
Abstract
Background
Questionnaire-based studies suggest atypical sensory perception in over 90% of individuals with autism spectrum conditions (ASC). Sensory questionnaire-based studies in ASC mainly record parental reports of their child’s sensory experience; less is known about sensory reactivity in adults with ASC. Given the DSM-5 criteria for ASC now include sensory reactivity, there is a need for an adult questionnaire investigating basic sensory functioning. We aimed to develop and validate the Sensory Perception Quotient (SPQ), which assesses basic sensory hyper- and hyposensitivity across all five modalities.
Methods
A total of 359 adults with (n = 196) and without (n = 163) ASC were asked to fill in the SPQ, the Sensory Over-Responsivity Inventory (SensOR) and the Autism-Spectrum Quotient (AQ) online.
Results
Adults with ASC reported more sensory hypersensitivity on the SPQ compared to controls (P < .001). SPQ scores were correlated with AQ scores both across groups (r = .-38) and within the ASC (r = -.18) and control groups (r = -.15). Principal component analyses conducted separately in both groups indicated that one factor comprising 35 items consistently assesses sensory hypersensitivity. The SPQ showed high internal consistency for both the total SPQ (Cronbach’s alpha = .92) and the reduced 35-item version (alpha = .93). The SPQ was significantly correlated with the SensOR across groups (r = -.46) and within the ASC (r = -.49) and control group (r = -.21).
Conclusions
The SPQ shows good internal consistency and concurrent validity and differentiates between adults with and without ASC. Adults with ASC report more sensitivity to sensory stimuli on the SPQ. Finally, greater sensory sensitivity is associated with more autistic traits. The SPQ provides a new tool to measure individual differences on this dimension.
Similar content being viewed by others


Background
In addition to the classic diagnostic criteria (social and communication difficulties alongside unusually narrow interests and repetitive behaviour) [1] atypical sensory reactivity is now also recognized as being at the core of autism spectrum conditions (ASC) [2, 3]. Under Symptom B the new autism criteria for DSM-5 include ‘Hyper- or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment (for example, apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement.’ [4]. The study of atypical sensory reactivity in individuals with autism is important given how common this is in ASC. Questionnaires are widely used to study sensory reactivity issues in children with and without ASC [5], in Sensory Processing Disorder [6] and other conditions [7]. Sensory questionnaire studies in ASC mainly record parental reports of their child’s sensory experience [5, 8–16]. Although parent reports are an important tool, self-report is also crucial, as sensory experiences are by definition subjective. Only a few questionnaire studies have investigated sensory reactivity issues in adults with ASC [17, 18].
The most widely used measure for adults with ASC is the Adolescent/Adult Sensory Profile (AASP), a 60-item self-report measure that finds differences in sensory processing in more than 90% of adults with ASC [17, 19]. There have been several studies using the AASP in ASC; one of them found that older individuals with ASC are more similar to control groups than are younger individuals [20]. In addition, adults with schizophrenia and bipolar disorder also show differences on the AASP compared to controls [21]. The AASP is a useful tool because it can be used in clinical settings and describes the particular sensory problems of an individual by assessing specific sensory types, such as sensory sensation seeking.
However, items on the AASP include questions about other factors that may influence our sensory experiences. For example, there are items about visual attention (for example, ‘I miss the street, building, or room signs when trying to go somewhere new’), and affective reactions towards sensory stimuli (for example, ‘I become frustrated when trying to find something in a crowded drawer’). As such, the AASP, while producing clear group differences, measures a broader set of perceptual processes and affective responses and not basic sensory function. Thus, there is a need for a more fine-grained questionnaire to dissect each perceptual process with greater precision.
More recently the Sensory Over-responsivity Scale (SensOR) was developed to assess sensory processing disorder (SPD), or more narrowly sensory over-responsivity [6]. Sensory Over-Responsivity (SOR) is defined as an exaggerated response to one or more types of sensory stimuli [6]. The SensOR measures SOR by asking how many sensations are experienced as aversive (for example, labels in clothes). The SensOR was developed in combination with an examiner-administered assessment of response to real-world stimuli; these two measures correlate moderately (r = .47) [6]. This association suggests that the SensOR is a valid and reliable tool to investigate sensory issues. However, like the Sensory Profile, items on the SensOR include affective reactions towards sensory stimuli (for example, participants have to rate which items in the environment bother them), so again, it is not measuring basic sensory sensitivity.
