
Abstract
Introduction
Immaturity of motility, intestinal epithelial barrier function and absorptive capacity may play a role in the pathophysiology of intestinal diseases in preterms. We determined the gastric electrical activity and emptying, and intestinal permeability, in preterm newborns to verify if a maturation pattern exists in preterm newborns during the first month of life.
Patients and methods
Eighteen preterm newborns (median 34 wks, range 2 wks) completed the study. They underwent the recording of gastric electrical activity by means of cutaneous electrogastrography, the ultrasound examination of gastric emptying, and the lactulose-to-mannitol ratio from permeability-absorption test on days 3, 7, 15, and 30 after birth.
Results
Gastric electrical activity and emptying showed only slight changes between day 3 and day 7. On the contrary, an evident maturation in permeability, expressed as L/Mratio, was evident over time (Friedman Repeated Measures Analysis, p = 0.004).
Conclusion
In preterm healthy newborns of 34 weeks gestational age, electrical and motor activity are completely developed at birth whilst the intestinal epithelial barrier clearly improves during the first week of life.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Feeding intolerance is a recurrent problem in the clinical care of preterm infants and occur mainly in the first week of life, suggesting the presence of a maturation pattern of gastrointestinal tract [1]. It is known that functional maturation of the gastrointestinal tract is quite different over time with respect to its anatomical development [2–4]. Adequate levels of some digestive enzymes are reached only at the end of gestation and lactase activity at 34 weeks gestation is only 30% of the level of full-term newborns [3]. To date there is little data available about the development of the motility function and of the mucosal barrier in newborns during early days of life.
Gastrointestinal motility can be recorded as a measure of gastric electrical activity, of the wall movements, and of gastric emptying time. A reliable method for recording gastric motility is cutaneous electrogastrography (EGG) [5–7]; electrogastrographic studies in newborns have demonstrated the absence of normal slow waves at birth and a maturation process modulated by enteral feedings [8–11]. Gastric emptying (GE) can be assessed by ultrasonography which is considered a non-invasive technique particularly suitable for young patients [12].
The functional integrity of the mucosal barrier of the intestine partly depends on the close interaction of adjacent mucosal cells. The most reliable in vivo method to study this functional integrity is the sugar absorption test (SAT), which has been performed on adults [13] and newborns, both preterm [14] and term ones [15]. Some of the key events involving permeability actually take place in the neonatal period, when the barrier is leakier. Coordinated motor function in the gastrointestinal tract plays a crucial role in the intestinal transportation, absorption and maintenance of the enteric bacterial ecology [16]. In particular, delayed intestinal transit time may contribute to increased mucosal permeability, and even to facilitated bacterial translocation [17].
The aim of the study was to investigate gastric motility and intestinal permeability to verify if a maturation pattern exists in preterm newborns during the first month of life.
Methods
Infants and protocol
The study was performed at the Neonatology Section of the Department of Pediatrics at the University of Bari. Healthy preterm newborns, born at a gestational age of 28–36 weeks, a birth weight > 1800 g, normal Apgar score, and a post natal age < = 24 h, were eligible to participate in the study. Newborns with: a) respiratory distress, b) congenital malformation, c) inborn errors of metabolism, or d) proven sepsis or infection, were not included. From an initial group of 38 preterm newborns, 18 entirely bottle-fed infants completed the study. The others were excluded for various reasons: a change in milk formula (4 newborns); an infectious disease (1 newborn); withdrawal from the study (7 newborns); inability to perform the scheduled SAT due to early transfer to another hospital (1 newborn) and/or failure to collect urine within the scheduled collection day (7 newborns). All the newborns enrolled reached the total amount of enteral feeding within the first week of life. All the preterm newborns were exclusively bottle-fed with the same preterm standard formula throughout the intervention period. The daily formula intake was approximately 30 ml/kg/day at baseline and 180 ml/kg/day at the end on the study.
Gastric electrical activity, gastric emptying time and intestinal permeability were recorded on days 3, 7, 15, and 30 after birth in order to evaluate the time changes in motility and permeability. The range of the data collection period was rigorously narrow (± 1 day). From birth until the end of the study, episodes of regurgitation, vomiting, number of evacuations, the time of complete emission of meconium, and the daily amount of feedings, were recorded. Written informed consent was obtained from the parents, and the study was approved by our local institutional ethics committee.
