
Abstract
Purpose
This study tested possible cross-country differences in the associations between diabetes and activities of daily living (ADLs), and possible confounding / mediating effects of socio-economic status, obesity, and exercise.
Methods
Data came from Research on Early Life and Aging Trends and Effects (RELATE). The study included a total number of 25,372 community sample of adults who were 40 years or older. We used data from community based surveys in seven countries including China, Mexico, Barbados, Brazil, Chile, Cuba, and Uruguay. Demographics (age and gender), socio-economic status (education and income), obesity, exercise, and ADL (bath, dress, toilet, transfer, heavy, shopping, meals) were measured. Self-reported data on physician diagnosis of diabetes was the independent variable. We tested if diabetes is associated with ADL, before and after adjusting for socio-economics, obesity, and exercise in each country.
Results
Based on Model I (age and gender adjusted model), diabetes was associated with limitation in at least one ADL in Mexico, Barbados, Brazil, Chile, Cuba, and Uruguay, but not China. Based on Model II that also controlled for education and income, education explained the association between diabetes and limitation in ADL in Mexico and Uruguay. Based on Model III that also controlled for exercise and obesity, in Cuba and Brazil, exercise explained the link between diabetes and limitation in performing ADLs. Thus, the link between diabetes and ADL was independent of our covariates only in Chile and Barbados.
Conclusions
There are cross-country differences in the link between diabetes and limitation in ADL. There are also cross-country differences in how socio-economic status, obesity, and exercise explain the above association.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
About three hundred fifty million people have diabetes worldwide [1]. With a direct medical cost of 465 billion U.S. dollars in the year 2011, diabetes is responsible for more than 10% of total healthcare expenditures in adults [2].
People with diabetes are more likely to experience limitations in activities of daily living (ADL), mobility, and role functioning [3–5]. Given the growing rate of diabetes and its associated disability burden in the world [2], for different reasons, more research is still needed on the link between diabetes and ADLs [6].
First, research on disability among people with diabetes may suggest avenues for reducing the disability attributable to this common chronic disease [3]. Second, although diabetes has been consistently related to a broad spectrum of health outcomes, including quality of life, ADL and mobility disability [7], and lower extremity function [8], it is not clear if the association between diabetes and ADL remains significant after controlling for other factors, and also it is not clear if the same link exits in different countries [9]. Third, a large proportion of a major part of evidence on the link between diabetes and burden of mobility-related disability has originated from studies conducted on patients, or disabled individuals [9]. However, clinical samples and community individuals vary on many factors and there is a need to show the ADLs among individuals with diabetes in a community sample. Finally, more research is needed on cross-country differences in associations between diabetes and disabilities.
Although literature has frequently shown that diabetes has a role in the disablement of people, further research is needed to extend the current limited knowledge about this association [9]. The current study tested cross-country differences in association between diabetes and ADLs.
Methods
Data came from Research on Early Life and Aging Trends and Effects (RELATE), that included seven different studies [10]. This analysis included 25,372 individuals who were age 40 or older. These individuals were sampled in the following seven countries: China, Mexico, Barbados, Brazil, Chile, Cuba, and Uruguay. All surveys were fully in compliance with the Helsinki Declaration on ethical principles for medical research involving humans. Different institutional review boards approved participating surveys.
The following countries were participating in RELATE project and represented countries from a diverse range in national income levels: Barbados represents high income countries; Cuba, Uruguay, Chile, Brazil, and Mexico represent upper middle income countries; and China represents lower middle income countries [11].
Although most country-specific surveys had sampling weights, as recommended, the current study did not apply sampling weights. The main reason was that sampling weights were not applicable to data from China (China Health and Nutrition Study; CHNS).
Measures
Demographic characteristics
The study measured age (continuous variable) and gender (dichotomous variable of male and female) as two demographic variables.
Socio-economic status
The study measured education (four level categorical variable of 1) no schooling, 2) primary to elementary, 3) secondary to intermediate, and 4) higher), and income(continuous variable) as socio-economic status.
Obesity and exercise
The study measured obesity and exercise based on self reported data. BMI larger than 30 was considered as obesity.
