the transcriptional level, various single-nucleotide polymorphisms in the PADI4 gene have been associated with RA in Asian but not in Caucasian populations (reviewed in [42]). Suzuki and colleagues [43] showed that the presence of the disease-associated PADI4 haplotype led to a more stable mRNA, which they suggested increased PAD4 expression and thus levels of citrullinated proteins. However, as PAD inhibitors would work on the post-transcriptional level, we will focus on the expression of PAD enzymes. PAD2 and PAD4 expression has been demonstrated in rheumatoid synovium [44] and synovial fluid cells [45] and extracellularly in synovial fluid [46]. PAD4 differs from other PAD isotypes in its capacity to undergo nuclear translocation due to the presence of a nuclear localization sequence and this translocation has been shown to be induced by tumor necrosis factor-alpha in murine and human oligodendroglial cell lines [47]. PAD expression in the synovial tissue is not specific to RA. It occurs in a variety of inflammatory synovitides [41] and diseases such as inflammatory bowel disease, polymyositis, and interstitial pneumonia [48]. While PAD2 is expressed in the synovia of both patients with inflammatory arthritis and osteoarthritis (OA), PAD4 is predominantly expressed in the synovia of patients with inflammatory arthritides rather than OA [44]. The converse was observed in the extracellular compartment, where Kinloch and colleagues [46] showed the presence of PAD4 in the synovial fluid of patients with RA, spondyloathropathies, and OA, while PAD2 expression was found in both groups of patients with inflammatory arthritis but was notably absent in those with OA. PAD2 and PAD4 expression in the synovium correlates with inflammatory cell infiltration, synovial lining thickness, and vascularity of the deep synovium [44]. Foulquier and colleagues [44] demonstrated PAD2 and PAD4 in close proximity to citrullinated fibrin deposits, although simultaneous detection of the two enzymes in the same area was rare.
Bacterial peptidylarginine deiminase
P. gingivalis, considered a primary pathogen in chronic periodontitis, is a Gram-negative, non-motile anaerobic bacterium that is the only prokaryote described to date to express a functional endogenous PAD enzyme [4]. To date, investigations of bacterial deiminases have focused mainly on enzymes that use free, non-peptidyl arginine or arginine derivatives such as arginine deiminase (ADI). ADIs are enzymes that catalyze the deimination of free arginine to citrulline, releasing ammonia. They are key enzymes in the widespread anaerobic pathway of arginine degradation and many pathogenic microorganisms use this pathway for energy production. Since ADIs are missing in higher eukaryotes, the enzyme constitutes a potential anti-parasitic and anti-bacterial drug target [49]. The other group of structurally and functionally related enzymes produced by most bacterial species consists of agmatine deiminases (agmatine iminohydrolases, or AIHs). AIHs deiminate agmatine (a decarboxylation product of arginine) to N-carbamoylputrescine and ammonia.
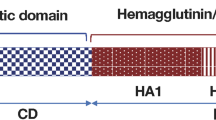
On the amino acid sequence level, PPAD shows no relation to eukaryotic PAD; instead, position-specific iterative-basic local alignment search tool (PSI-BLAST) search connects PPAD to the AIH family (Figure 2). Although the molecular structure of PPAD is unknown, its sequence similarity to AIHs with conservation of key catalytic and guanidino-binding residues indicates that the catalytic domain shares the common α/β-propeller fold of the guanidine-group modifying enzyme (GME) superfamily, which includes human PADs, microbial ADI, aminotransferases, dimethylarginine dimethylamino hydrolases, and AIH [50]. Of note, the database annotation of AIH is confusing since these enzymes are often referred to as 'Porphyromonas-type peptidyl-arginine deiminases' although they most likely do not possess PPAD activity. The three-dimensional structure of PPAD was predicted to consist of the amino-terminal catalytic α/β-propeller domain, followed by an immunoglobulinlike β sandwich. In comparison, the published structure of human PAD4 is composed of two amino-terminal immunoglobulin-like β sandwich domains, followed by the catalytic α/β-propeller domain [51].

Alignment of amino acid sequence of catalytic domains of Porphyromonas gingivalis PAD (PPAD) (residues 86 to 363), AIH from Dyadobacter fermentans DSM 18053 (locus Dfer_2630, residues 60 to 352), and human PAD4 (residues 306 to 556). Residues identical in PPAD and AIH and/or PAD4 are highlighted. Guanidino-binding (#) and catalytic residues (*) that are conserved in all families of guanidino-group modifying enzyme superfamily are indicated. The amino-terminal sequence of each enzyme is unique. In PAD4, the amino-terminal portion is folded into two consecutive immunoglobulin-like β-sandwich domains preceding the catalytic domain harboring the α/β-propeller fold [51]. A long 200-residue carboxy-terminal extension of PPAD is predicted to adopt an immunoglobulin-like β-sandwich structure [50]. AIH, agmatine iminohydrolase; PAD, peptidylarginine deiminase.
