
Abstract
Background
In sub-Saharan Africa, as high as 2/3 of tuberculosis patients are HIV/AIDS co-infected and tuberculosis is the most common cause of death among HIV/AIDS patients worldwide. Tuberculosis and HIV co-infections are associated with special diagnostic and therapeutic challenges and constitute an immense burden on healthcare systems of heavily infected countries like Ethiopia. The aim of the study was to determine the prevalence of pulmonary tuberculosis and their immunologic profiles among HIV positive patients.
Methods
A cross sectional study was conducted among adult HIV-positive patients attending HIV/AIDS clinic of Gondar University Hospital. Clinical and laboratory investigations including chest x-ray and acid fast staining were used to identify tuberculosis cases. Blood samples were collected to determine CD4+ lymphocyte count. A structured questionnaire was used to collect socio-demographic characteristics of study subjects. The data was entered and analyzed using SPSS version 16 software.
Results
A total of 400 HIV positive study participants were enrolled. Thirty (7.5%, 95%CI: 5.2-10.6%) of the study participants were found to have pulmonary tuberculosis. In multivariate analysis, only CD4+ lymphocyte count (AOR = 2.9; 95% CI: 1.002-8.368) was found to be independently associated with tuberculosis-HIV co-infection. Individuals who had advanced WHO clinical stage were also statistically significant for co-infection. The mean CD4+ lymphocyte count of HIV mono-infected participants were 296 ± 192 Cells/mm3 and tuberculosis-HIV co-infected patients had mean CD4+ lymphocyte count of 199 ± 149 Cells/mm3 with p value of 0.007.
Conclusions
We found high prevalence of tuberculosis-HIV co-infection. Lower CD4+ lymphocyte count was found to be the only predicting factor for co-infection. Early detection of co-infection is very necessary to prolong their ART initiation time and by then strengthening their immune status.
Similar content being viewed by others


Background
Tuberculosis (TB) and human immune deficiency virus (HIV) infections are two major public health problems in many parts of the world. The prevalence of TB-HIV Co-infection is higher worldwide and 90% of these co-infected cases live in developing nations [1–3]. Tuberculosis is the most common opportunistic disease and cause of the death for those infected with HIV [3]. Similarly, HIV infection is one of the most important risk factors associated with an increased risk of latent TB infection progressing to active TB disease [4, 5]. In persons infected with TB only, the lifetime risk of developing TB ranges between 10% and 20% [6, 7]. However in persons who have been co-infected with TB and HIV, the annual risk can exceed 10% [8–10].
An estimated 1.37 million HIV positive TB patients were diagnosed globally in 2007, and around 80% of them live in sub-Saharan Africa [11]. Tuberculosis and HIV co-infections are associated with special diagnostic and therapeutic challenges and constitute an immense burden on healthcare systems of heavily infected countries like Ethiopia [12].
Unlike other opportunistic infections which occur at CD4+ lymphocyte count below 200/mm3, active TB occurs throughout the course of HIV disease [13]. Clinical presentation of TB in HIV-infected individuals depends on the level of immunosuppression resulting from HIV infection. In patients with relatively intact immune function (CD4+ lymphocyte count >200/mm3), pulmonary tuberculosis (PTB) is more frequently seen than extra pulmonary TB [14, 15].
Ethiopia is among the countries most heavily affected by the HIV and TB. The World Health Organization (WHO) has classified Ethiopia 7th among the 22 high burden countries with TB and HIV infection in the world [16].
It is recognized that joint TB-HIV interventions will clearly require additional funding to improve both TB and HIV program performance and coverage, increase testing and counseling, prevent mother to child transmission of HIV infection, provide community home based care for people living with HIV/AIDS and provide antiretroviral treatment. Despite this needs, there is no adequate and recent data in Ethiopia especially in this study area. Therefore, the aim of this study was to determine the prevalence of PTB among pre-antiretroviral treatment (ART) HIV positive patients and their immunologic profiles which is important for health professionals and policy makers to make evidence based decisions.
Methods
Study design, period and setting
A cross sectional study was conducted from March 27 to May 30, 2011 at Gondar University Hospital, Northwest Ethiopia. Gondar University Hospital is a teaching referral hospital located 720 km North West of Addis Ababa. It is the only referral hospital for North West Ethiopia serving a population of about 5 million coming from different geographical locations surrounding it. The hospital provides inpatient and outpatient services, including care and treatment for TB and HIV/AIDS patients with ARTs. Patients being evaluated for ART initiation undergo a routine medical examination, including screening for TB disease and other opportunistic infections.