There is thus a need for a basic sensory perception questionnaire that does not assess social and affective aspects. In contrast to the SensOR and the Adult Sensory Profile, the Sensory Perception Quotient (SPQ), reported here for the first time, only investigates basic sensory sensitivity, with no reference to affective response (see Table 1). The SPQ was developed to quantify individual differences in sensory perception in the general population and adults with ASC, based on the assumption that this trait shows variance following a normal distribution in community samples. All five of the main sensory modalities (vision, hearing, touch, smell and taste) were included.
The purpose behind development of the SPQ is to assist researchers studying sensory perception in adults. Additionally, the SPQ is intended to be useful for occupational therapists and other clinicians. In summary, the objectives of the current study were: (1) to explore the factor structure of the new SPQ, its reliability and its concurrent validity with a previously validated instrument; (2) to investigate if adults with and without ASC show differences on the SPQ; and (3) to explore if sensory sensitivity is correlated with autistic traits, both across and within groups.
Methods
The Cambridge University Psychology Research Ethics Committee approved the study.
Participants
Adults with ASC were recruited via an online volunteer database hosted by the Autism Research Centre, University of Cambridge. These volunteers were invited to take part in the online questionnaire study via the website at http://www.autismresearchcentre.com. Data from participants with no ASC diagnosis were collected via a parallel website at http://www.cambridgepsychology.com. Only participants who reported to have no psychiatric history were included in the control group.
All participants first filled in background information including age, sex, and history of psychiatric conditions including when, where and by whom they were diagnosed. Only participants with an ASC diagnosis made by a qualified professional (psychologist or psychiatrist) were included in the ASC group. To validate diagnoses in the ASC group and to screen control participants, we used the Autism Spectrum Quotient (AQ) [22]. We used a standard inclusion criterion of an AQ cut-off score of 26 and above for the ASC group, and a score below 26 for the control group [22, 23]. Nine participants with ASC and 43 control participants were excluded on the basis of the AQ cut-off score, leaving 359 participants: n = 196 participants with ASC (100 males, 96 females) and n = 163 control participants (49 males, 114 females). Participants were not reimbursed for taking part in the current study.
Autism Spectrum Quotient
All participants completed the adult version of the AQ. The AQ is a short, 50-item questionnaire measuring autistic traits, with five subscales (social skills, attention switching, attention to detail, imagination and communication) [22, 23]. A score of 0 is assigned to the responses ‘definitely agree’ and ‘slightly agree’ and a score of 1 for ‘slightly disagree’ and ‘definitely disagree’ for half the items, and the reverse for the other half, designed to avoid a response bias. Total scores could therefore range from 0 to 50, with higher scores indicating more autistic traits. Results from the AQ have been replicated cross culturally [24, 25] and across different ages [26]. The AQ shows also good test-retest reliability [22–24].
Raven’s Progressive Matrices Test
IQ was estimated using a short online adaptation of the Raven’s Progressive Matrices (60 items) as a timed performance task [27]. The Raven’s Progressive Matrices Test has the advantage of being language-free and it can be used for a wide range of ages and cross-culturally (Raven, 2000). Each item consisted of a pattern consisting of a missing section, and the participant is asked to select the option that accurately completes the pattern shown (with 15 seconds allowed for each item).
Sensory over-responsivity scale
The SensOR Scale consists of a self-report inventory that measures over-responsivity in several sensory domains (touch, vision, hearing, smell, taste, and proprioception) [6]. Participants indicated which items in their daily environment bother them (for example, in the tactile domain: labels in clothing, or in the auditory domain: a clock ticking). The SensOR went through item analysis and reduction prior to item selection for this edition. The current SensOR edition consists of 76 items (28 tactile items, 20 auditory items, 9 taste items, 9 movement items, 5 vision and 5 smell items). The internal consistency reliability for the total test is high (r = .97) and concurrent validity of the SensOR score with the Sensory Profile score for sensory reactivity and sensory avoiding is moderate (r = .50) [6].
Sensory Perception Quotient (SPQ): Instrument development
We first generated items for vision, hearing, touch, smell and taste. Next, these items were given to experts in ASC and participants with and without ASC for feedback on wording and applicability. Words with affective aspects (such as like/dislike) were avoided. Instead we focused on basic detection and/or discrimination abilities (for example, ‘I would be able to detect if a strawberry was ripe or not by smell alone’). In addition we checked that where possible, items were worded appropriately given that adults with ASC prefer very specific, clear, unambiguous wording (for example, ‘I would notice if someone added 5 grains of salt to my water’). Half the items were worded to identify hypersensitive (that is, low thresholds) and half were worded to identify hyposensitive items (that is, high thresholds), to avoid bias (see Table 2 for a complete item breakdown). When scoring, hyposensitive items were reversed, so that a low total SPQ score indicates more reactivity.