Unlike mammalian enzymes, PPAD is able to deiminate both free arginine and peptidylarginine ([4] and our own unpublished observations) and preferentially targets carboxy-terminal arginine, although internal citrullination cannot be excluded. Furthermore, deimination by human PAD is calcium-dependent in contrast to that by PPAD, which does not appear to require any specific cofactors ([4, 52] and our own unpublished observations). P. gingivalis has been shown, however, to increase intracellular calcium concentrations by cleavage of proteinaseactivated receptor 2 (PAR 2), a G protein-coupled receptor found on the neutrophil surface, which may in turn promote human PAD activation [53].
The physiological role of PPAD is unclear. It was suggested that production of ammonia during deimination enhances the survival of P. gingivalis within the periodontal pocket [4]. Indeed, ADI- and AIH-catalyzed ammonium production among bacterial species is known to act as a virulence factor, promoting the survival of microbial pathogens in the host environment. Ammonia neutralizes acidic environments and thereby optimizes gingipain and PPAD function, inactivates hemagglutinins, promotes ATP production, and has negative effects on neutrophil function [4, 54]. Furthermore, it can be speculated that PPAD acts as a virulence factor by generating citrullinated peptides, which may assist the bacterium in spreading and circumventing the humoral immune response. However, the requirements for citrullination by PPAD have not been well investigated to date and it is unknown whether the citrullinated peptides are immunogenic.
Thus, we conclude that PPAD may be more relevant to the initiation of autoimmunity at a site distant from the joint, such as the gingiva, and that PAD2 and PAD4 are important in generating autoantigens that perpetuate autoimmunity in RA once tolerance is breached. Further work is required to identify the regulation and substrate specificity of each enzyme in order to establish a more precise role in the autoimmune response.
Therapeutic peptidylarginine deiminase blockade in rheumatoid arthritis
Although PAD4 has been most extensively studied as a potential therapeutic target in RA (mainly based on the availability of a crystal structure [51]), PAD2 may also be important. It is proposed that selective inhibition of PAD would reduce the levels of citrullinated proteins and consequently suppress the humoral immune response directed to citrullinated antigens in RA. Because PAD4 has an important physiological role in regulating gene expression and PAD4 translocates into the nucleus from the cytosol, potential inhibitors may need to be selective for the extracellular compartment or other PAD isotypes to avoid unwanted effects on gene transcription. It is, however, not known whether intracellular or extracellular PAD is important in the pathophysiology of RA.
Paclitaxel is a chemotherapeutic agent that was initially derived from the bark of the Pacific yew tree. It inhibits angiogenesis by interfering with microtubule function in cell mitosis, migration, chemotaxis, and intracellular transport [55]. In addition, in the millimolar range (half-maximal inhibitory concentration [IC50] = approximately 5 mM), paclitaxel inhibits PAD isolated from bovine brain [56]. It has been shown to prevent the induction of collagen-induced arthritis (CIA) and cause significant regression of existing CIA [57]. An open-label multicenter phase II study of paclitaxel in patients with RA was completed in July 2008, although results of this are still pending [58].
Other PAD inhibitors include F-amidine [N-α-benzoyl- N5-(2-fluoro-1-iminoethyl)-l-ornithine amide], Cl-amidine [N-α-benzoyl-N5-(2-chloro-1-iminoethyl)-l-ornithine amide], and 2-chloroacetamidine, of which Cl-amidine was reported to be the most potent (IC50 = 5.9 μM) [59]. Ex vivo studies with F-amidine and Cl-amidine, using a cell line and an assay measuring PAD4-mediated citrullination of a nuclear protein and the resulting enhancement in binding to another protein, indicated that these inhibitors are bioavailable [59, 60]. F-amidine irreversibly inhibits PAD4 via the specific modification of Cys 645, an active-site residue that is critical for enzyme catalysis. Cys 645 acts as a nucleophile to form a thiouronium intermediate that is hydrolyzed to form citrulline. Cl-amidine and 2-chloroacetamidine are thought to act via a similar mechanism [59, 61]. Inactivation by F-amidine and Cl-amidine is calcium-dependent [60]. In vitro studies with PAD4 have shown that calcium binding leads to a conformational change that moves Cys 645 and His 471 into positions that are competent for catalysis [51] and presumably reactive with F-amidine and Cl-amidine. This is of therapeutic importance as these compounds would therefore be expected to inhibit PAD4 in its activated state only at sites of inflammatory activity such as the synovium and not the inactive enzyme at other sites in the body, limiting toxicity [59]. Willis and colleagues [62] recently showed that Cl-amidine treatment in CIA is able to inhibit clinical disease activity scores by 55%, 53%, and 42% in the 50, 10, and 1 mg/kg per day groups, respectively. Histological severity scores and complement C3 deposition scores paralleled the decreases in disease activity. In addition, mice receiving Cl-amidine showed reduced epitope spreading by peptide microarray, especially to citrullinated joint antigens. Interestingly, there were no changes in the percentages of T-cell, B-cell, or monocyte populations in treated mice compared with controls [62]. These results suggest that Cl-amidine may represent a novel class of RA therapeutics that specifically target citrullination.