Main outcome
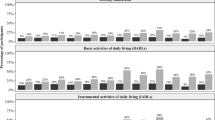
Seven activities of daily living (ADLs) were measured by a modified Barthel index [12–15]. ADL items that were included in this study included bath, dress, toilet, transfer, heavy, shopping, and meals. These items have been frequently used to assess ADLs in the community sample [16, 17].
Data analysis
Data analysis was conducted using SPSS for Windows. We used country specific logistic regressions to determine if diabetes is associated with ADLs, and if this link is independent of socio-economic factors (education, and income), obesity and exercise. In all models, at least one ADL limitation was our outcome. In Model I, we only adjusted for age and gender. In Model II, we also adjusted for education and income. In Model III, we also adjusted for obesity and exercise.
Results
Table 1 shows country differences by means of mean age, education, income, and ADLs. Mean age was lowest in China, and highest in Brazil. ADL limitation was highest in Chile, and lowest in Uruguay. Education was lowest in Brazil, and highest in Cuba. Income was highest in Uruguay and lowest in Cuba.
Model I
Based on the first model, with an exception of China, diabetes was associated with ADL, and this link was independent of age and gender. Gender and age were associated with ADL in all countries (Table 2).
Model II
Based on Model II that also controlled for education and income, education explained the association between diabetes and limitation in ADL in Mexico and Uruguay. Based on this model, gender and age were associated with ADL in all countries. However, education was not correlated with ADL in Barbados, Cuba, and Uruguay. Income was linked to ADL in China and Brazil (Table 3).
Model III
Based on Model III that also controlled for obesity and exercise, in Cuba and Brazil, exercise explained the link between diabetes and limitation in performing ADLs. Based on this model, the link between diabetes and ADL was independent of our covariates only in Chile and Barbados. Based on this model, gender and age were associated with ADL in all countries. Obesity was linked to ADL only in Barbados. Exercise was linked to ADL in all countries (Table 4).
Discussion
Our study showed at least four important cross-country differences in the pattern of association between diabetes and disability; 1) in most (i.e. Mexico, Barbados, Brazil, Chile, Cuba, and Uruguay) but not all countries (China), diabetes seems to be associated with ADL, 2) in some countries (i.e. Mexico and Uruguay), education explains the association between diabetes and ADL limitation, 3) in some countries (i.e. Cuba and Brazil), exercise explains the link between diabetes and ADLs, and 4) in some countries (i.e. Chile and Barbados), the link between diabetes and ADL seems to be independent of our covariates/mediators.
Only in Chile and Barbados was the link between diabetes and ADL independent of all study covariates/mediators. Based on a study in Japan, history of diabetes, bone fractures, and heart diseases contributed to some specific aspects of ADL disabilities, however, cerebrovascular disease influenced all aspects of ADL [18].
We showed that in Cuba and Brazil, physical activity might be a mechanism behind the link between diabetes and ADL. According to the literature, at least a part of the limitations in ADLs of patients with diabetes might be due to function in extremities. A study examined how hand disorders contribute to ADLs among elderly men with diabetes, and showed that limited joint motion (measured by prayer sign and Dupuytren's contracture) was more common in individuals with diabetes, compared to non-diabetics. Vibrotactile sense was impaired symmetrically in the index and little fingers in diabetics [19].
Peripheral artery disease and peripheral nerve dysfunction are known causes of diabetes -related disability [9, 20], and may explain more than 30% of the association of diabetes with disability related dysfunction in physical activity. Physical activity is particularly important for people with diabetes, because being physically active can improve the body's ability to use insulin and facilitate weight loss [21–25]. In the United States, for example, only one-third of individuals with diabetes and obesity are physically active [26, 27]. Interventions need to enhance physical activity of patients, and this may break the cycle by which diabetes causes limitation in performing ADLs.
The current study failed to show mediating or confounding effects of obesity on the association between diabetes and ADLs. However, obesity had an independent association with ADLs in one of the seven countries (Barbados). Literature suggests that obesity and overweight may mediate or confound the link between diabetes and disability. In a survey among obese diabetic individuals, ADL was linked to current exercise, using exercise programs, and self-reported weight history [28]. In a qualitative study among obese (body mass index [BMI] > 30 kg/m2) individuals with diabetes, patients believed that their performance of daily activities would improve with weight loss of 5–10% of body weight [29].