Assessment of gastric electrical activity
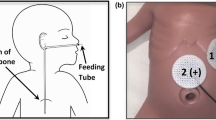
The EGG recordings were performed using portable equipment before and 120 min after meal, following a fasting period of 4 hours. Two silver-silver chloride bipolar electrodes (Clear Trace, ConMed, Utica, NY USA) were placed on the cleaned abdominal surface overlying the antro-pyloric axis to obtain the best signal-noise ratio. The reference electrode was placed to form an equilateral triangle [18]. Electrogastrography was performed using a portable EGG recorder (UPS 2020, Medical Management Systems, MMS, The Netherlands). The recordings and analysis of the EGG parameters (dominant frequency and normal slow wave percentage, power ratio) were previously described in different papers [11, 19]
Assessment of gastric emptying
The ultrasound gastric emptying examinations were always performed by the same investigator using a real-time apparatus (Image Point HX, Hewlett Packard Company, Palo Alto, CA, USA) equipped with a 3.5 MHz linear probe. The ultrasound examination and the measure of the antral area were performed according to the procedure reported in a previous work [11]. The EGG and GE were simultaneously recorded to avoid differences due to the rapid changes in physiological parameters. During the same EGG recording session, antral measurements were made before the test meal, and at regular 30-min intervals up to 180 min after the meal. In each patient, the half emptying time (T1/2) was calculated [11, 12, 20].
Assessment of intestinal permeability
The SAT was performed after oral ingestion, by suckling, of a solution containing 5.0 g of lactulose and 2.0 g of mannitol (Sigma Aldrich s.r.l., Milano, Italy) per 100 ml water (375 mosml/l) at a dose of 2 ml/kg of body weight. The newborns fasted two hours before and after the oral administration of the solution. All the urine passed in the subsequent five hours was collected in an adhesive urine bag (Sincrolag s.r.l. Italy). The complete urine volume was measured and stored at -80°C until analysis. Urinary concentration of lactulose and mannitol were determined by ion exchange chromatography with pulse amperometric detection [21]. Lactulose is a disaccharide that crosses the intestinal epithelium by passive diffusion through the paracellular tight junctions. Mannitol is a monosaccharide that crosses the intestinal epithelium mainly by transcellular passive diffusion through aqueous pores [22]. The evidence of an exclusively transcellular permeation of monosaccharides is still controversial. Mannitol is used for osmotic shrinkage of membrane vesicles, which would not be possible if permeation across cell membranes were unrestricted, and many experimental physiologists use it as an extracellular fluid volume marker suggesting a paracellular route of permeation for this probe [23].
The urinary excretion percentage of lactulose and mannitol are markers for paracellular and transcellular diffusion respectively. To correct for non-mucosal factors that may affect the intestinal uptake of these saccharides, including rate of gastric emptying, intestinal transit time and renal clearance, the urinary percentage of lactulose and mannitol were expressed as the L/M ratio.
Data analysis
The data were first analyzed using simple descriptive statistics of centrality and dispersion. Clinical parameters are expressed as median and range and physiological data are expressed as mean ± SEM. However, because of the sample size and absence of a normal distribution of the data, only non-parametric statistical analysis tests were performed. The overall effect over time of EGG, GE and SAT parameters was determined by a repeated measures analysis (Friedman Friedman Repeated Measures Anova). Because of missing data at some points, multiple comparisons were non available and differences among the recording points of EGG, GE and SAT parameters were made using the Wilcoxon signed rank test. All the differences were considered significant at a 5% level. The software package used for the statistical analysis was STATA (STATA ver 4.0 Statistical Software, Stata Corporation).
Results
Anthropometric and clinical parameters
These parameters are reported in Table 1. It clearly shows that a homogeneous group was collected. None of the newborns presented significant regurgitation and/or vomiting from birth until the last day of examination and all passed the meconium within the second day of life. All newborns reached the total amount of enteral feeding (140 ml/kg/day) within the seven days.