Bhattacharya and colleagues [63] demonstrated that human astrocytes subject to pressure showed elevated PAD2 levels, increased intracellular calcium concentrations, and increased citrullination. Treatment with the cell-permeable calcium chelating agent BAPTA-AM (1,2-bis-(o-Aminophenoxy)-ethane-N,N,N',N'-tetraacetic acid tetraacetoxymethyl ester) resulted in decreased intracellular calcium concentration and PAD2 levels. These results suggest that calcium modulation may be an alternative therapeutic strategy in modulating PAD activity and citrullination, although we would argue that this mechanism is too broad to be applicable in practice.
On the basis of the therapeutic use of tetracyclines in RA [23], Knuckley and colleagues [28] screened tetracycline derivatives (minocycline, doxycycline, tetracycline, and chlortetracycline) for their potential to inhibit PAD4 activity. Chlortetracycline was identified as the most potent inhibitor (IC50 = 100 μM) and was suggested to bind to a region distal from the active site [28]. Streptomycin, an aminoglycoside antibiotic, was also tested because of its two guanidinium groups that could act as inhibitors of PAD4. Streptomycin was found to inhibit PAD4, though with a lower potency (IC50 = approximately 1.8 mM), and was suggested to bind within or in close proximity to the active site. The data suggest that these compounds could provide a valuable scaffold for engineering inhibitors with greater potency and selectivity.
Porphyromonas gingivalispeptidylarginine deiminase as a target for treatment in rheumatoid arthritis
The unique nature of PPAD in terms of its different amino acid sequence, cofactor requirement, and domain organization compared with human PADs (Figure 2), along with its location on the bacterial cell surface [4], would make this enzyme a potential target in the treatment of RA provided that its possible involvement in disease etiology or pathology is substantiated in future studies. Development of therapeutics targeting PPAD is further encouraged by advances in design and synthesis of inhibitors against parasite-derived ADI with potentials to be used as anti-parasitic agents [64]. Since ADI, PADs, and PPAD are likely to use the same catalytic machinery to deiminate (peptidyl)arginine (Figure 2), a similar chemistry may be applied to develop PPAD inhibitors. The calcium-independent deimination of carboxy-terminal arginine residues specific to PPAD can be explored to develop highly selective compounds with little or no cross-reactivity with host enzymes.
McGraw and colleagues [4] reported that native PPAD, purified from the bacterial culture supernatant, was missing the N-terminus inferred from the DNA sequence because of proteolysis at the Arg43-Ala44 peptide bond. This might have been an artifact caused by the potent proteases, arginine-gingipains, which co-purified with PAD at the initial stages of protein purification, or might have true biological significance (for example, arising during export of the enzyme from the cell to form the mature protein). A recent paper on PPAD reported that the full-length, uncleaved form was unstable and had only 40% activity when compared with the truncated form of the enzyme [52]. Future studies aimed at identifying the mature, in vivo form of PPAD and its enzymology are required in order to pin down the biologically relevant form of the enzyme and as such the more appropriate target for therapeutic blockade.
As the PPAD enzyme is not well studied, there are no published studies on possible therapeutic inhibitors. To gain insight into the catalytic mode of PPAD, McGraw and colleagues [4] tested various compounds that might interfere with the catalytic cysteine residue (Cys 351) or substrate binding. They reported that the serine- and cysteine-protease inhibitor leupeptin is able to completely inhibit PPAD at millimolar levels (5 mM), with other inhibitors such as thiourea, thio-L-citrulline, and the serine- and cysteine-protease inhibitor TLCK (N-alpha-p-tosyl-L-lysine chloromethyl ketone) being inhibitory at higher concentrations (12.5 to 50 mM) [4]. Apart from the relatively low inhibitory potency, these compounds are either toxic (thiourea) or unselective (thio-L-citrulline is a potent inhibitor of nitric oxide synthase) [65] but nonetheless provide a basis for the development of more potent, specific inhibitors.
Conclusions
We have summarized a possible role for PPAD in breaking tolerance to citrullinated proteins, with human PAD2 or PAD4 or both maintaining the generation of citrullinated antigens in the joint. However, the evidence remains speculative and clearly requires further investigation of the mechanisms of activity of the enzymes involved and how the apparently unique PAD encoded by P. gingivalis could generate immunogenic peptides. If these hypotheses are further substantiated, PAD blockade has the potential to switch off autoimmunity at the point of initiation and inhibit the maintenance of the pathology in RA. Thus, inhibition of bacterial and human PADs could become the first treatment targeting the generation of the actual antigens that drive the disease.
