
Abstract
The aim of this study was to investigate the relationship between the biochemical markers of arthritis and the radiographic grading of osteoarthritis (OA) in knees. Seventy-one women aged 49–85 years with knee OA were studied. Anterior–posterior knee radiographs and hand radiographs were taken in all patients. The radiographic grading of OA in the knee was performed by using the Kellgren–Lawrence criteria and the joint space width. The 71 patients with knee OA were divided into two groups: 37 patients exhibiting generalized osteoarthritis (GOA) and 34 non-GOA patients, according to the grading of their hand radiograph. C-reactive protein (CRP), urinary pyridinoline, YKL-40, plasma matrix metalloproteinase (MMP)-3, MMP-9 and tissue inhibitor of metalloproteinases (TIMP)-1 were measured as the biochemical markers of arthritis. The radiographic grading with the Kellgren–Lawrence scale revealed a significant relationship to the joint space width (P = 0.003): the joint space width decreased with increasing Kellgren–Lawrence grade. All biochemical markers had negative correlations with the joint space width, but only urinary pyridinoline had a significant correlation (P = 0.039). Pyridinoline (P = 0.034) and TIMP-1 (P = 0.017) also exhibited a significant relationship to the Kellgren–Lawrence grade. In GOA evaluations, the joint space width did not differ between GOA and non-GOA patients. CRP, pyridinoline, YKL-40 and MMP-3 levels were significantly greater in GOA patients than in non-GOA patients. CRP, pyridinoline, YKL-40, MMP-3 and TIMP-1 levels each related to at least one of the radiographic gradings. Furthermore, pyridinoline related to every type of radiographic grading examined in the present study.
Similar content being viewed by others


Introduction
New approaches in the treatment of osteoarthritis (OA), including new drug development, are hindered by the lack of objective and measurable standards for disease progression by which such treatments can be evaluated. Current methods of evaluating disease progression, including radiographs and biochemical markers, are not accurate enough to be used in clinical trials of potential treatments. Generally, an interval of a year or two is needed to observe any significant change in radiographic grading, whereas only a few months may be sufficient with biochemical markers to observe changes in the joint, which is most advantageous for monitoring treatment efficacy in arthritis [1]. There is a great potential in the use of biochemical markers of arthritis to diagnose the disease at an earlier stage, assess the severity of the disease and monitor the effect of any treatment. However, few sufficiently sophisticated biochemical markers are currently used in clinical applications.
If such markers were to become available, effective drug treatment would be possible or the timing and choice of surgery could be improved. It is therefore very important to make progress in the study of imaging and biochemical markers currently available. The aim of this study is to investigate the relationship between radiographic grading and biochemical markers for arthritis.
Materials and methods
Subjects
The present study is based on 71 postmenopausal women aged 49–85 years (mean of 68.5) with OA of the knee, which was diagnosed from clinical symptoms, examinations and radiographic findings. Secondary OA patients, such as post-traumatic OA cases, were excluded from the study. All patients fulfilled the ACR criteria for knee OA [2]. The procedures followed were in accordance with the principles of the Declaration of Helsinki in 1975, as revised in 1983.
Grading of OA
Antero-posterior weight-bearing radiographs of both knees and postero-anterior hand radiographs were taken [3]. The bilateral weight-bearing antero-posterior knee radiograph was taken with the patient standing with toes pointed straight ahead, knees fully extended, and weight equally distributed on both feet. The X-ray beam was aimed at the lower pole of the patella and kept parallel to the joint surface. The target–film distance was 36 inches [3]. The grading of radiographs was scored by an experienced observer (KN) who was blinded to the source of subjects. The joint space width of the medial and lateral compartments of antero-posterior films of the knee was measured in millimetres. A vertical line was drawn from the midfemoral medial and lateral condyles to the tibial plateau, and the lesser of the two measurements was taken as the joint space width [4].
Knee radiographs were evaluated with the Kellgren–Lawrence grading scale: grade 1, doubtful narrowing of joint space and possible osteophytic lipping; grade 2, definite osteophytes and possible narrowing of joint space; grade 3, moderate multiple osteophytes, definite narrowing of joints space, some sclerosis and possible deformity of bone contour; grade 4, large osteophytes, marked narrowing of joint space, severe sclerosis and definite deformity of bone contour [5]. The grade used for analysis was the higher of the two knees.
