
Abstract
Background
Consensus has not been reached on safe alcohol consumption recommendations during pregnancy. The National Institutes for Care and Health Excellence (NICE) in the UK suggest that one to two drinks not more than twice per week is safe. However, the speech and language effects of even low levels of alcohol use among offspring are unknown. The aim of this study was to review systematically the evidence on studies of the effect of low to moderate levels of alcohol consumption during pregnancy (up to 70 grams of alcohol per week) compared to abstinence on speech and language outcomes in children.
Methods
Using medical subject headings, PubMed, Web of knowledge, Scopus, Embase, Cinahl and the Cochrane Library were searched from their inception up to March 2012. Case control and cohort studies were included. Two assessors independently reviewed titles, abstracts and full articles, extracted data and assessed quality.
Results
A total of 1,397 titles and abstracts were reviewed of which 51 full texts were retrieved. Three cohort studies totaling 10,642 women met the inclusion criteria. All three studies, (United States (2) and Australia (1)) indicated that language was not impaired as a result of low to moderate alcohol consumption during pregnancy. Two studies were judged to be of low quality based on a six-item bias classification tool. Due to heterogeneity, results could not be meta-analyzed.
Conclusion
Studies included in this review do not provide sufficient evidence to confirm or refute an association between low to moderate alcohol use during pregnancy and speech and language outcomes in children. High quality, population based studies are required to establish the safety of low to moderate levels of alcohol use such as those set out by the NICE guidelines in the UK.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Speech and language delays in infants and children occur when speech and language abilities are below that expected for a child’s chronological age, while still following the expected developmental sequence [1]. Speech and language development is known to be an important overall developmental milestone in children and early speech and language delays can result in poorer educational outcomes and longer term adverse cognitive and behavioral outcomes throughout the life course [2]. Although the prevalence of speech and language disorders depends on their exact classification and definition, recent studies suggest that some communication disorders may be as high as 13% in primary and secondary school children [3, 4].
Research on the predictors of late language emergence at 24 months in an Australian cohort have illustrated the complexity of the predictors of language emergence in the general population showing strong neurobiological and genetic causal mechanisms that operate across a wide variation in maternal and family characteristics [5]. Speech and language impairments are often one of the key features of neurologic damage in children with diagnoses of Fetal Alcohol Spectrum Disorders (FASD) which are as high as 5% in some regions of the United States and Europe [6–8]. However, while the impact of alcohol consumption during pregnancy on birth outcomes [9], mental development [10] and neuropsychological outcomes [11] is well investigated, the effect of alcohol consumption during pregnancy on speech and language development especially at lower or moderate levels is unknown [12].
In Denmark, the Netherlands, Australia, the United Kingdom, Ireland and the United States a number of large population-based longitudinal and cross sectional studies have estimated that between 12% and 81% of babies may be exposed to alcohol during gestation due to maternal alcohol consumption [13–20]. While most women who consume alcohol during pregnancy do so at low or moderate levels, the exact consequences of these levels of alcohol on fetal growth and development have not been established. Recent reviews have suggested that moderate drinking may not be harmful to birth weight, length of gestation or size for gestational age [9, 21]. However, evidence suggests that low to moderate alcohol use in pregnancy can still produce functional damage to the brain leading to adverse cognitive and neurological development without obviously affecting other systems such as growth [12]. Specifically, magnetic resonance imaging (MRI) studies have shown that prenatal alcohol exposure can impact on many areas of the brain involved in speech and language development, including the corpus collosum [22].
At present in Canada, the United States, Ireland and New Zealand recommendations advise complete abstinence from alcohol during pregnancy due to uncertain evidence on its effect on growth and development at lower to moderate levels [23–26]. However, the National Institute for Health and Care Excellence in the United Kingdom suggest that one to two units not more than once or twice per week is safe [27]. Establishing the impact of gestational alcohol exposure on speech and language outcomes in children is an important contribution toward understanding, both in the etiology of adverse speech and language development and in developing consistent and comprehensive clinical and government guidelines internationally around alcohol use during pregnancy.