The ability to remain physically active is an essential aspect of quality of life and is critical for the preservation of independence among patients with diabetes. Lower extremity function is a strong predictor of poor health outcomes, including disability, hospitalization, and death among patients [30, 31]. Recently, a search for potentially modifiable conditions associated with impaired mobility and lower extremity function identified several socio-demographic and behavioral characteristics, along with acute and chronic medical conditions [32, 33]. Among the latter group, diabetes has been shown to be consistently a correlate of poor extremity performance [34, 35].
Several impairments and comorbidities are involved in the disablement process associated with diabetes. Obesity, visual impairment, and cardiovascular diseases may mediate the association between diabetes and disability among diabetic patients. These conditions are important causes of different aspects of physical dysfunction in older individuals [36, 37].
The association between diabetes and ADLs did not stay significant in the multivariable models in most countries. The literature is also not informative about the question of whether or not the link between diabetes and disability is independent of other factors that contribute to disability. We know that several conditions that may contribute to the impairment in ADLs are more prevalent in diabetic patients than controls. These conditions may be the actual mechanisms by which diabetes is associated with physical disability. Some of these conditions include cardiovascular diseases, peripheral neuropathy, obesity, and visual deficits [35].
Our findings are important for different reasons. As very few studies have shown exact mechanisms by which disability is seen among patients with diabetes [35], our knowledge about the mechanisms underlying the disability among diabetic patients is limited. Further research is needed to know which complication of the disease plays a more important role in the disablement process. Further research is also needed on possible synergistic effects of different conditions associated with diabetes [38]. In addition, prevalence of diabetes is expected to increase considerably in the next decades [38]. And knowledge from similar studies may be important for planning strategies aimed at preventing or slowing functional decline in older persons and for tertiary prevention in subjects with diabetes [9].
Our study has strengths and limitations. This was a cross-national survey composed of different surveys conducted in seven countries [10]. Research on Early Life and Aging Trends and Effects (RELATE) did not collect data on duration of diabetes, or mental health of the participants. Duration of diabetes is known to be strongly linked to disability among patients with diabetes. We also did not collect data on degree of metabolic imbalance, as we know loss of control of glucose may be a mediator for the disabling effect of diabetes [9]. Based on the literature, high prevalence of depression among diabetic patients may explain a substantial proportion of the excess risk of disability associated with diabetes. Depression is common among patients with diabetes [39–41]. Longitudinal studies are warranted to elucidate the role of depression in the pathway from diabetes to disability. Our study is one of very few studies that contribute to our understandings of cross – country differences in morbidity related to diabetes. To study cross – country differences in mental health associates of diabetes, one study used data from World Mental Health, and showed that with a consistent pattern, in all countries, mood and anxiety disorders occurred with somewhat greater frequency among persons with diabetes than those without diabetes, and the strength of association did not differ significantly across countries [42]. It is essential to conduct more research to test if the association between diabetes and disability is independent of other chronic conditions or not [9].
Our study sheds light on cross – country differences in factors associated with well-being. Considerable differences in morbidity, life satisfaction, and well-being have been shown across the globe [43, 44]. The World Values Survey, European Values Study, Eurobarometer, and Latinobarometer, have consistently shown that life expectancy, physical health, all-cause mortality, and also subjective well-being vary across countries [45–48].
Conclusion
To conclude, our study showed considerable differences in the association between diabetes and disability across countries. The study also suggests that there might be some cross-country differences in the factors that may explain this link.