We define generalized OA (GOA) by the hypothesis that OA found in the hand is an indicator of disease in other large joints, including the spine. An individual was considered to have GOA if more than three interphalangeal joints scored at grades 2–4 on the Kellgren–Lawrence grading scale [5, 6]. With these criteria, 71 patients were divided into two groups: 37 GOA and 34 non-GOA patients.
Measurements of biochemical markers
Blood and urine samples were collected from all participants on the same day. Informed consent was obtained from all participants.
C-reactive protein (CRP)
CRP was assayed by latex photometric immunoassay as an in-hospital routine laboratory procedure. The assay detects CRP concentrations in the range 1–400 mg/l. The intra-assay and interassay coefficients of variance were below 10%.
Urinary pyridinoline
Aliquots of urine sample were hydrolysed with an equal volume of 12 M HCl for 20 hours at 110°C. Pyridinoline was measured with high-performance liquid chromatography (HPLC) directly linked to an ASPEC (Automated Sample Preparation with Extraction Columns) system [7]. The values of pyridinoline were corrected by urinary creatinine. The intra-assay and interassay coefficients of variance were 6.4% and 5.9%, respectively.
Serum YKL-40
Serum YKL-40 was measured with an enzyme-linked immunosorbent assay (ELISA) kit, a YKL-40™ (Metra Biosystems Inc, Mountain View, CA, USA), in accordance with the manufacturer's instructions [8]. The intra-assay variation of the method was 6.5% and the interassay variation was 12%.
Matrix metalloproteinases (MMPs) and tissue inhibitor of metalloproteinases (TIMP)
The plasma levels of MMP-3, MMP-9 and TIMP-1 were measured with enzyme immunoassay kits (Fuji Chemical Industries, Toyama, Japan) [9]. The intra-assay and interassay variations in MMP-3, MMP-9 and TIMP-1 were less than 8.9%.
Statistical analysis
The statistical significance between the two groups was determined by the Mann–Whitney U-test, and the statistical significance between three or more groups was determined with the Kruskal–Wallis test. Significant correlation was determined by the Spearman rank correlation test. P < 0.05 was considered significant.
Results
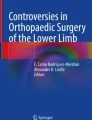
The relationship between the Kellgren–Lawrence grading and the joint space width is shown in Fig. 1. They were significantly related (P = 0.003): the joint space width decreased with increasing Kellgren–Lawrence grade. The relationship between the Kellgren–Lawrence grading and the biochemical markers is also shown in Fig. 1. A significant relationship was noted for pyridinoline (P = 0.034) and TIMP-1 (P = 0.017).

Relationship between Kellgren–Lawrence grading (KL), joint space width (JSW) and biochemical markers. Pyridinoline (Pyr) level is expressed as nmol/mmol creatinine. There were significant relationships between joint space width (P = 0.003), pyridinoline (P = 0.034) and TIMP-1 (P = 0.017) determined with the Kruskal–Wallis test. Bars indicate maximum and minimum values within the observation range. P values are shown in each panel; N.S. indicates not significant. CRP, C-reactive protein; MMP, matrix metalloproteinase; TIMP, tissue inhibitor of metalloproteinases.
Table 1 shows the correlations between the biochemical markers in all of the subjects as determined by the Spearman rank test. There were significant correlations between CRP and YKL-40, between pyridinoline and MMP-3, and between YKL-40 and MMP-3.
Table 2 shows the correlations between the joint space width and the biochemical markers. All markers had negative correlations with the joint space width, but only urinary pyridinoline had a significant correlation (P = 0.039).
Figure 2 shows the comparison of the joint space width and biochemical markers between patients with and without GOA. The joint space width did not differ between GOA and non-GOA. CRP (P = 0.043), pyridinoline (P = 0.046), YKL-40 (P < 0.0001) and MMP-3 (P = 0.008) were significantly greater in GOA than in non-GOA.

Comparison of joint space width (JSW) and the biochemical markers between generalized osteoarthritis (GOA) and non-GOA. Joint space width did not differ between GOA and non-GOA. C-reactive protein (CRP; P = 0.043), pyridinoline (Pyr; P = 0.046), YKL-40 (P < 0.0001) and matrix metalloproteinase-3 (MMP-3; P = 0.008) were significantly greater in GOA than in non-GOA determined with the Mann–Whitney U-test. Bars indicate maximum and minimum values within the observation range. P values are shown in each panel; N.S. indicates not significant. TIMP, tissue inhibitor of metalloproteinases.