Source population and Study participants
The source populations for this study were all HIV positive individuals who have the access to be served in Gondar University Hospital. The study participants were all ART naïve HIV positive adult individuals who have visited ART clinic at Gondar University Hospital during the study period. A total of 422 subjects were enrolled in the study considering 95% confidence, 5% margin of error, 50% of prevalence of TB (since there was no previous estimate of TB among HIV infected individuals in the area) and 10% contingency by using single proportion formula [17]. Study subjects were selected using systematic sampling technique from patient’s record in HIV/AIDS clinic by taking patients registered in every 6th interval. Those ART naïve adult HIV positive individuals who gave informed consent and enough amount of blood sample were included but Individuals who were on ART and those with known chronic illnesses like diabetes mellitus and hypertension were excluded from the study.
Data collection procedures
All subjects underwent TB screening which include: (1) symptom screening and physical examination, (2) patients having sputum production and clinical manifestations were requested to provide three sputum specimens (spot-morning-spot) for smear microscopy, and (3) chest radiography. Study participants were interviewed about the presence of clinical manifestations of TB. Socio-demographic characteristics and other related risk factors were collected using structured questionnaire by trained nurses and physical examination was done by physicians. Posterior and anterior chest x-ray (CXR) was done for patients having sputum production and clinical manifestations and interpreted. All patients having sputum production and clinical manifestations provided 3 sputum samples for smear examinations (spot-early morning-spot). Sputum was collected in a plastic leak-proof container and smear was done for acid fast staining using a direct Ziehl-Neelson (ZN) technique [18]. Five milliliter of venous Blood was aseptically collected in ethylene diamine-tetra-acetic acid (EDTA) tubes for CD4+ lymphocyte count. The CD4+ lymphocyte count was done by BD FACS count flow cytometry machine [19]. The daily, weekly and monthly maintenance of the BD FACS count flow cytometry was done according to the instruments manual and quality control for both the reagent and the machine was done daily.
Case definitions
Smear positive PTB was defined as one or more sputum smear examinations positive for acid fast bacilli (AFB). Smear-negative PTB was also defined as three sputum smear examinations negative for AFB but with clinical and radiographic abnormalities consistent with active tuberculosis [20].
Data analysis
Data were checked for completeness, cleaned manually and entered and analyzed using SPSS version 16 statistical software (SPSS Inc. Chicago, USA). Data were summarized using frequency tables. Backward Stepwise logistic regression model was fitted to identify different determinants of TB-HIV co-infection. Standard techniques for model checking, including the Hosmer-Lemeshow goodness of fit test, were carried out to determine the adequacy of the regression model. Statistical significance was inferred at P-value <0 .05. Mean plus standard deviation with 95% confidence interval (CI) was also used for continuous variables and the difference in means was compared with independent-sample t-test.
Ethical considerations
Ethical issues were approved by ethical review committee of Department of Microbiology, Immunology and Parasitology, College of Medicine and Health sciences, University of Gondar. Oral and verbal informed consent was obtained from the patients prior to enrolment. Patients having tuberculosis were directed to TB/HIV clinic for treatment.
Results
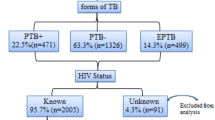
A total of 422 study subjects were sampled but 22 of them were not included because of absence of sputum production for microscopy. Out of 400 study participants, 122(30.5%) were males (with mean age of 37 + 9 years) and 278 (69.5%) were females (mean age of 32 + 9 years) with male to female ratio of 0.4:1. The lowest and the highest age of the study participants were 18 and 70 years respectively. Three hundred thirty five (83.8%) of study participants were from urban and the rest were from rural areas. Half of the participants (50%) were married and 151 (37.8) were illiterate. Out of the total study participants, 279 (69.8%) were housewives and daily laborers [Table 1].
Tuberculosis-HIV co-infection
Thirty (7.5%, 95%CI: 5.2-10.6%) of the study participants were found to have PTB. Of these TB-HIV co-infected cases, 19 (63.3%) were smear negative PTB. The majority of PTB cases 27 (90%) were found to have chest radiological abnormalities consistent with active PTB and about 93.3% of co-infected study subjects were found to have constitutional symptoms; cough of >2 weeks duration, fever, night sweat and weight loss. The majority of participants 263 (65.7%) were in WHO clinical stage of I followed by WHO clinical stage II 65 (16.3%) and WHO clinical stage III 61 (15.3%). Only 11 (2.8%) study participants were found to be in WHO clinical stage IV [Table 2].
