
Abstract
Introduction
Heterogeneity in risk of conversion to Alzheimer's disease (AD) among individualswith mild cognitive impairment (MCI) is well known. Novel statistical methods thatare based on partially ordered set (poset) models can be used to create modelsthat provide detailed and accurate information about performance with specificcognitive functions. This approach allows for the study of direct links betweenspecific cognitive functions and risk of conversion to AD from MCI. It also allowsfor further delineation of multi-domain amnestic MCI, in relation to specificnon-amnestic cognitive deficits, and the modeling of a range of episodic memoryfunctioning levels.
Methods
From the Alzheimer's Disease Neuroimaging Initiative (ADNI) study, conversion at24 months of 268 MCI subjects was analyzed. It was found that 101 of thosesubjects (37.7%) converted to AD within that time frame. Poset models were thenused to classify cognitive performance for MCI subjects. Respective observedconversion rates to AD were calculated for various cognitive subgroups, and byAPOE e4 allele status. These rates were then compared across subgroups.
Results
The observed conversion rate for MCI subjects with a relatively lower functioningwith a high level of episodic memory at baseline was 61.2%. In MCI subjects whoadditionally also had relatively lower perceptual motor speed functioning and atleast one APOE e4 allele, the conversion rate was 84.2%. In contrast, the observedconversion rate was 9.8% for MCI subjects with a relatively higher episodic memoryfunctioning level and no APOE e4 allele. Relatively lower functioning withcognitive flexibility and perceptual motor speed by itself also appears to beassociated with higher conversion rates.
Conclusions
Among MCI subjects, specific baseline cognitive profiles that were derived throughposet modeling methods, are clearly associated with differential rates ofconversion to AD. More precise delineation of MCI by such cognitive functioningprofiles, including notions such as multidomain amnestic MCI, can help in gainingfurther insight into how heterogeneity arises in outcomes. Poset-based modelingmethods may be useful for providing more precise classification of cognitivesubgroups among MCI for imaging and genetics studies, and for developing moreefficient and focused cognitive test batteries.
Similar content being viewed by others
Introduction
There is increasing interest in the recognition and treatment of prodromal stages ofAlzheimer's disease (AD), especially mild cognitive impairment (MCI). MCI is viewed as astate between normal cognitive functioning and dementia. Those with MCI arecharacterized as exhibiting mild problems with memory and/or other cognitive functions,while still being able to perform daily life activities normally or nearly so[1]. Despite having a higher overall riskof developing AD [1], conversion outcomes amongthose with MCI are quite heterogeneous. Only about 15% of these individuals convert toAD per year; many never convert, and some revert to normal cognition [2]. This heterogeneity makes it difficult to designefficient trials of agents designed to delay or prevent progression from MCI to AD or tointerpret the outcomes of these trials [3], or toevaluate potential AD biomarkers. Hence, there is a clear need to better delineatecognitive phenotypes in MCI.
Although MCI subgroups that reflect deficit heterogeneity, such as amnestic singledomain MCI, amnestic multidomain MCI, and non-amnestic multidomain MCI [4] have been developed, they lack specificity in theparticular cognitive functions that are impaired in each subgroup. This type ofspecification is challenging because neuropsychological (NP) response data are complex.It can be difficult to isolate a deficit in a particular cognitive function, sinceperforming well on most NP measures requires tapping into several cognitive functions,and it is often not possible to design tests that tap one cognitive domain to theexclusion of all others. For example, it is possible to perform poorly on a verballist-learning task as a result of impaired attention or word fluency, and in the absenceof an amnestic disturbance. Hence, if an individual performs poorly on a given measure,it may be difficult to pinpoint exactly which function is impaired.
Subscales are commonly used in an attempt to improve specificity in analysis of NPassessment data. For instance, subscales can be derived from factor analysis through theuse of factor scores. However, scale-based approaches are generally limited by theassumption of a direct correspondence between a subscale score and an associatedfunction. Poor performance on a subscale is interpreted as indicating a deficit in thefunction the subscale is purported to measure, even if the poor performance is due todeficits in functions not associated with the subscale. This makes it difficult to linkNP test performance to specific functional deficits, and hence to identify cognitivephenotypes that can be linked to outcomes such as conversion from MCI to AD.
Use of total scores on multi-item measures, such as the Alzheimer's disease assessmentscale-cognitive (ADAS-Cog) measure [5] or themini-mental status exam (MMSE) [6], as a basisfor cognitive phenotyping is also problematic. Total scores represent a (weighted) sumof response scores from items assessing several cognitive domains. However, the sametotal score can be derived from a range of different response patterns, without regardto the cognitive functions being assessed by each item. In this sense, items are viewedas interchangeable, even though the cognitive targets of assessment for the items canvary considerably. Because a wide range of response patterns and cognitiveinterpretations can give rise to the same score, resulting phenotypes lackspecificity.
The partially ordered set (poset) modeling approach to interpreting NP data
Poset models serve as a basis for novel methods tailored for classifying theperformance (that is, functioning) levels of subjects with respect to specificcognitive functions. Classification is conducted based on observed responses to NPmeasures. Each measure is associated with specific cognitive functions that areinvolved in performing well on that measure, so that the ties between observedresponses and functioning levels are clear. This approach is feasible because posetshave essential statistical convergence properties such as assuring that a subject'sstate is identified accurately with sufficient measurement, even in the presence ofmeasures that are associated with multiple functions. Theoretically derivedvalidation tools are available as well. Statistical theory and data-analyticframeworks for the poset approach have been established in Tatsuoka and Ferguson(2003) [7] and Tatsuoka (2002) [8].
