
Abstract
Background
Accurate microbial diagnosis is crucial for effective management of prosthetic joint infections. Culturing of multiple intraoperative tissue samples has increased diagnostic accuracy, but new preparatory techniques and molecular methods hold promise of further improvement. The increased complexity of sampling is, however, a tough challenge for surgeons and assistants in the operation theatre, and therefore we devised and tested a new concept of pre-packed boxes with a complete assortment of swabs, vials and additional tools needed in the operating theatre for non-standard samples during a clinical study of prosthetic joint infections.
Findings
The protocol for the clinical study required triplicate samples of joint fluid, periprosthetic tissue, bone tissue, and swabs from the surface of the prosthesis. Separate boxes were prepared for percutaneous joint puncture and surgical revision; the latter included containers for prosthetic components or the entire prosthesis. During a 2-year project period 164 boxes were used by the surgeons, 98 of which contained a complete set of samples. In all, 1508 (89%) of 1685 scheduled samples were received.
Conclusion
With this concept a high level of completeness of sample sets was achieved and thus secured a valid basis for evaluation of new diagnostics. Although enthusiasm for the project may have been a contributing factor, the extended project period suggests that the ‘All in a box’ concept is equally applicable in routine clinical settings with standardized but complex diagnostic sampling.
Similar content being viewed by others


Findings
Background
The microbiological diagnosis plays a crucial role in the effective management of patients with suspected prosthetic joint infection (PJIs)[1]. Diagnostic procedures include percutaneous aspiration of joint fluid as well as revision surgery with retention or removal of prosthetic elements. Chronic foreign body-related infections pose a special challenge because of the diversity of microorganisms involved and their adaption to a subdued lifestyle associated with formation of biofilms. Culturing of multiple samples has been shown to increase diagnostic accuracy, and there is growing evidence to support the utility of new preparatory techniques and molecular methods[2–4].
As a direct consequence of this development the number and types of samples wanted from the surgical field are increasing, and the sampling procedure thereby becomes more cumbersome for the surgeon. Even with assistance from a skilled nurse on the floor of the operating theatre important samples can be missed or deposited in an unsuitable transport medium, and the diagnostic accuracy can thereby be compromised[2, 4–6].
Within an ongoing research project comprising patients with a painful prosthetic joint (‘Prosthesis: Related Infection and Pain’ (PRIS), http://www.joint-prosthesis-infection-pain.dk) we have addressed this issue by designing pre-packed boxes containing disposable scalpels and forceps, swaps, transport vials, and labels needed for sampling during the surgical procedure. Additional boxes were made available for samples of synovial fluid obtained by percutaneous joint aspiration. Our primary aim was to overcome the variation in sampling technique within and between surgical teams and across difference hospitals, which otherwise might affect the validity of our clinical study. Our belief was that streamlining sampling procedures would maximize the completeness of sample sets. We here present the results from a 2-year project period.
All in a box
We applied the ‘All in a box’ concept to two surgical procedures and report the completeness of sampling within a prospective cohort of patients undergoing revision surgery.
The concept was developed jointly by orthopaedic surgeons, molecular biologists, and clinical microbiologists within the framework of the PRIS project. The project was approved by the Regional Committee on Health Research Ethics (June 2011; ref. no. N-20110022). Informed oral and written consent was obtained from each patient.
The sample repertoire was supplementary to five intraoperative soft tissue biopsies obtained according to the Kamme and Lindberg principle[7]. For revisions the non-standard samples comprised joint fluid, intraoperative soft tissue and bone biopsies, swabs from the surface of the prosthesis in situ, and prosthetic components or the entire prosthesis. Diagnostic methods included bacteriological culture, 16S rDNA gene amplification followed by amplicon sequencing, and fluorescence in situ hybridization (FISH). Thus, samples were obtained in triplicate except for the prosthesis itself or prosthetic components. Each sample was handled separately with disposable utensils in order to minimize cross-contamination[7, 8] and thus allow valid comparison of different sample types and analyses.