Discussion
We studied two radiographic grading criteria: Kellgren–Lawrence grading and joint space width. These two methods for evaluating the degree of OA are widely used. In the present study they were significantly related to each other: the Kellgren–Lawrence grade varied inversely with joint space width. We also used the concept of GOA as a means of radiographic grading of OA [10]. Several disease subsets in OA are recognized clinically. These subsets of OA fall into two broad groups: those causing biomechanical loading or instability at a specific joint, and those influencing generalized and systemic susceptibility to the process at multiple joints. The concept of generalized and systemic susceptibility is supported by studies indicating a subset of patients with polyarticular disease known as GOA. Earlier GOA is characterized by hand OA as a generalized nodal OA, which is a familial disease affecting mostly women and characterized by the development of Heberden nodes and a specific pattern of OA showing multiple joint involvement. Because levels of serum biochemical markers for arthritis depend on the circulating concentrations of molecules derived from the affected joints, the marker level is expected to be higher in patients with multiple joint involvement than in patients with a specific joint site. Therefore, in this study, to ascertain the ability of joint markers we used two OA populations: a knee OA group and a GOA group. The results obtained showed that CRP, pyridinoline, YKL-40 and MMP-3 were significantly greater in the GOA group than in the non-GOA group. In contrast, there was no significant difference in joint space width between the GOA and non-GOA groups.
There are two major categories of substances that are currently being investigated as potential biochemical markers for arthritis. One includes constituents of the extracellular matrix of the joint tissues; the other includes enzymes or cytokines that metabolize the molecules of the joint tissues. Among the biochemical markers investigated in the present study, pyridinoline is a major crosslink of collagen in the joint tissues, which is abundant both in cartilage and bone, and belongs to the former group. MMPs and TIMP are proteolytic enzymes that belong to the latter group [11]. We do not know which group YKL-40 belongs to, because the function and origin of this substance is still not clear [12]. Although the function of YKL-40 is not yet known, several studies have suggested that YKL-40 might be a useful new marker for patients with OA and rheumatoid arthritis [13]. However, the biochemical markers of bone metabolism are also proposed as indicators of disease progress of OA [14, 15]. Spector and colleagues demonstrated that bone resorption is increased in patients with progressive knee OA and is not increased in those with nonprogressive knee OA. Altered bone turnover might be a diagnostic or therapeutic target in patients with progressive OA [16].
Urinary pyridinoline has the most consistent relationship with radiographic grades of OA among the biochemical markers studied here. Pyridinium crosslinks consist of two major molecules, namely pyridinoline and its analogue deoxypyridinoline. Although both crosslinks are located in several tissues, deoxypyridinoline is more specifically located in bone, whereas pyridinoline is most abundant in cartilage and bone. Urinary excretion of deoxypyridinoline is therefore used clinically as a marker of bone metabolism, whereas urinary excretion of pyridinoline is considered to be a biochemical marker for cartilage destruction and metabolism as well as bone metabolism [17]. However, because pyridinoline locates in several tissues of the joint in a significant amount [18], urinary pyridinoline might be affected by the synthesis of osteophytes, sclerosis of subchondral bone and synovial degeneration as well as cartilage degeneration in the joints of OA.
Conclusion
In conclusion, CRP, pyridinoline, YKL-40, MMP-3 and TIMP-1 levels were each related to at least one of the radiographic gradings. Furthermore, pyridinoline was related to every type of radiographic grading examined in the present study.
Abbreviations
- CRP:
-
C-reactive protein
- GOA:
-
generalized osteoarthritis
- MMP:
-
matrix metalloproteinase
- OA:
-
osteoarthritis
- TIMP:
-
tissue inhibitor of metalloproteinases.
References
Garnero P, Landewe R, Boers M, Verhoeven A, Van Der Linden S, Christgau S, Van Der Heijde D, Boonen A, Geusens P: Association of baseline levels of markers of bone and cartilage degradation with long-term progression of joint damage in patients with early rheumatoid arthritis: the COBRA study. Arthritis Rheum. 2002, 46: 2847-2856. 10.1002/art.10616.
Altman RD: Criteria for classification of clinical osteoarthritis. J Rheumatol. 1991, 18 (suppl 27): 10-12.
