
Abstract
Microvascular injury, oxidative stress, and impaired angiogenesis are prominent features of systemic sclerosis (SSc). We compared serum markers of these phenomena at baseline and after treatment with nifedipine in SSc patients. Forty successive SSc patients were compared with 20 matched healthy subjects. All SSc patients stopped taking calcium-channel blockers 72 hours before measurements. Twenty SSc patients were also examined after 14 days of treatment with nifedipine (60 mg/day). Quantitative ELISA was used to measure the serum concentrations of vascular endothelial growth factor (VEGF), soluble VEGF receptor 1 (sVEGFR-1), soluble vascular cell adhesion molecule 1 (sVCAM-1), carbonyl residues, and advanced oxidation protein products (AOPP). The median concentrations of VEGF, sVEGFR-1, sVCAM-1, carbonyl residues, and AOPP were significantly higher in SSc patients than in healthy subjects at baseline. A correlation was found between VEGF concentration and carbonyl residue concentration (r = 0.43; P = 0.007). Nifedipine treatment led to a significant decrease in concentrations of sVCAM-1, carbonyl residues, and AOPP but did not affect concentrations of VEGF and sVEGFR-1. Nifedipine treatment ameliorated endothelium injury in patients with SSc, as shown by the concentrations of adhesion molecules and oxidative damage markers. The fact that VEGF and sVEGFR-1 concentrations were not changed whereas oxidative stress was ameliorated by nifedipine is consistent with the hypothesis that VEGF signalling is impaired in SSc. However, more experimental evidence is needed to determine whether the VEGF pathway is intrinsically defective in SSc.
Similar content being viewed by others
Introduction
Systemic sclerosis (SSc) is a connective tissue disease characterised by early generalised microangiopathy and culminating in systemic fibrosis. The pivotal steps of the disease are endothelium injury, immune activation, and collagen deposition by activated fibroblasts.
Vascular changes are suspected to occur at an early stage [1]. Changes include gaps between endothelial cells [2], apoptosis [3], endothelium activation with the expression of cell adhesion molecules, inflammatory cell recruitment, procoagulant state [4], and intimal proliferation and adventitial fibrosis, which may lead to vessel obliteration. The vasculature plays a major role in SSc pathogenesis, and prognosis and outcome are dependent on the extent and severity of the vascular lesions [5].
Endothelial injury is reflected by altered endothelium-related indices, including increased plasma levels of markers such as soluble vascular cell adhesion molecule 1 (sVCAM-1). Thus, sVCAM-1 could be a useful parameter for vascular assessment [6] and has been reported to be associated with changes in disease severity [7]. Angiogenesis has been reported to be disturbed in SSc patients despite high serum concentrations of vascular endothelial growth factor (VEGF) [8–10], suggesting that VEGF is counterbalanced by angiostatic factors [11] or is the consequence of signalling defects [9]. VEGF is a glycoprotein with potent angiogenic, mitogenic, and vascular permeability-enhancing activities specific for endothelial cells. It interacts with two receptor tyrosine kinases, VEGFR-1 (flt) and VEGFR-2 (flk). A defect in VEGF receptors could account for VEGF signalling abnormalities in SSc. The human VEGFR-1 gene produces two major transcripts, corresponding to the full-length receptor and a soluble receptor (sVEGFR-1) with biological activities [12]. Oxidative stress may modulate angiogenesis through microvascular toxicity but may also promote angiogenesis [13]. The free radicals generated by reperfusion injury (Raynaud's phenomenon) and the inflammatory process appear to play a key role in SSc [14].
Calcium-channel blockers, particularly those of the dihydropyridine type such as nifedipine, are of major importance for the treatment of Raynaud's phenomenon in SSc patients [15] and may have beneficial effects on cardiac involvement [16]. We recently reported that these drugs have acute and sustained beneficial effects on oxidative markers of damage in SSc patients [17].
The aim of our study was, first, to investigate serum endothelial cell markers of adhesion (sVCAM-1) and angiogenesis (VEGF, sVEGFR-1) together with oxidative damage markers (carbonyl residues and advanced oxidation protein products [AOPP]) at baseline and, secondly, to look for the influence of nifedipine treatment on all these parameters in SSc patients.