In this paper, our goal is to demonstrate that posets can improve our understandingof MCI heterogeneity. The modeling results in the development of states associatedwith profiles of cognitive functioning that summarize performance levels for each ofthe cognitive functions being tested by a given NP battery. Hence, a state can beviewed as similar to a diagnostic classification in which the diagnosis represents aparticular pattern of cognitive strengths and weaknesses. States are ordered bycomparing the associated performance levels for each of the functions included in theanalysis. One state is considered greater than a second state if its associatedperformance level on at least one function is strictly higher than the performancelevel for the second state, and its performance levels for all other functions are atleast as high. However, posets are flexible in that it is not necessary that onestate be greater than another, in other words, the states can be partially ordered.This arises when one state in comparison to another state has a higher performancelevel with respect to one function, while having a lower performance level withrespect to another function. This enables models to reflect a complex range ofresponses from an NP battery.
A probability distribution on the states is used to represent belief about whichstate best describes the cognitive capabilities of a subject. Bayes' rule is used toobtain updated posterior probabilities of state membership once responses to measuresare observed. This allows for a systematic manner in which the information obtainedfrom observing multiple measures can be combined for statistical classification. Tworesponse distributions are estimated per NP measure, one representing the responsetendencies of subjects who perform at a relatively high level on all functionsassociated with the particular measure and another for those subjects who do not.These distributions are used to weigh the relative likelihood of an observed responseindicating that a subject has the associated higher level functioning. The approachof estimating two response distributions per NP measure is parsimonious in that thereis no need to estimate response distribution parameters that are specific to eachprofile; rather, response distribution parameters are shared either by profiles thathave the associated functioning levels, or those that do not. Ideally, one state inthe model will have a probability close to 1 for each individual, while other stateswill have probabilities near 0, indicating that a subject's cognitive profile isknown with near certainty. As long as models are correctly specified, this nearcertainty will indeed be obtained given a sufficient amount of testing [7]. Once classification is completed, subjects whoshare a cognitive profile can be aggregated, and observed rates of conversion to ADbetween the resulting subgroups can be compared.
In our study, we used NP data collected by the Alzheimer's Disease NeuroimagingInitiative (ADNI) [9] to evaluate theusefulness of poset models to identify specific cognitive phenotypes associated withconversion from MCI to AD [7, 8, 10, 11]. Wehypothesized that poset modeling would generate interpretable and sufficientlydetailed cognitive phenotypes with clearly differentiated rates of conversion fromMCI to AD. Given its established importance in progression risk for AD,Apolipoprotein E (APOE) e4 status was also taken into account [12, 13].
Materials and methods
Study sample
MCI subjects enrolled in the ADNI (n = 389) were included in theclassification analysis if their scores on the selected NP battery were available atboth baseline and at 24 months. The sample was 64.5% male and 93.1% Caucasian. About3.8% were African American, 2.8% were Asian, and 0.3% were American Indian or AlaskanNative. Mean age was 74.8 years (SD = 7.5) and mean length of education was 15.7years (SD = 3.0).
Modeling and classification approach
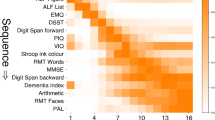
We used neuropsychologist expert opinion (JJ and HYT) to map the relationship betweenselected ADNI NP measures (ADAS delayed recall and word recognition subscales andnumber cancellation; auditory verbal learning test (AVLT) Trial 6 and List B; Bostonnaming test; category fluency; trail making Test A and Test B, and Wechsler adultintelligence scale-revised (WAIS-R) digit symbol substitution) and the cognitivefunctions required to perform them (episodic memory at four different levels, wordfluency, cognitive flexibility, perceptual motor speed, and attention). See Table1 for the listing of these specifications. Measures wereselected based on the types of functions they tested and retained based onstatistical criteria such as discriminatory properties and correspondence with modelfit. Given the reliance on expert opinion, data-analytic validation is important.Statistical details on how this validation was performed are provided in Additionalfile 1 (Appendix).
To acknowledge the key role of episodic memory impairment as an early symptom in ADand to better represent the varying levels of episodic memory required across themeasures, we identified four levels of episodic memory proficiency (levels 0 through3). These levels are ordered in terms of episodic memory demand, with level thehighest, and level 0 the lowest. Level 3 corresponds to relatively longer-termdelayed recall with distractors, while level 2 and level 1, respectively, relate toshorter and shorter recall durations involved in AVLT List B and immediate recall. Asubject at level 0 cannot perform well at any of the other levels. A brief summary ofthe practical interpretation of the episodic memory levels to be used here is givenin Table 2.
Through the assumed hierarchical ordering between levels of episodic memory, notethat the delayed recall measures that involve level 3 also can provide information onfunctioning with levels 1 and 2. High functioning at level 3 implies high functioningat levels 1 and 2 as well. Also, poor performance on word recognition, which isassociated with level 1, not only provides evidence that level 1 is at a low level,but that functioning at levels 2 and 3 should be low as well. Hence, even thoughassociations of measures involving episodic memory can be at different levels, theystill can inform other levels of episodic memory functioning, affording some degreeof replication.