References
Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al.: National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet 2011, 378: 31–40. 10.1016/S0140-6736(11)60679-X
International Diabetes Foundation: Global Burden. http://www.idf.org/diabetesatlas/5e/the-global-burden
Ryerson B, Tierney EF, Thompson TJ, Engelgau MM, Wang J, Gregg EW, Geiss LS: Excess physical limitations among adults with diabetes in the US population, 1997–1999. Diabetes Care 2003, 26: 206–10. 10.2337/diacare.26.1.206
Gregg EW, Beckles GL, Williamson DF, Leveille SG, Langlois JA, Engelgau MM, Narayan KM: Diabetes and physical disability among older US adults. Diabetes Care 2000, 23: 1272–7. 10.2337/diacare.23.9.1272
Volpato S, Blaum C, Resnick H, Ferrucci L, Fried LP, Guralnick JM: Women’s Health and Aging Study. Diabetes Care 2002, 25: 678–83. 10.2337/diacare.25.4.678
Von Korff M, Katon W, Lin EH, Simon G, Ludman E, Oliver M, Ciechanowski P, Rutter C, Bush T: Potentially modifiable factors associated with disability among people with diabetes. Psychosom Med 2005, 67(2):233–40. 10.1097/01.psy.0000155662.82621.50
Bourdel-Marchasson I, Dubroca B, Manciet G, Decamps A, Emeriau JP, Dartigues JF: Prevalence of diabetes and effect on quality of life in older French living in the community: the PAQUID Epidemiological Survey. J Am Geriatr Soc 1997, 45: 295–301.
Ferrucci L, Penninx BW, Leveille SG, Corti MC, Pahor M, Wallace R, Harris TB, Havlik RJ, Guralnik JM: Characteristics of nondisabled older persons who perform poorly in objective tests of lower extremity function. J Am Geriatr Soc 2000, 48: 1102–1110.
Volpato S, Blaum C, Resnick H, Ferrucci L, Fried LP, Guralnik JM: Women’s Health and Aging Study. Comorbidities and impairments explaining the association between diabetes and lower extremity disability: the Women's Health and Aging Study. Diabetes Care 2002, 25(4):678–83. 10.2337/diacare.25.4.678
McEniry M: Research on Early Life and Aging Trends and Effects (RELATE): A Cross-National Study. ICPSR34241-v1. Ann Arbor, MI: Inter-university Consortium for Political and Social Research [distributor]; 2013:06–12. 10.3886/ICPSR34241.v1 Persistent URL: http://dx.doi.org/10.3886/ICPSR34241.v1
The World Bank: How we Classify Countries. http://data.worldbank.org/about/country-classifications
Mahoney FI, Barthel D: Functional evaluation: the Barthel Index. Md State Med J 1965, 14: 56–61.
Loewen SC, Anderson BA: Predictors of stroke outcome using objective measurement scales. Stroke 1990, 21: 78–81. 10.1161/01.STR.21.1.78
Gresham GE, Phillips TF, Labi ML: ADL status in stroke: relative merits of three standard indexes. Arch Phys Med Rehabil 1980, 61: 355–358.
Collin C, Wade DT, Davies S, Horne V: The Barthel ADL Index: a reliability study. Int Disability Study 1988, 10: 61–63. 10.3109/09638288809164103
Dudgeon BJ, Hoffman JM, Ciol MA, Shumway-Cook A, Yorkston KM, Chan L: Managing activity difficulties at home: a survey of Medicare beneficiaries. Arch Phys Med Rehabil 2008, 89(7):1256–61. 10.1016/j.apmr.2007.11.038. Epub 2008 Jun 13 10.1016/j.apmr.2007.11.038
Ostchega Y, Harris TB, Hirsch R, Parsons VL, Kington R: The prevalence of functional limitations and disability in older persons in the US: data from the National Health and Nutrition Examination Survey III. J Am Geriatr Soc 2000, 48(9):1132–5.
Kishimoto M, Ojima T, Nakamura Y, Yanagawa H, Fujita Y, Kasagi F, Kodama K, Ueda K, Suzuki S, Kagamimori S: Relationship between the level of activities of daily living and chronic medical conditions among the elderly. J Epidemiol 1998, 8(5):272–7. 10.2188/jea.8.272
Cederlund RI, Thomsen N, Thrainsdottir S, Eriksson KF, Sundkvist G, Dahlin LB: Hand disorders, hand function, and activities of daily living in elderly men with type 2 diabetes. J Diabetes Complications 2009, 23(1):32–9. 10.1016/j.jdiacomp.2007.09.002
Dermott MM, Fried L, Simonsick E, Ling S, Guralnik JM: Asymptomatic peripheral arterial disease is independently associated with impaired lower extremity functioning: the Women’s Health and Aging Study. Circulation 2000, 101: 1007–1012. 10.1161/01.CIR.101.9.1007
Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, Chasan-Taber L, Albright AL, Braun B: American College of Sports Medicine; American Diabetes Association: exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care 2010, 33: e147-e167. 10.2337/dc10-9990
De Feo P, Di Loreto C, Ranchelli A, Fatone C, Gambelunghe G, Lucidi P, Santeusanio F: Exercise and diabetes. Acta Biomed 2006, 77(Suppl 1):14–17.