The aim of this review was to systematically search and appraise available case control and cohort studies on the effect of low to moderate alcohol use during pregnancy compared to abstinence from alcohol during pregnancy on speech and language outcomes in children to age 18 years.
Methods
Study eligibility criteria
In line with our study protocol, studies were included if they were case control or cohort studies published any time before 1 March 2012, in the English language in a peer reviewed journal. Studies which reported data on low or moderate alcohol exposure (defined as an average of less than 10 grams per day or 70 grams per week during pregnancy) compared to not drinking during pregnancy were included. Studies which reported on any measure or component of language, speech and communication delay, development or disorder in children up to 18 years were included, for example, acquired language disorders and semantic pragmatic disorders (see Additional file 1). We excluded duplicate publications and studies published only as abstracts. Other cognitive and developmental outcomes and nonverbal language outcomes were excluded. Studies of populations with special developmental needs, such as autism spectrum disorder, were also excluded. This review was not registered with PROSPERO [28].
Search strategy
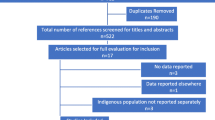
Embase, PubMed, Cinahl, SCOPUS, Web of Knowledge and The Cochrane Library were searched from their inception up until 1 March 2012 using all appropriate MESH headings related to “alcohol”, “speech and language outcomes”, “pregnancy” and “risk or odds” (see Additional file 1 for detailed search strategy: note that search strategy was not peer reviewed). Search limits of “human” and “female” were applied in PubMed only. All associated MESH terms were combined using “OR”. Finally, all terms were combined using “AND” to yield a total number of abstracts for each database. Reference lists of retrieved articles were also hand searched for further potentially relevant articles. Additionally, the authors of the cohort study by Faden and Graubard [29] were contacted for additional information on their study which was not available in the published paper. All citations were imported to Endnote citation manager and duplicates removed. Figure 1 shows a flow diagram of the results of the search strategy implemented.

Flow diagram of search strategy.
Study and data collection processes
LMOK designed and executed the search strategy (see Additional file 1) which was reviewed by PMK. Two assessors (LMOK, PMK) independently reviewed titles and abstracts of all identified citations. Both reviewers independently evaluated each full text article. Disagreements were resolved by consensus. Articles which were of uncertain relevance were obtained and the full text read. A data extraction form was designed and for the final three articles included in the review, two reviewers independently extracted data on country of origin, years of study, study design, characteristics of participants, exposure definition and ascertainment, outcomes, control for confounders and information on bias (Table 1) as well as available measures of association including odds and risk ratios (Table 2). Due to the heterogeneous nature of the exposure and outcomes across the three studies included in the review, it was not deemed appropriate to conduct a meta-analysis.
Quality assessment
The quality of included studies was assessed by evaluating six types of bias to include a rapid assessment of selection, exposure, outcome, confounding, analytical and attrition biases (Table 3) developed by McDonald and colleagues [32] (see Additional file 2). In line with these pre-specified definitions of bias, selection bias was deemed ‘minimal’ if studies reported sampling from a general population of pregnant women rather than a select group. Exposure and outcome assessment were ‘minimal’ if obtained from direct questioning of the mother on the exposure or by using a clearly validated instrument for measuring speech and language outcomes. Confounding bias was assessed as ‘high’ if no confounders were matched or controlled for and ‘minimal’ if at least basic demographic and other key confounders, such as the home environment and parenting variables, were addressed. Analytic bias was deemed ‘moderate’ if no sample size calculation was reported and only a subsample studied, and ‘high’ if inappropriate analyses were undertaken such as multiple unspecified a priori or inappropriate subgroup analyses. Attrition was ‘high’ if >20% were lost to follow-up without explanation of the causes.
Results
Search results
Overall, 1,397 abstracts were identified of which 387 duplicates were removed (Figure 1). Of the 1,010 articles remaining, 45 full text articles were retrieved. A further six citations were identified through hand searching of full texts leading to a total of 51 studies to undergo full review. Both assessors (LMOK, PMK) independently reviewed all 51 full texts in accordance with inclusion and exclusion criteria and disagreements were settled by consensus. The main reasons for exclusion were lack of reporting on the exposure and outcome of interest and exclusion due to study of alcohol in populations with other developmental disorders such as autism spectrum disorder. Three cohort studies were included, totaling 10,642 women. A summary of the study characteristics and results is shown in Tables 1 and 2.