Electrogastrographic and Gastric emptying data
Figure 1(a, b, c) shows the pattern over time of the percentage of normal slow waves recorded before and after meal, and the pattern of power ratio (Power ratio: Friedman Repeated Measures p = 0.18; Wilcoxon signed rank test, day 3 vs day 7 p = 0.02). Figure 2 plots the ultrasound T1/2 over time (Friedman Repeated Measures Analysis p = 0.69; Wilcoxon signed rank test day 3 vs day 7 p = 0.08). Both power ratio and gastric emptying time did show a slightly difference comparing day 3 and day 7, without a significant improvement over time.

Gastric electrical activity are reported as percentage of gastric slow waves (SW) at baseline (a), after meal (b), and power ratio (PR) (c). Repeated measurements analysis did not demonstrate any improvement in power ratio over time. Only a difference at day 7 respect to day 3 is evident. Data are means ± SEM.

Gastric emptying time is reported as the half emptying time (T1/2). Repeated measurements analysis did not show any improvement in T1/2 over time. A slightly difference at day 7 respect to day 3 is only evident. Data are means ± SEM.
Intestinal permeability data
Measurement of lactulose excretion demonstrated an evident reduction at day 7 and the subsequent recording days (Figure 3a). On the other hand, measurement of mannitol excretion demonstrated a fluctuation over time and an increase on day 7 without reaching a significant difference (Figure 3b). The L/M ratio showed a deep decline between day 3 and day 7, then the ratio became constantly low (Friedman Repeated Measures Analysis p = 0.004; Wilcoxon signed rank test: day 3 vs day 7 p < 0.05, day 3 vs day 15 p < 0.05, day 3 vs day 30 p < 0.05 (Figure 3c).

Intestinal permeability pattern as determined by urinary excretion of orally administered lactulose (a), mannitol (b), and L/M ratio (c) respectively. L/M ratio persistently and significantly reduces after day 3 (see text). Data are means ± SEM.
Discussion
In preterm newborns the gastric electrical activity is quite stable with slight differences in power ratio and emptying at given recording days. On the contrary, intestinal permeability showed a persistent improvement over the first week of postnatal life.
A few studies have investigated the gastric motility and intestinal permeability in preterm newborns. We studied the gastric electrical activity, gastric emptying and intestinal permeability in a time series in order to account for the effect of the different physiological variables over time. The pattern of slow wave percentage in the normal neonates showed a stable 3 cpm activity over time. During the first month of life the slow wave percentage was usually reported to be about 38% [24] from birth to 4 weeks, whilst according to others the slow wave percentage was about 50% [25]. Our data from premature newborns showed a higher percentage of normal slow wave, probably as a result of our broad interval in the normal EGG frequency ranges.
Intestinal immaturity is limited largely to infants of less than 34 weeks gestation but may extend to older gestational ages. Intestinal immaturity could explain poor gastroduodenal coordination and excessive quiescence in motor activity reported in very immature infants as poor gastric emptying, duodenogastric reflux and gastroduodenal hypomotility [26, 27]. Our group of healthy newborns were of about 34 weeks gestation and showed a normal EGG parameters and gastric emptying time, even if subtle differences between the recording days were found. These findings confirm that gastric development is complete in late preterm infants [28–30].
Different sugar-absorption tests for measuring intestinal permeability for sugars have been studied in a variety of gastrointestinal diseases. In vivo mannitol is absorbed via the transcellular pathway and serves as a marker of transcellular uptake [22, 23] while lactulose is only slightly absorbed, but exclusively across the intestinal membrane through the intercellular junctions, and serves as a marker for mucosal integrity [31]. In our study L/M ratio was sharply reduced at day 7, then it remained stable. The clinical significance of an increased intestinal permeability is still under investigation. Although alterations in intestinal permeability could cause bacterial translocation and septic complications, no evidence is reported in humans to support this assumption [32, 33]. A close relationship between luminal factors and permeability was demonstrated only for IgA, ovoalbumin, and bacterial peptides [34–36]. Overall, the human neonate shows a developmental pattern of sugar intestinal permeability that resembles gut closure observed in other mammals; intestinal permeability decreases faster in breast-fed newborns than in those fed with adapted or hydrolysed formula [37, 38]. However, both decreased and increased permeability during the first months of life have been reported [14, 39, 40]. The reasons for such discrepancies lie in the differences in study design such as gestational age, clinical condition, feeding regiments and postnatal age at the time of the studies. Our data are similar to that of Van Elburg, actually preterm newborns permeability is higher during the first 2 days of life than up to 6 days later, independently of birth weight and gestational age [41]. Our data showed a slight increase in mannitol permeability in day 7 and a dramatic reduction of L/M ratio between day 3 and day 7 related to reduced lactulose permeability. Even if the relationship between feeding and intestinal maturation was not studied in our paper, some authors have demonstrated that the starting of enteral feeding induces an increase in intestinal barrier function [42]. The fact that adult patients fed with total parenteral nutrition showed an impaired intestinal permeability confirms the link between enteral nutrition and permeability [43].
