
Abstract
Background
In acupuncture, deqi is the sensory experience related to clinical efficacy. As the first study taking into account cultural differences on deqi sensation, this pilot survey aims to corroborate the acupuncturists' general experience in clinical practice with functional magnetic resonance imaging (fMRI) findings.
Methods
Questionnaires were distributed to acupuncturists of TCM (traditional Chinese medicine)hospitals and acupuncturists attending workshops and seminars in the United States and China. Questions covered clinical significance of deqi, patient attitude and the nature of some pain-related sensations elicited by manual needling.
Results
47 out of a total of 86 acupuncturists agreed that dull pain was deqi and over half regarded it beneficial, while sharp pain was non-deqi and harmful instead. The patients' attitude toward deqi sensation showed a difference between US and China. There was no other dimension showing a difference.
Conclusion
Results of this pilot survey indicate that the acupuncturists' perception is consistent with our previous fMRI findings. Results showed almost complete agreement that dull pain is considered deqi and beneficial to treatment, while sharp pain is not deqi and harmful. Particularly, dull pain was deqi and was beneficial to treatment whereas sharp pain was not. Patients in China liked the deqi experience whereas those in the US did not.
Similar content being viewed by others


Background
Acupuncture stimulation elicits a sensory response termed deqi which literally means "the arrival of vital energy" in traditional Chinese medicine ( TCM). Multiple unique sensations experienced by the patient around the site of needle manipulation are often described as suan (aching or soreness), ma (numbness or tingling), zhang (fullness/distention or pressure) and zhong (heaviness) [1]. While pain is also experienced occasionally, the type of pain has not been well characterized. The increased resistance of the needle is felt by the acupuncturist (needle grasping) as tense, tight and full like "a fish biting onto the bait." as described in the literature [1–3]. Needle grasping is believed to be related to clinical efficacy [1–4] although little data are available [5–7]. The acupuncturist's skills, competence and understanding of the TCM theory also play an important role in the therapeutic outcome [8].
Randomized, placebo-controlled clinical trials of acupuncture evaluate its efficacy by separating the specific effects from the non-specific ones [8]. While a number of clinical trials failed to find verum acupuncture more effective than sham acupuncture in migraine [9, 10] low back pain [11, 12] and knee osteoarthritis [13, 14], both verum and sham acupuncture were more beneficial than the waiting control. However, many of the studies included in the analysis did not satisfy the criteria for dosage adequacy required for optimal clinical efficacy [15] and that sham is not necessarily inert [16, 17]. The intensity of the psychophysical and neurological response of deqi is now proposed to serve as a basis for dosage measurement [15, 18], calling for a better understanding of the qualitative and quantitative characterization of the deqi sensation.
Most studies described the qualitative characteristics of sensations unique to acupuncture based on interviews of patients and expert acupuncturists [5, 19]. Recently, several groups created quantitative sensation scales and deqi indices based on pain questionnaires distributed to acupuncture patients [5, 20–25]. Classical sensations such as aching, soreness, numbness, fullness and heaviness were included. Sharp pain is not regarded as a beneficial deqi sensation by most acupuncturists. Most reports failed to separate it from dull pain in the categorization of deqi response; only a few reports with quantitative measures distinguished sharp pain from deqi[15, 20, 22]. We attempted to separate the acupuncture sensations into two major categories, namely sensations that do not hurt (aching, soreness and dull pain) as deqi and sensations that do hurt (sharp pain) as noxious stimulation [26, 27]. Our findings showed that the deqi response was elicited in 71% acupuncture versus 24% tactile and that the frequency and intensity of sensations were significantly greater than tactile. Dull pain was significantly different from the tactile group among the gamut of sensations comprising deqi. Importantly, we have consistently observed distinct patterns of limbic network hemodynamic response in the brain, namely deactivation in deqi and activation in sharp pain. Our findings are in fair agreement with Macpherson's report [22] and the Southampton group [25]. Taken together, these psychophysical and hemodynamic response patterns may provide a qualitative and quantitative measure of the patient's response to manual needle manipulation [26–28].
This pilot survey aims to provide a picture by focusing on the items that are seldom described such as the subject's throbbing and dull pain and the acupuncturist's grasping sensation, serving as a foundation for a better understanding of acupuncture effects.