Description of included studies
Two studies were from the United States and one study was from Australia. One study collected data on alcohol exposure during pregnancy through direct face to face interviews [31] while the remaining two studies collected exposure status after pregnancy through a postal survey [29, 30]. O’Leary et al. [30] collected data on dose, pattern and timing of exposure for the three months before pregnancy and each trimester separately approximately 12 weeks after delivery. Faden and Graubard [29] collected data on mean alcohol drinks per day during pregnancy through a postal survey after pregnancy, while Greene et al. [31] collected data on the average number of ounces of alcohol per day reported to have been consumed over all sampled days throughout pregnancy by a face to face interview during pregnancy. All three studies used different validated instruments to measure language delay including the parent reported Ages and Stages Questionnaire [30], a parent reported seven-item Language Scale from the Denver Developmental Scale [29] and the Sequenced Inventory of Communication Development (SICD) at one, two and three years [31], a standardized procedure directly administered in the home of the child to diagnose developmental delay in the acquisition and use of language. Only two of the three studies (O’Leary et al. [30] and Greene et al. [31]) controlled for relevant confounders in their analyses and effect measures were also significantly heterogeneous. O’Leary et al. [30] reported crude and adjusted odds ratios while estimates by Faden and Graubard [29] reported mean number of drinks per day for each level of the seven-item Language Scale used. Greene et al. [31] reported mean SICD measures for selected levels of absolute alcohol per day at one, two and three years for expressive and receptive language outcomes.
Systematic review results
Table 3 describes the results of included studies. O’Leary et al. [30], retrospective cohort in 1,759 largely married, educated and non-indigenous Australian women, defined low alcohol consumption during pregnancy as 20 g or less per occasion or less than weekly. For low drinking in the first trimester, the odds of language delay were 0.97 (95% confidence interval (CI) 0.65 to 1.43) indicating that low drinkers were 3% less likely to have children with language delay compared to abstinent mothers though the results were not statistically significant as indicated by the wide confidence intervals that span the null value (odds ratio of 1). For low drinking in the second trimester the odds of language delay were 0.87 (95% CI 0.59 to 1.28) and for the third trimester, 0.84 (95% CI 0.57 to 1.23) which also indicated slightly reduced odds of language delay in low drinkers (13% and 16%, respectively) that were not statistically significant as indicated by the confidence intervals spanning the null value. Estimates were adjusted for a range of confounders, including maternal age, parity, marital status, smoking for each trimester, illicit drug use, depression, anxiety and stress, family factors (antenatal income, presence of partner in household, parenting ability, family functioning).
Faden and Graubard [29] retrospective cohort study of 8,885 women reported to have been sampled representatively from the national birth certificate in the United States but did not report socio-demographic and health characteristics of participants. The response rate upon first recruitment to the study was 74% with 83% of the original cohort completing the three-year follow-up. Stratified sampling by both ethnicity and birth weight was conducted. A seven-item language scale was used to measure language development. Potential scores on the scale ranged from 1 to 7 with a lower score indicating lower levels of language development. Mean alcoholic drinks per day during pregnancy were reported for each level of the seven-item language scale. Covariates were not adjusted for and the results reported did not show any dose–response relationship between lower levels of language development and mean number of drinks per day.
The prospective cohort study of 359 mother-infant pairs by Greene et al. 1990 [31] in women attending a hospital for antenatal care comprised over 50% black with a mean age of 22 and with over 30% reporting use of marijuana during pregnancy. Women who delivered small for gestational age infants or whose infants were admitted to neonatal intensive care were excluded from the study. This group was also socio-economically disadvantaged. The results were reported in mean SICD measures for selected levels of absolute alcohol per day and were adjusted for sex, race, parental education, maternal age, reported usage of street drugs, the day of first antenatal visit, the Home Observation for the Measurement of the Environment (HOME) score, the precise age at testing, the ratings of psychosocial stress, medical problems and maternal IQ. Significant differences in expressive and receptive language development at one, two and three years were not evident for all three measures of alcohol use obtained, including abstinence, one-third of a UK standard drink per day, greater than one-third to one and a half UK standard drinks per day or approximately two UK standard drinks per day.