The final version of the SPQ covered items for vision, hearing, touch, smell and taste. We aimed to investigate basic sensory processing and therefore included main receptors for each modality and/or the characteristics of the environment relevant to each sense (see Table 2). We developed questions about receptors from different modalities and corresponding environmental stimuli (for example, Pacinian corpuscles are tactile receptors, which are sensitive to vibrations). The only exception was olfaction since there are too many receptors to develop items for each one [28]. Instead, the main functions of olfaction were included. Equal weightings were assigned to vision, hearing and touch, on the basis that none of the senses is more important than others. However we included slightly fewer items for taste and smell since humans do not tend to depend on chemical senses as much as other animals [28]. Humans are microsmatic, having a poor sense of smell, whereas many animals are macrosmatic, having a good sense of smell [28]. Finally, we included a larger number of items in total, so as to be able to reduce these after an item analysis.
Scoring
Participants were asked to indicate to what extent they agreed or disagreed with each statement on a Likert scale (0 = strongly agree, 1 = agree, 2 = disagree, and 3 = strongly disagree). All item responses were summed [29], with a lower score indicating higher sensory sensitivity. Advantages of this scale are that it avoids uncertain answers, and it can be used for multidimensional constructs.
Procedure
Participants could complete the Raven’s Progressive Matrices, AQ, SensOR and SPQ tasks online in their preferred order, and were allowed to log out between tests.
Results
Descriptive statistics
PASW Statistics 18 was used to analyse the data. Tests of normality (Kolmogorov-Smirnov test; KS) showed that that SPQ scores were normally distributed (P > .20). There was no significant difference between the groups on age or IQ (P > .05). However as expected, the ASC group had a higher mean AQ score than the control group (t = 42.95, P < .0001) (see Table 3).
Principal component analysis
To investigate the underlying factor structure of the SPQ a principal component analysis (PCA) was conducted, using the Varimax rotation method. The PCA was first run for the data from the control participants, and subsequently repeated in the ASC group. Extraction of underlying dimensions was based on inspection of the scree plots, which suggested that the SPQ is composed of two underlying dimensions in both the control group and the ASC group.
Next, factor loadings were visually inspected. For the control group, most items (38 in total) loaded on Factor 1, whilst only a few items loaded on Factor 2. Items were retained if they showed a high factor loading (≥.35) on the one factor and a low loading (≤.35) on the other. We excluded ambiguous items that showed high loadings ≥ .35 on both factors [30]. A separate PCA for the ASC group showed similar results. In this group, 43 items loaded highly on Factor 1. In addition, 35 items that loaded on Factor 1 in the control group also loaded on Factor 1 in the ASC group (see Table 4). For Factor 2, the loadings across both groups were low and inconsistent. These results suggest that one factor, encompassing 35 items, consistently assesses sensory reactivity traits in both adults with ASC and controls.
Item distribution analysis
In addition, an item distribution analysis was conducted. Items on which more than 70% of the participants gave the same response were excluded, since items with very little variance are not informative [31]. Four such items were identified: item, 8, 16, 47 and 54. On these items most participants ‘strongly agreed’ (scoring 0). None of these items loaded on Factor 1.
Item reduction
In sum, the PCAs suggest that one factor including 35 items consistently assesses traits related to sensory reactivity in both a control group and a clinical group (see Table 4). All these 35 items show considerable response variation. Out of the 35 items loading onto Factor 1, 10 items assessed reactivity to touch, 10 items assessed smell, 6 vision, 5 hearing, and 4 taste. Most of the items (31 out of 35) were hypersensitive items.
Reliability
For all 92 items, the split-half reliability was high (Spearman-Brown = .91, P < .0001). Additionally, Cronbach’s alpha suggested excellent internal consistency for both the full 92 item version of the SPQ (α = .92) and for the reduced 35-item version (α = .93).
Concurrent validity
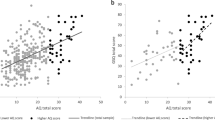
To test the concurrent validity of the SPQ the association with the SensOR was examined. High scores on the SensOR and low scores on the SPQ represent more reactivity to stimuli in the environment. The total SPQ and SensOR correlated moderately (r = -.50, P < .0001) both across groups and within the ASC (r = -.49, P = .007) and control group (r = -.23, P = .004) (see Figure 1). The concurrent validity was lower for the item reduced version of the SPQ (r = -.20, P = .0001).