Poset model generation
A poset model was generated based on the functions associated with each of the ADNINP measures. In the cognitive profiles associated to states in the model, performancelevels for a function were denoted either as relatively high, or relatively low, inrelation to the MCI and early AD sample. See Table 3 for acomplete list of profiles that can be distinguished by the given set of NP measuresthat were analyzed.
The resultant poset model comprised 29 states. These states (and associated cognitiveprofiles) represent the profiles that can be distinguished from the NP battery, andwere identified algorithmically from the expert-derived specifications in Table 1[14]. Table 3 shows how the cognitive functions we examined are distributedacross states to create distinct cognitive profiles. The corresponding partialordering of these profiles is graphically depicted in Figure 1as a Hasse diagram. Note that state 1 is the highest state in the poset, as it hasthe highest level of functioning for all five cognitive functions. State 29 is thelowest state, since all its functioning for all five functions is at the lowestlevel. For the in-between states, there exists at least one function for whichperformance is not at a relatively high level. In the diagram, connected linesbetween states indicate direct ordering, with the higher of the states being greaterthan the lower one.

Partially ordered set (poset) model for cognitive functioning of mildcognifitive impairment and early Alzheimer's disease subjects.
In our analysis, a uniform prior probability value of 1/29 was assigned to each statefor each subject to indicate prior belief about which profile would fit a givensubject. We then estimated two response distributions for each NP measure asdescribed above. These distributions were then used to weigh the relative likelihoodthat an observed response indicated that a subject had the associated higher levelfunctioning.
Response distributions
Responses from both the MCI subjects and also early AD subjects (an additional 174such subjects) were included in the estimation, to allow for a range of values. Giventhe apparent non-normality of response data, nonparametric approaches to responsedistribution estimation were adopted [10, 11, 15–17] (see Additional file 1).
Grouping of profiles and classified subjects
The ordered relationships between states arise when identifying subgroups with sharedfunctioning levels for a function. For instance, the subgroup of states that havehigh performance level for episodic memory level 2 are all the states greater than orequal to state 14. Precisely, this would be state 1 through 12, and state 14. Thecomplement of this subgroup (all states not greater than or equal to state 14) wouldthus comprise the states with lower performance level. Once subgroups such as thishave been identified and classification conducted, the probability that a subject hasa particular performance level for a function can be computed by summing theposterior probabilities of membership of each of the states in the subgroup. Theseprobabilities are used as a basis for cutoff values in function-related groupings,which are then compared statistically in terms of proportion of AD conversions fromMCI. All reported P-values are two-sided.
We treated cognitive flexibility slightly differently from other NP functions, due toconfounding of its functioning status in classification under certain profiles,specifically for states 7, 14, 21, and 28. Confounded profiles arise due tolimitations of the NP battery to distinguish all possible profiles. Profiles withconfounding give conflicting information about certain functions, but probabilitiesfor a subject being at certain functioning levels can still be obtained by weightingthe information provided across a set of confounded profiles (see Additional file1 for more details).
Model validation
Briefly, model fit appears to be good. Response distribution estimates for allmeasures correspond to the assumed order structure, in that those subjects expectedby the model to score well actually tended to do so, and those not expected to scorewell tended not to do so. Moreover, classification was fairly decisive, especiallygiven the limited number of NP measures employed. Observed responses to the measureswere thus consistent with the model specifications. See Figures S1 through S6 andTable S1 in Additional file 1.
Results and discussion
We explored different cognitive groupings within MCI subjects, to assess conversionrates to AD at two years post baseline. Not surprisingly, episodic memory is thecognitive function that appears to be most significantly related to future conversion.Still, the different performance levels of episodic memory in our model appear to havevarying degrees and ways of association with conversion outcomes. For instance, as seenin Table 4, level 2 episodic memory performance levels influencethe rate of conversion among those with MCI. In subjects for whom level 2 episodicmemory functioning is low (in other words, below the cutoff probability value of lessthan 0.275), 41 out of 67 (61.2%±11.7%, 95% CI) converted to AD within two years,which is much higher than the overall MCI to AD conversion rate in this sample of 101out of 268 (37.7%±5.8%, 95% CI). Those with relatively lower performance in level 2of episodic memory significantly differ in conversion rates compared with those withhigher performance, regardless of whether or not the APOE e4 allele is present. TheP-value for Fisher's exact test is 0.000 for a two-sided test of noassociation between conversion and having relatively low episodic memory level 2functioning.
Other functions where relatively lower functioning at baseline may indicate higher riskfor conversion from MCI to AD are perceptual motor speed and cognitive flexibility. Forperceptual motor speed, using a cutoff probability value of 0.40 to delineate a lowerfunctioning subgroup, and considering subjects with at least one APOE4 allele, 23 of 35(65.7%±15.7%, 95% CI) of MCI subjects with relatively low functioning convert to ADwithin 24 months. On the other hand, only 14 of 35 MCI subjects with relatively lowperceptual motor speed and without an APOE4 allele convert (40%±16.2%, 95% CI).Further, for cognitive flexibility, using a cutoff probability value of 0.30 todelineate a lower functioning subgroup, 28 of 48 (58.3%±13.9%, 95% CI) of MCIsubjects with relative low baseline functioning convert to AD within 24 months. In thiscase, the P-value for Fisher's exact test of no association is 0.007.