Materials and methods
Study population
We prospectively included successive SSc patients hospitalised for systematic follow-up of the disease. SSc was classified as 'limited' or 'diffuse' cutaneous according to the criteria of LeRoy and colleagues [18]. The exclusion criteria were the impossibility of stopping vasodilator therapy, pregnancy, current cigarette smoking, diabetes, association with severe diseases (cardiac or hepatic failure, cancer, gangrene), and immunosuppressive therapy. A three-month period of stable current treatment was required for inclusion.
The onset of the disease was defined as the time at which skin involvement occurred. The laboratory tests included the Westergren erythrocyte sedimentation rate, C-reactive protein levels, serum creatinine concentration, and antinuclear, anticentromere (indirect immunofluorescence on HEp2 cells), and antitopoisomerase I (counterimmunoelectrophoresis) antibody levels. Pulmonary involvement was assessed by computed tomography, forced vital capacity, and the ratio of carbon monoxide diffusion capacity to hemoglobin. Systolic pulmonary artery pressure was determined by Doppler echocardiography, and left ventricular ejection fraction, by radionuclide ventriculography. The control subjects were healthy nonsmokers from the laboratory staff.
Study design
Patients were asked to stop taking calcium-channel blockers 3 days before hospitalisation. The baseline evaluation was performed on the morning of admission after 1 hour of rest at room temperature. The duration of the wash-out period is long enough for calcium-channel blockers to have ceased to have an effect, because the half-life is between 6 and 11 hours. Twenty of the SSc patients evaluated at baseline were evaluated again after 14 days of treatment with nifedipine (60 mg/day) both for a cardiac study and for the present biological evaluation. The second evaluation was carried out in the morning, 1 hour after the last intake of nifedipine.
The study was approved by the local Ethics Committee (Cochin Hospital, Paris, France) and all patients gave their written informed consent. Blood samples (10 ml) were collected in pyrogen-free tubes. They were centrifuged at 3,000 gfor 10 minutes within an hour of collection and immediately stored in aliquots at -80°C until use; the storage duration was less than 6 months.
Serum vascular markers
Levels of VEGF, sVEGFR-1, and sVCAM-1 were determined by quantitative colorimetric sandwich ELISA (R&D Systems, Abingdon, UK) in accordance with the manufacturer's instructions. Concentrations were calculated using a standard curve generated with specific standards provided by the manufacturer.
The ELISA for VEGF recognises human VEGF165 as well as VEGF121 (two diffusible proteins from mature, monomeric VEGF), but not human placenta-derived growth factor, platelet-derived growth factor, or transforming growth factor. Inter- and intra-assay variances for VEGF, sVEGFR-1, and sVCAM-1 were lower than 10%. The minimum detectable concentration was less than 9 pg/ml for VEGF, less than 5 pg/ml for sVEGFR-1, and less than 2 ng/ml for sVCAM-1.
Serum markers of oxidative damage
Carbonyl residues were determined as previously described, using dinitrophenylhydrazine [19]. Briefly, samples were normalized to a concentration of 1 mg protein/ml. We then treated 0.5 ml of serum with 0.5 ml of 10 mM dinitrophenylhydrazine in 2 M HCl, or with 0.5 ml of 2 M HCl alone for the blank. Samples were incubated for 1 hour at room temperature in the dark, and then treated with 10% trichloroacetic acid and centrifuged. The pellet was washed three times in ethanol/ethylacetate and solubilized in 1 ml of 6 M guanidine in 20 mM potassium phosphate, adjusted to pH 2.3 with trifluoracetic acid; the resulting solution was incubated at 37°C for 15 min. Carbonyl concentration was determined by spectrophotometry, from the difference in absorbance at 366 nm between dinitrophenylhydrazine-treated and HCl-treated samples, with ε370 = 22 mM-1cm-1. Protein concentration was determined in parallel. Carbonyl content is expressed as nmoles of carbonyl permilligram of protein.