In conclusion, healthy late preterm newborns showed mature EGG and gastric emptying and a rapid improvement in intestinal permeability. The role of enteral nutrients is not merely linked to nourishing the developing intestine of the premature infants but may represent a kick off point. Optimization of nutrition in preterm infants could have major implications for health and outcome.
Abbreviations
- EGG:
-
Cutaneous electrogastrography
- GE:
-
Gastric emptying
- SAT:
-
Sugar absorption test
- DF:
-
Dominant frequency
- SW:
-
Slow waves
- PR:
-
Power ratio
- FFT:
-
Fast Fourier transform
- T1/2:
-
Half emptying time.
References
Piena-Spoel M, Albers MJ, Ten Kate J, Tibboel D: Intestinal permeability in newborns with necrotizing enterocolitis and controls: Does the Sugar absorption test provide guidelines to (re-)introduce enteral nutrition?. J Pediatr Surg. 2001, 36: 587-92. 10.1053/jpsu.2001.22288.
Neu J: Gastrointestinal development and meeting the nutritional needs of premature infants. Am J Clin Nutr. 2007, 85 (2): 629S-34S.
Lebenthal A, Lebenthal E: The ontogeny of the small intestinal epithelium. JPEN J Parenter Enteral Nutr. 1999, 23 (suppl): S3-6.
Berseth CL: Gastrointestinal motility in the neonate. Clin Perinatol. 1996, 23: 179-190.
Abell TL, Malagelada J-R: Electrogastrography. Current assessment and future perspectives. Dig Dis Sci. 1988, 83: 982-992. 10.1007/BF01535995.
Familoni BO, Bowes KL, Kingma YJ, Cote KR: Can transcutaneous recording detect gastric electrical abnormalities?. Gut. 1991, 32: 141-146. 10.1136/gut.32.2.141.
Geldof H, Schee Van der EJ: Electrogastrography, clinical application. Scand J Gastroenterol. 1989, 24: 5-82. 10.3109/00365528909091376.
Chen JDZ, Co E, Liang J, Pan J, Sutphen J, Torres-Pinedo RB: Pattern of gastric myoelectrical activity in human subjects of different ages. Am J Physiol. 1997, 272: G1022-G1027. (Gastrointest Liver Physiol 35)
Koch KL, Tran TN, Stern RM, Bingaman S, Sperry NJ: Gastric electrical activity in premature and term infants. J Gastrointest Mot. 1993, 5: 41-47.
Liang J, Co E, Zhang M, Pineda J, Chen JDZ: Development of gastric slow waves in preterm infants measured by electrogastrography. Am J Physiol. 1998, 274: G503-508. Gastrointest Liver Physiol 37
Riezzo G, Indrio F, Montagna O, Tripaldi C, Laforgia N, Chiloiro M: Gastric electrical activity and gastric emptying in term and preterm newborns. Neurogastroenterol Mot. 2000, 12: 223-229. 10.1046/j.1365-2982.2000.00203.x.
Bolondi L, Gaiani S, Barbara L: Ecografia Funzionale ed Ecodoppler in gastroenterologia. Milano: Masson. 1989
Fleming SC, Kapemba MS, Laker MF, Levin GE, Griffin GE: Rapid and simultaneous determination of lactulose and mannitol in urine, by HPLC with pulse amperometric detection, for use in studies of intestinal permeability. Clin Chem. 1990, 36: 797-799.