The correlation between the Sensory Perception Quotient (SPQ) with the sensory over-responsivity (SensOR). The lower the score on the SPQ the more sensitive a person is, and the higher the score on the SensOR the more sensitive. ASC, autism spectrum conditions.
Differences between the groups
A MANOVA with group and sex as fixed factors showed that groups differed significantly on the SPQ total scores (F(6,339) = 13.44, P < .0001) (see Table 5). Post hoc tests showed that groups differed significantly on the total SPQ, the item-reduced version, and for all subscales other than smell. Additionally, sex differences were found for the total SPQ (F (1) = 4.71, P < .005), and for smell and taste reactivity; females in both groups had lower scores on the SPQ (more sensitive) (see Table 5). Gender had however no effect on SPQ-short scores. Results from the SenSOR are reported elsewhere [32].
Correlation between Sensory Perception Quotient and autistic traits
The total SPQ was correlated with the AQ across groups (r = -.38, P = .0001) and within the ASC group (r = -.18, P = .009), and marginally within the control group (r = -.15, P = .06). A higher score on the AQ corresponds with more autistic traits, while lower scores on the SPQ suggest a lower sensory threshold and thus a higher sensory sensitivity. The reduced SPQ also correlated with the AQ (r = -.14, P = .007). There was no correlation between SPQ total scores and age (P = .58) or IQ (P = .95).
Discussion
The current study reports the development and validation of the Sensory Perception Quotient (SPQ), a new sensory questionnaire that provides a quantitative measurement of individual differences in basic sensory perception. The SPQ shows excellent internal consistency and good validity. Adults with ASC reported being more sensitive than control participants to sensory stimuli in vision, hearing, touch and taste, but not smell. Reliable sensory sensitivity measures for adults with ASC are needed since sensory symptoms are now recognized as being at the core of ASC. Past questionnaire-based studies already highlighted the importance of sensory reactivity in ASC, but often used parent reports [5, 8–16]. Since it is easier to judge your own sensory experiences the SPQ is an important new self-report questionnaire. This new questionnaire also adds to a battery of new dimensional measures (the Autism Spectrum Quotient (AQ), the Empathy Quotient (EQ) and the Systemizing Quotient (SQ)) that seek to provide a metric of the spectrum on which ASC lies, and the relationship between ASC and variation in the general population [22, 33, 34].
With regards to item analysis, principal component analyses suggest that one factor including 35 items consistently assesses traits related to sensory sensitivity, in both the clinical group and the control group. Both the short 35-item version and the total 92-item version of the SPQ showed high internal consistency. In addition the SPQ correlated with the AQ, meaning greater sensory reactivity is associated with more autistic traits. Furthermore the SPQ was moderately correlated to a validated sensory scale, the SensOR. It is not surprising that the SPQ and SensOR are not perfectly related, as the SensOR also assesses the affective response to sensory stimuli, whilst the SPQ focuses on basic sensory perception only. Future studies need to test whether SPQ scores correlate to laboratory-measured reactivity measures. In addition, future studies are needed to investigate other test characteristics, such as test-retest reliability.
A limitation of this study is the uneven sex ratio between the groups (more females in the control group). However the ASC and control group differed on the SPQ even when sex was included as a factor. Sex had an effect on the full SPQ, in line with findings from the Sensory Profile [35]. Females in both groups have lower scores on the SPQ, meaning women report being more sensitive. Since females with ASC reported they were more sensitive, the question arises if sensory issues affect females with ASC to a greater extent. A recent study shows that women with ASC report more life-time sensory issues compared to men with ASC [36]. This is important and needs more research since most studies neglect female participants with ASC and mostly include males. Finally, given that this is the first report of the SPQ, future studies are necessary to generate a normative dataset.
Conclusions
The SPQ is a reliable and valid new tool to measure sensory sensitivity in adults with and without ASC. Adults with ASC report more sensory sensitivity than controls, and this may have important implications for how they manage their everyday lives. The SPQ is a useful standardized measure for basic sensory perception in adults with ASC, other clinical disorder and neurotypical adults. Uses of the SPQ include assisting researchers studying sensory issues in adults (for example, in phenotyping studies), and to assist clinicians, such as occupational therapists, in assessing the sensory needs of people with autism.