Interestingly, we conversely found much lower rates of conversion among certaincognitive profiles. In particular, only four out of forty-one (9.8%±9.1%, 95% CI)MCI subjects with no APOE e4 alleles and relatively high level-3 episodic memoryfunctioning (cutoff probability value greater than 0.80) convert in two years. This rateappears to be lower than for subjects with no APOE e4 allele but without high level-3episodic memory functioning (P-value = 0.001, Fisher's exact test of noassociation).
Amnestic multidomain MCI identified with poset models
An advantage of the poset approach is the ability to provide classification toprofiles that address a range of functions. Subgroups, such as amnestic multidomainMCI, can be characterized more precisely by identifying specific functions that arerelatively impaired along with episodic memory.
In our sample, subjects with relatively low functioning on episodic memory level 2(probability of being at high level at level 2 being 0.275 or less) and perceptionspeed (probability cutoff value of 0.40 or less) were identified. As shown in Table5, among subjects with at least one APOE e4 allele and withrelatively low levels of both episodic memory and perception speed, 16 out of 19converted (84.2%±16.4%, 95% CI). Considering only subjects with lower level-2episodic memory functioning, those who additionally have lower functioning inperceptual motor speed appear even more likely to convert (P-value = 0.013,Fisher's exact test of no association). In contrast, additionally having lowerfunctioning with cognitive flexibility did not appear to significantly increase riskfor conversion. Among subjects with lower episodic memory level 2 functioning,observed percentages of conversion with and without lower cognitive flexibility were66.7% versus 57.5% (18 out of 27 versus 23 out of 40).
Cognitive change before conversion
Over the range of cognitive functions, histograms were generated for the respectiveprobabilities of converters having relatively high functioning over the 24 monthspreceding conversion. Analogous histograms were generated for non-converters over atime period of the same duration starting from baseline. See Figures 2, 3, 4, 5, 6, 7, 8. Note that for non-converters, only those subjects who did not convertover the full 36-month period of the study were included in the plots. By comparingcorresponding plots between converters and non-converters, it becomes clearer how theabove findings of heterogeneity in conversion outcomes by cognitive profilearose.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning with episodic memorylevel 1 from 24 to 0 months before conversion to AD among MCI subjects.Respectively, n = 75, 75, 68, 51, and 36 for 0, 6, 12, 18 and 24months before conversion. (b) Probability of relatively high functioningwith episodic memory level 1 from baseline (0 months) to 24 months among MCIsubjects who did not convert within 36 months; n = 90.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning with episodic memorylevel 2 from 0 to 24 months before conversion to AD among MCI subjects.(b) Probability of relatively high functioning with episodic memorylevel 2 from baseline to 24 months among MCI subjects who did not convertwithin 36 months.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning with episodic memorylevel 3 from 24 to 0 months before conversion to AD among MCI subjects.(b) Probability of relatively high functioning with episodic memorylevel 3 from baseline to 24 months among MCI subjects who did not convertwithin 36 months.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning with word fluency from24 to 0 months before conversion to AD among MCI subjects. (b)Probability of relatively high functioning with word fluency from baseline to24 months among MCI subjects who did not convert within 36 months.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning withattention/sustained vigilance from 24 to 0 months before conversion to AD amongMCI subjects. (b) Probability of relatively high functioning withattention/sustained vigilance from baseline to 24 months among MCI subjects whodid not convert within 36 months.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning with cognitiveflexibility from 24 to 0 months before conversion to AD among MCI subjects.(b) Probability of relatively high functioning with cognitiveflexibility from baseline to 24 months among MCI subjects who did not convertwithin 36 months.

Probabilities of functioning over time among mild cognitive impairment (MCI)converters to Alzheimer's disease (AD) versus MCI non-converters.(a) Probability of relatively high functioning with perceptual motorspeed from 24 to 0 months before conversion to AD among MCI subjects.(b) Probability of relatively high functioning with perceptual motorspeed from baseline to 24 months among MCI subjects who did not convert within36 months.
For Figures 2, 3, 4, which correspond to the episodic memory levels, note that relative tolevel 2, level 1 does not see the same amount of decline over 24 months forconverters, as reflected by a shift to lower probability values. Hence, thediscrepancy between the histograms in Figures 2a versus 2b overtime between converters and non-converters is not very strong. On the other hand, inFigures 3a and 3b, it is clear that forconverters, there is quite a bit of decline in level 2 values during this timeperiod, while non-converters appear stable. This makes level 2 attractive fordiscrimination and prediction over this duration. In Figures 4aand 4b, note that level 3 functioning is low among almost allconverters preceding conversion. However, lower functioning for this more difficultlevel also is common for non-converters, lessening the discriminatory properties oflevel 3. Still, there is a sizeable proportion of non-converters retaining highprobability values for level 3, which allows for cognitively-based identification ofa very low-risk group.
In Figures 5a and 5b, it appears thatthere may be decline in word fluency values for a relatively small subset of subjectsas they near conversion, but many converters also appear to retain high functioning.For non-converters, some subjects have lower functioning as well. Hence, word fluencydoes not appear useful for predicting conversion within a two-year period. In Figures6a and 6b, note that there may be someslight decline in attention/sustained vigilance for converters, but almost allsubjects still retain high probability values for being at a high level of attentionfunctioning.