Immunological profile of study subjects
The majority of study participants 285 (71.3%) had CD4+ lymphocyte count of less than 349 Cells/mm3 and 115 (28.7%) of study participants had CD4+ lymphocyte count of greater than or equal to 350 Cells/mm3 [Table 2]. Sixteen (53.3%) of co-infected patients were found to have CD4+ lymphocyte count less than 200 Cells/mm3. The mean CD4+ lymphocyte count of HIV mono-infected participants was 296 ± 192 Cells/mm3 and TB-HIV co-infected patients had mean CD4+ lymphocyte count of 199 ± 149 Cells/mm3 with P-value of 0.007.
Predictors of TB-HIV co-infection
In multivariate analysis, only CD4+ lymphocyte count was found to be independently associated with TB-HIV co-infection. Individuals who had CD4+ lymphocyte count of <200Cells/mm3 were 2.9 (95% CI: 1.002-8.368) times more likely to be co-infected than individuals who had CD4+ lymphocyte count of ≥350Cells/mm3. Though the independent effect (in multivariate analysis) of WHO clinical stage is not determined because of zero cells of stage I and stage II, individuals who had a WHO clinical stage of IV were 8.6 (95% CI:1.69-43.34) times more likely to be co-infected compared to individuals who had a WHO clinical stage of III in crude analysis. Government employed individuals were 56% less likely to be co-infected compared to commercial sex worker [Table 3].
Discussion
The ever-increasing prevalence of PTB in Ethiopia has been made worse by the increasing incidence of HIV/AIDS. In this study, we noted higher prevalence of PTB (7.5%) among HIV positive pre-ART patients. This finding is in line with studies conducted in Nigeria (7.8%) and Tanzania (8.5%) [21, 22]. However, the finding of this study was lower compared to studies conducted in Cambodia (12%), Nigeria (32.8%) and India (19.2%) [23–25]. The presence of this difference could be explained by the fact that this study considers only PTB but not other forms of TB. Our study was also restricted to pre-ART HIV positive patients in which relatively strong immunity might have contributed for lower prevalence of TB-HIV co-infection since opportunistic infections are more prevalent during compromised immune status.
Of pulmonary tuberculosis co-infected cases, 19 (63.3%) were smear negative. This result is almost in line with study findings of Tanzania (60%), India (68.9%) and Ethiopia (58%) [22, 25, 26] but lower than what was reported from Nigeria (82.5%) [21]. This difference might be due to the variation in concentration of acid fast bacilli in the sputum and the rate of caseation necrosis.
Tuberculosis can occur at any stage of HIV disease, and its manifestations depend largely on the level of immunosuppression. Early during HIV disease, symptoms and signs are similar to those in HIV-uninfected persons: the lungs are most commonly affected, with cough, fever, and respiratory signs along with radiographic lesions, often with cavitations [27]. In the present study, 93.3% of co-infected study subjects were found to have constitutional symptoms; cough of greater than two weeks duration, fever, night sweat and weight loss. Radiological abnormalities suggestive of PTB are also witnessed in 90% of co-infected study subjects. This result was in parallel with previous findings used for TB diagnosis and treatment guideline development.
The mean CD4+ lymphocyte count of HIV mono-infected participants was 296 ± 192 Cells/mm3 and TB-HIV co-infected patients had mean CD4+ lymphocyte count of 199 ± 149 Cells/mm3. The mean difference was statistically significant with p value of 0.007. Sixteen (53.3%) of co-infected patients were found to have CD4+ lymphocyte count of less than 200 Cells/mm3. As CD4+ lymphocyte count decreased the body defense mechanism will be overwhelmed by various opportunistic infections. In multivariate analysis, CD4+ lymphocyte count was found to be independently associated with TB/HIV co-infection. Individuals who had CD4+ lymphocyte count of <200Cells/mm3 were 2.9 times more likely to be co-infected than individuals who had CD4+ lymphocyte count of ≥350Cells/mm3. A study conducted in Nigeria revealed similar finding where lower CD4+ lymphocyte count was observed in co-infected patients than mono infected patients [21]. Our study had also revealed a significant statistical association between WHO clinical stage and TB-HIV co-infection. Individuals who had a WHO clinical stage of IV were 8.6 times more likely to be co-infected compared to individuals who had a WHO clinical stage of III in crude analysis. Those patients with advanced WHO clinical stage had higher likelihood of having TB and other opportunistic infections as it is seen in CD4+ lymphocyte count.