Abbreviations
- AASP:
-
adolescent/adult sensory profile
- ASC:
-
autism spectrum conditions
- ASP:
-
adult sensory profile
- SenSOR:
-
sensory over-responsivity scale
- KS:
-
Kolmogorov-Smirnov test
- PCA:
-
principal component analysis
- SPQ:
-
sensory perception quotient.
References
APA: Diagnostic and Statistical Manual of Mental Disorders. 1987, Washington DC: American Psychiatric Association, 3
Grandin T: My experiences with visual thinking, sensory problems and communication difficulties. Center Study Autism. 1996, Vintage Books
Chamak B, Bonniau B, Jaunay E, Cohen D: What can we learn about autism from autistic persons?. Psychother Psychosom. 2008, 77: 271-279. 10.1159/000140086.
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (DSM). 2013, 5
Tomchek SD, Dunn W: Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am J Occup Ther. 2007, 61: 190-200. 10.5014/ajot.61.2.190.
Schoen SA, Miller LJ, Green KE: Pilot study of the Sensory Over-Responsivity Scales: assessment and inventory. Am J Occup Ther. 2008, 62: 393-406. 10.5014/ajot.62.4.393.
Baranek GT, David FJ, Poe MD, Stone WL, Watson LR: Sensory Experiences Questionnaire: discriminating sensory features in young children with autism, developmental delays, and typical development. J Child Psychol Psychiatry. 2006, 47: 591-601. 10.1111/j.1469-7610.2005.01546.x.
Baranek GT, Boyd BA, Poe MD, David FJ, Watson LR: Hyperresponsive sensory patterns in young children with autism, developmental delay, and typical development. AJMR. 2007, 112: 233-245.
Hilton CL, Harper JD, Kueker RH, Lang AR, Abbacchi AM, Todorov A, LaVesser PD: Sensory responsiveness as a predictor of social severity in children with high functioning autism spectrum disorders. J Autism Dev Disord. 2010, 40: 937-945. 10.1007/s10803-010-0944-8.
Wiggins LD, Robins DL, Bakeman R, Adamson LB: Brief report: sensory abnormalities as distinguishing symptoms of autism spectrum disorders in young children. J Autism Dev Disord. 2009, 39: 1087-1091. 10.1007/s10803-009-0711-x.
Cheung PP, Siu AM: A comparison of patterns of sensory processing in children with and without developmental disabilities. Res Dev Disabil. 2009, 30: 1468-1480. 10.1016/j.ridd.2009.07.009.
Kientz MA, Dunn W: A comparison of the performance of children with and without autism on the Sensory Profile. Am J Occup Ther. 1997, 51: 530-537. 10.5014/ajot.51.7.530.
Lane AE, Dennis SJ, Geraghty ME: Brief report: further evidence of sensory subtypes in autism. J Autism Dev Disord. 2011, 41: 826-831. 10.1007/s10803-010-1103-y.
Ermer J, Dunn W: The sensory profile: a discriminant analysis of children with and without disabilities. Am J Occup Ther. 1998, 52: 283-290. 10.5014/ajot.52.4.283.
Lane AE, Young RL, Baker AE, Angley MT: Sensory processing subtypes in autism: association with adaptive behavior. J Autism Dev Disord. 2010, 40: 112-122. 10.1007/s10803-009-0840-2.
Schoen SA, Miller LJ, Brett-Green BA, Nielsen DM: Physiological and behavioral differences in sensory processing: a comparison of children with autism spectrum disorder and sensory modulation disorder. Front Integr Neurosci. 2009, 3: 29-
Crane L, Goddard L, Pring L: Sensory processing in adults with autism spectrum disorders. Autism. 2009, 13: 215-228. 10.1177/1362361309103794.
Kern JK, Trivedi MH, Grannemann BD, Garver CR, Johnson DG, Andrews AA, Savla JS, Mehta JA, Schroeder JL: Sensory correlations in autism. Autism. 2007, 11: 123-134. 10.1177/1362361307075702.
Kern G, Grannemann T, Carmody A: Examining sensory quadrants in autism. Res Autism Spectr Disord. 2007, 1: 185-193. 10.1016/j.rasd.2006.09.002.
Kern JK, Trivedi MH, Garver CR, Grannemann BD, Andrews AA, Savla JS, Johnson DG, Mehta JA, Schroeder JL: The pattern of sensory processing abnormalities in autism. Autism. 2006, 10: 480-494. 10.1177/1362361306066564.