In Figures 7a and 7b, there is definitelya fair amount of decline in values for cognitive flexibility among converters,although it is also not as pronounced as for episodic memory level 2. Also, someconverters retain high functioning. Most non-converters retain high functioning overthe duration. Hence, cognitive flexibility can be useful for discriminating futureconversion outcomes, but does not appear as informative as episodic memory level 2.Finally, in Figures 8a and 8b, forperceptual motor speed, note that there appears to be a subset of converters for whomperceptual motor speed becomes more impaired. While there are non-converters who alsohave low probability values, this number is outweighed by the converters over theduration. Moreover, as Table 5 indicates, these converters arelikely to also be relatively more impaired with episodic memory level 2 than thenon-converters. This allows us to identify this particular combination of lower levelfunctioning as being specifically associated with high risk for conversion.
Multivariate prediction using logistic regression models
A multivariate model was fit that recognized the above findings, and included othervariables such as gender, age, and educational level. The presence of an APOE4 allelewas viewed as a binary variable, as well as whether or not a subject had attendedcollege. Also, probability values for performing at a relatively high level forepisodic memory level 2, cognitive flexibility, and perceptual motor speed wereviewed as continuous explanatory variables. After an initial fit of a full model,gender, age, and educational level were clearly not significant predictors in themodel (respective P-values were 0.96, 0.65, and 0.81; Wald's test). Usinggoodness-of-fit tests based on the test statistic of -2 times the difference inlog-likelihood values to compare nested models, it appears the best fit is whenepisodic memory level 2, perceptual motor speed, and APOE4 status are included in themodel. Results are given in Table 6. Note that episodic memorylevel 2, perceptual motor speed, and APOE4 status all are significant predictors(P-value <0.05; Wald's test). When cognitive flexibility is includedwith these variables, it is not significant (P-value = 0.26).
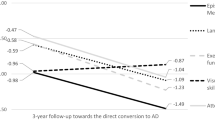
Using the model-based estimated probabilities of converting to AD as a predictor, andfor instance, using a cutoff value of 0.55 or higher, classification accuracy is66.8%, with positive predictive value of 61.5% (32 out of 52). Figure 9 displays receiver operating characteristic (ROC) curves for theselogistic regression probabilities, as well as for the probabilities for episodicmemory level 2, perceptual motor speed, and cognitive flexibility. Values for thearea under the curve (AUC) are 0.710, 0.678, 0.655, and 0.644, respectively. Using amultivariate approach can thus apparently improve prediction. However, compared torelying upon episodic memory level 2 alone without the need for APOE4 statusinformation, which would have practical appeal, the difference does not appear to bestriking.

Area under the curve (AUC). Multivariate logistic model probabilityvalues for conversion = 0.710, episodic memory level 2 probability of highfunctioning = 0.678, perceptual motor speed probability of high functioning =0.655, cognitive flexibility probability of high functioning = 0.644.
Other prediction approaches
A comprehensive review of research efforts using ADNI data is given in Weiner etal. (2012) [18]. This includes adescription of work on prediction of MCI to AD conversion. Taking advantage of therichness of the ADNI data, prediction models have been developed based on a range ofvarious imaging, cerebrospinal fluid, and genetic biomarkers, as well as cognition.Our prediction results appear to be comparable to non-cognitively oriented methodsthat rely on baseline data [19, 20]. Advantages of a cognitive testing approach includenon-invasiveness and cost, especially if focused and efficient NP batteries can bedesigned, and computer-based adaptive testing adopted in the future.
Other cognitive testing-based approaches to prediction include Tabert et al.(2006) [21] and Fleisher et al.(2007) [22]. Their prediction models dependdirectly on NP measurement scores, which in general may be difficult to interpret interms of identifying which cognitive functions may be the source of poor scores. Webelieve that the results presented here add to these works, such as through a morespecific consideration of multidomain MCI. Poset-based methods also provided insightinto the course of cognitive change in MCI, by indicating how specific functions areaffected over time. The findings depicted in Figure 4 allow forinsight into the heterogeneity in cognitive progressions that arise among MCI, andthus help in identifying profiles of high risk.
Conclusions
Our results suggest the utility of the poset-based approach in uncovering heterogeneityin risk for conversion from MCI to AD by generating subgroups tied to specific cognitivefunctions. Duration of 24 months from baseline measurement was considered. Among thecognitive functions evaluated, episodic memory was mostly strongly linked to conversionfrom MCI to AD. This confirms similar findings in Tierney et al. (2005)[23], Tabert et al. (2006)[21], Blacker et al. (2007)[24], and Landau et al. (2010)[18]. We did find that cognitiveflexibility and perceptual motor speed also is associated with conversion, as certainsubjects are apparently affected in these domains during the 24 months precedingconversion. Conversely, MCI subjects with relatively less episodic memory impairmentwere observed to convert at a much lower rate. The importance of the APOE e4 allele inaffecting risk for conversion is also clear [18, 19].
More precisely, it appears that in our model certain levels of episodic memoryfunctioning are more discriminatory than others in terms of identifying MCI subjects atespecially high risk for conversion. In particular, level-2 episodic memory functioning,more so than level-3, appears to best identify risk for conversion. It appears thatdelayed recall with distractors may be too difficult a task to discriminate risk verywell. On the other hand, for those that can perform well at level 3 relative to otherswith MCI, risk of conversion is much lower, as illustrated in Table 5.