Methods
Survey design
The questionnaire was created collaboratively by the clinical acupuncturists and research staff at the Athinoula Martinos Center of Biomedical Imaging (Charlestown, MA, United States). Instead of the traditional sensations such as soreness, numbness and heaviness, we focused on sensations that are often overlooked (ie dull pain, sharp pain and throbbing).
Paper questionnaires were answered by licensed Chinese medicine practitioners on a self-reported and voluntary basis. Participants were asked whether they considered a specific type of pain-related sensation elicited from manual needling was deqi and whether it was beneficial or harmful to the patient. The questions were designed in a multiple-choice format and tailored to specifically address the nature of acupuncture sensations and its clinical significance based on the experience of the patient and the acupuncturist. Besides definitive answers, the participant was allowed to select "unsure" and allocated space for comments.
Survey administration
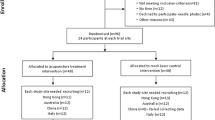
Fifty questionnaires were distributed to licensed acupuncturists attending workshop seminars directed by one of the co-authors (LL): 30 in Chicago (USA) and 20 in Shanghai (China). Questionnaires were also distributed to acupuncturists in Chinese medicine teaching institutions: 20 to the School of Traditional Chinese Medicine in San Francisco (United States) and 6 to Guang'anmen Hospital of the China Academy of Traditional Chinese Medicine in Beijing (China). Another ten questionnaires were distributed via email to the Beijing University of Chinese Medicine (China). Questionnaires were bilingual in English and Chinese. Survey participation was on a voluntary basis and did not involve patients; no consent form was needed. The acupuncturists' names were kept confidential. The distributors did not participate in the design of the questionnaires but in data analysis.
Statistical methods
A test of two proportions using two-tailed Fisher's Exact test was used to compare the sample proportions from the two countries using the conventional criterion for statistical significance, alpha = 0.05. Analyses were performed using Minitab v15 (Minitab® Statistical Software, USA).
Results
Participation rate
Of the 86 questionnaires distributed, 47 were returned, representing a 55% response rate. Of the 47 respondents, 26 were from the US and 21 from China. Four of the returned questionnaires from the US were excluded from analysis because the respondents indicated that the questions were unclear to them. The total of 43 returned questionnaires pooled from both countries for the final analysis represented 50% of the 86 questionnaires distributed and 92% of the 47 respondents. All the respondents in this study identified themselves in the survey as those practicing acupuncture of traditional Chinese style.
Participants
The training experience for participants pooled from the two countries averaged 6.4 years (range 2-18). Experience in practice averaged 12 years, (range 1-32). A larger range was observed for acupuncturists in China in years of practice (1-32 years) than those in the US (1.5-17 years).
Relative importance in clinical efficacy: subject's vs acupuncturist's sensations
When asked whether the patient's or the acupuncturist's deqi experience is more important for clinical efficacy (Table 1), an overwhelming majority (77%) of participants selected "both the acupuncturist's deqi experience and the subject's deqi experience are important" without favoring one or the other. A small number, 12%, favored the patient's experience and 5% favored the acupuncturist's.
Relationship between acupuncturist's needle grasping sensation and patient's deqi response
Participants were asked if there was a relationship between the needle grasping sensation felt by the acupuncturist and the patient's deqi experience (Table 1). Most respondents indicated that the acupuncturist's needle grasping and the patient's deqi experience occurred concurrently (41%) or that sometimes they occurred concurrently (31%). Almost a quarter of respondents (24%) was unsure or not providing an answer.
Patient's attitude towards deqi sensations
Participants were questioned about their patient's attitudes towards deqi sensations (Table 1). A total of 40% of participants reported that patients liked the deqi sensations whereas 19% reported "dislike" and rest neutral. There was an interesting difference between the two countries regarding the deqi sensation. Of the 17 respondents who indicated that the patients liked the sensations, only 2 were from the US and all the rest from China (P < 0.0001). In contrast, of all returned questionnaires that indicated "dislike" (19%), all were from the US and none from China (P = 0.0020).
Correlation between deqi response and efficacy
Participants were asked whether there was a correlation between deqi and clinical efficacy in their acupuncture practice (Table 1). A total of 30 respondents (73%) indicated a positive correlation; no cultural differences among the respondents.