Shulman RJ, Schanler RJ, Lau C, Heitkemper M, Ou CN, Smith EO: Early feeding, antenatal glucocorticoids, and human milk decrease intestinal permeability in preterm infants. Pediatr Res. 1998, 44: 519-523. 10.1203/00006450-199810000-00009.
Catassi C, Bonucci A, Coppa GV, Carlucci A, Giorgi PL: Intestinal permeability changes during the first month: effect of natural versus artificial feeding. J Pediatr Gastroenterol Nutr. 1995, 21: 383-386.
Gunningham KM, Horowitz M, Read NW: Gastrointestinal adaption to diets of differing fat composition in human volunteers. Gut. 1991, 32: 483-486. 10.1136/gut.32.5.483.
Valori R: Small intestinal motility. Curr Opin Gastroenterol. 1992, 8: 257-261. 10.1097/00001574-199204000-00010.
Riezzo G, Cucchiara S, Chiloiro M, Minella R, Guerra V, Giorgio I: Gastric emptying and myoelectrical activity in children with non-ulcer dyspepsia. Effect of Cisapride. Dig Dis Sci. 1995, 40: 1418-1434. 10.1007/BF02285188.
Schee Van Der EJ, Smout AJPM, Grashuis JL: Application of running spectrum analysis to electrogastrographic signals recorded from dog and man. Motility of the Digestive tract. Edited by: Wenbeck M. 1982, New York: Raven Press, 1241-1250.
Bolondi L, Bortolotti M, Santi V: Measurement of gastric emptying time by real time ultrasonography. Gastroenterology. 1985, 89: 752-759.
Van Elburg RM, Uil JJ, Kokke FT, Mulder AM, Broek van de WG, Mulder CJ: Repeatability of sugar-absorption test, using lattulose and mannitol, for measuring intestinal permeability for sugars. J Pediatr Gastroenterol Nutr. 1995, 20: 184-188.
Indrio F, Raimondi F, Laforgia N, Riezzo G, Polimeno L, Francavilla R: Effect of hyperbilirubinemia on intestinal permeability in healthy term newborns. Acta Pædiatrica. 2007, 96: 73-75. 10.1111/j.1651-2227.2006.00007.x.
Raimondi F, Santoro P, Maiuri L, Londei M, Annunziata S, Ciccimarra F, Rubino A: Reactive nitrogen species modulate the effects of rhein, an active component of senna laxatives, on human epithelium in vitro. J Pediatr Gastroenterol Nutr. 2002, 34: 529-34. 10.1097/00005176-200205000-00011.
Patterson M, Rintala R, Lloyd DA: A longitudinal study of electrogastrography in normal neonates. J Ped Surg. 2000, 35: 59-61.
Lange A, Huang L, Funch-Jensen P: Electrogastrography in neonates. Neurogastroenterol Mot. 2005, 17: 512-517. 10.1111/j.1365-2982.2005.00656.x.
Daniel EE, Wang YF: Control systems of gastrointestinal motility are immature at birth in dogs. Neurogastroenterol Motil. 1999, 11: 375-392. 10.1046/j.1365-2982.1999.00159.x.
Jadcherla SR, Kliegman RM: Studies of feeding intolerance in very low birth weight infants: definition and significance. Pediatrics. 2002, 109: 516-517. 10.1542/peds.109.3.516.
Koch KL, Stern RM: Electrogastrographic data acquisition and analysis. The Penn State Experience. Electrogastrography: Principles and Applications. Edited by: Chen JZ, McCallum RW. 1994, New York: Raven Press, 31-73.
Riezzo G, Indrio F, Montagna O, Tripaldi C, Laforgia N, Chiloiro M: Gastric electrical activity and gastric emptying in preterm newborns fed standard and hydrolysate formulas. J Pediatr Gastroenterol Nutr. 2001, 33: 290-295. 10.1097/00005176-200109000-00012.