Poset modeling also appears to be helpful in further clarifying the notion ofmultidomain MCI. Our analyses suggest that perceptual motor speed functioning may have astronger link to subsequent risk of AD progression than other cognitive functions whenconsidered in conjunction with relatively reduced function of level-2 episodic memory.On the other hand, additional impairment with cognitive flexibility does not appear toincrease risk beyond that due to episodic memory impairment. These results suggest thathaving relatively lower functioning across multiple functions can indeed increase riskfor AD, but, that it may matter which of the functions are impaired. Becausecorresponding samples become smaller as specific combinations of deficits are analyzed,however, these analyses must be viewed as preliminary.
A possible concern is that the ranges of performance levels for functions in the posetmodel are limited, particularly when a functioning level is either high or low. However,it should be kept in mind that there are also limited NP response data available, due tothe time-consuming and burdensome nature of NP measurement. Hence, there are statisticallimitations to the granularity of information on functioning that can be assessedaccurately. Our model was shown to be feasible, while still being able to providediscriminating information relating to AD conversion. Another limitation is the scope ofinference that can be made from the ADNI sample, which was overwhelmingly Caucasian, andimbalanced towards males. Certainly, these findings should be validated in otherdatasets.
Future directions
Since the poset model allows for precise and detailed cognitive profiles, thisapproach can be used in conjunction with imaging and genetic studies. As an example,a cluster analysis approach has recently been applied to characterize MCI subgroupsby cognitive characteristics [25]. Whilewhite matter lesion burden was found to differ by these groupings, in general,cognitive subtypes resulting from cluster analysis can at times be more difficult tointerpret than profiles generated with poset models. Also, note the persistentheterogeneity of conversion outcomes among MCI subjects even within the cognitivelyhomogeneous subgroups generated here. These subgroups could be an interesting basisfor functional magnetic resonance imaging (fMRI) studies of cognitive reserve, whichmay improve understanding of how this heterogeneity arises [26, 27]. Poset modeling may also beuseful in clinical trial design, as enriched sampling from subgroups of MCI subjectsthat have high positive predictive value of conversion could reduce sample sizerequirements.
Finally, poset models can serve as a basis for adaptive NP testing, with NP measuresbeing selected for administration dynamically, based on the responses that havealready been observed [7, 8]. As demonstrated, an attractive feature of poset models isthat since they are comprised of discrete states, accurate statistical classificationcan be conducted with relatively few measures. Adaptive tests can further reducesubject burden and allow for more focused and efficient testing, which in turn wouldenhance the appeal of cognitive testing for prediction.
Abbreviations
- AD:
-
Alzheimer's disease
- ADAS-Cog:
-
Alzheimer's disease assessment scale-cognitive
- ADNI:
-
Alzheimer's Disease Neuroimaging Initiative
- APOE:
-
Apolipoprotein E
- AUC:
-
area under thecurve
- AVLT:
-
auditory verbal learning test
- fMRI:
-
functional magnetic resonance imaging
- MCI:
-
mild cognitive impairment
- MMSE:
-
mini-mental status exam
- NP:
-
neuropsychological
- poset:
-
partially ordered set
- ROC:
-
receiver operator characteristic
- WAIS-R:
-
Wechsleradult intelligence scale-revised.
References
Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins PV, Ritchie K, Rossor M, Thal L, Winblad B: Current concepts in mild cognitive impairment. Arch Neurol. 2001, 58: 1985-1992. 10.1001/archneur.58.12.1985.
Petersen RC, Thomas RG, Grundman M, Bennett D, Doody R, Ferris S, Galasko D, Jin S, Kaye J, Levey A, Pfeiffer E, Sano M, van Dyck CH, Thal LJ, Alzheimer's Disease Cooperative Study Group: Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med. 2005, 352: 2379-2388. 10.1056/NEJMoa050151.
Andrieu S, Coley N, Aisen P, Carrillo MC, DeKosky S, Durga J, Fillit H, Frisoni GB, Froelich L, Gauthier S, Jones R, Jönsson L, Khachaturian Z, Morris JC, Orgogozo JM, Ousset PJ, Robert P, Salmon E, Sampaio C, Verhey F, Wilcock G, Vellas B: Methodological issues in primary prevention trials for neurodegenerativedementia. J Alzheimers Dis. 2009, 16: 235-270.
Petersen RC: Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004, 256: 183-194. 10.1111/j.1365-2796.2004.01388.x.
Rosen WG, Mohs RC, Davis KL: A new rating scale for Alzheimer's disease. Am J Psychiatry. 1984, 141: 1356-1364.
Folstein MF, Folstein SE, McHugh PR: "Mini-mental state". A practical method for grading the cognitive state ofpatients for the clinician. J Psychiatr Res. 1975, 12: 189-198. 10.1016/0022-3956(75)90026-6.
Tatsuoka C, Ferguson T: Sequential classification on partially ordered sets. Journal of the Royal Statistical Society, Series B. 2003, 65: 143-157. 10.1111/1467-9868.00377.
Tatsuoka C: Data analytic methods for latent partially ordered classification models. Journal of the Royal Statistical Society, Series C (Applied Statistics). 2002, 51: 337-350. 10.1111/1467-9876.00272. See also Corrigendum 2005, 54:465-467
Aisen PS, Petersen RC, Donohue MC, Gamst A, Raman R, Thomas RG, Walter S, Trojanowski JQ, Shaw LM, Beckett LA, Jack CR, Jagust W, Toga AW, Saykin AJ, Morris JC, Green RC, Weiner MW, Alzheimer's Disease Neuroimaging Initiative: Clinical core of the Alzheimer disease neuroimaging initiative: Progress andplans. Alzheimers Dement. 2010, 6: 239-246. 10.1016/j.jalz.2010.03.006.