Quality assessment
The results of the quality assessment undertaken are shown in Table 3. Attrition bias was present in all three studies and may have significantly impacted results. In addition, selection, confounding and analytic bias were also present. In the study by Greene et al. 1990 [31], selection bias was deemed to be ‘moderate’ due to ambiguous sample selection but ‘minimal’ in both other studies. Confounding bias was deemed to be ‘high’ in Faden and Graubard [29] due to lack of control for confounders but ‘minimal’ in both other studies while analytic bias, though present in both Faden and Graubard [29] and Greene et al. [31], was relatively low.
Discussion
In this systematic review we sought to determine the effect of low to moderate alcohol exposure during pregnancy on speech and language outcomes in children. Poorer language development was not observed in infants exposed to low or moderate alcohol levels [30, 31] or was not associated with mean number of drinks per day [29]. However, studies were methodologically heterogeneous and two studies (Faden and Graubard [29] and Greene et al. [31]) had a number of limitations including confounding, attrition and selection biases which reduce their validity. Although our search is now 18 months old, due to the low number of articles yielded in our original search of six large international health databases since their inception, we believe our review retains its validity, importance and timeliness.
The method of exposure ascertainment has an impact on the accuracy and validity of reporting of exposure and subsequently the direction of the associations detected. In the studies included in this review, two studies used retrospective ascertainment of exposure while one used concurrent collection. Retrospective data collection used by Faden and Graubard [29] and O’Leary et al. [30] is suggested to be subject to higher risk of recall bias and differential misclassification of exposure status whereas concurrent data used by Greene et al. [31] are shown to yield more valid information when examining neurodevelopmental outcomes [33]. Alternately, self-administered questionnaires used by both O’Leary et al. [30] and Faden and Graubard [29] have been shown to obtain more truthful responses in relation to socially undesirable behaviors, such as alcohol use during pregnancy, than face to face interviews which were employed by Greene and colleagues [34]. In relation to outcome measurement, three different standardized, validated measurement tools were used which cover different domains or aspects of language development and at different ages in three ethnically and culturally diverse populations. Consequently, the presence of adverse effects on speech and language outcomes in children exposed to low to moderate alcohol levels in pregnancy remains difficult to determine from the evidence included in this review due to their heterogeneous populations and exposure and outcome ascertainment.
The presence of attrition and selection bias is likely to have biased reported results toward the null in all studies and explain the lack of a reported association between moderate alcohol use in pregnancy and language delay. In the Australian cohort [30], only 85% of women who agreed to participate originally did so at year two when language outcome was being measured. However, this study had many other strengths and a low level of bias which may have counteracted this effect. Similarly, of the 74% who originally responded to the survey in the cohort studied by Faden and Graubard [29], only 83% completed the three-year follow-up. As participation may be associated with alcohol status and child neurodevelopmental functioning, an apparent association could be masked if children with speech and language problems were systematically lost to follow-up in these studies [35]. For Greene et al. [31] selection bias may have also influenced the reported findings. In particular, children with a gestational age under 37 weeks or with admission to neonatal intensive care were excluded from the study. This may have led to the exclusion of children who had a higher risk of language delay or a different pattern of alcohol exposure to other participants.