AOPP were quantified as described previously [20]. We placed 200 μl of serum diluted 1:5 in phosphate-buffered saline into each well of a 96-well microtitre plate and added 20 μl of acetic acid to each well. For the standards, we added 10 μl of 1.16 M potassium iodide (Sigma, St Louis, MO, USA) to 200 μl of chloramine-T solution (0 to 100 μmol/l) (Sigma, St Louis, MO, USA) in a well and then added 20 μl of acetic acid. The absorbance of the reaction mixture was immediately read at 340 nm against a blank consisting of 200 μl of phosphate-buffered saline, 10 μl of 1.16 M potassium iodide, and 20 μl of acetic acid. AOPP concentrations are expressed as micromoles/litre of chloramine-T equivalents.
Statistical analysis
Data were analysed with the following nonparametric statistical methods: Mann–Whitney (unpaired data) and Wilcoxon (paired data) tests for comparison of groups, and Spearman's rank correlation test for assessment of the relationships between quantitative variables. P values of less than 0.05 were considered significant. All quantitative data are expressed as medians (range).
Results
We included 40 successive SSc patients (33 women and 7 men), with a mean age of 57 ± 12 years and a mean disease duration of 6 ± 4.5 years (21 patients had a disease duration of less than 5 years). The clinical and laboratory data for these patients are presented in Table 1. The control group was constituted of 20 healthy subjects (17 women, mean age 51 ± 7 years).
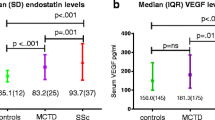
Serum markers of vascular injury (sVCAM), oxidative damage (carbonyl residues, AOPP), and angiogenesis (VEGF, sVEGFR-1) were all significantly higher in SSc patients than in controls (Table 2).
No correlation was found between VEGF concentrations and sVEGFR-1 concentration (r = 0.2; P = 0.2). The mean [VEGF]/[sVEGFR-1] ratio was not statistically different between SSc patients and controls (1580 ± 1750 vs 1660 ± 1580, P = 0.8). Baseline VEGF concentrations were correlated with carbonyl values (r = 0.43; P = 0.007; Fig. 1) but not with AOPP levels (r = 0.007; P = 0.9).

Correlation between carbonyl residue and vascular endothelial growth factor (VEGF) concentrations in systemic sclerosis patients at baseline (n = 40; r = 0.43; P = 0.007).
Concentrations of VEGF were inversely correlated with disease duration (r = -0.4; P = 0.01); patients who had had SSc for less than 5 years had higher median values than those with longer disease duration (633 [105–1915] vs 424 [26–961]; P = 0.03). VEGF levels were not significantly associated with the cutaneous subtypes; patients with diffuse disease had median VEGF concentrations similar to those of patients with limited cutaneous disease (603.5 [130–1915] vs 570 [26–1594]; P = 0.37). Concentrations of sVCAM-1 were not associated with SSc patient characteristics. We could not discern an influence on sVCAM-1, VEGF, or sVEGFR-1 concentrations of inflammation or treatment taken by SSc patients.
Nifedipine treatment significantly improved the vascular marker sVCAM-1 and markers of oxidative damage (carbonyls, AOPP) in patients with systemic sclerosis (SSc) but did not significantly influence VEGF or sVEGFR-1 concentrations (Table 3; Figs 2,3). There were significant correlations between individual levels at baseline and after nifedipine treatment for sVCAM-1 (r = 0.49; P = 0.03), carbonyl residues (r = 0.68; P = 0.003), and AOPP (r = 0.67; P = 0.005). The mean [VEGF]/[sVEGFR-1] ratio was not statistically different before and after nifedipine treatment (1100 ± 1190 vs 1450 ± 1280; P = 0.4).

Individual and median values of serum carbonyl concentrations in control subjects (n = 20) and patients with systemic sclerosis (SSc) at baseline and after treatment with 60 mg nifedipine per day (n = 20).

Individual and median values of serum sVCAM-1 concentrations in control subjects (n = 20) and patients with systemic sclerosis (SSc) at baseline and after treatment with 60 mg nifedipine per day (n = 20).