Though it is not statistically significant, government employed individuals were 56% less likely to be co-infected compared to commercial sex worker. This could happen due to obvious reasons that commercial sex workers are liable for many opportunistic infections as an occupational risk. It needs great emphasis for prevention and interventional activities to reduce the burden of opportunistic infections and other complications associated with HIV/AIDS.
Our study included only pre-ART HIV positive patients which have relatively strong immunity compared to patients on ART. This needs great emphasis to avoid misapprehension by health professionals for early detection of opportunistic infections. Hence the main point of selecting only ART naïve patients in this study is to appreciate the value of close follow up of pre-ART patients to prevent early deterioration of patients by undetected opportunistic infections. Early detection of opportunistic infections including tuberculosis could be performed by lower level of health institutions including health extension workers involvement. This study was conducted at HIV/AIDS clinic and recruited those patients having regular follow up to imitate the situation present in the area. The limitation of this study is that laboratory diagnosis of TB was made only by ZN technique in addition to clinical and radiological investigations. Culture and molecular techniques were not used because of unavailability.
Conclusion
Higher prevalence of PTB was found in pre- ART HIV positive patients. Lower CD4+ lymphocyte count was found to be the only predicting factor for co-infection. Early detection of co-infection is very necessary to prolong their ART initiation time and by then strengthening their immune status. Further research both on ART and pre-ART patients is recommended to know the co-infection rate.
Abbreviations
- AFB:
-
Acid Fast Bacilli
- AIDS:
-
Acquired Immune Deficiency Syndrome
- ART:
-
Anti Retroviral Treatment
- BD FACS:
-
Becton Dickinson Fluorescence-Activated Cell Sorting
- CD4:
-
Cluster of Differentiation
- CI:
-
Confidence Interval
- CXR:
-
Chest X-Ray
- EDTA:
-
Ethylene Diamine-Tetra-acetic Acid
- HIV:
-
Human Immunodeficiency Virus
- OR:
-
Odds Ratio
- PTB:
-
Pulmonary Tuberculosis
- SD:
-
Standard Deviation
- SPSS:
-
Statistical Packages for Social Sciences
- TB:
-
Tuberculosis
- WHO:
-
World Health Organization
- ZN:
-
Ziehl-Neelson.
References
WHO, UCSF: Report on HIV/AIDS in Ethiopia. CDC MMWR. 2003, 52: 217-
Harrington M: From HIV to Tuberculosis and Back Again: A Tale of Activism in 2 Pandemics. Clin Infect Dis. 2010, 50: S260-S266. 10.1086/651500.
Friedland G, Churchyard GJ, Nardell E: Tuberculosis and HIV coinfection: current state of knowledge and research priorities. J Infect Dis. 2007, 196: S1-S3. 10.1086/518667.
Meya DB, McAdam KP: The TB pandemic: an old problem seeking new solutions. J Intern Med. 2007, 261: 309-329. 10.1111/j.1365-2796.2007.01795.x.
Girardi E, Raviglione MC, Antonucci G, Godfrey-Faussett P, Ippolito G: Impact of the HIV epidemic on the spread of other diseases: the case of tuberculosis. AIDS. 2000, 14: 3S47-3S56.
Sutherland I: Recent studies in the epidemiology of tuberculosis, based on the risk of being infected with tubercle bacilli. Adv Tuberc Res. 1976, 19: 1-63.
Vynnycky E, Fine PE: The natural history of tuberculosis: the implications of age-dependent risks of disease and the role of re-infection. Epidemiol Infect. 1997, 119: 183-201. 10.1017/S0950268897007917.
Bucher HC, Griffith LE, Guyatt GH, Sudre P, Naef M, Sendi P, Battegay M: Isoniazid prophylaxis for tuberculosis in HIV infection: a meta-analysis of randomized controlled trials. AIDS. 1999, 13: 501-507. 10.1097/00002030-199903110-00009.
Selwyn PA, Hartel D, Lewis VA, Schoenbaum EE, Vermund ST, Klein RS, Walker AT, Friedland GH: A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med. 1989, 320: 545-550. 10.1056/NEJM198903023200901.
Girardi E, Raviglione MC, Antonucci G, Godfrey-Faussett P, Ippolito G: Impact of the HIV epidemic on the spread of other diseases: the case of tuberculosis. AIDS. 2000, 14: S47-S56.
Lawn SD, Churchyard G: Epidemiology of HIV-associated tuberculosis. Curr Opin HIV AIDS. 2009, 4: 325-333. 10.1097/COH.0b013e32832c7d61.