Riezzo G, Castellana RM, De Bellis T, Laforgia F, Indrio F, Chiloiro M: Gastric electrical activity in normal neonates during the first year of life: effect of feeding with breast milk and formula. J Gastroenterol. 2003, 38: 836-843. 10.1007/s00535-003-1158-z.
Bjarnason I, McPherson A, Hollander D: Intestinal permeability: An Overview. Gastroenterology. 1995, 108: 1566-1581. 10.1016/0016-5085(95)90708-4.
O'Boyle CJ, MacFie J, Dave K, Sagar PS, Poon P, Mitchel CJ: Alteration in intestinal barrier function do not predispose to translocation of enteric bacteria in gastroenterological patients. Gut. 1999, 44: 283-289.
Kanwar S, Windsor AC, Welsh F, Barclay GR, Guillou PJ, Reynolds JV: Lack of correlation between failure of gut barrier function and septic complications after major upper gastrointestinal surgery. Ann Surg. 2000, 231: 88-95. 10.1097/00000658-200001000-00013.
Ramage JK, Stanisz A, Schicchiatano R, Hunt RH, Perdue MH: Effects of immunologic reactions on rat intestinal epithelium. Correlation of increased intestinal permeability to chromium 51ethylendiaminetetraacetc acid and ovoalbumin during acute inflammation and anaphylaxis. Gastroenterology. 1988, 94: 1368-1375.
Davin JC, Forget P, Mahieu PR: Increased intestinal permeability to 51Cr-EDTA is correlated with IgA immune-complex-plasma levels in children with associated nephropaties. Acta Pediatr Scand. 1988, 77: 118-124. 10.1111/j.1651-2227.1988.tb10609.x.
Ferry DM, Butt TJ, Broom MF, Hunter J, Chadwick VS: Bacterial chemotactic oligopeptides and the intestinal mucosal barrier. Gastroenterology. 1989, 97: 61-67.
Weaver LT, Laker MF, Nelson R, Lucas A: Milk feeling and changes in intestinal permeability and morphology in the newborn. J Pediatr Gastroenterol Nutr. 1987, 6: 351-8.
Catassi C, Bonucci A, Coppa GV, Carlucci A, Giorgi PL: Intestinal permeability changes in the first month: effect of natural versus artificial feeding. J Pediatr Gastroenterol Nutr. 1995, 21: 383-6.
Weaver LT, Laker MF, Nelson R: Intestinal permeability in the newborns. Arch Dis Child. 1984, 59: 236-241. 10.1136/adc.59.3.236.
Beach RC, Menzies IS, Claiden GS, Scoper JW: Gastrointestinal permeability changes in in the preterm neonates. Arch Dis Child. 1982, 57: 141-145. 10.1136/adc.57.2.141.
Van Elburg RM, Fetter WP, Bunkers CM, Heymans HS: Intestinal permeability in relation to birth weight and gestational and postnatal age. Arch Dis Child Fetal Neonatal Ed. 2003, 88: F52-5. 10.1136/fn.88.1.F52.
Corpeleijn WE, van Vliet I, de Gast-Bakker DH: Effect of Enteral IGF-1 Supplementation on Feeding Tolerance, Growth, and Gut Permeability in Enterally Fed Premature Neonates. J Pediatr Gastroenterol Nutr. 2008, 46: 184-190. 10.1097/MPG.0b013e31815affec.
Hulst van der RR, van Kreel BK, von Meyenfeldt MF, Brummer RJ, Arends JW, Deutz NE, Soeters PB: Glutamine and the preservation of gut integrity. Lancet. 1993, 334 (8857): 1363-1365.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
GR conceived of the study, carried out the recording of the gastric electrical activity and drafted the manuscript. FI conceived of the study, and carried out the permeability tests and polish the manuscript. RF participated in the design of the study. OM carried out the permeability tests and gastric emptying studies. GS participated in the design of the study. MB performed the statistical analysis. LC participated in the coordination of the study. RF participated in the coordination of the study and polish the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Riezzo, G., Indrio, F., Raimondi, F. et al. Maturation of gastric electrical activity, gastric emptying and intestinal permeability in preterm newborns during the first month of life. Ital J Pediatr 35, 6 (2009). https://doi.org/10.1186/1824-7288-35-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1824-7288-35-6