Discussion
We found that 14 days of treatment with nifedipine decreased serum vascular and oxidative damage markers in patients with SSc but did not significantly modify the concentration of VEGF or sVEGFR-1. Our results suggest that nifedipine can ameliorate endothelium injury in SSc and that VEGF signalling may by impaired in this disease without implication of the sVEGFR-1.
Endothelium injury is critical in SSc and is suspected to occur early in the disease process. Circulating sVCAM-1 is a recognised marker of disease activity and a possible marker of disease severity [6, 7, 21]; the expression of adhesion molecules seems crucial in this disease, which is characterised by early interactions between endothelial cells and mononuclear cells [22].
We previously demonstrated a sustained major decrease in oxidative stress in response to treatment with dihydropyridine-type calcium-channel blockers [17]. The data reported herein confirm these results with a different design of the study (midterm effects) and extend the known beneficial effects of these drugs to a vascular marker (sVCAM). The mechanism of the beneficial effects of dihydropyridines has not yet been determined and could result from intrinsic antioxidant properties [23] or from a secondary effect due to the improvement of the vasospastic disease. Whatever the mechanism involved, the concomitant decrease of sVCAM-1 concentration and oxidative stress markers suggests that these drugs improve endothelium injury. A decrease of sVCAM-1 by nifedipine was previously reported in SSc [24]. The improvement of all these markers and the correlation between the values before and after treatment suggest a powerful general action on endothelial injury. Calcium-channel blockers of the dihydropyridine type have clearly been shown to have an effect on Raynaud's syndrome in SSc and several studies have suggested that they act on coronary microvascular involvement [25]. Biological data showing their effects on SSc are scarce, but it has been suggested that nifedipine has an antiplatelet action [26]. Moreover, experimentally nifedipine may prevent apoptosis of endothelial cells [27].
Angiogenesis seems to be impaired in SSc and this could result from excessive angiostatic factors or disrupted VEGF signalling. We confirm herein the high concentration of VEGF in serum and its association with the early phase of the disease [9]. Moreover, we report high concentrations of the sVEGFR-1 in patients with SSc. sVEGFR-1 has a strong antagonistic activity and neutralises the effects of VEGF; it plays a pivotal role in the generation of vascular diseases such as pre-eclampsia and intrauterine growth retardation [28]. We hypothesised that the high VEGF concentration with impaired angiogenesis could result from sVEGFR-1 abnormalities; our results do not support this hypothesis, as the ratio between [VEGF] and [sVEGFR-1] did not differ between patients with SSc and controls. Several factors contribute to VEGF production, including hypoxic conditions and stimulation by transforming growth factor, CD40 ligand, interleukin 1, or interleukin 6 [10]. Oxidative stress also promotes angiogenesis [13]. The link between oxidative stress and angiogenesis is emphasised in SSc by the baseline correlation between carbonyl residues and VEGF concentrations. However, although oxidative damage markers were improved by nifedipine treatment, we did not detect significant changes in VEGF or sVEGFR-1 concentrations. Whereas it cannot be excluded that nifedipine does not target the VEGF pathway, this apparent lack of change supports the hypothesis that VEGF signalling is impaired in SSc, but more experimental data are needed in order to determine whether the VEGF pathway is intrinsically defective.
Conclusion
Nifedipine treatment ameliorated endothelium injury in patients with SSc, as shown by the concentrations of adhesion molecules and oxidative damage markers. The fact that VEGF and sVEGFR-1 concentrations were not changed whereas oxidative stress was ameliorated by nifedipine is consistent with the hypothesis that VEGF signalling is impaired in SSc. Our results also do not support the implication of the sVEGFR-1 in the VEGF dysregulation, but more experimental evidence is needed to determine whether the VEGF pathway is intrinsically defective in SSc.
Abbreviations
- AOPP:
-
advanced oxidation protein product(s)
- ELISA:
-
enzyme-linked immunosorbent assay
- SSc:
-
systemic sclerosis
- sVCAM-1:
-
soluble vascular cell adhesion molecule 1
- sVEGFR-1:
-
soluble VEGF receptor 1
- VEGF:
-
vascular endothelial growth factor.
References
LeRoy EC: Systemic sclerosis: a vascular perspective. Rheum Dis Clin North Am. 1996, 22: 675-694.