Jaeger J, Tatsuoka C, Berns S, Varadi F, Czobor P, Uzelac S: Associating functional recovery with neurocognitive profiles identified usingpartially ordered classification models. Schizophr Res. 2006, 85: 40-48. 10.1016/j.schres.2006.03.005.
Jaeger J, Tatsuoka C, Berns SM, Varadi F: Distinguishing neurocognitive functions in schizophrenia using partially orderedclassification models. Schizophr Bull. 2006, 32: 679-691.
Landau SM, Harvey D, Madison CM, Reiman EM, Foster NL, Aisen PS, Petersen RC, Shaw LM, Trojanowski JQ, Jack CR, Weiner MW, Jagust WJ, Alzheimer's Disease Neuroimaging Initiative: Comparing predictors of conversion and decline in mild cognitive impairment. Neurology. 2010, 75: 230-238. 10.1212/WNL.0b013e3181e8e8b8.
Aggarwal NT, Wilson RS, Beck TL, Bienias JL, Berry-Kravis E, Bennett DA: The apolipoprotein E epsilon4 allele and incident Alzheimer disease in personswith mild cognitive impairment. Neurocase. 2005, 11: 3-7. 10.1080/13554790490903038.
Tatsuoka C: Sequential classification on partially ordered sets. PhD thesis. 1996, Cornell University, Statistics Department
Ishwaran H, James LF: Approximate Dirichlet process computing in finite normal mixtures: Smoothing andprior information. J Comp Graph. 2002, 97: 1154-1166.
Tatsuoka C, Varadi F, Jaeger J: Latent partially ordered classification models and normal mixtures. Journal of Educational and Behavioral Statistics.
Geweke J: Evaluating the accuracy of sampling-based approaches to the calculation ofposterior moments. Bayesian Statistics 4. Edited by: Bernardo JM, Berger J, Dawid AP, Smith AFM. 1992, Oxford, UK: Oxford University Press,
Weiner MW, Veitch DP, Aisen PS, Beckett LA, Cairns NJ, Green RC, Harvey D, Jack CR, Jagust W, Liu E, Morris JC, Petersen RC, Saykin AJ, Schmidt ME, Shaw L, Siuciak JA, Soares H, Toga AW, Trojanowski JQ, Alzheimer's Disease Neuroimaging Initiative: The Alzheimer's Disease Neuroimaging Initiative: A review of papers publishedsince its inception. Alzheimer's & Dementia. 2012, 8 (Suppl): S1-S68.
Querbes O, Aubry F, Pariente J, Lotterie JA, Demonet JF, Duret V, Puel M, Berry I, Fort JC, Celsis P, Alzheimer's Disease Neuroimaging Initiative: Early diagnosis of Alzheimer's disease using cortical thickness: impact ofcognitive reserve. Brain. 2009, 132: 2036-2047. 10.1093/brain/awp105.
Ewers M, Walsh C, Trojanowski JQ, Shaw LM, Petersen RC, Jack CR, Feldman HH, Bokde AL, Alexander GE, Scheltens P, Vellas B, Dubois B, Weiner M, Hampel H, North American Alzheimer's Disease Neuroimaging Initiative (ADNI): Prediction of conversion from mild cognitive impairment to Alzheimer's diseasedementia based upon biomarkers and neuropsychological test performance. Neurobiol Aging. 2012, 33: 1203-1214. 10.1016/j.neurobiolaging.2010.10.019.
Tabert MH, Manly JJ, Liu X, Pelton GH, Rosenblum S, Jacobs M, Zamora D, Goodkind M, Bell K, Stern Y, Devanand DP: Neuropsychological prediction of conversion to Alzheimer disease in patients withmild cognitive impairment. Arch Gen Psychiatry. 2006, 63: 916-24. 10.1001/archpsyc.63.8.916.
Fleisher AS, Sowell BB, Taylor C, Gamst AC, Petersen RC, Thal LJ: Clinical predictors of progression to Alzheimer disease in amnestic mild cognitiveimpairment. Neurology. 2007, 68: 1588-1595. 10.1212/01.wnl.0000258542.58725.4c.
Tierney MC, Yao C, Kiss A, McDowell I: Neuropsychological tests accurately predict incident Alzheimer disease after 5 and10 years. Neurology. 2005, 64: 1853-1859. 10.1212/01.WNL.0000163773.21794.0B.
Blacker D, Lee H, Muzikansky A, Martin EC, Tanzi R, McArdle JJ, Moss M, Albert M: Neuropsychological measures in normal individuals that predict subsequentcognitive decline. Arch Neurol. 2007, 64: 862-871. 10.1001/archneur.64.6.862.
Delano-Wood L, Bondi MW, Sacco J, Abeles N, Jak AJ, Libon DJ, Bozoki A: Heterogeneity in mild cognitive impairment: Differences in neuropsychologicalprofile and associated white matter lesion pathology. J Int Neuropsychol Soc. 2009, 15: 906-914. 10.1017/S1355617709990257.
Stern Y: Cognitive reserve and Alzheimer disease. Alzheimer Dis Assoc Disord. 2006, 20 (Suppl 2): S69-S74.
Stern Y: Cognitive reserve. Neuropsychologia. 2009, 47: 2015-2028. 10.1016/j.neuropsychologia.2009.03.004.