Types of pain and deqi
Participants were asked to indicate "deqi" or "not deqi" for sensations often associated with pain, such as throbbing, dull pain and sharp pain and whether these sensations were beneficial or harmful. Of all participants, 72% agreed that dull pain was characteristic of deqi and beneficial to clinical efficacy (53%). Only 2-3% indicated dull pain was "not deqi" and harmful. About 20% of returned questionnaires did not have the answer for the question.
Very few participants considered sharp pain to be deqi or beneficial (7% and 14% respectively) and 50% classified it as "not deqi" and 42% believed it was harmful.
Respondents were less certain about the nature of throbbing and its relation to efficacy than they were about dull pain or sharp pain. Responses were almost equally divided between "deqi" (28%) and "not deqi" (21%). While over two-thirds answered "unsure" or did not provide an answer, 14% considered throbbing as "beneficial" and 21% "harmful".
In summary (Table 2), the majority of respondents considered dull pain to be deqi (91%), beneficial and clinically efficacious (96%). Conversely, 88% of respondents considered sharp pain to be "not deqi" and 75% considered sharp pain harmful and non-efficacious. In respect of throbbing, while respondents who opted for no answer or 'unsure' were the majority, no significant differences were observed between those favoring deqi and beneficial or non-deqi and harmful.
Discussion
Limitations
The sample size of this study was small and the scope of this survey is narrow. The exclusion of the timing of deqi assessment and sensations is also a limitation of this study. We consider a participant's reliance on memory in respect of sensation timing may result inaccuracy in a survey; therefore, we advocate a detailed exploration of dosage and patient attitude in an apposite clinical lab setting.
Relation between deqi and clinical efficacy
Most participants (77%) in both countries believed there was a positive correlation between deqi and clinical efficacy. Our fMRI studies found a positive correlation between a subject's psychophysical and hemodynamic response: ie strong deqi sensations induced strong deactivation of the limbic system [27, 28]. Such correlation provides strong evidence, albeit indirect, that neurophysiological effects of acupuncture deqi are mediated via specific brain networks.
Most participants indicated that both the patient's deqi and the acupuncturists' grasping sensation were important. However, this pilot survey found that a small percentage of participants disagreed with the majority, with 12% favoring the patient's experience and 5% favoring the acupuncturist's sensory experience.
Dull pain, sharp pain and throbbing
Of the three types of pain related sensations, dull pain was generally considered to be deqi and beneficial while sharp pain was considered to be unrelated and noxious instead. In regard to throbbing, about half of the respondents were uncertain; the rest were almost equally divided between the two categories. Dull pain is seldom described in acupuncture literature. Park and Lee mentioned a 'dull' sensation but did not specify whether it was pain-related [23]. We first called attention to dull pain as a characteristic component of deqi and noted that it often occurred before or independent of sharp pain instead of occurring after sharp pain as described in the literature [26, 27]. This pilot survey found that most respondents indicated dull pain as deqi and beneficial and sharp pain as noxious and harmful. These sensations and their relationship to deqi are often overlooked/neglected sensations. We regard their importance as we encounter them in our studies. With fMRI monitoring, we demonstrated that dull pain deactivated the limbic system and that sharp pain activated it [27, 28]. Our findings are in agreement with MacPherson's report [22].
The survey results on throbbing were less definitive than dull pain or sharp pain; most participants were unsure of its nature and the rest were equally divided between deqi and not deqi as well as between beneficial and harmful. There is little information on throbbing in the literature. Occasional reports suggest that it occurs more often in electro- than in manual acupuncture; it's association with neuronal activity is unclear [5, 23]. Our fMRI studies found that this sensation could be associated with either predominant deactivation or activation of the limbic system and pain matrix; throbbing may represent an intermediate stage in the excitation of the fine pain conducting fibers; a progressive increase in the intensity of mechanical stimulation may cause transition from the more innocuous dull pain to throbbing and finally to overt noxious sharp pain.
The significant difference between the two countries in respect of the patients' attitudes towards deqi sensation may have clinical implications. Most respondents in China reported that patients liked the deqi sensations while those from the US disliked them. Interestingly, this was the only response that showed significant difference between the two countries. A difference in patients' attitudes may affect how acupuncturists adjust their techniques and intensity of stimulationto the sentiments of his patients. This raises an important question as to how TCM practices are translated and practiced across cultures and uncovers confounds in meta-analysis of clinical efficacy studies. It is possible that acupuncturists in the US adopt less intensive and shorter durations of stimulations out of consideration for the patients' attitudes towards the sensory experience, resulting in lower dosage levels and lower therapeutic effects. Further investigation with large clinical sample sizes is warranted.