Fleiszchmajer R, Perlish JS: Capillary alterations in scleroderma. J Am Acad Dermatol. 1980, 2: 161-170.
Sgonc R, Gruschwitz MS, Boeck G, Sepp N, Gruber J, Wick G: Endothelial cell apoptosis in systemic sclerosis is induced by antibody-dependent cell-mediated cytotoxicity via CD95. Arthritis Rheum. 2000, 43: 2550-2562. 10.1002/1529-0131(200011)43:11<2550::AID-ANR24>3.0.CO;2-H.
Cerinic MM, Valentini G, Sorano GG, D'Angelo S, Cuomo G, Fenu L, Generini S, Cinotti S, Morfini M, Pignone A, Guiducci S, Del Rosso A, Kalfin R, Das D, Marongiu F: Blood coagulation, fibrinolysis, and markers of endothelial dysfunction in systemic sclerosis. Semin Arthritis Rheum. 2003, 32: 285-295. 10.1053/sarh.2002.50011.
Altman RD, Medsger TA, Bloch DA, Michel BA: Predictors of survival in systemic sclerosis (scleroderma). Arthritis Rheum. 1991, 34: 403-413.
Kahaleh B, Meyer O, Scorza R: Assessment of vascular involvement. Clin Exp Rheumatol. 2003, Suppl 29: S9-S14.
Denton CP, Bickerstaff MC, Shiwen X, Carulli MT, Haskard DO, Dubois RM, Black CM: Serial circulating adhesion molecule levels reflect disease severity in systemic sclerosis. Br J Rheumatol. 1995, 34: 1048-1054.
Kikuchi K, Kubo M, Kadono T, Yazawa N, Ihn H, Tamaki K: Serum concentrations of vascular endothelial growth factor in collagen diseases. Br J Dermatol. 1998, 139: 1049-1051. 10.1046/j.1365-2133.1998.02563.x.
Distler O, Del Rosso A, Giacomelli R, Cipriani P, Conforti ML, Guiducci S, Gay RE, Michel BA, Bruhlmann P, Muller-Ladner U, Gay S, Matucci-Cerinic M: Angiogenic and angiostatic factors in systemic sclerosis: increased levels of vascular endothelial growth factor are a feature of the earliest disease stages and are associated with the absence of fingertip ulcers. Arthritis Res. 2002, 4: R11-10.1186/ar596.
Choi JJ, Min DJ, Cho ML, Min SY, Kim SJ, Lee SS, Park KS, Seo YI, Kim WU, Park SH, Cho CS: Elevated vascular endothelial growth factor in systemic sclerosis. J Rheumatol. 2003, 30: 1529-1533.
Hebbar M, Peyrat JP, Hornez L, Hatron PY, Hachulla E, Devulder B: Increased concentrations of the circulating angiogenesis inhibitor endostatin in patients with systemic sclerosis. Arthritis Rheum. 2000, 43: 889-893. 10.1002/1529-0131(200004)43:4<889::AID-ANR21>3.0.CO;2-5.
Shibuya M: Structure and dual function of vascular endothelial growth factor receptor-1 (Flt-1). Int J Biochem Cell Biol. 2001, 33: 409-420. 10.1016/S1357-2725(01)00026-7.
Maulik N, Das DK: Redox signaling in vascular angiogenesis. Free Radic Biol Med. 2002, 33: 1047-1060. 10.1016/S0891-5849(02)01005-5.
Simonini G, Pignone A, Generini S, Falcini F, Cerinic MM, Gabriele S, Alberto P, Sergio G, Fernanda F, Marco MC: Emerging potentials for an antioxidant therapy as a new approach to the treatment of systemic sclerosis. Toxicology. 2000, 155: 1-15. 10.1016/S0300-483X(00)00272-9.
Thompson AE, Shea B, Welch V, Fenlon D, Pope JE: Calcium-channel blockers for Raynaud's phenomenon in systemic sclerosis. Arthritis Rheum. 2001, 44: 1841-1847. 10.1002/1529-0131(200108)44:8<1841::AID-ART322>3.0.CO;2-8.