Implications for practice
MRI studies have shown that prenatal alcohol exposure can impact upon a number of regions of the brain involved in verbal communication development, such as the corpus collosum, by displacing it, producing shape variability or reducing volume, area and length [22]. Though a lack of association between moderate alcohol use during pregnancy and speech and language development in infants is not implausible, given the low number of studies conducted, the inherent problems of accurate alcohol measurement during pregnancy and lack of biological plausibility with pathophysiological evidence, further research is required. In particular, future studies which more robustly assess the impact of alcohol use on speech and language outcomes due to the likely impact of attrition, selection and confounding biases are required. Losses to follow-up were considerable threats to validity in studies reviewed. Efforts to account for both participation bias which occurs upon recruitment to studies and attrition bias occurring later in the study should be incorporated in future studies of this nature. The complex nature of the development of speech and language delays including the interaction of environmental, neurodevelopmental and familial factors [5] as well as the underlying cultural and ethnic differences that may result in varying attitudes, practices and norms relating to alcohol and speech and language outcomes must be addressed [16]. Consequently, until, large scale, population-based, longitudinal studies of gestational alcohol use and speech and language outcomes emerge, healthcare providers should advise women to abstain from consuming alcohol during pregnancy while policy makers should remain aware of limited research evidencing safe alcohol consumption thresholds during pregnancy.
Conclusions
International guidelines have not reached consensus on safe alcohol recommendations for pregnant women. The findings of this review reveal the dearth of research on the effect of low to moderate gestational alcohol use and speech and language outcomes in children. Future research should carefully address the validity and accuracy of exposure and outcome ascertainment and pay particular attention to reducing the risk of selection, attrition and confounding biases. Healthcare providers should continue to advice abstinence from alcohol during pregnancy until further evidence on the effect of low-moderate gestational alcohol use becomes available. Policy makers should remain aware of limited research showing the safety of alcohol use in pregnancy in relation to childhood development such as speech and language outcomes.
Authors’ information
Linda Marie O’Keeffe is a PhD candidate at University College Cork, Ireland. Her PhD thesis focuses on examining the growth and cognitive impact of alcohol use during pregnancy. This topic is important and timely because significant controversy exists around the safety of low levels of alcohol consumption during pregnancy. Secondly, the prevalence of alcohol use during pregnancy remains high in many Western European countries, such as Ireland (in excess of 50%), despite the absence of a threshold below which harm to the fetus does not occur. Conducting systematic reviews of the effect of low levels of alcohol use on cognitive and developmental outcomes in childhood is an important part of assessing comprehensively fetal alcohol effects beyond birth.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- NICE:
-
National Institutes for Health and Care Excellence
- NR:
-
Not reported
- SICD:
-
Sequenced Inventory of Communication Development
- HOME:
-
Home Observation for Measurement of the Environment.
References
Law J, Boyle J, Harris F, Harkness A: Screening for speech and language delay: a systematic review of the literature. Health Technol Assess. 1998, 2: 1-184.
Nelson HD, Nygren P, Walker M, Panoscha R: Screening for speech and language delay in preschool children: systematic evidence review for the US preventive services task force. Pediatrics. 2006, 117: e298-e319. 10.1542/peds.2005-1467.
McLeod S, Harrison LJ: Epidemiology of speech and language impairment in a nationally representative sample of 4- to 5-year-old children. J Speech Lang Hear Res. 2009, 52: 1213-10.1044/1092-4388(2009/08-0085).
McLeod S, McKinnon DH: Prevalence of communication disorders compared with other learning needs in 14,500 primary and secondary school students. Int J Lang Commun Disord. 2007, 42 (Suppl 1): 37-59.
Hawkins SS, Stern AD, Gillman MW: Do state breastfeeding laws in the USA promote breast feeding?. J Epidemiol Community Health. 2013, 67: 250-256. 10.1136/jech-2012-201619.
Mattson SN, Crocker N, Nguyen TT: Fetal alcohol spectrum disorders: neuropsychological and behavioral features. Neuropsychol Rev. 2011, 21: 81-101. 10.1007/s11065-011-9167-9.
May PA, Gossage JP, Kalberg WO, Robinson LK, Buckley D, Manning M, Hoyme HE: Prevalence and epidemiologic characteristics of FASD from various research methods with an emphasis on recent in-school studies. Dev Disabil Res Rev. 2009, 15: 176-192. 10.1002/ddrr.68.