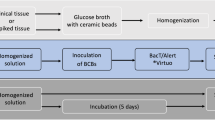
The two types of boxes are presented in Figure 1 and Table 1. The sample collecting kit for revision surgery consisted of scalpels and forceps, and a special needle for a bone biopsy (Vertebroplasty Needle, Synthes, West Chester PA, USA). Sample tubes were colour coded according to sample type. For collection of biopsies, tubes with a broad neck were chosen to facilitate handling in the operating theatre as well as in the laboratories. A sterile container of an appropriate size for the prosthetic component was included for revision surgery. The only item not included in the pre-packed boxes was a blood culture vial for synovial fluid due to its limited shelf life.

Sample boxes for joint puncture (A) and revision surgery (B). A: Joint fluid is both inoculated directly into a blood culture flask (BacT/Alert, bioMérieux, Marcy l’Etoil, France) and submitted for extensive culture examination and molecular diagnostics. B: Sample tubes are colour coded in the revision surgery box in order to assist the operation staff in achieving complete sample sets. Sample tubes had a broad neck in order to facilitate the deposition of the sample.
From the surgical theatre the boxes were transported at ambient temperature to the Department of Clinical Microbiology and processed within 24 h. Most samples were processed within 2 h after removal of the prosthesis, whereas samples from acute surgery undertaken out of hours were kept at 4°C overnight except for the blood culture vial that was held at room temperature. When delivered to the lab, samples for molecular analysis were subjected to vigorous agitation (vortexing for 30 sec) and stored immediately at -80°C until batch wise processing and analysis. For microbiological culture components of the prosthesis (covered with PBS-buffer, pH7.4) were vortexed and sonicated (summarised in[2]). Bone biopsies were treated similarly before culturing. The joint fluid, tissue biopsies, and the prosthesis swab were cultured without pre-processing. All sample types were cultured aerobically and anaerobically for 14 days with subcultivation from enrichment broth after 6 days for positive samples and after 10 days for negative samples.
All surgeons undertaking revision surgery were informed about the box design and agreed to the concept. The implementation benefitted further from liaison with the nurses assisting in the operating theatre. Of note, joint punctures took place in both ambulatory and in-hospital settings, and they were less rigidly standardized compared with revisions.
‘Proof of concept’
The scheduled number of samples was four for percutaneous joint aspiration (box A) and 13 for revision surgery (box B) (Table 1). From December 2011 through February 2014 we obtained 98 boxes with a complete sample set out of 164 consecutive boxes (box A: 25/42 (60%); box B: 73/122 (60%)). In all, 1508 of 1685 scheduled samples were obtained (overall completeness 89%). The main reasons for missing samples were deviations from the pre-planned surgical procedure for clinical reasons or absence of a trained assistant. In 8 cases the sample set in box B was incomplete as a consequence of acute surgery (69 of 104 scheduled samples (66%)).
Experience and perspective
We find the ‘All in a box’ to be a promising logistic concept for obtaining multiple samples as part of surgical procedures. The concept may be applicable not only to the diagnosis of PJIs but also to other diagnostic procedures and would be well suited especially in circumstances where limited amounts of sample material must be shared between several diagnostic tests and the use of a correct transport medium plays an important role for the performance of the diagnostic test. An obvious addition to the different microbiological tests in this clinical study would be tissue samples for histopathology. Despite the complex intraoperative sampling procedure the ‘All in a box’ concept provided an overall completeness around 90% in a research project involving several orthopaedic surgeons, numerous nurses, and different hospital premises.
The concept should also be applicable to other complex sampling procedures utilizing a standardized panel of diagnostic sample types and thus has a potential for time saving and optimization in different diagnostic settings. Although we ascribe the high level of completeness in our study to the ‘All in a box’ concept, it must be acknowledged that enthusiasm surrounding the research project may also have been involved. Still, the positive attitude often withers when procedures are complicated and involve many surgeons and nurses, but it was our impression that the box logistics helped to maintain the spirit in this case. A drawback to the concept was the time consumed by the meticulous preparation of the boxes, a task which can be managed within the framework of a scientific project, but may be difficult to tackle on a routine basis in hospitals and clinics. We estimate the cost of materials for box A to be 130 €, and the full diagnostic work-up of samples in this box may amount to 1075 € including extensive 16S rDNA sequencing. Implementation of only the most effective diagnostic modalities may help to decrease these costs. Moreover, the concept could be of interest to providers of diagnostic utensils and could also be instrumental in implementing standardized sampling procedures eventually based on international guidelines.