Abbreviations
- ADI:
-
arginine deiminase
- AIH:
-
agmatine iminohydrolase
- CEP-1:
-
citrullinated enolase peptide-1
- CIA:
-
collagen-induced arthritis
- Cl-amidine:
-
N-α-benzoyl- N5-(2-chloro-1-iminoethyl)-L-ornithine amide
- F-amidine:
-
N-α-benzoyl- N5-(2-fluoro-1-iminoethyl)-L-ornithine amide
- IC50:
-
half-maximal inhibitory concentration (concentration of inhibitor that yields 50% inhibition)
- OA:
-
osteoarthritis
- PAD:
-
peptidylarginine deiminase
- PPAD:
-
Porphyromonas gingivalis peptidylarginine deiminase
- RA:
-
rheumatoid arthritis.
References
Wegner N, Lundberg K, Kinloch A, Fisher B, Malmström V, Feldmann M, Venables PJ: Autoimmunity to specific citrullinated proteins gives the first clues to the etiology of rheumatoid arthritis. Immunol Rev. 2010, 233: 34-54. 10.1111/j.0105-2896.2009.00850.x.
Schellekens GA, Visser H, de Jong BA, Hoogen van den FH, Hazes JM, Breedveld FC, van Venrooij WJ: The diagnostic properties of rheumatoid arthritis antibodies recognizing a cyclic citrullinated peptide. Arthritis Rheum. 2000, 43: 155-163. 10.1002/1529-0131(200001)43:1<155::AID-ANR20>3.0.CO;2-3.
Chavanas S, Mechin MC, Takahara H, Kawada A, Nachat R, Serre G, Simon M: Comparative analysis of the mouse and human peptidylarginine deiminase gene clusters reveals highly conserved non-coding segments and a new human gene, PADI6. Gene. 2004, 330: 19-27. 10.1016/j.gene.2003.12.038.
McGraw WT, Potempa J, Farley D, Travis J: Purification, characterization, and sequence analysis of a potential virulence factor from Porphyromonas gingivalis, peptidylarginine deiminase. Infect Immun. 1999, 67: 3248-3256.
Vossenaar ER, Smeets TJ, Kraan MC, Raats JM, van Venrooij WJ, Tak PP: The presence of citrullinated proteins is not specific for rheumatoid synovial tissue. Arthritis Rheum. 2004, 50: 3485-3494. 10.1002/art.20584.
Nielen MM, van Schaardenburg D, Reesink HW, Stadt van de RJ, Horst-Bruinsma van der IE, de Koning MH, Habibuw MR, Vandenbroucke JP, Dijkmans BA: Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum. 2004, 50: 380-386. 10.1002/art.20018.
Rosenstein ED, Greenwald RA, Kushner LJ, Weissmann G: Hypothesis: the humoral immune response to oral bacteria provides a stimulus for the development of rheumatoid arthritis. Inflammation. 2004, 28: 311-318. 10.1007/s10753-004-6641-z.
Lundberg K, Kinloch A, Fisher BA, Wegner N, Wait R, Charles P, Mikuls TR, Venables PJ: Antibodies to citrullinated alpha-enolase peptide 1 are specific for rheumatoid arthritis and cross-react with bacterial enolase. Arthritis Rheum. 2008, 58: 3009-3019. 10.1002/art.23936.
de Pablo P, Chapple IL, Buckley CD, Dietrich T: Periodontitis in systemic rheumatic diseases. Nat Rev Rheumatol. 2009, 5: 218-224. 10.1038/nrrheum.2009.28.
Borrell LN, Burt BA, Taylor GW: Prevalence and trends in periodontitis in the USA: the [corrected] NHANES, 1988 to 2000. J Dent Res. 2005, 84: 924-930. 10.1177/154405910508401010.
de Pablo P, Dietrich T, McAlindon TE: Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J Rheumatol. 2008, 35: 70-76.
Mercado F, Marshall RI, Klestov AC, Bartold PM: Is there a relationship between rheumatoid arthritis and periodontal disease?. J Clin Periodontol. 2000, 27: 267-272. 10.1034/j.1600-051x.2000.027004267.x.
Socransky SS, Haffajee AD: Periodontal microbial ecology. Periodontol 2000. 2005, 38: 135-187. 10.1111/j.1600-0757.2005.00107.x.
Tatakis DN, Kumar PS: Etiology and pathogenesis of periodontal diseases. Dent Clin North Am. 2005, 49: 491-516. 10.1016/j.cden.2005.03.001.