Alzheimer's Disease Neuroimaging Initiative (ADNI) database. [http://www.loni.ucla.edu/ADNI]
Alzheimer's Disease Neuroimaging Initiative (ADNI) investigators. [http://www.loni.ucla.edu/ADNI/Collaboration/ADNI_Authorship_list.pdf]
Foundation for the National Institutes of Health. [http://www.fnih.org]
Alzheimer's Disease Neuroimaging Initiative (ADNI). [http://www.adni-info.org]
Acknowledgements
This work was funded in part by the grants from AstraZeneca Pharmaceuticals and TheG.R. Lincoln Family Foundation. Data collection and sharing for this project wasfunded by the ADNI (National Institutes of Health Grant U01 AG024904). ADNI is fundedby the National Institute on Aging, the National Institute of Biomedical Imaging andBioengineering, and through generous contributions from the following: Abbott,AstraZeneca AB, Bayer Schering Pharma AG, Bristol-Myers Squibb, Eisai Global ClinicalDevelopment, Elan Corporation, Genentech, GE Healthcare, GlaxoSmithKline,Innogenetics, Johnson and Johnson, Eli Lilly and Co., Medpace, Inc., Merck and Co.,Inc., Novartis AG, Pfizer Inc, F. Hoffman-La Roche, Schering-Plough, Synarc, Inc., aswell as non-profit partners, the Alzheimer's Association and Alzheimer's DrugDiscovery Foundation, with participation from the US Food and Drug Administration.Private sector contributions to ADNI are facilitated by the Foundation for theNational Institutes of Health [30]. Thegrantee organization is the Northern California Institute for Research and Education,and the study is coordinated by the Alzheimer's Disease Cooperative Study at theUniversity of California, San Diego. ADNI data are disseminated by the Laboratory forNeuroimaging at the University of California, Los Angeles. This research was alsosupported by NIH grants P30 AG010129, K01 AG030514, and the Dana Foundation.
Alzheimer's Disease Neuroimaging Initiative (ADNI): 'Data used in the preparation ofthis article were obtained from the Alzheimer's Disease Neuroimaging Initiative(ADNI) database [28]. The ADNI was launchedin 2003 by the National Institute on Aging (NIA), the National Institute ofBiomedical Imaging and Bioengineering (NIBIB), the Food and Drug Administration(FDA), private pharmaceutical companies and non-profit organizations, as a $60million, 5-year public private partnership. The primary goal of ADNI has been to testwhether serial magnetic resonance imaging (MRI), positron emission tomography (PET),other biological markers, and the progression of mild cognitive impairment (MCI) andearly Alzheimer's disease (AD). Determination of sensitive and specific markers ofvery early AD progression is intended to aid researchers and clinicians to developnew treatments and monitor their effectiveness, as well as lessen the time and costof clinical trials. The Principal Investigator of this initiative is Michael WWeiner, MD, VA Medical Center and University of California - San Francisco.
ADNI is the result of efforts of many co-investigators from a broad range of academicinstitutions and private corporations, and subjects have been recruited from over 50sites across the US and Canada. The initial goal of ADNI was to recruit 800 adults,ages 55 to 90, to participate in the research - approximately 200 cognitively normalolder individuals to be followed for 3 years, 400 people with MCI to be followed for3 years and 200 people with early AD to be followed for 2 years.' For up-to-dateinformation, see [31].
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
Dr Tatsuoka was funded in part by AstraZeneca Pharmaceuticals to do this research, andhas written a related patent. Drs Tseng, Varadi, Smyth and Yamada have no conflicts ofinterest to report. Dr Jaeger was Director, Global Medicines Development, Neuroscience,AstraZeneca Pharmaceuticals during the funding of this research, and is now withCogState, Inc. Dr Smith was a consultant for Anavex Life Sciences Corporation,Medivation, Eisai, Glaxo Welcome Kline, and Neurotez; he owns stock options in Neurotez,Aria, Panancea, and Curaxis Pharmaceuticals. Dr Lerner receives research support fromForest Labs, Pfizer, Medivation, Baxter Labs, and Avid Pharmaceuticals.
Authors' contributions
CT developed the statistical methods, conducted statistical analyses, and helped preparethe manuscript; HYT conducted analyses; JJ helped frame and conduct the analyses; FVprogrammed the software, helped in developing the statistical methods, and helped in theanalysis; MS helped in the analyses; TY conducted analyses; KS helped in the analysesand prepared the manuscript; AL helped frame and conduct the analyses, and prepare themanuscript. All authors have read and approved the manuscript for publication. Data usedin the preparation of this article were obtained from the ADNI database [28]. As such, the investigators within the ADNIcontributed to the design and implementation of ADNI and/or provided data but did notparticipate in analysis or writing of this report. ADNI investigators include a completelisting available at [29].
Electronic supplementary material
13195_2012_141_MOESM1_ESM.PDF
Additional file 1: Appendix: Statistical framework for data analysis and model validation.This file contains statistical details relating to the poset modeling,including parameter estimates and classification summaries. It also describeshow model validation was conducted. (PDF 7 MB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Tatsuoka, C., Tseng, H., Jaeger, J. et al. Modeling the heterogeneity in risk of progression to Alzheimer's disease acrosscognitive profiles in mild cognitive impairment. Alz Res Therapy 5, 14 (2013). https://doi.org/10.1186/alzrt168
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/alzrt168