Kirk A, De Feo P: Strategies to enhance compliance to physical activity for patients with insulin resistance. Appl Physiol Nutr Metab 2007, 32: 549–556. 10.1139/H07-023
Balducci S, Zanuso S, Nicolucci A, De Feo P, Cavallo S, Cardelli P, Fallucca S, Alessi E, Fallucca F, Pugliese G: Italian Diabetes Exercise Study (IDES) Investigators: effect of an intensive exercise intervention strategy on modifiable cardiovascular risk factors in subjects with type 2 diabetes mellitus. Arch Intern Med 2010, 170: 1794–1803. 10.1001/archinternmed.2010.380
National Institute of Diabetes and Digestive and Kidney Diseases: What I Need to Know About Physical Activity and Diabetes. 2008. (accessed February 2011) http://www.diabetes.niddk.nih.gov
Nelson KM, Reiber G, Boyko EJ: Diet and exercise among adults with type 2 diabetes: findings from the Third National Health and Nutritional Examination Survey (NHANES III). Diabetes Care 2002, 25: 1722–1728. 10.2337/diacare.25.10.1722
Moratto EH, Hill JO, Wyatt HR, Ghushchyan V, Sullivan PW: Physical activity in U.S. adults with diabetes and at risk for developing diabetes. Diabetes Care 2007, 30: 203–209. 10.2337/dc06-1128
Hayes RP, Nelson DR, Meldahl ML, Curtis BH: Ability to perform daily physical activities in individuals with type 2 diabetes and moderate obesity: a preliminary validation of the Impact of Weight on Activities of Daily Living Questionnaire. Diabetes Technol Ther 2011, 13(7):705–12. 10.1089/dia.2011.0027
Curtis B, Hayes R, Fehnel S, Zografos L: Assessing the effect of weight and weight loss in obese persons with type 2 diabetes. Diabetes Metab Syndr Obes 2008, 1: 13–23.
Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB: Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med 1995, 332: 556–561. 10.1056/NEJM199503023320902
Penninx BW, Ferrucci L, Leveille SG, Rantanen T, Pahor M, Guralnik JM: Lower extremity performance in nondisabled older persons as a predictor of subsequent hospitalization. J Gerontol A Biol Sci Med Sci 2000, 55: M691-M697. 10.1093/gerona/55.11.M691
Ensrud KE, Nevitt MC, Yunis C, Cauley JA, Seeley DG, Fox KM, Cummings SR: Correlates of impaired function in older women. J Am Geriatr Soc 1994, 42: 481–489.
Ferrucci L, Guralnik JM, Pahor M, Corti MC, Havlik RJ: Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled. JAMA 1997, 277: 728–734. 10.1001/jama.1997.03540330050034
Perkowski LC, Stroup-Benham CA, Markides KS, Lichtenstein MJ, Angel RJ, Guralnik JM, Goodwin JS: Lower-extremity functioning in older Mexican Americans and its association with medical problems. J Am Geriatr Soc 1998, 46: 411–418.