May PA, Fiorentino D, Phillip Gossage J, Kalberg WO, Eugene Hoyme H, Robinson LK, Coriale G, Jones KL, del Campo M, Tarani L, Romeo M, Kodituwakku PW, Deiana L, Buckley D, Ceccanti M: Epidemiology of FASD in a province in Italy: prevalence and characteristics of children in a random sample of schools. Alcohol Clin Exp Res. 2006, 30: 1562-1575. 10.1111/j.1530-0277.2006.00188.x.
Patra J, Bakker R, Irving H, Jaddoe VW, Malini S, Rehm J: Dose–response relationship between alcohol consumption before and during pregnancy and the risks of low birthweight, preterm birth and small for gestational age (SGA)-a systematic review and meta-analyses. BJOG. 2011, 118: 1411-1421. 10.1111/j.1471-0528.2011.03050.x.
Testa M, Quigley BM, Das Eiden R: The effects of prenatal alcohol exposure on infant mental development: a meta-analytical review. Alcohol Alcohol. 2003, 38: 295-304. 10.1093/alcalc/agg087.
Flak AL, Su S, Bertrand J, Denny CH, Kesmodel US, Cogswell ME: The association of mild, moderate, and binge prenatal alcohol exposure and child neuropsychological outcomes: a meta‒analysis. Alcohol Clin Exp Res. 2013, Epub ahead of print
Gray R, Mukherjee RAS, Rutter M: Alcohol consumption during pregnancy and its effects on neurodevelopment: what is known and what remains uncertain. Addiction. 2009, 104: 1270-1273. 10.1111/j.1360-0443.2008.02441.x.
Colvin L, Payne J, Parsons D, Kurinczuk JJ, Bower C: Alcohol consumption during pregnancy in nonindigenous west Australian women. Alcohol Clin Exp Res. 2007, 31: 276-284. 10.1111/j.1530-0277.2006.00303.x.
Kelly Y, Sacker A, Gray R, Kelly J, Wolke D, Quigley MA: Light drinking in pregnancy, a risk for behavioural problems and cognitive deficits at 3 years of age?. Int J Epidemiol. 2009, 38: 129-140. 10.1093/ije/dyn230.
Bakker R, Pluimgraaff LE, Steegers EA, Raat H, Tiemeier H, Hofman A, Jaddoe VW: Associations of light and moderate maternal alcohol consumption with fetal growth characteristics in different periods of pregnancy: the Generation R Study. Int J Epidemiol. 2010, 39: 777-789. 10.1093/ije/dyq047.
Andersen AM, Andersen PK, Olsen J, Grønbæk M, Strandberg-Larsen K: Moderate alcohol intake during pregnancy and risk of fetal death. Int J Epidemiol. 2012, 41: 405-413. 10.1093/ije/dyr189.
Mullally A, Cleary BJ, Barry J, Fahey TP, Murphy DJ: Prevalence, predictors and perinatal outcomes of peri-conceptional alcohol exposure - retrospective cohort study in an urban obstetric population in Ireland. BMC Pregnancy Childbirth. 2011, 11: 27-10.1186/1471-2393-11-27.
Royal College of Obstetricians and Gynecologists: Alcohol consumption and the outcomes of pregnancy (RCOG Statement No 5). 2006,http://www.rcog.org.uk/womens-health/clinical-guidance/alcohol-consumption-and-outcomes-pregnancy,
McCarthy FP, O'Keeffe LM, Khashan AS, North RA, Poston L, McCowan LM, Baker PN, Dekker GA, Roberts CT, Walker JT: Association between maternal alcohol consumption in early pregnancy and pregnancy outcomes. Obstet Gynecol. 2013, 122: 830-837. 10.1097/AOG.0b013e3182a6b226.
O'Keeffe LM, Kearney PK, Greene RA: Surveillance during pregnancy: methods and response rates to a hospital based cross sectional study of the pregnancy risk assessment monitoring system in Ireland. BMC Pregnancy Childbirth. 2013, 13: 180-10.1186/1471-2393-13-180.