Mikuls TR, Payne JB, Reinhardt RA, Thiele GM, Maziarz E, Cannella AC, Holers VM, Kuhn KA, O'Dell JR: Antibody responses to Porphyromonas gingivalis (P. gingivalis) in subjects with rheumatoid arthritis and periodontitis. Int Immunopharmacol. 2009, 9: 38-42. 10.1016/j.intimp.2008.09.008.
Moen K, Brun JG, Madland TM, Tynning T, Jonsson R: Immunoglobulin G and A antibody responses to Bacteroides forsythus and Prevotella intermedia in sera and synovial fluids of arthritis patients. Clin Diagn Lab Immunol. 2003, 10: 1043-1050.
Moen K, Brun JG, Valen M, Skartveit L, Eribe EK, Olsen I, Jonsson R: Synovial inflammation in active rheumatoid arthritis and psoriatic arthritis facilitates trapping of a variety of oral bacterial DNAs. Clin Exp Rheumatol. 2006, 24: 656-663.
Ogrendik M, Kokino S, Ozdemir F, Bird PS, Hamlet S: Serum antibodies to oral anaerobic bacteria in patients with rheumatoid arthritis. MedGenMed. 2005, 7: 2-
Martinez-Martinez RE, Abud-Mendoza C, Patino-Marin N, Rizo-Rodriguez JC, Little JW, Loyola-Rodriguez JP: Detection of periodontal bacterial DNA in serum and synovial fluid in refractory rheumatoid arthritis patients. J Clin Periodontol. 2009, 36: 1004-1010. 10.1111/j.1600-051X.2009.01496.x.
Ogrendik M: Treatment of rheumatoid arthritis with ornidazole: a randomized, double-blind, placebo-controlled study. Rheumatol Int. 2006, 26: 1132-1137. 10.1007/s00296-006-0145-0.
Ogrendik M: Levofloxacin treatment in patients with rheumatoid arthritis receiving methotrexate. South Med J. 2007, 100: 135-139.
Ogrendik M: Effects of clarithromycin in patients with active rheumatoid arthritis. Curr Med Res Opin. 2007, 23: 515-522. 10.1185/030079906X167642.
O'Dell JR, Haire CE, Palmer W, Drymalski W, Wees S, Blakely K, Churchill M, Eckhoff PJ, Weaver A, Doud D, Erikson N, Dietz F, Olson R, Maloley P, Klassen LW, Moore GF: Treatment of early rheumatoid arthritis with minocycline or placebo: results of a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 1997, 40: 842-848. 10.1002/art.1780400510.
Kloppenburg M, Breedveld FC, Terwiel JP, Mallee C, Dijkmans BA: Minocycline in active rheumatoid arthritis. A double-blind, placebo-controlled trial. Arthritis Rheum. 1994, 37: 629-636. 10.1002/art.1780370505.
Amin AR, Attur MG, Thakker GD, Patel PD, Vyas PR, Patel RN, Patel IR, Abramson SB: A novel mechanism of action of tetracyclines: effects on nitric oxide synthases. Proc Natl Acad Sci USA. 1996, 93: 14014-14019. 10.1073/pnas.93.24.14014.
Greenwald RA, Golub LM, Lavietes B, Ramamurthy NS, Gruber B, Laskin RS, McNamara TF: Tetracyclines inhibit human synovial collagenase in vivo and in vitro. J Rheumatol. 1987, 14: 28-32.
Chen M, Ona VO, Li M, Ferrante RJ, Fink KB, Zhu S, Bian J, Guo L, Farrell LA, Hersch SM, Hobbs W, Vonsattel JP, Cha JH, Friedlander RM: Minocycline inhibits caspase-1 and caspase-3 expression and delays mortality in a transgenic mouse model of Huntington disease. Nat Med. 2000, 6: 797-801. 10.1038/80538.
Knuckley B, Luo Y, Thompson PR: Profiling Protein Arginine Deiminase 4 (PAD4): a novel screen to identify PAD4 inhibitors. Bioorg Med Chem. 2008, 16: 739-745. 10.1016/j.bmc.2007.10.021.
Imamura T, Matsushita K, Travis J, Potempa J: Inhibition of trypsin-like cysteine proteinases (gingipains) from Porphyromonas gingivalis by tetracycline and its analogues. Antimicrob Agents Chemother. 2001, 45: 2871-2876. 10.1128/AAC.45.10.2871-2876.2001.
Jang B, Kim E, Choi JK, Jin JK, Kim JI, Ishigami A, Maruyama N, Carp RI, Kim YS, Choi EK: Accumulation of citrullinated proteins by up-regulated peptidylarginine deiminase 2 in brains of scrapie-infected mice: a possible role in pathogenesis. Am J Pathol. 2008, 173: 1129-1142. 10.2353/ajpath.2008.080388.
Gyorgy B, Toth E, Tarcsa E, Falus A, Buzas EI: Citrullination: a posttranslational modification in health and disease. Int J Biochem Cell Biol. 2006, 38: 1662-1677. 10.1016/j.biocel.2006.03.008.