Duboc D, Kahan A, Maziere B, Loc'h C, Crouzel C, Menkes CJ, Amor B, Strauch G, Guerin F, Syrota A: The effect of nifedipine on myocardial perfusion and metabolism in systemic sclerosis. A positron emission tomographic study. Arthritis Rheum. 1991, 34: 198-203.
Allanore Y, Borderie D, Lemaréchal H, Ekindjian OG, Kahan A: Acute and sustained effects of dihydropyridine-type calcium channel antagonists on oxidative stress in systemic sclerosis. Am J Med. 2004, 116: 595-600. 10.1016/j.amjmed.2003.11.022.
LeRoy EC, Black C, Fleischmajer R, Jablonska S, Krieg T, Medsger TA, Rowell N, Wollheim F: Scleroderma (systemic sclerosis): classification, subsets and pathogenesis. J Rheumatol. 1988, 1: 202-205.
Reznick AZ, Packer L: Oxidative damage to proteins: spectrophotometric method for carbonyl assay. Methods Enzymol. 1994, 233: 357-363.
Witko-Sarsat V, Friedlander M, Capelliere-Blandin C, Nguyen-Khoa T, Nguyen AT, Zingraff J, Jungers P, Descamps-Latscha B: Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49: 1304-1313.
Shahin AA, Anwar S, Elawar AH, Sharaf AE, Hamid MA, Eleinin AA, Eltablawy M: Circulating soluble adhesion molecules in patients with systemic sclerosis: correlation between circulating soluble vascular cell adhesion molecule-1 (sVCAM-1) and impaired left ventricular diastolic function. Rheumatol Int. 2000, 20: 21-4. 10.1007/s002960000072.
Prescott RJ, Freemont AJ, Jones CJ, Hoyland J, Fielding P: Sequential dermal microvascular and perivascular changes in the development of scleroderma. J Pathol. 1992, 166: 255-263.
Fukuo K, Yang J, Yasuda O, Mogi M, Suhara T, Sato N, Suzuki T, Morimoto S, Ogihara T: Nifedipine indirectly upregulates superoxide dismutase expression in endothelial cells via vascular smooth muscle cell-dependent pathways. Circulation. 2002, 106: 356-361. 10.1161/01.CIR.0000021924.02006.BA.
Dziadzio M, Denton CP, Smith R, Howell K, Blann A, Bowers E, Black CM: Losartan therapy for Raynaud's phenomenon and scleroderma: clinical and biochemical findings in a fifteen-week, randomized, parallel-group, controlled trial. Arthritis Rheum. 1999, 42: 2646-2655. 10.1002/1529-0131(199912)42:12<2646::AID-ANR21>3.0.CO;2-T.
Kahan A, Devaux JY, Amor B, Menkes CJ, Weber S, Nitenberg A, Venot A, Guerin F, Degeorges M, Roucayrol JC: Nifedipine and thallium-201 myocardial perfusion in progressive systemic sclerosis. N Engl J Med. 1986, 314: 1397-1402.
Rademaker M, Meyrick Thomas RH, Kirby JD, Kovacs IB: The anti-platelet effect of nifedipine in patients with systemic sclerosis. Clin Exp Rheumatol. 1992, 10: 57-62.
Sugano M, Tsuchida K, Makino N: Nifedipine prevents apoptosis of endothelial cells induced by oxidized low-density lipoproteins. J Cardiovasc Pharmacol. 2002, 40: 146-152. 10.1097/00005344-200207000-00018.
Carsten Hornig, Bernhard Barleon, Shakil Ahmad, Piia Vuorela, Asif Ahmed, Herbert A Weich: Release and complex formation of soluble VEGFR-1 from endothelial cells and biological fluids. Lab Invest. 2000, 80: 443-454.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Allanore, Y., Borderie, D., Lemaréchal, H. et al. Nifedipine decreases sVCAM-1 concentrations and oxidative stress in systemic sclerosis but does not affect the concentrations of vascular endothelial growth factor or its soluble receptor 1. Arthritis Res Ther 6, R309 (2004). https://doi.org/10.1186/ar1183
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/ar1183