References
Zimmerli W, Trampuz A, Ochsner PE: Prosthetic-joint infections. N Engl J Med. 2004, 351: 1645-1654. 10.1056/NEJMra040181.
Larsen LH, Lange J, Xu Y, Schønheyder HC: Optimizing culture methods for diagnosis of prosthetic joint infections: a summary of modifications and improvements reported since 1995. J Med Microbiol. 2012, 61: 309-316. 10.1099/jmm.0.035303-0.
Xu Y, Rudkjøbing VB, Simonsen O, Pedersen C, Lorenzen J, Schønheyder HC, Nielsen PH, Thomsen T: Bacterial diversity in suspected prosthetic joint infections: an exploratory study using 16S rRNA gene analysis. FEMS Immunol Med Microbiol. 2012, 65: 291-304. 10.1111/j.1574-695X.2012.00949.x.
Atkins BL, Athanasou N, Deeks JJ, Crook DW, Simpson H, Peto TE, Lardy-Smith P, Berendt AR, The OSIRIS Collaborative Study Group: Prospective evaluation of criteria for microbiological diagnosis of prosthetic-joint infection at revision arthroplasty. J Clin Microbiol. 1998, 36: 2932-2939.
Gomez E, Patel R: Laboratory diagnosis of prosthetic joint infection, Part I. Clin Microbiol Newsl. 2011, 33: 55-60. 10.1016/j.clinmicnews.2011.03.004.
Gomez E, Patel R: Laboratory diagnosis of prosthetic joint infection, Part II. Clin Microbiol Newsl. 2011, 33: 63-70. 10.1016/j.clinmicnews.2011.04.001.
Kamme C, Lindberg L: Aerobic and anaerobic bacteria in deep infections after total hip arthroplasty: differential diagnosis between infectious and non-infectious loosening. Clin Orthop Relat Res. 1981, 154: 201-207.
Tunney MM, Patrick S, Curran MD, Ramage G, Hanna D, Nixon JR, Gorman SP, Davis RI, Anderson N: Detection of prosthetic hip infection at revision arthroplasty by immunofluorescence microscopy and PCR amplification of the bacterial 16S rRNA gene. J Clin Microbiol. 1999, 37: 3281-3290.
Acknowledgments
This technical note was prepared within the framework of the ‘Prosthetic-Related Infection and Pain’ (PRIS) - Innovation project, http://www.joint-prosthesis-infection-pain.dk. The study was supported by a grant for the PRIS Innovation Consortium from The Danish Council for Technology and Innovation (no. 09–052174).
Thanks to the PRIS Study Group and especially to Poul T. Nielsen, Jess T. Riis, Andreas Kappel, Mogens B. Jørgensen, Mogens B. Laursen, Vesal Khalid, Camilla R. Rethleff, Ulla Hornum, Dorthe Kvorning, Lasse Lengsø, Susanne Bielidt, Lena Mortensen, Mette Mølvadgaard, Jan Lorenzen and the staff from the Department of Clinical Microbiology and the Orthopaedics Departments for their practical contributions to the sampling.
Special thanks also to Santina Castriciano (Copan Italia A.S.P.) for her unfailing interest in our project.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interest.
The transport medium ‘Modified Amies media with 20% glycerol’ was developed in cooperation between the authors and Copan Italia S.P.A. (Brescia, Italy). All transport media were provided by Copan, if not otherwise indicated. Copan did not influence on the manuscript and the authors have no financial interests to declare.
Authors’ contributions
OS, TRT and HCS designed and developed the first versions of the boxes. After inputs from YX and CP the first pilot study was conducted with OS and CP as surgeons[3]. LHL, YX, TRT, HCS and OS optimized the boxes for the clinical study. LHL and YX were responsible for the overall management of the boxes. LHL prepared the first draft of the manuscript and all authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Larsen, L.H., Xu, Y., Simonsen, O. et al. ‘All in a box’ a concept for optimizing microbiological diagnostic sampling in prosthetic joint infections. BMC Res Notes 7, 418 (2014). https://doi.org/10.1186/1756-0500-7-418
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1756-0500-7-418