Young DS, Meersman F, Oxley D, Webster J, Gill AC, Bronstein I, Lowe CR, Dear DV: Effect of enzymatic deimination on the conformation of recombinant prion protein. Biochim Biophys Acta. 2009, 1794: 1123-1133.
Neeli I, Dwivedi N, Khan S, Radic M: Regulation of extracellular chromatin release from neutrophils. J Innate Immun. 2009, 1: 194-201. 10.1159/000206974.
Wang Y, Li M, Stadler S, Correll S, Li P, Wang D, Hayama R, Leonelli L, Han H, Grigoryev SA, Allis CD, Coonrod SA: Histone hypercitrullination mediates chromatin decondensation and neutrophil extracellular trap formation. J Cell Biol. 2009, 184: 205-213. 10.1083/jcb.200806072.
Tanikawa C, Ueda K, Nakagawa H, Yoshida N, Nakamura Y, Matsuda K: Regulation of protein Citrullination through p53/PADI4 network in DNA damage response. Cancer Res. 2009, 69: 8761-8769. 10.1158/0008-5472.CAN-09-2280.
Neeli I, Khan SN, Radic M: Histone deimination as a response to inflammatory stimuli in neutrophils. J Immunol. 2008, 180: 1895-1902.
Proost P, Loos T, Mortier A, Schutyser E, Gouwy M, Noppen S, Dillen C, Ronsse I, Conings R, Struyf S, Opdenakker G, Maudgal PC, Van Damme J: Citrullination of CXCL8 by peptidylarginine deiminase alters receptor usage, prevents proteolysis, and dampens tissue inflammation. J Exp Med. 2008, 205: 2085-2097. 10.1084/jem.20080305.
Loos T, Mortier A, Gouwy M, Ronsse I, Put W, Lenaerts JP, Van Damme J, Proost P: Citrullination of CXCL10 and CXCL11 by peptidylarginine deiminase: a naturally occurring posttranslational modification of chemokines and new dimension of immunoregulation. Blood. 2008, 112: 2648-2656. 10.1182/blood-2008-04-149039.
Okumura N, Haneishi A, Terasawa F: Citrullinated fibrinogen shows defects in FPA and FPB release and fibrin polymerization catalyzed by thrombin. Clin Chim Acta. 2009, 401: 119-123. 10.1016/j.cca.2008.12.002.
Chang X, Yamada R, Sawada T, Suzuki A, Kochi Y, Yamamoto K: The inhibition of antithrombin by peptidylarginine deiminase 4 may contribute to pathogenesis of rheumatoid arthritis. Rheumatology (Oxford). 2005, 44: 293-298. 10.1093/rheumatology/keh473.
Chapuy-Regaud S, Sebbag M, Baeten D, Clavel C, Foulquier C, De Keyser F, Serre G: Fibrin deimination in synovial tissue is not specific for rheumatoid arthritis but commonly occurs during synovitides. J Immunol. 2005, 174: 5057-5064.
Suzuki A, Yamada R, Yamamoto K: Citrullination by peptidylarginine deiminase in rheumatoid arthritis. Ann N Y Acad Sci. 2007, 1108: 323-339. 10.1196/annals.1422.034.
Suzuki A, Yamada R, Chang X, Tokuhiro S, Sawada T, Suzuki M, Nagasaki M, Nakayama-Hamada M, Kawaida R, Ono M, Ohtsuki M, Furukawa H, Yoshino S, Yukioka M, Tohma S, Matsubara T, Wakitani S, Teshima R, Nishioka Y, Sekine A, Iida A, Takahashi A, Tsunoda T, Nakamura Y, Yamamoto K: Functional haplotypes of PADI4, encoding citrullinating enzyme peptidylarginine deiminase 4, are associated with rheumatoid arthritis. Nat Genet. 2003, 34: 395-402. 10.1038/ng1206.
Foulquier C, Sebbag M, Clavel C, Chapuy-Regaud S, Al Badine R, Méchin MC, Vincent C, Nachat R, Yamada M, Takahara H, Simon M, Guerrin M, Serre G: Peptidyl arginine deiminase type 2 (PAD-2) and PAD-4 but not PAD-1, PAD-3, and PAD-6 are expressed in rheumatoid arthritis synovium in close association with tissue inflammation. Arthritis Rheum. 2007, 56: 3541-3553. 10.1002/art.22983.
Vossenaar ER, Radstake TR, Heijden van der A, van Mansum MA, Dieteren C, de Rooij DJ, Barrera P, Zendman AJ, van Venrooij WJ: Expression and activity of citrullinating peptidylarginine deiminase enzymes in monocytes and macrophages. Ann Rheum Dis. 2004, 63: 373-381. 10.1136/ard.2003.012211.