Conclusion
Results of this pilot survey indicate that the acupuncturists' perception is consistent with our previous fMRI findings. This survey contributes valuable information regarding the opinions of practicing acupuncturists on the nature of deqi in U.S. and China, to support our fMRI findings. Particularly, dull pain was deqi and was beneficial to treatment whereas sharp pain was not. Patients in China liked the deqi experience whereas those in the U.S. did not.
Abbreviations
- fMRI:
-
Functional Magnetic Imaging
- TCM:
-
Traditional Chinese Medicine
- US:
-
United States
References
Cheng XN: Chinese Acupuncture and Moxibustion. 1987, Beijing: Foreign Language Press
Li Y: Yi Xue Ru Men. 2006, Beijing: People's Health Publishing
Yang JZ: Great Compendium of Acupuncture and Moxibustion (Zhen Jiu Da Cheng). 1987, Beijing: People's Health Publishing
Wu JN: Ling Shu or the Spiritual Pivot. Beijing: People's Health Publishing. 1963
Kong J, Gollub R, Huang T, Polich G, Napadow V, Hui KKS, Vangel M, Rosen B, Kaptchuk TJ: Acupuncture de qi, from qualitative history to quantitative measurement. J Altern Complement Med. 2007, 10: 1059-1070. 10.1089/acm.2007.0524.
Xu HZ: Acupuncture (Zhen Jiu Xue). 2004, Beijing: People's Health Publishing
Liang FR: Acupuncture (Zhen Jiu Xue). 2005, Beijing: China Traditional Chinese Medicine Publishing
Liu T: Role of acupuncturists in acupuncture treatment. Evid Based Complement Alternat Med. 2007, 1: 3-6. 10.1093/ecam/nel061.
Linde K, Streng A, Jurgens S, Hoppe A, Brinkhaus B, Witt C, Wagenpfeil S, Pfaffenrath V, Hammes MG, Weidenhammer W, Willich SN, Melchart D: Acupuncture for patients with migraine: a randomized controlled trial. JAMA. 2005, 293: 2118-2125. 10.1001/jama.293.17.2118.
Diener HC, Kronfeld K, Boewing G, Lungenhausen M, Maier C, Molsberger A, Tegenthoff M, Trampisch HJ, Zenz M, Meinert R, GERAC Migraine Study Group: Efficacy of acupuncture for the prophylaxis of migraine, a multicentre randomized controlled clinical trial. Lancet Neurol. 2006, 5: 310-6. 10.1016/S1474-4422(06)70382-9.
Brinkhaus B, Witt CM, Jena S, Linde K, Streng A, Wagenpfeil S, Irnich D, Walther HU, Melchart D, Willich SN: Acupuncture in patients with chronic low back pain -- a randomized controlled trial. Arch Intern Med. 2006, 166: 450-457. 10.1001/.450.
Haake M, Müller HH, Schade-Brittinger C, Basler HD, Schäfer H, Maier C, Endres HG, Trampisch HJ, Molsberger A: German Acupuncture Trials (GERAC) for chronic low back pain: randomized, multicenter, blinded, parallel-group trial with 3 groups. Arch Intern Med. 2007, 167: 1892-1898. 10.1001/archinte.167.17.1892.
Scharf HP, Mansmann U, Streitberger K, Witte S, Kramer J, Maier C, Trampisch HJ, Victor N: Acupuncture and knee osteoarthritis: a three-armed randomized trial. Ann Intern Med. 2006, 145: 12-20.
Witt CM, Jena S, Brinkaus B, Liecker B, Wegscheider K, Willich SN: Acupuncture in patients with osteoarthritis of the knee or hip. A randomized, controlled trial with an additional nonrandomized arm. Arthritis Rheum. 2006, 54: 3485-3493. 10.1002/art.22154.