Brown C, Tollefson N, Dunn W, Cromwell R, Filion D: The Adult Sensory Profile: measuring patterns of sensory processing. Am J Occup Ther. 2001, 55: 75-82. 10.5014/ajot.55.1.75.
Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E: The Autism Spectrum Quotient (AQ): evidence from Asperger syndrome/high functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord. 2001, 31: 5-17. 10.1023/A:1005653411471.
Baron-Cohen S, Hoekstra RA, Knickmeyer R, Wheelwright S: The Autism-Spectrum Quotient (AQ)-Adolescent Version. J Autism Dev Disord. 2006, 36: 343-350. 10.1007/s10803-006-0073-6.
Hoekstra RA, Bartels M, Cath DC, Boomsma DI: Factor structure, reliability and criterion validity of the Autism-Spectrum Quotient (AQ): a study in Dutch population and patient groups. J Autism Dev Disord. 2008, 38: 1555-1566. 10.1007/s10803-008-0538-x.
Wakabayashi A, Baron-Cohen S, Wheelwright S, Tojo Y: The Autism-Spectrum Quotient (AQ) in Japan: A cross-cultural comparison. J Autism Dev Disord. 2006, 36: 263-270. 10.1007/s10803-005-0061-2.
Auyeung B, Baron-Cohen S, Wheelwright S, Allison C: The Autism Spectrum Quotient: Children's Version (AQ-Child). J Autism Dev Disord. 2008, 38: 1230-1240. 10.1007/s10803-007-0504-z.
Raven J: The Raven's progressive matrices: change and stability over culture and time. Cogn Psychol. 2000, 41: 1-48. 10.1006/cogp.1999.0735.
Goldstein AG: Sensation and Perception. 2002, Belmont: Publisher Wadsworth
Hoyle RH, Haris MJ, Judd CM: Research Methods in Social Relations. 2002, Belmont, CA: Thomson/Wadsworth
Lee S, Ma Y, Tsang A: Psychometric properties of the Chinese 15-item Patient Health Questionnaire in the general population of Hong Kong. J Psychosom Res. 2011, 71: 69-73. 10.1016/j.jpsychores.2011.01.016.
Rust J, Golomok S: Modern Psychometrics: The Science of Psychological Assessment., Second edition. 1999, London: Routledge
Tavassoli T, Miller L, Schoen S, Nilson D, Baron Cohen S: Sensory over-responsivity in adults with autism spectrum disoder. Autism. 2013, doi:10.1177/1362361313477246
Baron Cohen S, Wheelwright S: The Empathy Quotient (EQ). An investigation of adults with Asperger Syndrome or high functioning autism, and normal sex differences. J Autism Dev Disord. 2004, 34: 163-175.
Wakabayashi A, Baron-Cohen S, Wheelwright S, Goldenfeld N, Delaney J, Fine D, Smith R, Weil L: Development of short forms of the Empathy Quotient (EQ-short) and the Systemizing Quotient (SQ-short). Personal Individ Differ. 2006, 41: 929-940. 10.1016/j.paid.2006.03.017.
Dunn W, Westman K: The sensory profile: the performance of a national sample of children without disabilities. Am J Occup Ther. 1997, 51: 25-34. 10.5014/ajot.51.1.25.
Lai M, Lombardo M, Pasco G, Ruigrok A, Wheelwright S, Sadek S, Chakrabarti B, Consortium MRCAIMS, Baron-Cohen S:A behavioral comparison of male and female adults with high functioning autism spectrum conditions. PLoS One. 2011, 6: e20835-10.1371/journal.pone.0020835.
Acknowledgements
TT was supported by the Wallace Research Foundation and the Autism Science Foundation. SBC was supported by the MRC UK, the Wellcome Trust, and the Autism Research Trust. This work was conducted in association with the NIHR CLAHRC EoE. We are grateful to the participants for their generous cooperation, and to Dr. Carrie Allison for her help.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors of this paper report that they have no biomedical financial interests or potential conflicts of interest.
Authors’ contributions
TT and SBC designed the SPQ. TT collected the data and TT and RH carried out the data analyses. All authors were involved in writing the manuscript and approved the final version.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Tavassoli, T., Hoekstra, R.A. & Baron-Cohen, S. The Sensory Perception Quotient (SPQ): development and validation of a new sensory questionnaire for adults with and without autism. Molecular Autism 5, 29 (2014). https://doi.org/10.1186/2040-2392-5-29
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2040-2392-5-29