Kinloch A, Lundberg K, Wait R, Wegner N, Lim NH, Zendman AJ, Saxne T, Malmstrom V, Venables PJ: Synovial fluid is a site of citrullination of autoantigens in inflammatory arthritis. Arthritis Rheum. 2008, 58: 2287-2295. 10.1002/art.23618.
Mastronardi FG, Wood DD, Mei J, Raijmakers R, Tseveleki V, Dosch HM, Probert L, Casaccia-Bonnefil P, Moscarello MA: Increased citrullination of histone H3 in multiple sclerosis brain and animal models of demyelination: a role for tumor necrosis factor-induced peptidylarginine deiminase 4 translocation. J Neurosci. 2006, 26: 11387-11396. 10.1523/JNEUROSCI.3349-06.2006.
Makrygiannakis D, af Klint E, Lundberg IE, Lofberg R, Ulfgren AK, Klareskog L, Catrina AI: Citrullination is an inflammation-dependent process. Ann Rheum Dis. 2006, 65: 1219-1222. 10.1136/ard.2005.049403.
Galkin A, Kulakova L, Sarikaya E, Lim K, Howard A, Herzberg O: Structural insight into arginine degradation by arginine deiminase, an antibacterial and parasite drug target. J Biol Chem. 2004, 279: 14001-14008. 10.1074/jbc.M313410200.
Shirai H, Mokrab Y, Mizuguchi K: The guanidino-group modifying enzymes: structural basis for their diversity and commonality. Proteins. 2006, 64: 1010-1023. 10.1002/prot.20863.
Arita K, Hashimoto H, Shimizu T, Nakashima K, Yamada M, Sato M: Structural basis for Ca(2+)-induced activation of human PAD4. Nat Struct Mol Biol. 2004, 11: 777-783. 10.1038/nsmb799.
Rodriguez SB, Stitt BL, Ash DE: Expression of peptidylarginine deiminase from Porphyromonas gingivalis in Escherichia coli: enzyme purification and characterization. Arch Biochem Biophys. 2009, 488: 14-22. 10.1016/j.abb.2009.06.010.
Lourbakos A, Chinni C, Thompson P, Potempa J, Travis J, Mackie EJ, Pike RN: Cleavage and activation of proteinase-activated receptor-2 on human neutrophils by gingipain-R from Porphyromonas gingivalis. FEBS Lett. 1998, 435: 45-48. 10.1016/S0014-5793(98)01036-9.
Niederman R, Brunkhorst B, Smith S, Weinreb RN, Ryder MI: Ammonia as a potential mediator of adult human periodontal infection: inhibition of neutrophil function. Arch Oral Biol. 1990, 35 (Suppl): 205S-209S. 10.1016/0003-9969(90)90159-8.
Belotti D, Rieppi M, Nicoletti MI, Casazza AM, Fojo T, Taraboletti G, Giavazzi R: Paclitaxel (Taxol(R)) inhibits motility of paclitaxel-resistant human ovarian carcinoma cells. Clin Cancer Res. 1996, 2: 1725-1730.
Pritzker LB, Moscarello MA: A novel microtubule independent effect of paclitaxel: the inhibition of peptidylarginine deiminase from bovine brain. Biochim Biophys Acta. 1998, 1388: 154-160.
Brahn E, Tang C, Banquerigo ML: Regression of collagen-induced arthritis with taxol, a microtubule stabilizer. Arthritis Rheum. 1994, 37: 839-845. 10.1002/art.1780370611.
ClinicalTrials.gov: search of: paclitaxel AND rheumatoid: a study using intravenous paxceed to treat patients with rheumatoid arthritis. [http://clinicaltrials.gov/ct2/results?term=paclitaxel+AND+rheumatoid]
Luo Y, Arita K, Bhatia M, Knuckley B, Lee YH, Stallcup MR, Sato M, Thompson PR: Inhibitors and inactivators of protein arginine deiminase 4: functional and structural characterization. Biochemistry. 2006, 45: 11727-11736. 10.1021/bi061180d.
Luo Y, Knuckley B, Lee YH, Stallcup MR, Thompson PR: A fluoroacetamidinebased inactivator of protein arginine deiminase 4: design, synthesis, and in vitro and in vivo evaluation. J Am Chem Soc. 2006, 128: 1092-1093. 10.1021/ja0576233.
Stone EM, Schaller TH, Bianchi H, Person MD, Fast W: Inactivation of two diverse enzymes in the amidinotransferase superfamily by 2-chloroacetamidine: dimethylargininase and peptidylarginine deiminase. Biochemistry. 2005, 44: 13744-13752. 10.1021/bi051341y.