White A, Cummings M, Barlas P, Cardini F, Filshie J, Foster NE, Lundeberg T, Stener-Victorin E, Witt C: Defining an adequate dose of acupuncture using a neurophysiological approach. Acupunct Med. 2008, 26: 111-120. 10.1136/aim.26.2.111.
Dincer F, Linde K: Sham interventions in randomized clinical trials of acupuncture - a review. Complement Ther Med. 2003, 11: 235-242. 10.1016/S0965-2299(03)00124-9.
Lund I, Naslund J, Lundeberg T: Minimal acupuncture is not a valid placebo control in randomized controlled trials of acupuncture: a physiologist's perspective. Chin Med. 2009, 4: 1-10.1186/1749-8546-4-1.
Benham A, Johnson MI: Could acupuncture needle sensation be a predictor of analgesic response?. Acupunct Med. 2009, 27: 65-67. 10.1136/aim.2008.000174.
Kim Y, Park J, Lee H, Bang H, Park HJ: Content validity of an acupuncture sensation questionnaire. J Altern Complement Med. 2008, 14: 957-963. 10.1089/acm.2007.0565.
Asghar AUR, Green G, Lythgoe MF, Lewith G, MacPherson H: Acupunture needling sensations: The neural correlates of deqi using fMRI. Brain Res. 2010, 1315: 111-8. 10.1016/j.brainres.2009.12.019.
Leung AY, Park J, Schultels G, Duann JR, Yaksh T: The electrophysiology of de qi sensations. J Altern Complement Med. 2006, 8: 743-50. 10.1089/acm.2006.12.743.
MacPherson H, Asghar A: Acupuncture needle sensations associated with de qi: A classification based on expert's ratings. J Altern Complement Med. 2006, 7: 633-637. 10.1089/acm.2006.12.633.
Park J, Lee H: Does Deqi (needle sensation) exist?. Am J Chin Med (Gard City N Y). 2002, 30: 45-50. 10.1142/S0192415X02000053.
Vincent CA, Richardson PH, Black JJ, Pither CE: The significance of needle placement site in acupuncture. J Psychosom Res. 1989, 33: 489-496. 10.1016/0022-3999(89)90010-X.
White P, Bishop F, Hardy H, Abdollahian S, White A, Park J, Kaptchuk TJ, Lewith GT: Southampton needle sensation questionnaire: development and validation of a measure to gauge a needle sensation. J Altern Complement Med. 2008, 14: 373-9. 10.1089/acm.2007.0714.
Hui KKS, Nixon EE, Vangel MG, Liu J, Marina O, Napadow V, Hodge SM, Rosen BR, Makris N, Kennedy DN: Characterization of the "deqi" response in acupuncture. BMC Complement Altern Med. 2007, 1: 33-10.1186/1472-6882-7-33.
Hui KKS, Liu J, Marina O, Napadow V, Haselgrove C, Kwong KK, Kennedy DN, Makris N: The integrated response of the human cerebro-cerebellar and limbic systems to acupuncture stimulation at ST36 as evidenced by fMRI. Neuroimage. 2005, 3: 479-496. 10.1016/j.neuroimage.2005.04.037.
Hui KK, Marina O, Claunch JD, Nixon EE, Fang J, Liu J, Li M, Napadow V, Vangel M, Makris N, Chan ST, Kwong KK, Rosen BR: Acupuncture mobilizes the brain's default mode and its anti-correlated network in healthy subjects. Brain Res. 2009, 1287: 84-103. 10.1016/j.brainres.2009.06.061.
Acknowledgements
The work was supported by the NIH/National Center for Complementary and Alternative Medicine (1-P01-002048-01) (2-P01-002048-06), National Center for Research Resources (P41RR14075), Mental Illness and Neuroscience Discovery Institute (MIND) and Brain Project Grant (NS 34189).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
KKSH and LL conceived the study design and interpreted the data. KKSH wrote the manuscript. LL finalized the manuscript. TS performed data analysis and helped write the manuscript. ML performed the acupuncture in our acupuncture database in our previous studies. MGV conducted and supervised statistical analysis. JF participated in the design of the questionnaire. All authors have read and approved the final version of the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Hui, K.K., Sporko, T.N., Vangel, M.G. et al. Perception of Deqi by Chinese and American acupuncturists: a pilot survey. Chin Med 6, 2 (2011). https://doi.org/10.1186/1749-8546-6-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1749-8546-6-2