Menz HB, Lord SR, St George R, Fitzpatrick RC: Walking stability and sensorimotor function in older people with diabetic peripheral neuropathy. Arch Phys Med Rehabil 2004, 85(2):245–52. Feb 10.1016/j.apmr.2003.06.015
Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang Y, Wilson PW, Kelly-Hayes M, Wolf PA, Kreger BE, Kannel WB: The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am J Public Health 1994, 84: 351–358. 10.2105/AJPH.84.3.351
Fried LP, Bandeen-Roche K, Kasper JD, Guralnik JM: Association of comorbidity with disability in older women: the Women’s Health and Aging Study. J Clin Epidemiol 1999, 52: 27–37. 10.1016/S0895-4356(98)00124-3
Mokdad AH, Ford ES, Bowman BA, Nelson DE, Engelgau MM, Vinicor F, Marks JS: Diabetes trends in the U.S.: 1990–1998. Diabetes Care 2000, 23: 1278–1283. 10.2337/diacare.23.9.1278
Lustman PJ, Anderson RJ, Freedland KE, de Groot M, Carney RM, Clouse RE: Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes Care 2000, 23: 934–942. 10.2337/diacare.23.7.934
Talbot F, Nouwen A: A review of the relationship between depression and diabetes in adults. Diabetes Care 2000, 23: 1556–1562. 10.2337/diacare.23.10.1556
Penninx BW, Guralnik JM, Ferrucci L, Simonsick EM, Deeg DJ, Wallace RB: Depressive symptoms and physical decline in community-dwelling older persons. JAMA 1998, 279: 1720–1726. 10.1001/jama.279.21.1720
Lin EH, Korff MV, Alonso J, Angermeyer MC, Anthony J, Bromet E, Bruffaerts R, Gasquet I, de Girolamo G, Gureje O, Haro JM, Karam E, Lara C, Lee S, Levinson D, Ormel JH, Posada-Villa J, Scott K, Watanabe M, Williams D: Mental disorders among persons with diabetes–results from the World Mental Health Surveys. J Psychosom Res 2008, 65(6):571–80. 10.1016/j.jpsychores.2008.06.007
Fabrega JJ: The study of disease in relation to culture. Behav Sci 1972, 17: 183–203. 10.1002/bs.3830170202
Gureje O, Ustun TB, Simon GE: The syndrome of hypochondriasis: a cross-national study in primary care. Psychol Med 1997, 27: 1001–10. 10.1017/S0033291797005345
Easterlin RA, McVey LA, Switek M, Sawangfa O, Zweig JS: The happiness-income paradox revisited. Proc Natl Acad Sci U S A 2010, 107(52):22463–8. 10.1073/pnas.1015962107
Jen MH, Sund ER, Johnston R, Jones K: Trustful societies, trustful individuals, and health: an analysis of self-rated health and social trust using the World Value Survey. Health Place 2010, 16(5):1022–9. 10.1016/j.healthplace.2010.06.008
Jen MH, Jones K, Johnston R: Global variations in health: evaluating Wilkinson's income inequality hypothesis using the World Values Survey. Soc Sci Med 2009, 68(4):643–53. 10.1016/j.socscimed.2008.11.026
Kim D, Kawachi I, Hoorn SV, Ezzati M: Is inequality at the heart of it? Cross-country associations of income inequality with cardiovascular diseases and risk factors. Soc Sci Med 2008, 66(8):1719–32. 10.1016/j.socscimed.2007.12.030
Acknowledgement
Research on Early Life and Aging Trends and Effects (RELATE) was funded by United States Department of Health and Human Services, National Institutes of Health, and National Institute on Aging (K25AG027239). This fund was used to create the RELATE dataset from existing data sources. The following individuals and Principal Investigators also deserve recognition for being instrumental in the release of the first public version of RELATE: Drs. George Alter, Barry Popkin, David Weir, Yi Zeng, Luis Rosero-Bixby, Ana Luisa Dávila, Alberto Palloni, Somnath Chatterji, Paul Kowal, Pamela Herd, and Bob Hauser. A full detail of funding sources for each of the country specific studies are available in the appendices for the RELATE data [10].
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SA designed the study and conducted data analysis, MML and RML conducted the literature review and drafted the manuscript. All authors read and approved the final manuscript.
An erratum to this article is available at http://dx.doi.org/10.1186/2251-6581-13-73.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Assari, S., Lankarani, R.M. & Lankarani, M.M. Cross-country differences in the association between diabetes and disability. J Diabetes Metab Disord 13, 3 (2014). https://doi.org/10.1186/2251-6581-13-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2251-6581-13-3