Leach RE, Gregg T, Siber FJ: Weight-bearing radiography in osteoarthritis of the knee. Radiology. 1970, 97: 265-268.
Altman RD, Fries JF, Bloch DA, Carstens J, Cooke TD, Genant H, Gofton P, Groth H, McShane DJ, Murphy WA, et al: Radiographic assessment of progression in osteoarthritis. Arthritis Rheum. 1987, 30: 1214-1225.
Kellgren JH, Lawrence JS: Radiological assessment of osteoarthrosis. Ann Rheum Dis. 1957, 16: 494-502.
Doherty M, Watt I, Diepple P: Influence of primary generalized osteoarthritis on development of secondary osteoarthritis. Lancet. 1983, ii: 8-11. 10.1016/S0140-6736(83)90003-X.
Pratt DA, Daniloff Y, Duncan A, Robins SP: Automated analysis of the pyridinium crosslinks of collagen in tissue and urine using solid-phase extraction and reversed-phase high-performance liquid chromatography. Anal Biochem. 1992, 207: 168-175. 10.1016/0003-2697(92)90519-D.
Harvey S, Weisman M, O'Dell J, Scott T, Krusemeier M, Visor J, Swindlehurst C: YKL-40: new marker of joint disease. Clin Chem. 1998, 44: 509-516.
Obata K, Iwata K, Okada Y, Kohrin Y, Ohuchi E, Yoshida S, Shinmei M, Hayakawa T: A one-step sandwich enzyme immunoassay for human matrix metalloproteinase 3 (stromelysin-1) using monoclonal antibodies. Clin Chim Acta. 1992, 211: 59-72. 10.1016/0009-8981(92)90105-Y.
Cooper C, Egger P, Coggon D, Hart DJ, Masud T, Cicuttini F, Doyle DV, Spector TD: Generalized osteoarthritis in women: pattern of joint involvement and approaches to definition for epidemiological studies. J Rheumatol. 1996, 23: 1938-1942.
Hasty KA, Reife RA, Kang AH, Stuart JM: The role of stromelysin in the cartilage destruction that accompanies inflammatory arthritis. Arthritis Rheum. 1990, 33: 388-397.
Steck E, Breit S, Breusch SJ, Axt M, Richter W: Enhanced expression of the human chitinase 3-like 2 gene (YKL-39) but not chitinase 3-like 1 gene (YKL-40) in osteoarthritic cartilage. Biochem Biophys Res Commun. 2002, 299: 109-115. 10.1016/S0006-291X(02)02585-8.
Johansen JS, Kirwan JR, Price PA, Sharif M: Serum YKL-40 concentrations in patients with early rheumatoid arthritis: relation to joint destruction. Scand J Rheumatol. 2001, 30: 297-304. 10.1080/030097401753180381.
Naitou K, Kushida K, Takahashi M, Ohishi T, Inoue T: Bone mineral density and bone turnover in patients with knee osteoarthritis compared with generalized osteoarthritis. Calcif Tissue Int. 2000, 66: 325-329. 10.1007/s002230010068.
Hunter DJ, Spector TD: The role of bone metabolism in osteoarthritis. Curr Rheumatol Rep. 2003, 5: 15-19.
Bettica P, Cline G, Hart DJ, Meyer J, Spector TD: Evidence for increased bone resorption in patients with progressive knee osteoarthritis: longitudinal results from the Chingford study. Arthritis Rheum. 2002, 46: 3178-3184. 10.1002/art.10630.
Robins SP, Stewart P, Astbury C, Bird HA: Measurement of the cross linking compound, pyridinoline, in urine as an index of collagen degeneration in joint disease. Ann Rheum Dis. 1986, 45: 969-973.
Takahashi M, Kushida K, Hoshino H, Suzuki M, Sano M, Miyamoto S, Inoue T: Concentrations of pyridinoline and deoxypyridinoline in joint tissue from patients with osteoarthritis or rheumatoid arthritis. Ann Rheum Dis. 1996, 55: 324-327.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Takahashi, M., Naito, K., Abe, M. et al. Relationship between radiographic grading of osteoarthritis and the biochemical markers for arthritis in knee osteoarthritis. Arthritis Res Ther 6, R208 (2004). https://doi.org/10.1186/ar1166
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/ar1166