Willis V, Gizinski A, Knuckley B, Banda N, Cordova K, Luo Y, Causey C: Treatment with Cl-amidine, a peptidyl arginine deiminase (PAD) inhibitor significantly reduces collagen-induced arthritis (CIA) [abstract]. Arthritis Rheum. 2009, 60 (suppl 10): 665-
Bhattacharya SK, Bhat MB, Takahara H: Modulation of peptidyl arginine deiminase 2 and implication for neurodegeneration. Curr Eye Res. 2006, 31: 1063-1071. 10.1080/02713680600991437.
Li L, Li Z, Chen D, Lu X, Feng X, Wright EC, Solberg NO, Dunaway-Mariano D, Mariano PS, Galkin A, Kulakova L, Herzberg O, Green-Church KB, Zhang L: Inactivation of microbial arginine deiminases by L-canavanine. J Am Chem Soc. 2008, 130: 1918-10.1021/ja0760877.
Frey C, Narayanan K, McMillan K, Spack L, Gross SS, Masters BS, Griffith OW: L-thiocitrulline. A stereospecific, heme-binding inhibitor of nitric-oxide synthases. J Biol Chem. 1994, 269: 26083-26091.
Nachat R, Mechin MC, Takahara H, Chavanas S, Charveron M, Serre G, Simon M: Peptidylarginine deiminase isoforms 1-3 are expressed in the epidermis and involved in the deimination of K1 and filaggrin. J Invest Dermatol. 2005, 124: 384-393. 10.1111/j.0022-202X.2004.23568.x.
Nachat R, Mechin MC, Charveron M, Serre G, Constans J, Simon M: Peptidylarginine deiminase isoforms are differentially expressed in the anagen hair follicles and other human skin appendages. J Invest Dermatol. 2005, 125: 34-41. 10.1111/j.0022-202X.2005.23763.x.
Mechin MC, Enji M, Nachat R, Chavanas S, Charveron M, Ishida-Yamamoto A, Serre G, Takahara H, Simon M: The peptidylarginine deiminases expressed in human epidermis differ in their substrate specificities and subcellular locations. Cell Mol Life Sci. 2005, 62: 1984-1995. 10.1007/s00018-005-5196-y.
Sambandam T, Belousova M, Accaviti-Loper MA, Blanquicett C, Guercello V, Raijmakers R, Nicholas AP: Increased peptidylarginine deiminase type II in hypoxic astrocytes. Biochem Biophys Res Commun. 2004, 325: 1324-1329. 10.1016/j.bbrc.2004.10.173.
Ishigami A, Ohsawa T, Hiratsuka M, Taguchi H, Kobayashi S, Saito Y, Murayama S, Asaga H, Toda T, Kimura N, Maruyama N: Abnormal accumulation of citrullinated proteins catalyzed by peptidylarginine deiminase in hippocampal extracts from patients with Alzheimer's disease. J Neurosci Res. 2005, 80: 120-128. 10.1002/jnr.20431.
Urano Y, Watanabe K, Sakaki A, Arase S, Watanabe Y, Shigemi F, Takeda K, Akiyama K, Senshu T: Immunohistochemical demonstration of peptidylarginine deiminase in human sweat glands. Am J Dermatopathol. 1990, 12: 249-255. 10.1097/00000372-199006000-00005.
Ishigami A, Ohsawa T, Asaga H, Akiyama K, Kuramoto M, Maruyama N: Human peptidylarginine deiminase type II: molecular cloning, gene organization, and expression in human skin. Arch Biochem Biophys. 2002, 407: 25-31. 10.1016/S0003-9861(02)00516-7.
Vossenaar ER, Zendman AJ, van Venrooij WJ, Pruijn GJ: PAD, a growing family of citrullinating enzymes: genes, features and involvement in disease. Bioessays. 2003, 25: 1106-1118. 10.1002/bies.10357.
Hagiwara T, Nakashima K, Hirano H, Senshu T, Yamada M: Deimination of arginine residues in nucleophosmin/B23 and histones in HL-60 granulocytes. Biochem Biophys Res Commun. 2002, 290: 979-983. 10.1006/bbrc.2001.6303.
Acknowledgements
This work was supported by the Arthritis Research Campaign (NW and PJV) and in part by grants DE 09761 and 1642/B/P01/2008/35 from the National Institutes of Health (Bethesda, MD, USA) and the Department of Scientific Research of the Polish Ministry of Science and Education, respectively (JP). The Faculty of Biochemistry, Biophysics, and Biotechnology of the Jagiellonian University Krakow is a recipient of structural funds from the European Union (grant number POIG.02.01.00-12-064/08 - 'Molecular biotechnology for health').
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Mangat, P., Wegner, N., Venables, P.J. et al. Bacterial and human peptidylarginine deiminases: targets for inhibiting the autoimmune response in rheumatoid arthritis?. Arthritis Res Ther 12, 209 (2010). https://doi.org/10.1186/ar3000
Published:
DOI: https://doi.org/10.1186/ar3000