Henderson J, Gray R, Brocklehurst P: Systematic review of effects of low–moderate prenatal alcohol exposure on pregnancy outcome. BJOG. 2007, 114: 243-252. 10.1111/j.1471-0528.2006.01163.x.
Lebel C, Roussotte F, Sowell ER: Imaging the impact of prenatal alcohol exposure on the structure of the developing human brain. Neuropsychol Rev. 2011, 21: 102-118. 10.1007/s11065-011-9163-0.
Butt P, Beirness D, Gliksman L: Alcohol and Health in Canada: A summary of Evidence and Guidelines for Low Risk Drinking. 2011, Ottawa: Canadian Centre on Substance Abuse
Health Services Executive: Alcohol and Pregnancy.http://www.yourdrinking.ie/alcohol-and-pregnancy,
Ministry of Health: Alcohol and Pregnancy: A Practical Guide for Health Professionals. 2010, Wellington: Ministry of Health
U.S. Department of Health and Human Services: U.S. surgeon general releases advisory on alcohol use in pregnancy. [http://www.surgeongeneral.gov/news/2005/02/sg02222005.html]
National Institute for Care and Clinical Excellence (NICE): Antenatal Care: Routine Care for Healthy Pregnant Women: NICE Clinical Guidelines 62. 2008
PROSPERO: International prospective register of systematic reviews.http://www.crd.york.ac.uk/prospero/,
Faden VB, Graubard BI: Maternal substance use during pregnancy and developmental outcome at age three. J Subst Abuse. 2000, 12: 329-340. 10.1016/S0899-3289(01)00052-9.
O'Leary C, Zubrick SR, Taylor CL, Dixon G, Bower C: Prenatal alcohol exposure and language delay in 2-year-old children: the importance of dose and timing on risk. Pediatrics. 2009, 123: 547-554. 10.1542/peds.2008-0459.
Greene T, Ernhart CB, Martier S, Sokol R, Ager J: Prenatal alcohol exposure and language development. Alcohol Clin Exp Res. 1990, 14: 937-945. 10.1111/j.1530-0277.1990.tb01842.x.
McDonald SD, Han Z, Mulla S, Murphy KE, Beyene J, Ohlsson A: Preterm birth and low birth weight among in vitro fertilization singletons: a systematic review and meta-analyses. Eur J Obstet Gynecol Reprod Biol. 2009, 146: 138-10.1016/j.ejogrb.2009.05.035.
Jacobson SW, Chiodo LM, Sokol RJ, Jacobson JL: Validity of maternal report of prenatal alcohol, cocaine, and smoking in relation to neurobehavioral outcome. Pediatrics. 2002, 109: 815-10.1542/peds.109.5.815.
Bloomfield K, Hope A, Kraus L: A review of alcohol survey methodology: towards a standardised measurement instrument for Europe. Drug: Educ, Prev, Policy. 2011,http://www.alcsmart.ipin.edu.pl/files/prop_01.pdf,
Kesmodel U, Bertrand J, Støvring H, Skarpness B, Denny C, Mortensen E: The effect of different alcohol drinking patterns in early to mid pregnancy on the child’s intelligence, attention, and executive function. BJOG. 2012, 119: 1180-1190. 10.1111/j.1471-0528.2012.03393.x.
Acknowledgements
This work was funded by the HRB in Ireland under Grant No. PHD/2007/16 and conducted as part of module PG7016 at University College Cork, Ireland.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors have no conflicts of interest to disclose.
Authors’ contributions
LMO’K conceptualized and designed the study, devised and conducted the search strategy, drafted the initial manuscript, and approved the final manuscript as submitted. RAG contributed to the concept and design of the study, reviewed and revised the manuscript, and approved the final manuscript as submitted. PMK supervised the methods, critically reviewed the manuscript, and approved the final manuscript as submitted. All authors read and approved the final manuscript.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
O’Keeffe, L.M., Greene, R.A. & Kearney, P.M. The effect of moderate gestational alcohol consumption during pregnancy on speech and language outcomes in children: a systematic review. Syst Rev 3, 1 (2014). https://doi.org/10.1186/2046-4053-3-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2046-4053-3-1