Federal Ministry of Health (FMOH), HIV Prevention and Control Office: Single Point HIV Prevalence Estimate. 2007, , Addis Ababa, Ethiopia,http://www.etharc.org/aidsineth/publications/singlepointprev,
Havlir DV, Barnes PF: Tuberculosis in patients with human immunodeficiency virus infection. N Engl J Med. 1999, 340: 367-373. 10.1056/NEJM199902043400507.
Jones BE, Young SM, Antoniskis D, Davidson PT, Kramer F, Barnes PF: Relationship of the manifestations of tuberculosis to CD4 cell counts in patients with human immunodeficiency virus infection. Am Rev Respir Dis. 1993, 148: 1292-1297.
Zumla A, Malon P, Henderson J, Grange JM: Impact of HIV infection on tuberculosis. Postgrad Med J. 2000, 76: 259-268. 10.1136/pmj.76.895.259.
World Health Organization: Global Tuberculosis control: Surveillance, planning and Financing. 2008,http://www.who.int/tb/publications/global_report/en/_,
Daniel WW: Biostatistics. A foundation for analysis in the Health Sciences. 2004, Wiley International Edition, USA, 8
International Union against Tuberculosis and Lung Disease: Sputum examination for tuberculosis by direct microscopy in low income countries. 2000, IUATLD, Paris, 5
BD FACS Count System User’s Guide for Use with BD FACS Count CD4 Reagents. 2008,http://www.bdbiosciences.com/external_files/pm/doc/manuals/live/web_enabled/339011,
Tuberculosis care with TB-HIV co-management: Integrated Management of Adolescent and Adult Illness. 2007
Iliyasu Z, Babashani M: Prevalence and Predictors of Tuberculosis Coinfection among HIV-Seropositive Patients Attending the Aminu Kano Teaching Hospital, Northern Nigeria. Epidemiology. 2009, 19: 81-87. 10.2188/jea.JE20080026.
Ngowi BJ, Mfinanga SG, Bruun JN, Morkve O: Pulmonary tuberculosis among people living with HIV/AIDS attending care and treatment in rural northern Tanzania. BMC Publ Health. 2008, 8: 341-10.1186/1471-2458-8-341.
Kimerling ME, Schuchter J, Chanthol E, Kunthy T, Stuer F, Glaziou P, Ee O: Prevalence of pulmonary tuberculosis among HIV-infected persons in a home care program in Phnom Penh, Cambodia. Int J Tuberc Lung Dis. 2002, 6: 988-994.
Awoyemi OB, Ige M, Onadeko BO: Prevalence of active pulmonary tuberculosis in human immunodeficiency virus seropositive adult patients in University College Hospital, Ibadan, Nigeria. Afr J Med Med Sci. 2002, 31: 329-332.
Rajasekaran S, Mahilmaran A, Annadurai S, Kumar S, Raja K: Manifestation of tuberculosis in patients with human immunodeficiency virus: A large Indian study. Ann Thorac Med. 2007, 2: 58-60. 10.4103/1817-1737.32231.
Kassu A, Mengistu G, Ayele B, Diro E, Mekonnen F, Ketema D, Moges F, Mesfin T, Getachew A, Ergicho B, Elias D, Aseffa A, Wondmikun Y, Ota F: Coinfection and clinical manifestations of tuberculosis in human immunodeficiency virus-infected and -uninfected adults at a teaching hospital, northwest Ethiopia. J Microbiol Immunol Infect. 2007, 40: 116-122.
Swaminathan S, Padmapriyadarsini C, Narendran G: HIV-Associated Tuberculosis: Clinical Update. Clin Infect Dis. 2010, 50: 1377-1386. 10.1086/652147.
Acknowledgements
We acknowledge the technical support provided by Gondar University hospital. Our special thanks and appreciation also goes to all the study participants who voluntarily participate in this study. Lastly but not least, we also thank Gondar University hospital ART laboratory personnel for their consistent support with reagents and other materials during the project work.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YW: participated in conception and design of the study, data collection, analysis and interpretations of the findings, reviewed the manuscript. DM: participated in the design of the study, analysis and interpretations of the findings, drafting the manuscript and write up. YB: supervision of the study, analysis and interpretations of the findings, reviewed the manuscript. All authors reviewed and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Wondimeneh, Y., Muluye, D. & Belyhun, Y. Prevalence of Pulmonary tuberculosis and immunological profile of HIV co-infected patients in Northwest Ethiopia. BMC Res Notes 5, 331 (2012). https://doi.org/10.1186/1756-0500-5-331
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1756-0500-5-331